
Periodontal and Peri-Implant Diseases and Systemically Administered Statins: A Systematic Review

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
- P—Population: subjects with untreated periodontitis and peri-implant disease without comorbidities potentially affecting their periodontal/peri-implant status and not under drugs affecting lipid nor bone metabolism;
- I—Intervention: effect of routine use of systemically delivered statin;
- C—Comparison: no systemically delivered statin use/placebo administration;
- O—Outcome: periodontal parameters around natural teeth and implants.
2.2. Information Sources and Search
- Statin/statins;
- OR simvastatin/atorvastatin/cerivastatin/fluvastatin/lovastatin/pitavastatin/pravastatin/ rosuvastatin;
- OR hydroxymethylglutaryl-coa reductase/hmgcoa reductase inhibitors;
- Periodontitis;
- OR periodontal health/diseases/inflammation/pocket/lesion(s)/treatment/therapy/debridement/defect/parameters;
- OR peri-implantitis;
- OR peri-implant tissues/health/diseases/inflammation/mucositis/pocket/lesion(s)/treatment/therapy/debridement/defect/parameters;
- OR CAL (acronym of Clinical Attachment Level);
- OR PPD (acronym of Periodontal Probing Depth);
- OR BoP (acronym of Bleeding on Probing);
- OR guided periodontal tissue/guided bone regeneration;
- OR crevicular cytokines/IL-1B/TNF-a/IL-6/IL-8.
2.3. Study Selection Process
2.4. Data Collection Process and Items
2.5. Risk of Bias Assessment for Individual Studies
- Selection (random sequence generation, allocation concealment);
- Performance (blinding of investigators and participants);
- Detection (blinding of outcome assessment);
- Attrition (incomplete outcome data);
- Reporting (selective outcome reporting);
- Others.
- Confoundingvariables;
- Selection of participants;
- Classification of interventions;
- Deviations from intended interventions;
- Missing data;
- Measurement of outcomes;
- Selection of the reported result.
3. Results
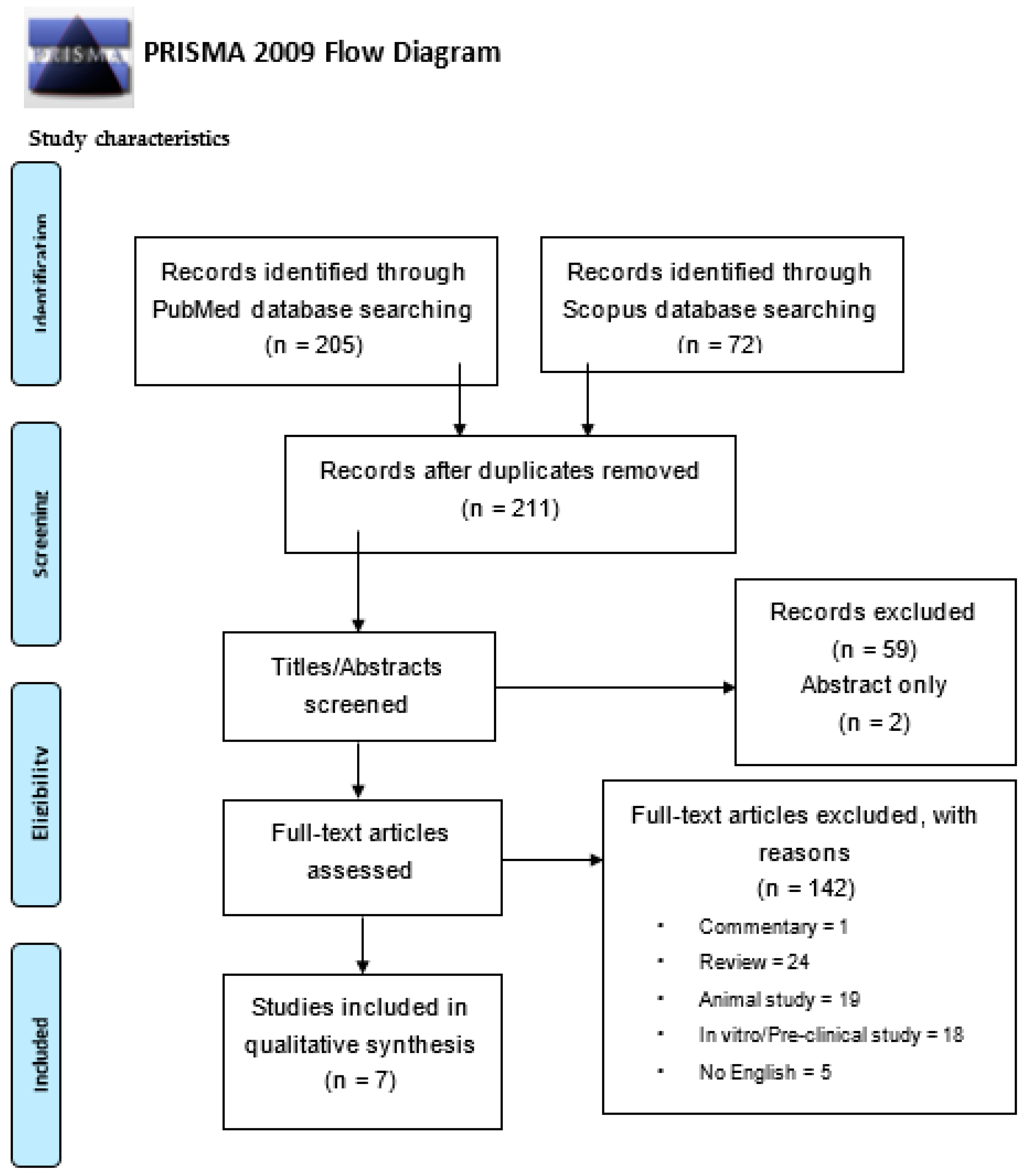
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abraham, S.; Premnath, A.; Arunima, P.R.; Kassim, R.M. Critical Appraisal of Bidirectional Relationship between Periodontitis and Hyperlipidemia. J. Int. Soc. Prev. Community Dent. 2019, 9, 112–118. [Google Scholar] [CrossRef]
- Nelson, R.H. Hyperlipidemia as a Risk Factor for Cardiovascular Disease. Prim. Care Clin. Off. Pract. 2013, 40, 195–211. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S74–S84. [Google Scholar] [CrossRef]
- Löe, H.; Silness, J. Periodontal Disease in Pregnancy I. Prevalence and Severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Ramaglia, L.; Di Spirito, F.; Sirignano, M.; La Rocca, M.; Esposito, U.; Sbordone, L. A 5-year longitudinal cohort study on crown to implant ratio effect on marginal bone level in single implants. Clin. Implant. Dent. Relat. Res. 2019, 21, 916–922. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Brevi, B.; Martuscelli, R.; Sbordone, L.; Di Spirito, F. Computed tomography-aided descriptive analysis of maxillary and mandibular atrophies. J. Stomatol. Oral Maxillofac. Surg. 2018, 120, 99–105. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef]
- Michaud, D.S.; Liu, Y.; Meyer, M.; Giovannucci, E.; Joshipura, K. Periodontal disease, tooth loss, and cancer risk in male health professionals: A prospective cohort study. Lancet Oncol. 2008, 9, 550–558. [Google Scholar] [CrossRef]
- Di Spirito, F.; Toti, P.; Pilone, V.; Carinci, F.; Lauritano, D.; Sbordone, L. The Association between Periodontitis and Human Colorectal Cancer: Genetic and Pathogenic Linkage. Life 2020, 10, 211. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Genco, R.; on behalf of working group 2 of the joint EFP/AAP workshop. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef] [PubMed]
- Lauritano, D.; Sbordone, L.; Nardone, M.; Iapichino, A.; Scapoli, L.; Carinci, F. Focus on periodontal disease and colorectal carcinoma. Oral Implant. 2017, 10, 229–233. [Google Scholar] [CrossRef]
- Soory, M. Association of periodontitis with rheumatoid arthritis and atherosclerosis: Novel paradigms in etiopathogeneses and management? Open Access. Rheumatol. 2010, 2, 1–6. [Google Scholar] [CrossRef][Green Version]
- Di Spirito, F.; La Rocca, M.; De Bernardo, M.; Rosa, N.; Sbordone, C.; Sbordone, L. Possible Association of Periodontal Disease and Macular Degeneration: A Case-Control Study. Dent. J. 2020, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Sbordone, L.; Pilone, V.; D’Ambrosio, F. Obesity and Periodontal Disease: A Narrative Review on Current Evidence and Putative Molecular Links. Open Dent. J. 2019, 13, 526–536. [Google Scholar] [CrossRef]
- Fu, Y.-W.; Li, X.-X.; Xu, H.-Z.; Gong, Y.-Q.; Yang, Y. Effects of periodontal therapy on serum lipid profile and proinflammatory cytokines in patients with hyperlipidemia: A randomized controlled trial. Clin. Oral Investig. 2015, 20, 1263–1269. [Google Scholar] [CrossRef] [PubMed]
- Pussinen, P.J.; Vilkuna-Rautiainen, T.; Alfthan, G.; Palosuo, T.; Jauhiainen, M.; Sundvall, J.; Vesanen, M.; Mattila, K.; Asikainen, S. Severe Periodontitis Enhances Macrophage Activation via Increased Serum Lipopolysaccharide. Arter. Thromb. Vasc. Biol. 2004, 24, 2174–2180. [Google Scholar] [CrossRef]
- D’Aiuto, F.; Ready, D.; Tonetti, M.S. Periodontal disease and C-reactive protein-associated cardiovascular risk. J. Periodontal Res. 2004, 39, 236–241. [Google Scholar] [CrossRef]
- Ide, M.; McPartlin, D.; Coward, P.; Crook, M.; Lumb, P.; Wilson, R. Effect of treatment of chronic periodontitis on levels of serum markers of acute-phase inflammatory and vascular responses. J. Clin. Periodontol. 2003, 30, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Cruz, J.; Saver, B.; Maupome, G.; Hujoel, P. Statin Use and Tooth Loss in Chronic Periodontitis Patients. J. Periodontol. 2006, 77, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Muniz, F.W.M.G.; Taminski, K.; Cavagni, J.; Celeste, R.K.; Weidlich, P.; Rösing, C.K. The effect of statins on periodontal treatment-a systematic review with meta-analyses and meta-regression. Clin. Oral Investig. 2018, 22, 671–687. [Google Scholar] [CrossRef] [PubMed]
- Baigent, C.; Keech, A.C.; Kearney, P.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Paulose-Ram, R.; Burt, V.L.; Kit, B.K. Prescription cholesterol-lowering medication use in adults aged 40 and over: United States, 2003–2012. NCHS Data Brief 2014, 177, 1–8. [Google Scholar]
- Maron, D.J.; Fazio, S.; Linton, M.F. Current Perspectives on Statins. Circulation 2000, 101, 207–213. [Google Scholar] [CrossRef]
- Lindy, O.; Suomalainen, K.; Mäkelä, M.; Lindy, S. Statin use is associated with fewer periodontal lesions: A retrospective study. BMC Oral Health 2008, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Saxlin, T.; Suominen-Taipale, L.; Knuuttila, M.; Alha, P.; Ylöstalo, P. Dual effect of statin medication on the periodontium. J. Clin. Periodontol. 2009, 36, 997–1003. [Google Scholar] [CrossRef]
- Valentaviciene, G.; Paipaliene, P.; Nedzelskiene, I.; Zilinskas, J.; Anuseviciene, O.V. The relationship between blood serum lipids and periodontal condition. Stomatologija 2006, 8, 96–100. [Google Scholar]
- Tahamtan, S.; Shirban, F.; Bagherniya, M.; Johnston, T.P.; Sahebkar, A. The effects of statins on dental and oral health: A review of preclinical and clinical studies. J. Transl. Med. 2020, 18, 1–42. [Google Scholar] [CrossRef]
- Petit, C.; Batool, F.; Bugueno, I.M.; Schwinté, P.; Benkirane-Jessel, N.; Huck, O. Contribution of Statins towards Periodontal Treatment: A Review. Mediat. Inflamm. 2019, 2019, 1–33. [Google Scholar] [CrossRef]
- Kellesarian, S.; Al Amri, M.; Al-Kheraif, A.; Ghanem, A.; Malmstrom, H.; Javed, F. Efficacy of Local and Systemic Statin Delivery on the Osseointegration of Implants: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2017, 32, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Bertl, K.; Parllaku, A.; Pandis, N.; Buhlin, K.; Klinge, B.; Stavropoulos, A. The effect of local and systemic statin use as an adjunct to non-surgical and surgical periodontal therapy—A systematic review and meta-analysis. J. Dent. 2017, 67, 18–28. [Google Scholar] [CrossRef]
- Estanislau, I.M.G.; Terceiro, I.R.C.; Lisboa, M.R.P.; Teles, P.D.B.; Carvalho, R.D.S.; Martins, R.S.; Moreira, M.M.S.M. Pleiotropic effects of statins on the treatment of chronic periodontitis-a systematic review. Br. J. Clin. Pharmacol. 2015, 79, 877–885. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, 12–13. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2008. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Al-Kuraishy, H.M.; Kadhim, S.S.; Al-Windy, S.A.; Al-Nami, M.S.; Al-Gareeb, A.I. Possible Role of Statins on the Inflammatory Biomarkers in Patients with Periodontal Disease: A Cross-Sectional Study. Dent. Hypotheses 2019, 10, 70. [Google Scholar] [CrossRef]
- Sangwan, A.; Tewari, S.; Singh, H.; Sharma, R.; Narula, S. Periodontal Status and Hyperlipidemia: Statin Users Versus Non-Users. J. Periodontol. 2013, 84, 3–12. [Google Scholar] [CrossRef]
- Suresh, S.; Narayana, S.; Jayakumar, P.; Sudhakar, U.; Pramod, V. Evaluation of anti-inflammatory effect of statins in chronic periodontitis. Indian J. Pharmacol. 2013, 45, 391–394. [Google Scholar] [CrossRef]
- Magán-Fernández, A.; Papay-Ramírez, L.; Tomás, J.; Marfil-Álvarez, R.; Rizzo, M.; Bravo, M.; Mesa, F. Association of Simvastatin and Hyperlipidemia with Periodontal Status and Bone Metabolism Markers. J. Periodontol. 2014, 85, 1408–1415. [Google Scholar] [CrossRef]
- Sayar, F.; Fallah, S.; Akhondi, N.; Jamshidi, S. Association of Serum Lipid Indices and Statin Consumption with Periodontal Status. Oral Dis. 2016, 22, 775–780. [Google Scholar] [CrossRef]
- Ari, V.C.; Ilarslan, Y.D.; Erman, B.; Sarkarati, B.; Tezcan, I.; Karabulut, E.; Oz, S.G.; Tanriover, M.D.; Sengun, D.; Berker, E. Statins and IL-1β, IL-10, and MPO Levels in Gingival Crevicular Fluid: Preliminary Results. Inflammation 2016, 39, 1547–1557. [Google Scholar] [CrossRef]
- Wagley, S.; Marra, K.V.; Salhi, R.A.; Gautam, S.; Campo, R.; Veale, P.; Veale, J.; Arroyo, J.G. Periodontal disease and age-related macular degeneration: Results from the National Health and Nutrition Examination Survey III. Retina 2015, 35, 982–988. [Google Scholar] [CrossRef]
- Di Spirito, F.; Pelella, S.; Argentino, S.; Sisalli, L.; Sbordone, L. Oral manifestations and the role of the oral healthcare workers in COVID-19. Oral Dis 2020, 1–2. [Google Scholar] [CrossRef]
- Di Spirito, F.; Iacono, V.J.; Iandolo, A.; Amato, A.; Sbordone, L. Evidence-based Recommendations on Periodontal Practice and the Management of Periodontal Patients during and after the COVID-19 Era: Challenging Infectious Diseases Spread by Air-borne Transmission. Open Dent. 2021, 15, 325–336. [Google Scholar] [CrossRef]
- Murphy, C.; Deplazes, E.; Cranfield, C.G.; Garcia, A. The Role of Structure and Biophysical Properties in the Pleiotropic Effects of Statins. Int. J. Mol. Sci. 2020, 21, 8745. [Google Scholar] [CrossRef] [PubMed]
- Fajardo, M.E.; Rocha, M.L.; Sánchez-Marin, F.J.; Espinosa-Chávez, E.J. Effect of atorvastatin on chronic periodontitis: A randomized pilot study. J. Clin. Periodontol. 2010, 37, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Billings, M.; Holtfreter, B.; Papapanou, P.N.; Mitnik, G.L.; Kocher, T.; Dye, B.A. Age-dependent distribution of periodontitis in two countries: Findings from NHANES 2009 to 2014 and SHIP-TREND 2008 to 2012. J. Clin. Periodontol. 2018, 45, S130–S148. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef]
- Graziani, F.; Karapetsa, D.; Alonso, B.; Herrera, D. Nonsurgical and surgical treatment of periodontitis: How many options for one disease? Periodontology 2000 2017, 75, 152–188. [Google Scholar] [CrossRef]
- Barone, A.; Chatelain, S.; Derchi, G.; Di Spirito, F.; Martuscelli, R.; Porzio, M.; Sbordone, L. Antibiotic’s effectiveness after erupted tooth extractions: A retrospective study. Oral Dis. 2020, 26, 967–973. [Google Scholar] [CrossRef]
- Poston, C.J.; Pierce, T.C.; Li, Y.; Brinson, C.W.; Lu, Z.; Lauer, A.W.; Leite, R.S.; Huang, Y. Statin intake is associated with MMP-1 level in gingival crevicular fluid of patients with periodontitis. Oral Dis. 2016, 22, 438–444. [Google Scholar] [CrossRef]
- Fentoğlu, Ö.; Sözen, T.; Öz, S.G.; Kale, B.; Sönmez, Y.; Öztürk Tonguç, M.; Gürgan, C.A.; Aykaç, Y.; Kırzıoğlu, F. Short-term effects of periodontal therapy as an adjunct to anti-lipemic treatment. Oral Dis. 2010, 16, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Alves, L.B.; Coelho, T.D.R.C.; de Azevedo, R.A.; Dos Santos, J.N.; Neves, F.S.; Cury, P.R. Systemic risk indicators for peri-implant diseases in individuals with implant-supported fixed prostheses: A cross-sectional study. Int. J. Oral Implantol. 2020, 13, 255–266. [Google Scholar]


{kind=link}
| Study Eligibility | Inclusion Criteria | Non-Inclusion Criteria |
|---|---|---|
| Sources | ||
| Databases | Electronic | Manual |
| Language | English language | Non-English language |
| Publication status | Published/in press/ahead of print | Submitted |
| Publication date | No restrictions | No restrictions |
| Text availability | Full-text access | Abstract-only |
| Study Characteristics | ||
| Type | Clinical | In vitro |
| Preclinical in vivo | ||
| Design | Randomized Clinical Trials (RCT) | Case reports |
| Prospective | Case series | |
| Retrospective | Narrative reviews | |
| Case-control | Conference papers | |
| Cross-sectional | Oral communications | |
| Books and chapters | ||
| Sample size | ≥70 | <70 |
| Population | Periodontal subjects | Periodontally healthy subjects |
| Age | ≥30 years old | <30 years old |
| Gender | No restrictions | No restrictions |
| Characteristics | Smoker/no smokers | Pregnancy; lactation |
| Comorbidities | Hyperlipidemia | Systemic disease affecting lipid/bone metabolism or periodontal disease |
| Cardiovascular disease | Medication-related osteonecrosis of the jaws | |
| Neoplastic disease | ||
| Non-surgical/surgical periodontal treatment (within ≥3 months) | ||
| Corticosteroids, antibiotics (within 3 months) | ||
| Drugs affecting bone metabolism Radiations (head and neck) | ||
| Treatments | None | |
| Intervention | Statin use | No statin use |
| Type | Systemically delivered statins (any) | Locally delivered statins (any) |
| Duration | ≥1 months | <1 months |
| Dosing | Low dose | High dose |
| Comparison | No statin use | Combined therapies |
| Other types of statin | ||
| Placebo use | ||
| Outcome(s) | Periodontal status | Endodontic–periodontal lesions |
| Endodontic lesions | ||
| Clinical periodontal parameters | Clinical Attachment Level (CAL) | |
| Periodontal Probing Depth (PPD) | ||
| Bleeding on Probing (BoP) | ||
| Gingival Index (GI) | ||
| Plaque Index (PI) | ||
| Tooth loss | ||
| Number of residual teeth | ||
| Radiographic periodontal parameters | Bone loss | |
| Other periodontal parameters | Gingival crevicular (GC) Inflammatory mediators |
| Included Studies | Methods | Periodontal Parameters Evaluated | Outcome(s) | Conclusions and Considerations |
|---|---|---|---|---|
| Author Year Journal Study design Reference […] Fundings | Participants Subjects (n.) Age (y.o.) Male/Female Smoking habit Intervention Statin type Dosing Duration Comparison No drug therapy (hyperlipidemics)/different statin (hyperlipidemics)/ No statin (normolipidemics) Procedure(s) Any | Clinical CAL PPD BoP Gingival Index (GI) Plaque Index (PI) Tooth loss Teeth n. Radiographic Bone loss Gingival crevicular (GC) Inflammatory mediators | Statistically significant (p < 0.05) | |
| Cicek Ari 2016 Inflam Case–control study [42] The study was financially supported by the Hacettepe University Scientific Research Projects Coordination Unit | Participants Subjects n. 127 Non-smokers Classified as: HL-S 20M/33F Sub-classified as: - “Ph” (n.14) Age (53.0 ± 13.08 y.o.) - G (n. 17) Age (55.47 ± 11.59 y.o.) - P” (n.22) Age (58.86 ± 6.93 y.o.) HL-D 8M/18F Sub-classified as: - Ph (n.14) Age (53.0 ± 13.08 y.o.) - G (n. 13) Age (46.08 ± 12.38 y.o.) - P (n.13) Age (53.69 ± 9.8 y.o.) NL-NS 17 M/31F Sub-classified as: - Ph (n.18) Age (27.7 ± 3.6 y.o.) - G (n. 15) Age (29.67 ± 11.5 y.o.) - P (n.15) Age (41.40 ± 8.8 y.o.) Intervention Statin type: n.a. Dosing: n.a. Duration: n.a. Comparison No drug therapy (diet)/no statin Procedure(s) - Periodontal exam - Gingival crevicular fluid (GCF) sampling and analysis for IL-1B, IL-10, MPO - Blood sampling and analysis of serum triglycerides, total cholesterol, LDL, HDL and fasting plasma glucose | Clinical CAL PPD PI GI BOP Gingival crevicular IL-1B IL-10 MPO | PPD (mm): HL-S-P (2.30 ± 0.85) < HL-D-P (2.76 ± 1.01) < NL-NS-P (3.03 ± 0.58) p = 0.012 GCF IL-1B (pg/mL): HL-S-P (72.43 ± 65.19) < NL-NS-P (90.41 ± 67.78) < HL-D-P (142.08 ± 79.82) p < 0.05 | PPD values of hyperlipidemic statin users with periodontitis were significantly lower compared to normolipidemics with periodontitis IL-1B levels of hyperlipidemic statin users with periodontitis were significantly lower compared to hyperlipidemics on diet with periodontitis Statin use decreased the IL-1B and MPO levels and enhanced IL-10 in GCF Statins may decrease periodontal inflammation and periodontitis progression |
| Fernandez 2014 J Perio Cross-sectional study [40] The study was partially funded by Research GroupCTS-583 of the Andalusian Regional Government | Participants Subjects n. 73 Classified as: HL-S-Ph/G/P (n.29) Age (63.1 ± 8.9 y.o.) 18M/11F Smokers: 10.3% HL-D-Ph/G/P (n.28) Age (52.7 ± 9.0 y.o.) 10M/8F Smokers: 21.5% NL-NS-Ph/G/P (n.16) Age (46.3 ± 10.7 y.o.) 8M/8F Smokers: 37.5% Intervention Statin type: simvastatin Dosing: n.a. Duration: 3–132 months Comparison No drug therapy (diet)/no statin Procedure(s) - Periodontal exam - Blood sampling and analysis of serum triglycerides, total cholesterol, LDL, HDL and fasting plasma glucose, C-reactive protein, erythrocyte sedimentation rate and bone metabolismmarkers (osteoprotegerin, osteocalcin, procollagen type I N-terminal propeptide and C-terminal telopeptide of type I collagen) | Clinical CAL PPD PI GI | CAL (mm): HL-S-P (2.7 ± 1.2) < NL-NS-P (3.0 ± 1.6) p = 0.05 | CAL values of hyperlipidemic statin users with periodontitis were significantly lower compared to normolipidemics with periodontitis Periodontal status was similar betweenhyperlipidemic statin users with periodontitis and normolipidemics with periodontitis, but worse in hyperlipidemics on diet with periodontitis |
| Kadhim 2019 Dental Hypothesis Cross-sectional study [37] No fundings | Participants Subjects n. 74 Age (40–69 y.o.) M/F: n.a. Smokers (40/74) Classified as: HL-S-P (n.40) HL-NS-P (n.34) NL-NS-Ph (n.30) Intervention Statin type: simvastatin (45.00%) /atorvastatin (55.00%) Dosing: n.a. Duration: > 6 months Comparison No statin Procedure(s) - Periodontal exam - Blood sampling and analysis of serum triglycerides, total cholesterol, LDL, HDL and of inflammatory biomarkers (C-reactive protein, Interleukin-6, Tumor Necrosis Factor- a, malondialdehyde) - Blood pressure measurement | Clinical Community Periodontal Index Teeth n. PI GI | Community Periodontal Index: HL-S-P < HL-NS-P p < 0.01 Teeth (n.): HL-NS-P + HL-S-P (15.73 ± 1.58) <NL-NS-Ph (22.28 ± 1.63) p = 0.001 PI: HL-S-P < HL-NS-P p < 0.01 GI: HL-S-P < HL-NS-P p < 0.01 Smokers: NL-NS-Ph (n.7) < HL-S-P + HL-NS-P (n.33) p = 0.04 | Hyperlipidemic statin users and non-users with periodontitis had higher levels of smoking status and number of residual teeth compared with normolipidemic nonperiodontal subjects Atorvastatin and simvastatin produced comparable effects in the reduction of PI, GI and Community Periodontal Index in hyperlipidemic statin users with periodontitis |
| Sangwan 2013 Eur J Dent Cross-sectional study [38] No fundings | Participants Subjects n. 140 Non-smokers Classified as: HL-S-P (n.50) Age (45.62–9.90 y.o.) 29M/21F HL-NS/D/E-P (n.44) Age (41.34–10.02 y.o.) 25M/19F NL-NS-P (n.46) Age (42.54–9.91 y.o.) 22M/24F Intervention Statin type: atorvastatin Dosing: 20 mg/die Duration: ≥ 3 months Comparison No drug therapy (diet and exercise)/no statin Procedure(s) - Periodontal exam - Blood sampling and analysis of serum triglycerides, total cholesterol, LDL and HDL levels | Clinical CAL PPD Teeth n. GI PI | CAL (mm): NL-NS-P (3.64 ± 0.86) < HL-S-P + HL-NS-P (4.12 ± 1.26) p = 0.047 PPD (mm): NL-NS-P (2.78 ± 0.53) < HL-S-P + HL-NS-P (3.24 ± 0.89) p = 0.003 Teeth n.: NL-NS-P (26.76 ± 1.58) < HL-S-P + HL-NS-P (25.18 ± 2.99) p = 0.002 PPD (mm): HL-S-P (3.00 ± 0.81) < HL-NS/D/E-P (3.52 ± 0.90) p = 0.001 GI: HL-S-P (1.44 ± 0.30) < HL-NS/D/E-P (1.59 ± 0.33) p = 0.022 | Hyperlipidemic statin users and non-users with periodontitis had higher CAL and PPD values and number of lost teeth compared with normolipidemic periodontal subjects Hyperlipidemic non-statin users with periodontitis had higher GI values compared with hyperlipidemic statin users with periodontitis and normolipidemic periodontal subjects Statins (atorvastatin) may positively affect gingival inflammation |
| Sayar 2016 Oral dis Cross-sectional study [41] No fundings | Participants Subjects n. 150 Non-smokers Classified as: HL-S-P (n.50) Age (47.10 ± 5.61 y.o.) 28M/22F HL-NS/D/E-P (n.50) Age (46.98 ± 5.79 y.o.) 21M/29F NL-NS-P (n.50) Age (45.42 ± 6.61 y.o.) 24M/26F Intervention Statin type: simvastatin Dosing: 40 mg/die Duration: ≥ 3 months Comparison No drug therapy (diet and exercise)/no statin Procedure(s) - Periodontal exam - Blood sampling and analysis of serum triglycerides, total cholesterol, LDL and HDL levels | Clinical CAL PPD BoP PI | CAL (mm). NL-NS-P (1.03 ± 0.35) < HL-S-P (1.83 ± 0.67) < HL-NS-P (2.00 ± 0.72) p = 0.0001 PPD (mm): NL-NS-P (2.24 ± 0.35)< HL-S-P (2.76 ± 0.39) < HL-NS-P (3.15 ± 0.46) p = 0.0001 PI: HL-S-P (2.32 ± 0.54) < HL-NS-P (2.67 ± 0.45) p = 0.005 | Hyperlipidemic statin users and non-users with periodontitis had higher PD and CAL values compared with normolipidemic periodontal subjects Hyperlipidemic statin users with periodontitis had lower PI values compared with hyperlipidemic non-statin users with periodontitis and normolipidemic periodontal subjects Statins (simvastatin) may exert an anti-inflammatory effect |
| Saxlin 2009 J Clin Perio Cross-sectional study [25] The study was partly supported by the Finnish Dental Association and by the Finnish Dental Society Apollonia | Participants Subjects n. 2032 Age (40–69 y.o.) 43,4M/56,5F Non-smokers Classified as: HL-S-P (n.134) Age (58,4 y.o.) 53M/47F Sub-classified as: - Simvastatin users (n.58) - Atorvastatin users (n.38) - Other statin type users (n.38) NL-NS-P (n.1898) Age (52,1 y.o.) 43M/57F Intervention Statin type: simvastatin/atorvastatin/other statin Dosing: n.a. Duration: n.a. Comparison No statin/Simvastatin/Atorvastatin/Other statin Procedure(s) - Periodontal exam | Clinical PPD (N. teeth with deepened periodontal pockets ≥ 4 mm; N. teeth with deeper periodontal pockets ≥ 6 mm) BoP Presence of Plaque | N. teeth with deepened periodontal pockets ≥ 4 mm: HL-S-P with gingival bleeding (RR 0.9, 95% CI 0.7–1.1) > NL-NS-P N. teeth with deeper periodontal pockets ≥ 6 mm: HL-S-P with gingival bleeding (RR 0.6, 95% CI 0.3–1.1) > NL-NS-P | Beneficial effect of statins was seen in hyperlipidemic statin users with periodontitis with dental plaque or gingival bleeding. Among hyperlipidemic statin users with periodontitis but no dental plaque nor gingival bleeding; statins were associated with deepened periodontal pockets Statins may have beneficial effects on the periodontium Statin effect may be dependent on the inflammatory conditions of the periodontium |
| Suresh 2013 Indian J Pharmacol Cross-sectional [39] No fundings | Participants Subjects n. 30 Age (40–60 y.o.) 16M/14F Non-smokers Classified as: HL-S-P (n.15) HL-NS-P (n.15) Intervention Statin type: atorvastatin Dosing: 20 mg/die Duration: ≥ 6 months Comparison No statin Procedure(s) - Periodontal exam - Gingival crevicular Fluid (GCF)—Sampling and analysis for IL-1B | Clinical CAL PI GI Gingival crevicular IL-1B | GCF IL-1B (pg/mL): HL-S-P (180.73 ± 32.15) < HL-NS-P(308.20 ± 27.73) p < 0.001 CAL, PI and GI: HL-S-P = HL-NS-P (selection criteria) Specifically, CAL (mm): HL-S-P (4.1) = HL-NS-P (3.9); PI: HL-S-P (2.6 ± 0.51) = HL-NS-P (2.4 ± 0.51) GI:HL-S-P (2.55 ± 0.35) = HL-NS-P (2.65) | Hyperlipidemic statin users with periodontitis had lower levels of GCF IL-1Bcompared to hyperlipidemic statin users with periodontitis and similar CAL, PI and GI values Atorvastatin may exert an anti-inflammatory effect on chronic periodontitis |
| Study | Confounding | Selection of Participants | Classification of Interventions | Deviations from Intended Interventions | Measurement of Outcomes | Missing Data | Selection of the Reported Result |
|---|---|---|---|---|---|---|---|
| Cicek Ari, 2016 | Unclear | Low | Low | Low | High | Low | Low |
| Fernandez, 2014 | Unclear | Low | Low | Low | High | Unclear | Unclear |
| Kadhim, 2019 | Unclear | Low | Low | Low | High | Unclear | Unclear |
| Sangwan, 2013 | Unclear | Low | Low | Low | High | Low | Low |
| Sayar, 2016 | Unclear | Low | Low | Low | High | Low | Low |
| Saxlin, 2009 | Unclear | Low | Low | Low | High | Low | Low |
| Suresh, 2013 | Unclear | Low | Low | Low | High | Unclear | Unclear |
| Periodontal Parameter(s) | Author, Year | Study Design | Main Result(s) |
|---|---|---|---|
| CAL | Cicek Ari, 2016 | Case–control | CAL values were lower in statin users but did not reach statistically significant difference between statin and non-statin users |
| Fernandez, 2014 | Cross-sectional study | CAL values were lower in statin users compared to non-statin users | |
| Sangwan, 2013 | Cross-sectional study | CAL values were similar between statin and no statin users | |
| Sayar, 2016 | Cross-sectional study | CAL values were higher in non-statin compared to statin users | |
| Suresh, 2013 | Cross-sectional study | CAL values were similar in statin and non-statin users | |
| PPD | Cicek Ari, 2016 | Case/control | PPD values were lower in statin users compared to normolipidemic non-statin users |
| Sangwan, 2013 | Cross-sectional study | PPD values were lower in statin compared to hyperlipidemic non-statin users | |
| Sayar, 2016 | Cross-sectional study | PPD values were lower in statin compared to non-statin users | |
| BoP | Cicek Ari, 2016 | Case/control | BoP values were lower in statin compared to non-statin users |
| Saxlin, 2009 | Cross-sectional study | BoP values were higher in statin compared to non-statin users | |
| Sayar, 2016 | Cross-sectional study | BoP values were similar in statin compared to non-statin users | |
| GI | Cicek Ari, 2016 | Case–control | Statins use did not improve GI |
| Kadhim, 2019 | Cross-sectional study | GI values were lower in statin compared to non-statin users | |
| Suresh, 2013 | Cross-sectional study | CAL values were similar in statin and non-statin users | |
| PI | Kadhim, 2019 | Cross-sectional study | PI values were lower in statin compared to non-statin users |
| Sangwan, 2013 | Cross-sectional study | PI values were similar in statin and non-statin users | |
| Sayar, 2016 | Cross-sectional study | PI values were lower in statin compared to non-statin users | |
| Suresh, 2013 | Cross-sectional study | PI values were similar in statin and non-statin users | |
| Tooth loss | Saxlin, 2009 | Cross-sectional study | Statin use was associated with decreased tooth loss among subjects with chronic periodontitis |
| Residual teeth | Sangwan, 2013 | Cross-sectional study | The number of residual teeth was negatively associated with TGs |
| IL-1B (crevicular) | Cicek Ari, 2016 | Case–control | GCF IL-1b levels were lower in statin compared to non-statin users |
| Suresh, 2013 | Cross-sectional study | GCF IL-1B levels were lower in statin compared to non-statin users | |
| IL-10 (crevicular) | Cicek Ari, 2016 | Case–control | GCF IL-10 levels were higher in statin compared to non-statin users |
| MPO (crevicular) | Cicek Ari, 2016 | Case–control | GCF MPO were lower in statin compared to non-statin users |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Spirito, F.; Schiavo, L.; Pilone, V.; Lanza, A.; Sbordone, L.; D’Ambrosio, F. Periodontal and Peri-Implant Diseases and Systemically Administered Statins: A Systematic Review. Dent. J. 2021, 9, 100. https://doi.org/10.3390/dj9090100
Di Spirito F, Schiavo L, Pilone V, Lanza A, Sbordone L, D’Ambrosio F. Periodontal and Peri-Implant Diseases and Systemically Administered Statins: A Systematic Review. Dentistry Journal. 2021; 9(9):100. https://doi.org/10.3390/dj9090100
Chicago/Turabian StyleDi Spirito, Federica, Luigi Schiavo, Vincenzo Pilone, Antonio Lanza, Ludovico Sbordone, and Francesco D’Ambrosio. 2021. "Periodontal and Peri-Implant Diseases and Systemically Administered Statins: A Systematic Review" Dentistry Journal 9, no. 9: 100. https://doi.org/10.3390/dj9090100
APA StyleDi Spirito, F., Schiavo, L., Pilone, V., Lanza, A., Sbordone, L., & D’Ambrosio, F. (2021). Periodontal and Peri-Implant Diseases and Systemically Administered Statins: A Systematic Review. Dentistry Journal, 9(9), 100. https://doi.org/10.3390/dj9090100