
Success Rates and Complications Associated with Single Immediate Implants: A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
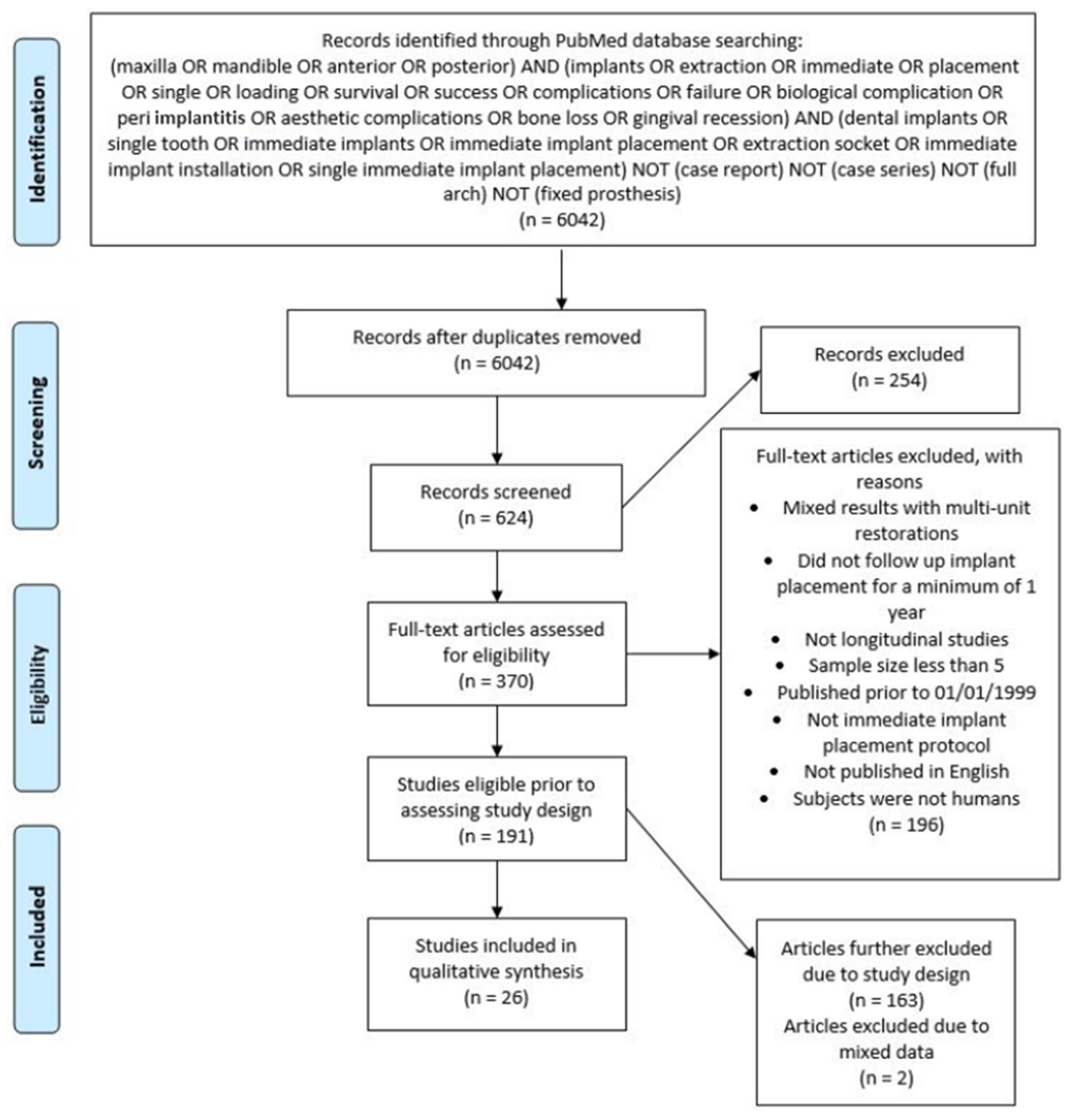
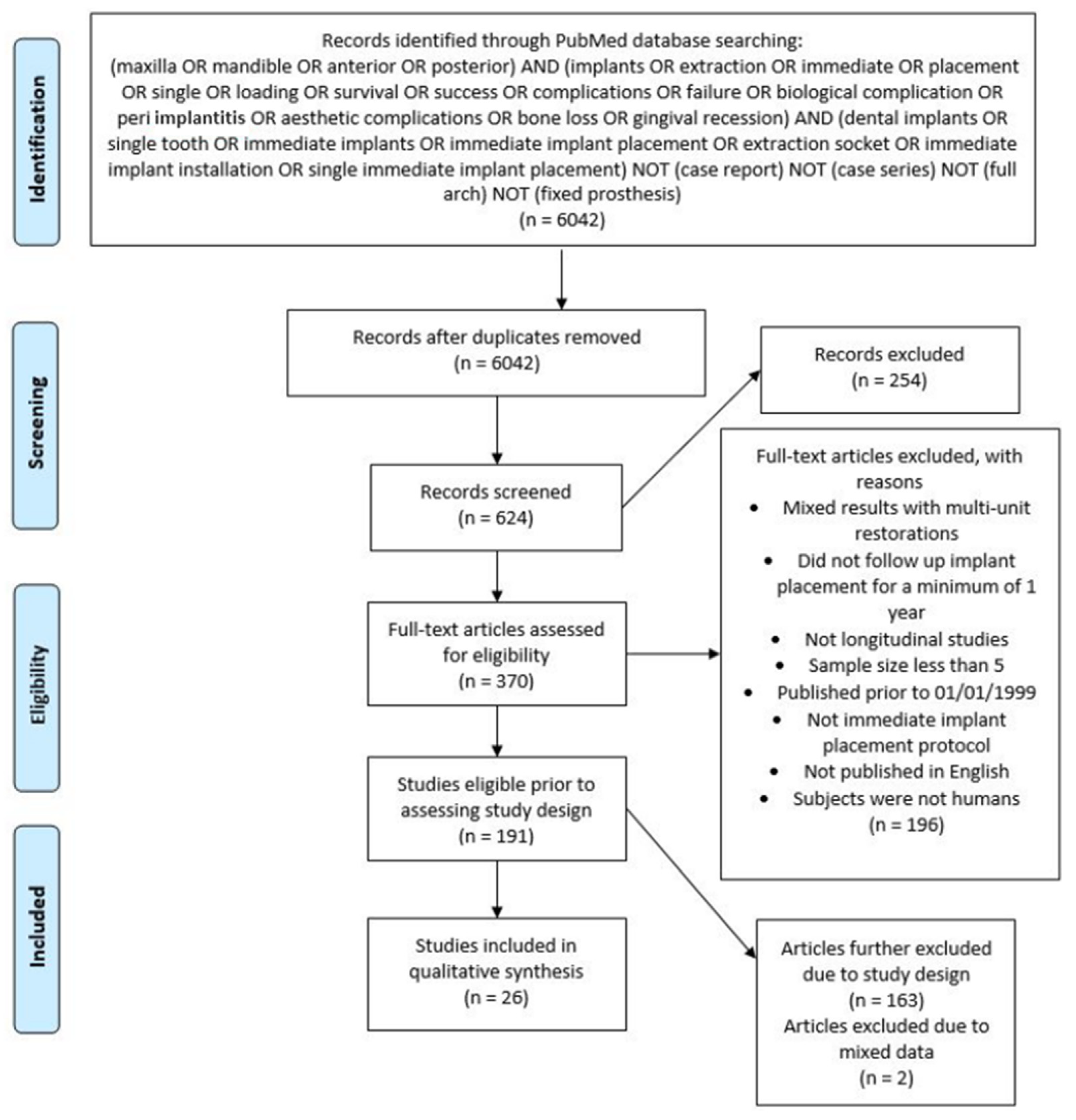
2.1. Search Strategy
2.2. Focused Question
- Pink Esthetic Score (PES): Where the score was based on seven parameters: mesial papilla, distal papilla, soft tissue level, soft tissue contour, alveolar process deficiency, soft tissue color, and texture. Each parameter was assessed with a 2–1–0 score, with 2 being the best and 0 being the worst result. A maximum score of 14 can be achieved [20].
- Papilla Index Score (PIS): This includes index-0 means no papilla present, index-1 means less than one half the papilla height is present and a convex nature of the adjacent tissue nature is noted, index-2 means greater than half the height of the papilla is present although not to the full extent of the contact point, papilla is not in complete harmony, index-3 means the papilla fills the entire proximal space and is in good harmony, and finally, index-4 means the papilla is hyperplastic [21].
- Midfacial gingival level: Which can be measured as the most apical portion of the midfacial peri-implant mucosa. Change over time/recession is determined by comparing to a baseline measurement (pre-operatively or to an untreated adjacent tooth).
- White Esthetic Score (WES): Where the score includes five variables: Tooth form, tooth volume, tooth color including the assessment of hue and value, tooth texture, and translucency. Each parameter is assessed with a 0–1–2 score with 2 being the best and 0 being the worst score. A maximum score of 10 can be reached [22].
- Implant Crown Aesthetic Index (ICAI): Is an index based off nine variables where penalty points are assigned if not matching to the desired situation: one penalty point for minor (slight) deviations and five penalty points for major (gross) deviations. Zero penalty points means excellent; one or two points means satisfactory; three or four points means moderate; five or more points means poor aesthetics. The nine categories are: mesiodistal dimension of the crown, position of the incisal edge of the crown, labial convexity of the crown, color and translucency of the crown, surface of the crown, position of the labial margin of the peri-implant mucosa, position of mucosa in the proximal embrasures, contour of the labial surface of the mucosa, color and surface of the labial mucosa [23].
2.3. Eligibility Criteria
- Publications between January 1999 and January 2021.
- Randomized controlled trials of immediate single implants.
- Sample size of no less than six human subjects.
- Minimum follow up period of one year.
- Studies published in English.
2.4. Study Selection
2.5. Data Extraction
2.6. Risk of Bias Assessment
3. Results
3.1. Risk of Bias within and across Studies
3.2. Study Characteristics
3.3. Success Rates
3.4. Biological Complications
3.5. Hardware Complications
3.6. Technical Complications
3.7. Mechanical Complications
3.8. Aesthetic Complications
3.9. Clinical Aesthetic Outcome (PES/WES/ICAI)
3.10. Midfacial Gingival Change
3.11. Papillary Height
3.12. Patient Satisfaction
4. Discussion
4.1. Success
4.2. Biological Complications
4.3. Hardware Complications
4.4. Aesthetics Complications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brånemark, P.-I.; Breine, U.; Adell, R.; Hansson, B.; Lindström, J.; Ohlsson, Å. Intra-osseous anchorage of dental prostheses: I. Experimental studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar] [CrossRef] [PubMed]
- Cosyn, J.; De Lat, L.; Seyssens, L.; Doornewaard, R.; Deschepper, E.; Vervaeke, S. The effectiveness of immediate implant placement for single tooth replacement compared to delayed implant placement: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 224–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, M.; Grusovin, M.G.; Polyzos, I.P.; Felice, P.; Worthington, H.V. Timing of implant placement after tooth extraction: Immediate, immediate-delayed or delayed implants? A Cochrane systematic review. Eur. J. Oral Implant. 2010, 3, 189–205. [Google Scholar]
- Schulte, W.; Kleineikenscheidt, H.; Lindner, K.; Schareyka, R. The Tübingen immediate implant in clinical studies. Dtsch. Zahnarztl. Z. 1978, 33, 348–359. [Google Scholar]
- Chen, J.; Cai, M.; Yang, J.; Aldhohrah, T.; Wang, Y. Immediate versus early or conventional loading dental implants with fixed prostheses: A systematic review and meta-analysis of randomized controlled clinical trials. J. Prosthet. Dent. 2019, 122, 516–536. [Google Scholar] [CrossRef] [Green Version]
- Ebenezer, V.; Balakrishnan, R. Immediate Vs Delayed Implants: Comparative study of 100 cases. Biomed. Pharmacol. J. 2015, 8, 375–378. [Google Scholar] [CrossRef]
- Huynh-Ba, G.; Oates, T.W.; Williams, M.A. Immediate loading vs. early/conventional loading of immediately placed implants in partially edentulous patients from the patients’ perspective: A systematic review. Clin. Oral Implant. Res. 2018, 29, 255–269. [Google Scholar] [CrossRef] [Green Version]
- Haas, R.; Grzadziel, A.; Millesi, W.; Fürhauser, R.; Mailath-Pokorny, G.; Busenlechner, D.; Pommer, B. Immediate vs. delayed implant placement in the esthetic zone-10-year survival and bone level analysis. Clin. Oral Implant. Res. 2018, 29, 95. [Google Scholar] [CrossRef] [Green Version]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant Success, Survival, and Failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Carr, A.; Wolfaardt, J.; Garrett, N. Capturing patient benefits of treatment. Int. J. Oral Maxillofac. Implant. 2011, 26, 85–92. [Google Scholar]
- Ortega-Martinez, J.; Perez-Pascual, T.; Mareque-Bueno, S.; Hernandez-Alfaro, F.; Ferrés-Padró, E. Immediate implants following tooth extraction. A systematic review. Medicina Oral Patología Oral Cirugia Bucal 2012, 17, e251–e261. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.; Palmer, R. Periodontology* WGotVEWo. Clinical research in implant dentistry: Study design, reporting and outcome measurements: Consensus report of W orking G roup 2 of the VIII E uropean W orkshop on P eriodontology. J. Clin. Periodontol. 2012, 39, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Pun, L.; Lau, K.Y.; Li, K.Y.; Wong, M.C. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin. Oral Implant. Res. 2011, 23, 39–66. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, P.W. Popping the (PICO) question in research and evidence-based practice. Appl. Nurs. Res. 2002, 15, 197–198. [Google Scholar] [CrossRef] [PubMed]
- Hämmerle, C.H.F.; Chen, S.T.; Wilson, T.G., Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int. J. Oral Maxillofac. Implant. 2004, 19, 26–28. [Google Scholar]
- Bragger, U.; Heitz-Mayfield, L. ITI Treatment Guide Volume 8: Biological and Hardware Complications in Implant Dentistry; Quintessence Pub.: Batavia, IL, USA, 2015. [Google Scholar]
- Zitzmann, N.U.; Berglundh, T. Definition and prevalence of peri-implant diseases. J. Clin. Periodontol. 2008, 35, 286–291. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45, S1–S8. [Google Scholar] [CrossRef]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin. Oral Implant. Res. 2005, 16, 639–644. [Google Scholar] [CrossRef]
- Jemt, T. Regeneration of gingival papillae after single-implant treatment. Int. J. Periodontics Restor. Dent. 1997, 17, 326–333. [Google Scholar]
- Belser, U.C.; Grütter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.-P.; Buser, D. Outcome Evaluation of Early Placed Maxillary Anterior Single-Tooth Implants Using Objective Esthetic Criteria: A Cross-Sectional, Retrospective Study in 45 Patients With a 2- to 4-Year Follow-Up Using Pink and White Esthetic Scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Meijer, H.J.A.; Stellingsma, K.; Meijndert, L.; Raghoebar, G.M. A new index for rating aesthetics of implant-supported single crowns and adjacent soft tissues—The Implant Crown Aesthetic Index. Clin. Oral Implant. Res. 2005, 16, 645–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Altman, D.G. Assessing Risk of Bias in Included Studies. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2008; pp. 187–241. [Google Scholar]
- Canullo, L.; Caneva, M.; Tallarico, M. Ten-year hard and soft tissue results of a pilot double-blinded randomized controlled trial on immediately loaded post-extractive implants using platform-switching concept. Clin. Oral Implant. Res. 2017, 28, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Goglia, G.; Iurlaro, G.; Iannello, G. Short-term bone level observations associated with platform switching in immediately placed and restored single maxillary implants: A preliminary report. Int. J. Prosthodont. 2009, 22, 277–282. [Google Scholar]
- Crespi, R.; Capparé, P.; Gherlone, E. A 4-Year Evaluation of the Peri-Implant Parameters of Immediately Loaded Implants Placed in Fresh Extraction Sockets. J. Periodontol. 2010, 81, 1629–1634. [Google Scholar] [CrossRef] [Green Version]
- De Rouck, T.; Collys, K.; Wyn, I.; Cosyn, J. Instant provisionalization of immediate single-tooth implants is essential to optimize esthetic treatment outcome. Clin. Oral Implant. Res. 2009, 20, 566–570. [Google Scholar] [CrossRef]
- Koh, R.U.; Oh, T.-J.; Rudek, I.; Neiva, G.F.; Misch, C.E.; Rothman, E.D.; Wang, H.-L. Hard and Soft Tissue Changes after Crestal and Subcrestal Immediate Implant Placement. J. Periodontol. 2011, 82, 1112–1120. [Google Scholar] [CrossRef] [Green Version]
- Palattella, P.; Torsello, F.; Cordaro, L. Two-year prospective clinical comparison of immediate replacement vs. immediate restoration of single tooth in the esthetic zone. Clin. Oral Implant. Res. 2008, 19, 1148–1153. [Google Scholar] [CrossRef]
- Pieri, F.; Aldini, N.N.; Marchetti, C.; Corinaldesi, G. Influence of implant-abutment interface design on bone and soft tissue levels around immediately placed and restored single-tooth implants: A randomized controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2011, 26, 169. [Google Scholar]
- Prosper, L.; Gherlone, E.; Redaelli, S.; Quaranta, M. Four-year follow-up of larger-diameter implants placed in fresh extraction sockets using a resorbable membrane or a resorbable alloplastic material. Int. J. Oral Maxillofac. Implant. 2003, 18, 856. [Google Scholar]
- Shibly, O.; Kutkut, A.; Patel, N.; Albandar, J.M. Immediate Implants with Immediate Loading vs. Conventional Loading: 1-Year Randomized Clinical Trial. Clin. Implant Dent. Relat. Res. 2012, 14, 663–671. [Google Scholar] [CrossRef]
- Slagter, K.W.; Meijer, H.J.; Bakker, N.A.; Vissink, A.; Raghoebar, G.M. Feasibility of immediate placement of single-tooth implants in the aesthetic zone: A 1-year randomized controlled trial. J. Clin. Periodontol. 2015, 42, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Van Nimwegen, W.G.; Raghoebar, G.M.; Zuiderveld, E.G.; Jung, R.E.; Meijer, H.J.A.; Muehlemann, S. Immediate placement and provisionalization of implants in the aesthetic zone with or without a connective tissue graft: A 1-year randomized controlled trial and volumetric study. Clin. Oral Implant. Res. 2018, 29, 671–678. [Google Scholar] [CrossRef]
- Yoshino, S.; Kan, J.Y.K.; Rungcharassaeng, K.; Roe, P.; Lozada, J.L. Effects of Connective Tissue Grafting on the Facial Gingival Level Following Single Immediate Implant Placement and Provisionalization in the Esthetic Zone: A 1-Year Randomized Controlled Prospective Study. Int. J. Oral Maxillofac. Implant. 2014, 29, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Zuiderveld, E.G.; Meijer, H.J.A.; Hartog, L.D.; Vissink, A.; Raghoebar, G.M. Effect of connective tissue grafting on peri-implant tissue in single immediate implant sites: A RCT. J. Clin. Periodontol. 2018, 45, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Bignozzi, I.; Cocchetto, R.; Cristalli, M.P.; Iannello, G. Immediate positioning of a definitive abutment versus repeated abutment replacements in post-extractive implants: 3-year follow-up of a randomised multicentre clinical trial. Eur. J. Oral Implant. 2010, 3, 285. [Google Scholar]
- Cecchinato, D.; Lops, D.; Salvi, G.E.; Sanz, M. A prospective, randomized, controlled study using OsseoSpeed™ implants placed in maxillary fresh extraction socket: Soft tissues response. Clin. Oral Implant. Res. 2015, 26, 20–27. [Google Scholar] [CrossRef]
- Cordaro, L.; Torsello, F.; Roccuzzo, M. Clinical outcome of submerged vs. non-submerged implants placed in fresh extraction sockets. Clin. Oral Implant. Res. 2009, 20, 1307–1313. [Google Scholar] [CrossRef]
- Cucchi, A.; Vignudelli, E.; Franco, S.; Levrini, L.; Castellani, D.; Pagliani, L.; Rea, M.; Modena, C.; Sandri, G.; Longhi, C. Tapered, Double-Lead Threads Single Implants Placed in Fresh Extraction Sockets and Healed Sites of the Posterior Jaws: A Multicenter Randomized Controlled Trial with 1 to 3 Years of Follow-Up. BioMed Res. Int. 2017, 2017, 8017175. [Google Scholar] [CrossRef] [Green Version]
- De Angelis, N.; Felice, P.; Pellegrino, G.; Camurati, A.; Gambino, P.; Esposito, M. Guided bone regeneration with and without a bone substitute at single post-extractive implants: 1-year post-loading results from a pragmatic multicentre randomised controlled trial. Eur. J. Oral Implantol. 2011, 4, 313. [Google Scholar]
- Degidi, M.; Nardi, D.; Daprile, G.; Piattelli, A. Nonremoval of Immediate Abutments in Cases Involving Subcrestally Placed Postextractive Tapered Single Implants: A Randomized Controlled Clinical Study. Clin. Implant Dent. Relat. Res. 2013, 16, 794–805. [Google Scholar] [CrossRef]
- Esposito, M.; Barausse, C.; Pistilli, R.; Jacotti, M.; Grandi, G.; Tuco, L.; Felice, P. Immediate loading of post-extractive versus delayed placed single implants in the anterior maxilla: Outcome of a pragmatic multicenter randomised controlled trial 1-year after loading. Eur. J. Oral Implant. 2015, 8, 347. [Google Scholar]
- Felice, P.; Pistilli, R.; Barausse, C.; Trullenque-Eriksson, A.; Esposito, M. Immediate non-occlusal loading of immediate post-extractive versus delayed placement of single implants in preserved sockets of the anterior maxilla: 1-year post-loading outcome of a randomised controlled trial. Eur. J. Oral Implant. 2015, 8, 361. [Google Scholar]
- Grandi, T.; Guazzi, P.; Samarani, R.; Maghaireh, H.; Grandi, G. One abutment-one time versus a provisional abutment in immediately loaded post-extractive single implants: A 1-year follow-up of a multicentre randomised controlled trial. Eur. J. Oral Implant. 2014, 7, 141. [Google Scholar]
- Tallarico, M.; Xhanari, E.; Pisano, M.; De Riu, G.; Tullio, A.; Meloni, S.M. Single post-extractive ultra-wide 7 mm-diameter implants versus implants placed in molar healed sites after socket preservation for molar replacement: 6-month post-loading results from a randomised controlled trial. Eur. J. Oral Implant. 2016, 9, 263. [Google Scholar]
- Tallarico, M.; Xhanari, E.; Pisano, M.; Gatti, F.; Meloni, S.M. Molar replacement with 7 mm-wide diameter implants: To place the implant immediately or to wait 4 months after socket preservation? 1 year after loading results from a randomised controlled trial. Eur. J. Oral Implant. 2017, 10, 169. [Google Scholar]
- Block, M.S.D.M.D.; Mercante, D.E.P.; Lirette, D.B.S.R.D.H.; Mohamed, W.D.D.S.M.D.; Ryser, M.D.M.D.M.D.; Castellon, P.D.D.S. Prospective Evaluation of Immediate and Delayed Provisional Single Tooth Restorations. J. Oral Maxillofac. Surg. 2009, 67, 89–107. [Google Scholar] [CrossRef]
- Migliorati, M.; Amorfini, L.; Signori, A.; Biavati, A.S.; Benedicenti, S. Clinical and Aesthetic Outcome with Post-Extractive Implants with or without Soft Tissue Augmentation: A 2-Year Randomized Clinical Trial. Clin. Implant Dent. Relat. Res. 2013, 17, 983–995. [Google Scholar] [CrossRef]
- Urban, T.; Kostopoulos, L.; Wenzel, A. Immediate implant placement in molar regions: A 12-month prospective, randomized follow-up study. Clin. Oral Implant. Res. 2011, 23, 1389–1397. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implant. 1986, 1, 11–25. [Google Scholar]
- Smith, D.E.; Zarb, G.A. Criteria for success of osseointegrated endosseous implants. J. Prosthet. Dent. 1989, 62, 567–572. [Google Scholar] [CrossRef]
- Roos-Jansåker, A.M.; Lindahl, C.; Renvert, H.; Renvert, S. Nine-to fourteen-year follow-up of implant treatment. Part II: Presence of peri-implant lesions. J. Clin. Periodontol. 2006, 33, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Fransson, C.; Wennström, J.; Berglundh, T. Clinical characteristics at implants with a history of progressive bone loss. Clin. Oral Implant. Res. 2008, 19, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-T.; Huang, Y.-W.; Zhu, L.; Weltman, R. Prevalences of peri-implantitis and peri-implant mucositis: Systematic review and meta-analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Salvi, G.; Brägger, U. Mechanical and Technical Risks in Implant Therapy. Int. J. Oral Maxillofac. Implant. 2009, 24, 69–85. [Google Scholar]
- Papaspyridakos, P.; Chen, C.-J.; Chuang, S.-K.; Weber, H.-P.; Gallucci, G.O. A systematic review of biologic and technical complications with fixed implant rehabilitations for edentulous patients. Int. J. Oral Maxillofac. Implant. 2012, 27, 102–110. [Google Scholar]
- Zembic, A.; Kim, S.; Zwahlen, M.; Kelly, J.R. Systematic review of the survival rate and incidence of biologic, technical, and esthetic complications of single implant abutments supporting fixed prostheses. Int. J. Oral Maxillofac. Implant. 2014, 29, 99–116. [Google Scholar] [CrossRef] [Green Version]
- Zurdo, J.; Romão, C.; Wennström, J.L. Survival and complication rates of implant-supported fixed partial dentures with cantilevers: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. S4), 59–66. [Google Scholar] [CrossRef]
- Cosyn, J.; Eghbali, A.; De Bruyn, H.; Collys, K.; Cleymaet, R.; De Rouck, T. Immediate single-tooth implants in the anterior maxilla: 3-year results of a case series on hard and soft tissue response and aesthetics. J. Clin. Periodontol. 2011, 38, 746–753. [Google Scholar] [CrossRef]
- Guarnieri, R.; Placella, R.; Testarelli, L.; Iorio-Siciliano, V.; Grande, M. Clinical, radiographic, and esthetic evaluation of immediately loaded laser microtextured implants placed into fresh extraction sockets in the anterior maxilla: A 2-year retrospective multicentric study. Implant Dent. 2014, 23, 144. [Google Scholar] [CrossRef]
- Mangano, F.; Mangano, C.; Ricci, M.; Sammons, R.L.; Shibli, J.A.; Piattelli, A. Single-tooth Morse taper connection implants placed in fresh extraction sockets of the anterior maxilla: An aesthetic evaluation. Clin. Oral Implant. Res. 2011, 23, 1302–1307. [Google Scholar] [CrossRef] [PubMed]
- Raes, F.; Cosyn, J.; De Bruyn, H. Clinical, Aesthetic, and Patient-Related Outcome of Immediately Loaded Single Implants in the Anterior Maxilla: A Prospective Study in Extraction Sockets, Healed Ridges, and Grafted Sites. Clin. Implant Dent. Relat. Res. 2012, 15, 819–835. [Google Scholar] [CrossRef] [PubMed]
- Arora, H.; Ivanovski, S. Evaluation of the influence of implant placement timing on the esthetic outcomes of single tooth implant treatment in the anterior maxilla: A retrospective study. J. Esthet. Restor. Dent. 2018, 30, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, R.; Belleggia, F.; Grande, M. Immediate versus Delayed Treatment in the Anterior Maxilla Using Single Implants with a Laser-Microtextured Collar: 3-Year Results of a Case Series on Hard- and Soft-Tissue Response and Esthetics. J. Prosthodont. 2015, 25, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Mangano, C.; Ricci, M.; Sammons, R.L.; Shibli, J.A.; Piattelli, A. Esthetic Evaluation of Single-Tooth Morse Taper Connection Implants Placed in Fresh Extraction Sockets or Healed Sites. J. Oral Implant. 2013, 39, 172–181. [Google Scholar] [CrossRef]
- Kan, J.Y.K.; Rungcharassaeng, K.; Lozada, J.L.; Zimmerman, G. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: A 2- to 8-year follow-up. Int. J. Oral Maxillofac. Implant. 2011, 26, 179–187. [Google Scholar]

{kind=link}
| Author, Year | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias |
|---|---|---|---|---|---|---|---|
| Block et al. 2009 |  | | | | | | |
| Cannizzaro et al. 2010 | | | | | | |  |
| Canullo et al. 2009/2016 | | | | | | | |
| Canullo et al. 2010 | |  | | | | | |
| Cecchinato et al. 2015 | | | | | | | |
| Cordaro et al. 2009 | | | | | | | |
| Crespi et al. 2008 | | | | | | | |
| Cucchi et al. 2017 | | | | | | | |
| De Angelis et al. 2011 | | | | | | | |
| De Rouck et al. 2009 | | | | | | | |
| Degidi et al. 2014 | | | | | | | |
| Esposito et al. 2015 | | | | | | | |
| Felice et al. 2015 | | | | | | | |
| Grandi et al. 2014 | | | | | | | |
| Koh et al. 2011 | | | | | | | |
| Migliorati et al. 2013 | | | | | | | |
| Nimwegen et al. 2018 | | | | | | | |
| Palatella et al. 2008 | | | | | | | |
| Pieri et al. 2011 | | | | | | | |
| Prosper et al. 2003 | | | | | | | |
| Shibly, Kutkut and Patel 2010 | | | | | | | |
| Slagter et al. 2015 | | | | | | | |
| Tallarico et al. 2016 | | | | | | | |
| Urban et al. 2011 | | | | | | | |
| Yoshino et al. 2014 | | | | | | | |
| Zuiderveld et al. 2018 | | | | | | | |
= Low Risk
= Unclear Risk
= High Risk.| Author and Year | Country | Setting | Population | Intervention | Follow Up (Months) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Number of Patients and Implants | Male: Female | Mean Age and Range in Years | Region | Reason for Extraction | |||||
| Block et al., 2009 | USA | - | 55/55 | - | - | 15–25 | PD + NPD | Immediate Implant | 18–24 |
| Canullo et al., 2010 | Italy | Mc, 3 PP | 25/25 | 16:9 | Provisional = 51 Definitive = 55 | 15, 14, 24, 25 | NPD | Immediate Implant | 36 |
| Canullo et al., 2009/2016 | Italy | Mc, 2 PP | 22/22 imp platform is 5.5 mm (11 with 3.8 abutment-test and 11 with 5.5 abutment-control) At 10 years, 19/19 | 13:9 | 50, 32–76 | 15–25 | - | Immediate Implant | 300/120 |
| Cecchinato et al., 2015 | Italy | MC | 93/93 | 48:45:00 | 51 (19–80) | 15–25 | PD + NPD | Immediate Implant | 36 |
| Cordaro et al., 2009 | Italy | PP | 30/30 | - | 18–70 | 15–25, 33–35, 43–45 | NPD | Immediate Implant | 0, 1.5, 3, 6, 12, 18 |
| Crespi et al., 2008 | Italy | U | 40/40 = (A = 20 and D = 20) | 16:24 A 6:14 D 10:10 | 47, 24–68 | PD + NPD | Immediate Implant | 24 | |
| Cucchi et al., 2017 | Italy | Mc | 92/97 | 43:49:00 | 51.0 (20–79) | Premolars and Molars | PD + NPD | Immediate Implant | 12–36 |
| De Angelis et al., 2011 | Italy | Mc (4), PP | 80/80 | 38:42:00 | 47.05 | All regions | - | Immediate Implant | 12 |
| De Rouck et al., 2009 | Belgium | U | 49/49 = (A = 24 and D = 25) | A 11:13 D 12:13 | A: 55(13) D: 52(12) | 15–25 | PD + NPD | Immediate Implant | 12 |
| Degidi et al., 2014 | Italy | PP | 53/53 | - | 43.9 year | 13–23 | PD + NPD | Immediate Implant | 24 |
| Esposito et al., 2015 | Italy | Mc (3) PP | 106/106 (54 Type A, D; 52 E, F, placed at 4 months) | 22:32 (A, D) 24:28 (E, F) | 48 (28–70) for A, D 50 (30–72) for E, F | 15–25 | - | Immediate Implant | 12 |
| Felice et al., 2015 | Italy | (4) PP | 48/48 (25 A, D; 25 E, F; 2 dropped out at review both from E/F already removed from number^) | 12:13 (A, D) 13:12 (E, F) | 51.32 (32–71) for A, D 53.08 (39–72) for E, F | 15–25 | - | Immediate Implant | 4, 12 |
| Grandi et al., 2014 | Italy | Mc | 25/25 | 9:16 | 56.54 year (39–74 year) | 15–25 | PD + NPD? | Immediate Implant | 12 |
| Koh et al., 2011 | USA | U | 20/20 | 12:8 | 21–73 | 15–25 | NPD | Immediate Implant | 12 |
| Migliorati et al., 2013 | Italy | - | 48/48 | 23:25 | 47.5 (range 22–70) | 14–24 | NPD | Immediate Implant | 0, 0.5 (crown insertions), 12, 24 |
| Palattella et al., 2008 | Italy | U | 16/18 = (A = 9 and C = 9) | 6:10 | 35 | 13–23 | PD + NPD | Immediate Implant | 24 |
| Pieri et al., 2011 | Italy | U | 38/38 M = 20 and C = 20 | 15:25 M- 7:13 C- 8:12 | 45, 26–67 | 15,14, 24,25 | PD + NPD | Immediate Implant | 12 |
| Prosper et al., 2003 | Italy | U | 71/120 (60 A; 60 D) (Single crown restorations) | 35:36:00 | 58.3 (range 26–72) | 16–17, 26–27, 36–37, 46–47 | PD, NPD | Immediate Implant | 3, 6, 9, 12, 24, 26, 48 |
| Shibly et al., 2010 | USA | U | 60/60 (55 at 1-year) | 25:35:00 | 25–94 | 18—Max posterior 18—max anterior 18—mnd posterior 1—mnd anterior | PD | Immediate Implant | 3, 6, 12 |
| Slagter et al., 2015 | Netherlands | U | 40/40 | 13:27 | A: 39.4 (19–70) D: 42.3 (22–66) | 14–24 | Group A: 39.4 year (19–70 year) Group D: 42.3 year (23–66 year) | Immediate Implant | 12 |
| Tallarico et al., 2016 | Italy | PP | 24/24 | 8:16 | 53.9 (37–67) | Molar region of maxilla or mandible | 53.9 (37–67) | Immediate Implant | 12 |
| Tallarico et al., 2017 | Italy | PP | 24/24 | 8:16 | 37–67 | Maxillary and mandibular molars | 37–67 | Immediate Implant | 12 |
| Urban et al., 2011 | Denmark | - | 92/92 (76 at follow up) | 48:44:00 | 50 (23–77) | Molar region of Mnd and Mx | 50 years (range 23–77 years) | Immediate Implant | 12 |
| Van Nimwegen et al., 2018 | Netherlands | U | 60/60 | 28:32:00 | 46.6 (19.5–82.2) | 14–24 | 46.6 year (19.5–82.2 year) | Immediate Implant | 12 |
| Yoshino et al., 2014 | USA | U | 20/20 (10 vs. 10) | 7:13 | 52.6 (27–87) | 15–25 | 52.6, 27–87 | Immediate Implant | 12 |
| Zuiderveld et al., 2018 | Netherlands | U | 60/60 | 28:32:00 | 46.7 (19.5–82.2) | 14–24 | 46.7 year (19.5–82.2) | Immediate Implant | 12 |
| Reference | Comparison | Outcomes | ||||
|---|---|---|---|---|---|---|
| Success Criteria | Success Rate | Aesthetic Complications | Technical Complications | Biological Complications | ||
| Block et al., 2009 | A vs. E, A = 26 and E = 29 | - | - | |||
| Canullo et al., 2010 | A* (provisional abutment vs. definitive abutment), Provisional = 10, Definitive = 15 | Self-Defined success criteria: if implant remained in function and not need to be substituted | 100% | - | - | - |
| Canullo et al., 2009/2016 | A* (Platform switching vs. standard restoration), Platform switching = 11, Standard = 11 | - | - | - | ||
| Cecchinato et al., 2015 | D vs. D (cylindrical vs. conical/cylindrical implant), Cylindrical = 45, Conical/cylindrical = 48 | 40/164 (24.4%) of all sites has a PIS of 0 or 1 17 mesial papilla and 23 distal papilla | - | - | ||
| Cordaro et al., 2009 | D (submerged vs. non-submerged), submerged = 14, non-submerged = 16 | - | - | - | ||
| Crespi et al., 2008 | A (IL) vs. D (IL), A = 20, D = 20 | - | 4 occlusal screws became unscrewed in the provisional plastic abutments | - | ||
| Cucchi et al., 2017 | D, F D = 48, F = 44 | Albrektsson et al. (1986) criteria | 100% | - | - | - |
| De Angelis et al., 2011 | D, GBR n = 80 GBR = 40, GBR + BS = 40 | - | For the GBR group: 1 incidence of loosening of the cover screw at 4-6 weeks postoperatively, as well as decementation of the final crown of an implant in position 25. For the GBR + BS (Bone substitute): 1 incidence Loosening of the provisional abutment (position 26), 1 incidence of loosening of the cover screw at 4/6 weeks post-operatively (position 36) | 1 case of a small lesion in the peri-implant mucosa of tooth 25. 1 case of peri-implant mucositis on tooth 36. | ||
| De Rouck et al., 2009 | A vs. D A = 24, D = 25 | - | - | - | ||
| Degidi et al., 2014 | A (non removal of abutments vs. standard removal protocol) Test = 24 Control = 29 | - | - | 1 case of edema at surgery site with loss of thermal sensitivity in the 3-3 region. | ||
| Esposito et al., 2015 | A, D vs. E, F (both socket preservation), GBR | - | The complications in A,D were partial fracture of the provisional crown (four patients); loosening of the provisional crowns (two patients) | - | ||
| Felice et al., 2015 | A, D vs. E, F, GBR A + D = 54 E + F = 52 | - | Loosening of the provisional 1 crown 3 months after loading for A,D. Loosening of provisional crown in 2 patients, 1 and 3 months after loading for E + F. | - | ||
| Grandi et al., 2014 | A* (definitive abutment vs. provisional abutment) DA = 12, PA = 13 | - | One patient in the PA group had an abutment screw loosening 3 weeks after healing. 4 patients in the DA group had excess cement that had to be removed prior to final crown cementation | 1 case of peri-implant mucositis in the 5-5 region. | ||
| Koh et al., 2011 | D n = 24 | Misch et al. (2008)—ICOI Pisa Consensus Conference Criteria Self-Defined success criteria: individual implants exhibiting 1.5 mm bone remodelling and thereafter 0.2 mm annually. Lack of mobility, persistent infection, pain or was removed. | - | - | - | - |
| Migliorati et al., 2013 | A, SCTG vs. non-SCTG SCTG = 24 non SCTG = 24 | 17.3% (n = 4) of sites resulted in a poor aesthetic outcome (PES < 6) in a control group consisting of ungrafted immediate implants, Whereas the grafted test group reported no unacceptable aesthetic outcomes. | - | - | ||
| Palattella et al., 2008 | A vs. C A = 9, C = 8 | 5/36 (13.9%) total sites has a PIS of 0 or 1 3/18 (16.7%) of patients in the IP + IR group 2/18 (11.7%) in the IP + DR group. Note results were not split into mesial and distal papilla. DIfference not statistically significant. | - | - | ||
| Pieri et al., 2011 | A*, (Morse-Taper vs. conventional) Morse-taper = 20 Conventional = 20 | Smith and Zarb (1989) criteria | 97.4% for test group, 100% in the control group | - | Control group: one abutment screw loosening 2 months after delivery of definitive crown (6 months after implant placement). One other patient had a provisional crown fracture after 3 weeks. This was replaced within 24 h | - |
| Prosper et al., 2003 | D, (Hydroxyapatite vs. Resorbable Membrane). Synthetic hydroxyapatite (HA) = 56 vs. membrane (MR) = 55 | Albrektsson (1986) criteria | 98.2% for implants placed with resorbable synthetic hydroxyapatite (HA), 96.4% for implants placed with a resorbable membrane (MR). This leads to an overall success rate of 97.3% | - | - | - |
| Shibly et al., 2010 | A(IL) v D A = 30, D = 30 | 7/29 (24.1%)implants had a decreased attached gingiva in group D, 4 of which needed corrective mucogingival surgery versus 3/26 (11.5%) implants in group A(IL) with decreased attached gingiva, of which 1 needed mucogingival surgery. | - | 1 implant in the conventional loading group failed due to an acute infection within 2 weeks of replacement implant (mandibular second premolar). | ||
| Slagter et al., 2015 | A vs. D A = 20, D = 20 | Self-Defined success criteria: Clinically stable and fulfilled their function without any discomfort to the patient for 1 year | - | Clinically unsatisfactory ICAI and PES/WES scores were found in a total of 6% of patients (n = 2) across both groups, with no significant difference between the scores of the groups | - | - |
| Tallarico et al., 2016 | D v F (with socket preservation) D = 12, F = 12 | - | - | - | ||
| Tallarico et al., 2017 | D,F with socket preservation in both D = 12, F = 12 | - | - | - | ||
| Urban et al., 2011 | D (autologous bone chips, ossix membrane, combination) AB = 26, OM = 28, ABOM = 23 | - | - | - | ||
| Van Nimwegen et al., 2018 | A (SCTG vs. No SCTG) SCTG = 30, No SCTG = 30 | - | - | - | ||
| Yoshino et al., 2014 | A (SCTG vs. No SCTG) SCTG = 10, No SCTG = 10 | Smith and Zarb (1989) criteria | 100% | 9/20 (22.5%) of total sites had a PIS of 0 or 1. Control group = 1 mesial papilla and 3 distal papilla Test group = 3 mesial papilla and 2 distal papilla No statistical difference between groups | 1 episode of provisional restoration debonding. 1 provisional restoration fractured near the cervical aspect during removal at the time of final impression making | - |
| Zuiderveld et al., 2018 | A (SCTG vs. no SCTG) SCTG = 30, No SCTG = 30 Note one implant in each group lost due to failure of survival | Albrektsson et al. (1986) criteria | 96.7% | Zuiderveld et al. (2018) reported 21.3% (12/58)of cases with an unacceptable level of aesthetics (PES <6) for the peri-implant mucosa and 14.9% (8/58) for the implant crown aesthetics (WES < 6) across both groups, with no difference in PES/WES scores between groups. 15.5% (9/58) of total sites had a PIS of 0 or 1.No difference in scores in between Control and test Control group: 3 mesial papilla and 2 distal papilla Test group: 2 mesial papilla and 2 distal papilla | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thanissorn, C.; Guo, J.; Jing Ying Chan, D.; Koyi, B.; Kujan, O.; Khzam, N.; Miranda, L.A. Success Rates and Complications Associated with Single Immediate Implants: A Systematic Review. Dent. J. 2022, 10, 31. https://doi.org/10.3390/dj10020031
Thanissorn C, Guo J, Jing Ying Chan D, Koyi B, Kujan O, Khzam N, Miranda LA. Success Rates and Complications Associated with Single Immediate Implants: A Systematic Review. Dentistry Journal. 2022; 10(2):31. https://doi.org/10.3390/dj10020031
Chicago/Turabian StyleThanissorn, Charn, Jason Guo, Dianna Jing Ying Chan, Bryar Koyi, Omar Kujan, Nabil Khzam, and Leticia Algarves Miranda. 2022. "Success Rates and Complications Associated with Single Immediate Implants: A Systematic Review" Dentistry Journal 10, no. 2: 31. https://doi.org/10.3390/dj10020031
APA StyleThanissorn, C., Guo, J., Jing Ying Chan, D., Koyi, B., Kujan, O., Khzam, N., & Miranda, L. A. (2022). Success Rates and Complications Associated with Single Immediate Implants: A Systematic Review. Dentistry Journal, 10(2), 31. https://doi.org/10.3390/dj10020031