Laser-Assisted aPDT Protocols in Randomized Controlled Clinical Trials in Dentistry: A Systematic Review

 , , ,
, , , 

Abstract
1. Introduction
- As noted above, the sub-cellular localisation of the photosensitizer. Within the target cell, the photosensitizer may affect lysosomes, mitochondria, the plasma membrane, Golgi apparatus and the endoplasmic reticulum. Most of the photosensitizers localise within mitochondria, where apoptosis is provoked via mitochondrial damage; lysosomes accumulate photosensitizers with more aggregation. The photosensitizer Foscan (a chlorin named m-tetrahydroxyphenylchlorin) may target the Golgi apparatus and the endoplasmic reticulum [6]. However, the plasma membrane is rarely noted as a site of photosensitizer accumulation [10].
- The chemical characteristics of the photosensitizer. The different physiology of Gram-positive and Gram-negative bacteria can affect the degree of binding of different photosensitizers. Indeed, Gram-positive bacteria can efficiently bind to cationic, neutral and anionic photosensitizers, while only cationic ones can bind to Gram-negative bacteria [15].
- The concentration of the photosensitizer applied. High concentrations of photosensitizer can be naturally cytotoxic in a non-illuminated state, and obstruct light transmission into tissue target sites [16].
- The blood serum content. The presence of serum in the medium can decrease the effectiveness of the therapy, in view of probable chemical and physicochemical interactions between such agents and selected serum biomolecules [17].
- The incubation time, also known as equilibration time, of the photosensitizer at target sites. This should ideally commence shortly prior to illumination (of a ca. a few minutes’ duration), since this favours localisation into the microorganisms, and does not allow penetration into host cells (this process requires many hours to occur) [18].
- The phenotype of the target cell. It is known that different tissue types have differential light optical properties of light (i.e., absorption and scattering) [6].
2. Materials and Methods
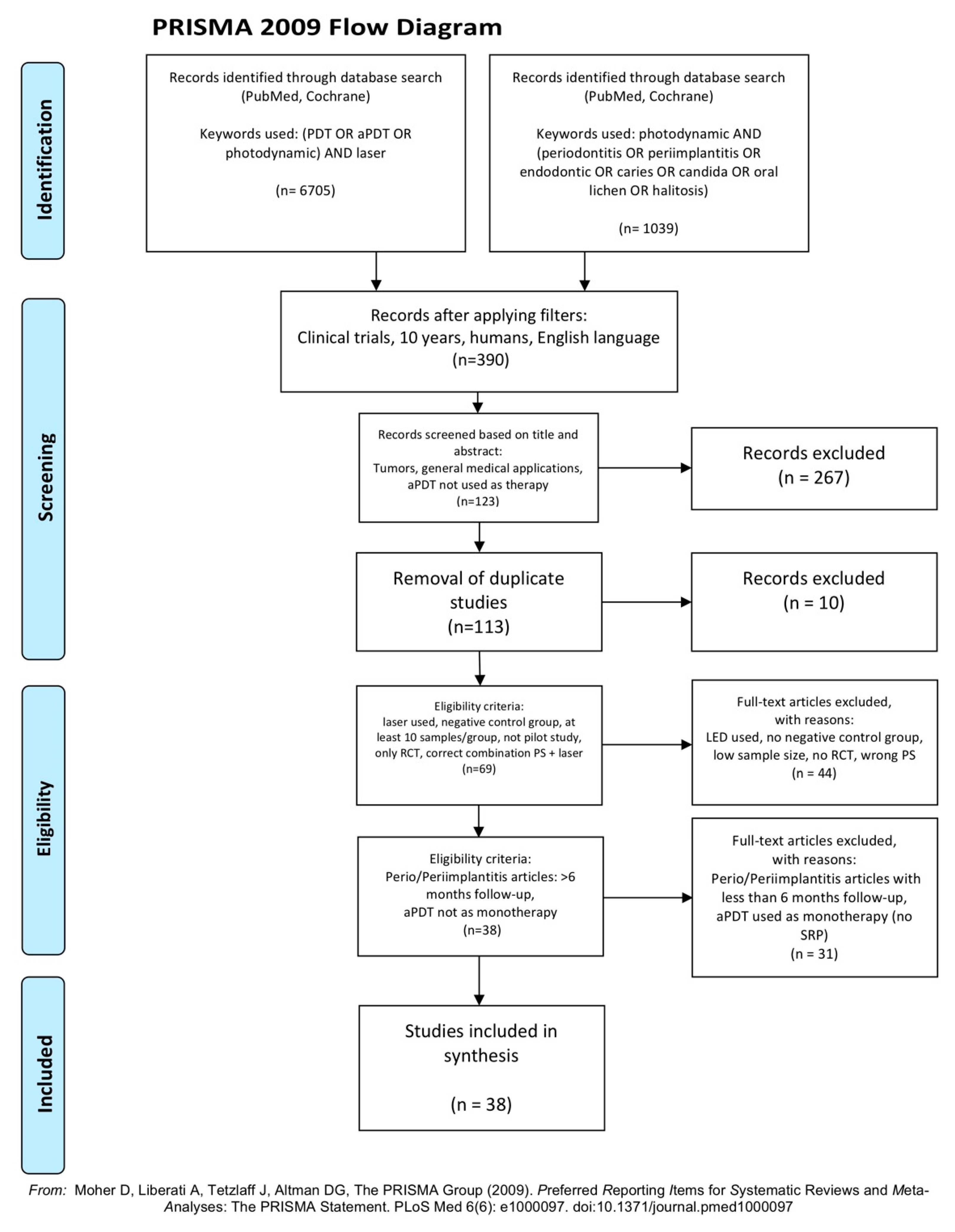
2.1. Search Strategy
- laser used as light source;
- negative control group;
- at least 10 samples/patients per group;
- only randomized controlled clinical trials;
- correct combinations of photosensitizer (PS) and the laser source employed;
- a minimum of a 6 month follow-up for periodontitis/peri-implantitis articles.
- duplicates or studies with the same ethical approval number;
- tumours, general medical applications, aPDT form not used as a therapy;
- LED or lamps used as light sources;
- no negative control group;
- low sample/patients sizes (less than 10 per group);
- no randomized controlled clinical trials or pilot studies;
- erroneous combinations of photosensitizer and laser employed;
- for periodontitis/peri-implantitis articles:
- ➢
- <6 month follow-up
- ➢
- aPDT used as a monotherapy (without scaling and root planning—SRP)
- periodontitis: 17
- peri-implantitis: 4
- endodontics: 5
- caries disinfection: 5
- candida disinfection: 2
- halitosis: 1
- oral lichen planus (OLP): 3
- healing of pericoronitis: 1
2.2. Data Extraction
- Citation (first author and publication year);
- Type of study/number of samples/pocket depth (only for periodontitis and peri-implantitis articles);
- Test/control groups;
- Laser and photosensitizer used (PS concentration);
- aPDT protocol/number of sessions involved;
- Follow-up;
- Outcome.
2.3. Quality Assessment
- Randomization?
- Sample size calculation and required sample numbers included?
- Baseline situation similar to that of the test group?
- Blinding?
- Parameters of laser use described appropriately, and associated calculations correct?
- Power meter used?
- Numerical results available (statistics)?
- No missing outcome data?
- All samples/patients completed the follow-up evaluation?
- Correct interpretation of data acquired?
- High risk: 0–4
- Moderate risk: 5–7
- Low risk: 8–10
3. Results
3.1. Primary Outcome
3.2. Data Presentation
3.3. Quality Assessment Presentation
3.4. Analysis of Data
- 0/2 in candida disinfection;
- 1/1 in halitosis [55];
- 0/1 in healing pericoronitis.
- incubation time: 2/16 (12.5%);
- power: 4/16 (25%);
- tip or spot size: 13/16 (81.2%);
- fluence value incorrectly calculated (i.e., either the tip or energy applied is erroneous): 2/16 (12.5%).
4. Discussion
4.1. aPDT Components
4.1.1. Photosensitizers
4.1.2. Light Diffusion
4.1.3. Oxygen
4.2. Healing
4.3. Clinical Aspects
- Selectivity for prokaryotic cells over eukaryotes, so that collateral damage to healthy tissue is minimised;
- Short incubation time, so that binding selectivity is achieved;
- High quantum yields for photochemical reactions and low quantum yields for photobleaching;
- High extinction coefficient, which demonstrates the ability of a molecule to absorb light at a specific wavelength (usually at the maximum absorption band) [8];
- Possess cationic charge and therefore be effective against both Gram-positive and Gram-negative microorganisms;
- Ability to kill multiple kinds of microorganisms at low concentrations and at low light fluences;
- Low side effects, such as photosensitivity and pain;
- Low dark toxicity without applied illumination;
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- St. Denis, T.G.; Dai, T.; Izikson, L.; Astrakas, C.; Anderson, R.R.; Hamblin, M.R.; Tegos, G.P. All you need is light, antimicrobial photoinactivation as an evolving and emerging discovery strategy against infectious disease. Virulence 2011, 2, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Diaz, M.; Huang, Y.Y.; Hamblin, M.R. Use of fluorescent probes for ROS to tease apart Type I and Type II photochemical pathways in photodynamic therapy. Methods 2016, 109, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Carrera, E.T.; Dias, H.B.; Corbi, S.C.T.; Marcantonio, R.A.C.; Bernardi, A.C.A.; Bagnato, V.S.; Hamblin, M.R.; Rastelli, A.N.S. The application of antimicrobial photodynamic therapy (aPDT) in dentistry: A critical review. Laser Phys. 2016, 26, 12300. [Google Scholar] [CrossRef] [PubMed]
- Nyman, E.; Hynninen, P. Research advances in the use of tetrapyrrolic photosensitizers for photodynamic therapy. J. Photochem. Photobiol. B Biol. 2004, 73, 1–28. [Google Scholar] [CrossRef]
- Wainwright, M.; Byrne, M.; Gattrell, M. Phenothiazinium-based photobactericidal materials. J. Photochem. Photobiol. B Biol. 2006, 84, 227–230. [Google Scholar] [CrossRef]
- Castano, A.P.; Demidova, T.N.; Hamblin, M.R. Mechanisms in photodynamic therapy: Part one—Photosensitizers, photochemistry and cellular localization. Photodiagnosis Photodyn. Ther. 2004, 1, 279–293. [Google Scholar] [CrossRef]
- Coluzzi, D.; Aoki, A.; Chiniforush, N. Light source Chapter 14.6. In Lasers in Dentistry-Current Concepts, 1st ed.; Coluzzi, D., Parker, S., Eds.; Springer: Cham, Switzerland, 2017; p. 309. ISBN 978-3-319-51944-9. [Google Scholar]
- Sellera, F.; Nascimento, C.; Ribeiro, M. Photodynamic Therapy in Veterinary Medicine: From Basics to Clinical Practice, 1st ed.; Springer: Cham, Switzerland, 2016; ISBN 978-3-319-45007-0. [Google Scholar]
- Parker, S. The use of diffuse laser photonic energy and indocyanine green photosensitiser as an adjunct to periodontal therapy. Br. Dent. J. 2013, 215, 167–171. [Google Scholar] [CrossRef]
- Parker, S. Photodynamic Antimicrobial Chemotherapy in the General Dental Practice (Introduction). J. Laser Dent. 2009, 17, 131–138. [Google Scholar]
- Konopka, K.; Goslinski, T. Photodynamic therapy in dentistry. J. Dent. Res. 2007, 86, 694–707. [Google Scholar] [CrossRef]
- Abrahamse, H.; Hamblin, M.R. New photosensitizers for photodynamic therapy. Biochem. J. 2016, 473, 347–364. [Google Scholar] [CrossRef]
- Yin, R.; Hamblin, M. Antimicrobial Photosensitizers: Drug Discovery under the Spotlight. Curr. Med. Chem. 2015, 22, 2159–2185. [Google Scholar] [CrossRef]
- Merkel, P.; Kearns, D. Remarkable solvent effects on the lifetime of 1Δg oxygen. J. Am. Chem. Soc. 1972, 94, 1029–1030. [Google Scholar] [CrossRef]
- George, S.; Hamblin, M.R.; Kishen, A. Uptake pathways of anionic and cationic photosensitizers into bacteria. Photochem. Photobiol. Sci. 2009, 8, 788. [Google Scholar] [CrossRef] [PubMed]
- Fukuzumi, S.; Ohkubo, K.; Zheng, X.; Chen, Y.; Pandey, R.; Zhan, R.; Kadish, K. Metal Bacteriochlorins Which Act as Dual Singlet Oxygen and Superoxide Generators. J. Phys. Chem. B 2008, 112, 2738–2746. [Google Scholar] [CrossRef]
- Hamblin, M.R.; Hasan, T. Photodynamic therapy: A new antimicrobial approach to infectious disease? Photochem. Photobiol. Sci. 2004, 3, 436. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, M.; Maisch, T.; Nonell, S.; Plaetzer, K.; Almeida, A.; Tegos, G.P.; Hamblin, M.R. Photoantimicrobials—Are we afraid of the light? Lancet Infect. Dis. 2017, 17, e49–e55. [Google Scholar] [CrossRef]
- Gursoy, H.; Ozcakir-Tomruk, C.; Tanalp, J.; Yilmaz, S. Photodynamic therapy in dentistry: A literature review. Clin. Oral Investig. 2013, 17, 1113–1125. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Higgins, J.; Savović, J.; Page, M.; Elbers, R.; Sterne, J. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., Welch, V., Eds.; John Wiley & Sons: Chichester, UK, 2019; pp. 205–228. [Google Scholar] [CrossRef]
- Grzech-Leśniak, K.; Gaspirc, B.; Sculean, A. Clinical and microbiological effects of multiple applications of antibacterial photodynamic therapy in periodontal maintenance patients. A randomized controlled clinical study. Photodiagnosis Photodyn. Ther. 2019, 27, 44–50. [Google Scholar] [CrossRef]
- Gandhi, K.; Pavaskar, R.; Cappetta, E.; Drew, H. Effectiveness of Adjunctive Use of Low-Level Laser Therapy and Photodynamic Therapy After Scaling and Root Planing in Patients with Chronic Periodontitis. Int. J. Periodontics Restor. Dent. 2019, 39, 837–843. [Google Scholar] [CrossRef]
- Hill, G.; Dehn, C.; Hinze, A.V.; Frentzen, M.; Meister, J. Indocyanine green-based adjunctive antimicrobial photodynamic therapy for treating chronic periodontitis: A randomized clinical trial. Photodiagnosis Photodyn. Ther. 2019, 26, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Bechara Andere, N.M.R.; dos Santos, N.C.C.; Araujo, C.F.; Mathias, I.F.; Rossato, A.; de Marco, A.C.; Santamaria, M.; Jardini, M.A.N.; Santamaria, M.P. Evaluation of the local effect of nonsurgical periodontal treatment with and without systemic antibiotic and photodynamic therapy in generalized aggressive periodontitis. A randomized clinical trial. Photodiagnosis Photodyn. Ther. 2018, 24, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Theodoro, L.H.; Assem, N.Z.; Longo, M.; Alves, M.L.F.; Duque, C.; Stipp, R.N.; Vizoto, N.L.; Garcia, V.G. Treatment of periodontitis in smokers with multiple sessions of antimicrobial photodynamic therapy or systemic antibiotics: A randomized clinical trial. Photodiagnosis Photodyn. Ther. 2018, 22, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Segarra-Vidal, M.; Guerra-Ojeda, S.; Vallés, L.S.; López-Roldán, A.; Mauricio, M.D.; Aldasoro, M.; Alpiste-Illueca, F.; Vila, J.M. Effects of photodynamic therapy in periodontal treatment: A randomized, controlled clinical trial. J. Clin. Periodontol. 2017, 44, 915–925. [Google Scholar] [CrossRef]
- Tabenski, L.; Moder, D.; Cieplik, F.; Schenke, F.; Hiller, K.A.; Buchalla, W.; Schmalz, G.; Christgau, M. Antimicrobial photodynamic therapy vs. local minocycline in addition to non-surgical therapy of deep periodontal pockets: A controlled randomized clinical trial. Clin. Oral Investig. 2017, 21, 2253–2264. [Google Scholar] [CrossRef]
- Da Cruz Andrade, P.V.; Euzebio Alves, V.T.; de Carvalho, V.F.; De Franco Rodrigues, M.; Pannuti, C.M.; Holzhausen, M.; De Micheli, G.; Conde, M.C. Photodynamic therapy decrease immune-inflammatory mediators levels during periodontal maintenance. Lasers Med. Sci. 2017, 32, 9–17. [Google Scholar] [CrossRef]
- Skurska, A.; Dolinska, E.; Pietruska, M.; Pietruski, J.K.; Dymicka, V.; Kemona, H.; Arweiler, N.B.; Milewski, R.; Sculean, A. Effect of nonsurgical periodontal treatment in conjunction with either systemic administration of amoxicillin and metronidazole or additional photodynamic therapy on the concentration of matrix metalloproteinases 8 and 9 in gingival crevicular fluid in patients with aggressive periodontitis. BMC Oral Health 2015, 15, 1–5. [Google Scholar] [CrossRef]
- Carvalho, V.F.; Andrade, P.V.C.; Rodrigues, M.F.; Hirata, M.H.; Hirata, R.D.C.; Pannuti, C.M.; De Micheli, G.; Conde, M.C. Antimicrobial photodynamic effect to treat residual pockets in periodontal patients: A randomized controlled clinical trial. J. Clin. Periodontol. 2015, 42, 440–447. [Google Scholar] [CrossRef]
- Alwaeli, H.A.; Al-Khateeb, S.N.; Al-Sadi, A. Long-term clinical effect of adjunctive antimicrobial photodynamic therapy in periodontal treatment: A randomized clinical trial. Lasers Med. Sci. 2015, 30, 801–807. [Google Scholar] [CrossRef]
- Müller Campanile, V.S.; Giannopoulou, C.; Campanile, G.; Cancela, J.A.; Mombelli, A. Single or repeated antimicrobial photodynamic therapy as adjunct to ultrasonic debridement in residual periodontal pockets: Clinical, microbiological, and local biological effects. Lasers Med. Sci. 2015, 30, 27–34. [Google Scholar] [CrossRef]
- Betsy, J.; Prasanth, C.S.; Baiju, K.V.; Prasanthila, J.; Subhash, N. Efficacy of antimicrobial photodynamic therapy in the management of chronic periodontitis: A randomized controlled clinical trial. J. Clin. Periodontol. 2014, 41, 573–581. [Google Scholar] [CrossRef]
- Luchesi, V.H.; Pimentel, S.P.; Kolbe, M.F.; Ribeiro, F.V.; Casarin, R.C.; Nociti, F.H.; Sallum, E.A.; Casati, M.Z. Photodynamic therapy in the treatment of class II furcation: A randomized controlled clinical trial. J. Clin. Periodontol. 2013, 40, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Balata, M.L.; de Andrade, L.P.; Santos, D.B.N.; Cavalcanti, A.N.; Tunes, U.d.R.; Ribeiro, E.d.P.; Bittencourt, S. Photodynamic therapy associated with full-mouth ultrasonic debridement in the treatment of severe chronic periodontitis: A randomized-controlled clinical trial. J. Appl. Oral Sci. 2013, 21, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Cappuyns, I.; Cionca, N.; Wick, P.; Giannopoulou, C.; Mombelli, A. Treatment of residual pockets with photodynamic therapy, diode laser, or deep scaling. A randomized, split-mouth controlled clinical trial. Lasers Med. Sci. 2012, 27, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Noro Filho, G.A.; Casarin, R.C.V.; Casati, M.Z.; Giovani, E.M. PDT in non-surgical treatment of periodontitis in HIV patients: A split-mouth, randomized clinical trial. Lasers Surg. Med. 2012, 44, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Albaker, A.M.; ArRejaie, A.S.; Alrabiah, M.; Al-Aali, K.A.; Mokeem, S.; Alasqah, M.N.; Vohra, F.; Abduljabbar, T. Effect of antimicrobial photodynamic therapy in open flap debridement in the treatment of peri-implantitis: A randomized controlled trial. Photodiagnosis Photodyn. Ther. 2018, 23, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Abduljabbar, T. Effect of mechanical debridement with and without adjunct antimicrobial photodynamic therapy in the treatment of peri-implant diseases in prediabetic patients. Photodiagnosis Photodyn. Ther. 2017, 17, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Romeo, U.; Nardi, G.M.; Libotte, F.; Sabatini, S.; Palaia, G.; Grassi, F.R. The antimicrobial photodynamic therapy in the treatment of peri-implantitis. Int. J. Dent. 2016, 2016. [Google Scholar] [CrossRef]
- Bassetti, M.; Schär, D.; Wicki, B.; Eick, S.; Ramseier, C.A.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin. Oral Implants Res. 2014, 25, 279–287. [Google Scholar] [CrossRef]
- Coelho, M.S.; Vilas-Boas, L.; Tawil, P.Z. The effects of photodynamic therapy on postoperative pain in teeth with necrotic pulps. Photodiagnosis Photodyn. Ther. 2019, 27, 396–401. [Google Scholar] [CrossRef]
- De Miranda, R.G.; Colombo, A.P.V. Clinical and microbiological effectiveness of photodynamic therapy on primary endodontic infections: A 6-month randomized clinical trial. Clin. Oral Investig. 2018, 22, 1751–1761. [Google Scholar] [CrossRef] [PubMed]
- Garcez, A.S.; Arantes-Neto, J.G.; Sellera, D.P.; Fregnani, E.R. Effects of antimicrobial photodynamic therapy and surgical endodontic treatment on the bacterial load reduction and periapical lesion healing. Three years follow up. Photodiagnosis Photodyn. Ther. 2015, 12, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Jurič, I.B.; Plečko, V.; Pandurić, D.G.; Anić, I. The antimicrobial effectiveness of photodynamic therapy used as an addition to the conventional endodontic re-treatment: A clinical study. Photodiagnosis Photodyn. Ther. 2014, 11, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Garcez, A.S.; Nuñez, S.C.; Hamblin, M.R.; Suzuki, H.; Ribeiro, M.S. Photodynamic therapy associated with conventional endodontic treatment in patients with antibiotic-resistant microflora: A preliminary report. J. Endod. 2010, 36, 1463–1466. [Google Scholar] [CrossRef] [PubMed]
- Alves, L.V.G.L.; Curylofo-Zotti, F.A.; Borsatto, M.C.; de Souza Salvador, S.L.; Valério, R.A.; Souza-Gabriel, A.E.; Corona, S.A.M. Influence of antimicrobial photodynamic therapy in carious lesion. Randomized split-mouth clinical trial in primary molars. Photodiagnosis Photodyn. Ther. 2019, 26, 124–130. [Google Scholar] [CrossRef]
- Bargrizan, M.; Fekrazad, R.; Goudarzi, N.; Goudarzi, N. Effects of antibacterial photodynamic therapy on salivary mutans streptococci in 5- to 6-year-olds with severe early childhood caries. Lasers Med. Sci. 2019, 34, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Ornellas, P.O.; Antunes, L.S.; Motta, P.C.; Mendonça, C.; Póvoa, H.; Fontes, K.; Iorio, N.; Antunes, L.A.A. Antimicrobial Photodynamic Therapy as an Adjunct for Clinical Partial Removal of Deciduous Carious Tissue: A Minimally Invasive Approach. Photochem. Photobiol. 2018, 94, 1240–1248. [Google Scholar] [CrossRef]
- Steiner-Oliveira, C.; Longo, P.; Aranha, A.; Ramalho, K.; Mayer, M.; de Paula Eduardo, C. Randomized in vivo evaluation of photodynamic antimicrobial chemotherapy on deciduous carious dentin. J. Biomed. Opt. 2015, 20, 108003. [Google Scholar] [CrossRef]
- Camila de Almelda, B.G.; Luz, M.A.; Simionato MR, L.; Ramalho, K.M.; Imparato, J.C.; Pinheiro, S.L. Clinical use of photodynamic antimicrobial chemotherapy for the treatment of deep carious lesions. J. Biomed. Opt. 2011, 16, 088003. [Google Scholar] [CrossRef]
- Afroozi, B.; Zomorodian, K.; Lavaee, F.; Zare Shahrabadi, Z.; Mardani, M. Comparison of the efficacy of indocyanine green-mediated photodynamic therapy and nystatin therapy in treatment of denture stomatitis. Photodiagnosis Photodyn. Ther. 2019, 27, 193–197. [Google Scholar] [CrossRef]
- De Senna, A.M.; Vieira, M.M.F.; Machado-de-Sena, R.M.; Bertolin, A.O.; Núñez, S.C.; Ribeiro, M.S. Photodynamic inactivation of Candida ssp. on denture stomatitis. A clinical trial involving palatal mucosa and prosthesis disinfection. Photodiagnosis Photodyn. Ther. 2018, 22, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Costa da Mota, A.C.; França, C.M.; Prates, R.; Deana, A.M.; Costa Santos, L.; Lopes Garcia, R.; Leal Gonçalves, M.L.; Mesquita Ferrari, R.A.; Porta Santos Fernandes, K.; Kalil Bussadori, S. Effect of photodynamic therapy for the treatment of halitosis in adolescents—A controlled, microbiological, clinical trial. J. Biophotonics 2016, 9, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Mirza, S.; Rehman, N.; Alrahlah, A.; Alamri, W.R.; Vohra, F. Efficacy of photodynamic therapy or low level laser therapy against steroid therapy in the treatment of erosive-atrophic oral lichen planus. Photodiagnosis Photodyn. Ther. 2018, 21, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, D.; Moussa, E.; Alnouaem, M. Evaluation of photodynamic therapy in treatment of oral erosive lichen planus in comparison with topically applied corticosteroids. Photodiagnosis Photodyn. Ther. 2017, 19, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Jajarm, H.H.; Falaki, F.; Sanatkhani, M.; Ahmadzadeh, M.; Ahrari, F.; Shafaee, H. A comparative study of toluidine blue-mediated photodynamic therapy versus topical corticosteroids in the treatment of erosive-atrophic oral lichen planus: A randomized clinical controlled trial. Lasers Med. Sci. 2015, 30, 1475–1480. [Google Scholar] [CrossRef]
- Eroglu, C.N.; Keskin Tunc, S.; Erten, R.; Usumez, A. Clinical and histological evaluation of the efficacy of antimicrobial photodynamic therapy used in addition to antibiotic therapy in pericoronitis treatment. Photodiagnosis Photodyn. Ther. 2018, 21, 416–420. [Google Scholar] [CrossRef]
- Parker, S.; Cronshaw, M.; Anagnostaki, E.; Bordin-Aykroyd, S.; Lynch, E. Systematic Review of Delivery Parameters Used in Dental Photobiomodulation Therapy. Photobiomodulation Photomed. Laser Surg. 2019, 37, 784–797. [Google Scholar] [CrossRef]
- Dimofte, A.; Finlay, J.; Ong, Y.; Zhu, T. A quality assurance program for clinical PDT. In Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic Therapy XXVII, 1st ed.; Kessel, D., Hassan, T., Eds.; SPIE Proceedings: Bellingham, DC, USA, 2018; p. 10476. [Google Scholar] [CrossRef]
- Chiniforush, N.; Pourhajibagher, M.; Shahabi, S.; Bahador, A. Clinical approach of high technology techniques for control and elimination of endodontic microbiota. J. Lasers Med. Sci. 2015, 6, 139–150. [Google Scholar] [CrossRef]
- Monzavi, A.; Chinipardaz, Z.; Mousavi, M.; Fekrazad, R.; Moslemi, N.; Azaripour, A.; Bagherpasand, O.; Chiniforush, N. Antimicrobial photodynamic therapy using diode laser activated indocyanine green as an adjunct in the treatment of chronic periodontitis: A randomized clinical trial. Photodiagnosis Photodyn. Ther. 2016, 14, 93–97. [Google Scholar] [CrossRef]
- Tegos, G.; Anbe, M.; Yang, C.; Demidova, T.; Satti, M.; Mroz, P.; Janjua, S.; Gad, F.; Hamblin, M. Protease-Stable Polycationic Photosensitizer Conjugates between Polyethyleneimine and Chlorin(e6) for Broad-Spectrum Antimicrobial Photoinactivation. Antimicrob. Agents Chemother. 2006, 50, 1402–1410. [Google Scholar] [CrossRef]
- Kostryukova, L.; Prozorovskiy, V.; Medvedeva, N.; Ipatova, O. Comparison of a new nanoform of the photosensitizer chlorin e6, based on plant phospholipids, with its free form. FEBS Open Biol. 2018, 8, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Ivanaga, C.; Miessi, D.; Nuernberg, M.; Claudio, M.; Garcia, V.; Theodoro, L. Antimicrobial photodynamic therapy (aPDT) with curcumin and LED, as an enhancement to scaling and root planing in the treatment of residual pockets in diabetic patients: A randomized and controlled split-mouth clinical trial. Photodiagnosis Photodyn. Ther. 2019, 27, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Ricci Donato, H.; Pratavieira, S.; Grecco, C.; Brugnera-Júnior, A.; Bagnato, V.; Kurachi, C. Clinical Comparison of Two Photosensitizers for Oral Cavity Decontamination. Photomed. Laser Surg. 2017, 35, 105–110. [Google Scholar] [CrossRef]
- Panhóca, V.; Esteban Florez, F.; Corrêa, T.; Paolillo, F.; de Souza, C.; Bagnato, V. Oral Decontamination of Orthodontic Patients Using Photodynamic Therapy Mediated by Blue-Light Irradiation and Curcumin Associated with Sodium Dodecyl Sulfate. Photomed. Laser Surg. 2016, 34, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Paschoal, M.; Moura, C.; Jeremias, F.; Souza, J.; Bagnato, V.; Giusti, J.; Santos-Pinto, L. Longitudinal effect of curcumin-photodynamic antimicrobial chemotherapy in adolescents during fixed orthodontic treatment: A single-blind randomized clinical trial study. Lasers Med. Sci. 2014, 30, 2059–2065. [Google Scholar] [CrossRef]
- Leite, D.; Paolillo, F.; Parmesano, T.; Fontana, C.; Bagnato, V. Effects of Photodynamic Therapy with Blue Light and Curcumin as Mouth Rinse for Oral Disinfection: A Randomized Controlled Trial. Photomed. Laser Surg. 2014, 32, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Araújo, N.; Fontana, C.; Gerbi, M.; Bagnato, V. Overall-Mouth Disinfection by Photodynamic Therapy Using Curcumin. Photomed. Laser Surg. 2012, 30, 96–101. [Google Scholar] [CrossRef]
- Sterenborg, H.; van Veen, R.; Aans, J.B.; Amelink, A.; Robinson, D.J. Light Dosimetry for Photodynamic Therapy: Basic Concepts. In Handbook of Photomedicine, 1st ed.; Hamblin, M., Huang, Y., Eds.; Taylor and Francis: Boca Raton, FL, USA, 2014; p. 282. [Google Scholar] [CrossRef]
- Sabino, C.P.; Garcez, A.S.; Núñez, S.C.; Ribeiro, M.S.; Hamblin, M.R. Real-time evaluation of two light delivery systems for photodynamic disinfection of Candida albicans biofilm in curved root canals. Lasers Med. Sci. 2015, 30, 1657–1665. [Google Scholar] [CrossRef]
- Garcez, A.S.; Hamblin, M.R. Methylene Blue and Hydrogen Peroxide for Photodynamic Inactivation in Root Canal—A New Protocol for Use in Endodontics. Eur. Endod. J. 2017, 2, 29. [Google Scholar] [CrossRef]
- Alvarenga, L.H.; Simões Ribeiro, M.; Kato, I.T.; Núñez, S.C.; Prates, R.A. Evaluation of red light scattering in gingival tissue—In vivo study. Photodiagnosis Photodyn. Ther. 2018. [Google Scholar] [CrossRef]
- Wenzler, J.-S.; Böcher, S.; Frankenberger, R.; Braun, A. Feasibility of transgingival laser irradiation for antimicrobial photodynamic therapy. Photodiagnosis Photodyn. Ther. 2019, 28, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, Y.; Hayashi, J.I.; Fujimura, T.; Iwamura, Y.; Yamamoto, G.; Nishida, E.; Ohno, T.; Okada, K.; Yamamoto, H.; Kikuchi, T.; et al. New irradiation method with indocyanine green-loaded nanospheres for inactivating periodontal pathogens. Int. J. Mol. Sci. 2017, 18, 154. [Google Scholar] [CrossRef] [PubMed]
- Finlay, J.C. Light Dosimetry for Photodynamic Therapy: Basic Concepts. In Handbook of Photomedicine, 1st ed.; Hamblin, M., Huang, Y., Eds.; Taylor and Francis: Boca Raton, FL, USA, 2014; p. 296. [Google Scholar] [CrossRef]
- Sharma, S.; Chiang, L.; Hamblin, M. Photodynamic therapy with fullerenesin vivo: Reality or a dream? Nanomedicine 2011, 6, 1813–1825. [Google Scholar] [CrossRef] [PubMed]
- Kareliotis, G.; Liossi, S.; Makropoulou, M. Assessment of singlet oxygen dosimetry concepts in photodynamic therapy through computational modeling. Photodiagnosis Photodyn. Ther. 2018, 21, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Fekrazad, R.; Khoei, F.; Hakimiha, N.; Bahador, A. Photoelimination of Streptococcus mutans with two methods of photodynamic and photothermal therapy. Photodiagnosis Photodyn. Ther. 2013, 10, 626–631. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Citation [ref] | Type of Study/Number of Samples/Pocket Depth | Test/Control Groups | Laser + PS Used (PS Concentration) | aPDT Protocol/Number of Sessions | Follow-Up | Outcome |
|---|---|---|---|---|---|---|
| Grzech-Lesniak et al. (2019) [22] | Parallel-group RCT/40 patients/one pocket with PD ≥ 5 mm, Chronic peridontitis | SRP + PDT (20 patients)/SRP (20 patients) | 635 nm + TBO (1 mg/mL) | One minute incubation time, wash with water, 200 mW, CW, 800 μm tip, diffusor tip, 30 s irradiation per pocket. sweeping movement, 117.64 J/mm2/3 sessions: 0, 7, 14 days | 6 months | No significant difference between groups in PD, PI, CAL, GR. PDT + SRP group sig. difference p = 0.007 in BOP and total bacterial count except A.a. |
| Gandhi et al. (2019) [23] | Split-mouth RCT/26 patients/one pocket with PD ≥ 5 mm in each quadrant, Chronic periodontitis | SRP + PDT (1)/SRP + LLLT (2), SRP alone (two quadrants) (3) | 810 nm + ICG (unknown concentration) | Two minutes incubation time, rinsing after with saline, 100 mW, 60 s irradiation inside pocket and upward movement, 60 s irradiation over outer gingiva/1 session: day 0 | 9 months | Groups 1 and 2 significantly better results than group 3 in P.g. and A.a. pathogen reduction, PI, GI, CAL, PD Groups 1 and 2 no difference |
| Hill et al. (2019) [24] | Split-mouth RCT/20 patients/one single and one multi-rooted tooth with PD ≥ 4 mm in each quadrant, Chronic periodontitis | SRP + PDT/SRP | 808 nm + ICG (0.1 mg/mL) | One minute incubation time, wash with water, 100 mW average, 2 kHz, 300 μm tip, 20 s irradiation, 2829 J/cm2 dose per tooth (4sites)/1 session: day 0 | 6 months | No significant difference between the groups in BOP, PD, GR, CAL and pathogen reduction |
| Bechara et al. (2018) [25] | Parallel split-mouth RCT/36 patients/one site in each quadrant with PD and CAL ≥ 5 mm and BOP, Aggressive periodontitis | SRP + PDT, SRP + PDT + clarithr. (18 patients)/SRP, SRP + clarithr. (18 patients) | 660 nm + MB (10 mg/mL) | One minute incubation time, wash with water, 60 mW, 60 s irradiation per site, 129 J/cm2 dose/1 session: day 0 | 6 months | Significant difference in PD and residual pockets only to antibiotics groups (PDT or not) |
| Theodoro et al. (2018) [26] | Parallel-group RCT/51 smoking patients/one tooth with PD ≥ 5 mm and one tooth with PD ≥ 7 mm in each quadrant, Chronic periodontitis | SRP + PDT (15 patients)/SRP + antibiotics MTZ + AMX (14 patients), SRP (14 patients) | 660 nm + MB (10 mg/mL) | One minute incubation time, 100 mW, spot size 0.03 cm2, 48 s irradiation per pocket, 160 J/cm2, 4.8 J/3 sessions: day 0, 2, 4 | 6 months | SRP + PDT significant difference in CAL compared to SRP SRP + PDT and SRP + antibiotics significant reduction in the number of pockets No significant difference between SRP + PDT and SRP + antibiotics groups |
| Segarra et al. (2017) [27] | Parallel-group RCT/20 healthy patients and 37 with periodontitis/four pockets with PD ≥ 5 mm and BOP, Chronic periodontitis | SRP + PDT (19 patients)/SRP (18 patients), healthy no treatment (20 patients) | 670 nm + MB (0.05 mg/mL) | Manufacturer’s instructions, 150 mW, 60 s irradiation each pocket/3 sessions: week 1, 5 and 13 | 6 months | No significant difference in CAL, PI, PD, GR, BOP, reduction in P.g. and T.f., no pathogen reduction in T.d., P.i., C.rectus aPDT + SRP significant difference in A.a. |
| Tabenski et al. (2017) [28] | Parallel-group RCT/45 patients/four teeth with PD ≥ 6 mm, Chronic periodontitis | SRP + PDT (15 patients)/SRP + minocycline (15 patients), SRP (15 patients) | 670 nm + MB (10 mg/mL) | Manufacturer’s instructions, 3 min incubation time, wash with saline, 75 mW/cm2, 6 sites per tooth, 10 s irradiation per site (60 s per tooth)/2 sessions: day 0, 7 | 12 months | No significant difference between groups in PPD, CAL, BOP A.a, P.g, T.f, T.d |
| DaCruz et al. (2017) [29] | Parallel-group RCT/28 patients/pockets with PD ≥ 4 mm, Chronic periodontitis | SRP + PDT (14 patients)/SRP (14 patients) | 660 nm + MB (0.1 mg/mL) | Five minutes incubation time, washed with water, 200 μm tip, 40 mW, 90 s irradiation per pocket, upward movement, 90 J/cm2 dose, powermeter used/1 session: week 6 | 12 months | No significant difference between groups in PD CAL, BOP, PI. IL-1α and IL-1β significant reduction in aPDT group. Benefit in immunomodulatory response. |
| Skurska et al. (2015) [30] | Parallel-group RCT/36 patients/three sites with PD ≥ 6 mm, Aggressive periodontitis | SRP + PDT (18 patients)/SRP + antibiotics (18 patients) | 660 nm + MB (10 mg/mL) | Three minutes incubation time, wash with saline, upward movement, 60 s irradiation per pocket/1 session: day 0 | 6 months | Control group significant reduction in MMP-8 No significant difference between groups in MMP-9 |
| Carvalho et al. (2015) [31] | Parallel-group RCT/34 patients/four sites with residual pockets with PD ≥ 5 mm, Chronic periodontitis | SRP + PDT (18 patients)/SRP (16 patients) | 660 nm + MB (0.1 mg/mL) | Five minutes incubation time, wash with water, 40 mW, 90 s irradiation per pocket, 90 J/cm2 dose, power meter used/1 session: day 45 | 12 months | No significant difference between groups in PD, BOP, CAL, PI |
| Alwaeli et al. (2015) [32] | Split-mouth RCT/16 patients/one tooth with attachment loss ≥ 4 mm in every quadrant, Chronic periodontitis | SRP + PDT/SRP | 660 nm + MB (10 mg/mL) | One to three minutes incubation time, 60 mW, 6 sites per tooth, 10 s irradiation per site/1 session: day 0 | 12 months | PDT + SRP group significant difference in PD, CAL, BOP |
| Mueller et al. (2015) [33] | Split-mouth RCT/27 patients/one site in each quadrant with residual pockets with PD ≥ 4 mm, Chronic Periodontitis | SRP + PDT/SRP | 670 nm + MB (0.05 mg/mL) | One minute incubation time, 280 mW, 60 s irradiation per pocket, diffusor tip/2 sessions: day 0, 7 | 6 months | No significant difference between groups in PD, BOP, CAL, total bacterial count |
| Betsy et al. (2014) [34] | Parallel-group RCT/88 patients/pockets with PD: 4–6 mm at least in two quadrants, Chronic periodontitis | SRP + PDT (44 patients)/SRP (44 patients) | 655 nm + MB (10 mg/mL) | Three minutes incubation time, wash with water, 60 mW/cm2, 200 μm tip, 60 s irradiation per pocket/1 session: day 0 | 6 months | PDT + SRP group significant difference in PD, CAL No significant difference between groups in halitosis |
| Luchesi et al. (2013) [35] | Parallel-group RCT/37 patients/one class II furcation with PD ≥ 5 mm and BOP, Chronic periodontitis | SRP + PDT (16 patients)/SRP + MB alone (21 patients) | 660 nm + MB (10 mg/mL) | One minute incubation time, wash with water, 60 mW, 600 μm tip, 60 s irradiation per pocket, upward movement, 129 J/cm2 dose/1 session: day 0 | 6 months | SRP + PDT group: significant difference in BOP, P.g, T.f and IL-1β reduction No significant difference between groups in PD, CAL, A.a., cytokines |
| Balata et al. (2013) [36] | Split-mouth RCT/22 patients/one pocket with PD ≥ 7 mm, one pocket with PD ≥ 5 mm and BOP on each side, Severe chronic periodontitis | SRP + PDT/SRP | 660 nm + MB (0.05 mg/mL) | Two minutes incubation time, 100 mW, 9 J, 600 μm tip, 90 s irradiation per pocket, 320 J/cm2 dose, powermeter used, transgingival, calculated distance must be 3 mm/1 session: day 0 | 6 months | No significant difference between groups in PD, CAL, GI, BOP, GR |
| Cappuyns et al. (2012) [37] | Split-mouth RCT/32 patients/one site in each quadrant with residual pockets with PD ≥ 4 mm and BOP, Chronic periodontitis | SRP + PDT (1)/SRP + 810 nm (2), SRP (3) | 660 nm + MB (0.1 mg/mL) | One minute incubation time, wash with water, 40 mW, 60 s irradiation per pocket/1 session: day 0 | 6 months | No significant difference between groups in PD, BOP, REC and A.a., P.g., T.f., T.d. |
| Filho et al. (2012) [38] | Split-mouth RCT/12 HIV patients/one site in each quadrant with PD ≥ 4 mm and BOP, Chronic periodontitis | SRP + PDT/SRP | 660 nm + MB (0.1 mg/mL) | Five minutes incubation time, 30 mW, spot size 0.07 cm2, 133 s irradiation per point (3 buccal—3 lingual), transgingival use/1 session: day 0 | 6 months | SRP + PDT significant difference in PD, CAL No significant difference between groups in A.a., P.g., T.f. |
| Citation [ref] | Type of Study/Number of Samples/Pocket Depth | Test/Control Groups | Laser + PS Used (PS Concentration) | aPDT Protocol/Number of Sessions | Follow-Up | Outcome |
|---|---|---|---|---|---|---|
| Albaker et al. (2018) [39] | Parallel-group RCT/24 patients/implants with PD ≥ 5 mm and BOP, Peri-implantitis | OFD + aPDT (11 patients)/OFD (13 patients) | 670 nm + MB (0.05 mg/mL) | Ten seconds incubation time, 150 mW, 600 μm tip, 60 s irradiation per pocket/1 session: day 0 | 12 months | No significant difference between groups in PD, BOP, MBL |
| Abduljabbar (2017) [40] | Parallel-group RCT/60 prediabetic patients/implants with PD ≥ 4 mm and BOP, Peri-implantitis | MD + aPDT/MD | 660 nm + MB (10 mg/mL) | Two minutes incubation time, wash with H2O2 3%, diffusor tip, 100 mW, 10 s irradiation per pocket/1 session: day 0 | 6 months | No significant difference between groups in PD, BOP |
| Romeo et al. (2016) [41] | Parallel-group RCT/40 patients/at least one implant site with PD ≥ 4 mm and BOP and suppuration, Peri-implantitis | MD + aPDT (63 implants)/MD (59 implants) | 670 nm + MB (10 mg/mL) | One minute incubation, wash with water, 75 mW/cm2, 5 J, 600 μm tip, diffusor tip, 60 s irradiation per pocket, total 1592 J/cm2, 25.54 W/cm2/1 session: day 0 | 6 months | MD + aPDT showed better results in PD, BOP No p-value available |
| Bassetti et al. (2014) [42] | Parallel-group RCT/40 patients/at least one implant with PD: 4–6 mm and bone loss: 0.5–2 mm, Initial peri-implantitis | MD + aPDT/MD + local minocycline | 660 nm + MB (10 mg/mL) | Three minutes incubation time, wash with H2O2 3%, 100 mW, diffusor tip, 10 s irradiation per pocket/2 sessions: day 0, 7 | 12 months | No significant difference between groups in PD, CAL, REC, BOP |
| Citation [ref] | Type of Study/Number of Samples | Test/Control Groups | Laser + PS Used (PS Concentration) | aPDT Protocol/Number of Sessions | Follow-Up | Outcome |
|---|---|---|---|---|---|---|
| Coelho et al. (2019) [43] | Parallel-group RCT/60 patients/single-rooted teeth with fully developed apices, no probing and no mobility Rubber dam used | aPDT + RC tx (30 patients)/RC tx (30 patients) Both groups received MB for 2 min | 660 nm + MB (0.5 mg/mL) | Two minutes incubation time, 100 mW, 180 s irradiation in vertical motion, 18 J, 600 J/cm2/1 session: day 0 | 7 days | aPDT + RC tx group showed significant difference in VAS score (lower) after 24 h and 72 h After 7 days no pain and no flare-up in both groups |
| de Miranda et al. (2018) [44] | Parallel-group RCT/16 patients/mandibular molars with apical periodontitis Rubber dam used | aPDT+RC tx (16 molars)/RC tx (16 molars) Both groups received Ca(OH)2 for 7 days before obturation | 660 nm + MB (25 mg/mL) | Five minutes incubation time, 100 mW, 300 s irradiation in vertical motion, 300 μm tip/1 session: day 0 | 6 months | Clinically no significant difference, (symptoms and bacteria counts) Radiographically significant better healing |
| Garcez et al. (2015) [45] | Repeated measures/28 teeth with periapical periodontitis and apical bone lesion Microbiological samples: 1. after access of bone lesion 2. after conventional surgery 3. after aPDT | Conventional apical surgery + aPDT Sampling before + after aPDT | 660 nm + MB (19 mg/mL) | Three minutes incubation time, 40 mW, 180 s irradiation time, 7.2 J, 200 μm tip/1 session: day 0 Additionally aPDT in the surgical cavity | Bacteria before/after Radiographs 3 years | Bacteria reduction: Conventional therapy 3.5 log surgery + aPDT 5 log (significant) Radiographic area reduction 78% (surgery + aPDT) |
| Juric et al. (2014) [46] | Repeated measures/21 teeth with periapical periodontitis, endodontic retreatment (endo ≥ 2 years), apical bone lesion 3 × 3 mm Microbiological samples: 1. after access of canal 2. after endo re-treatment 3. after aPDT Rubber dam used | Conventional endo re-treatment + aPDT Sampling before + after aPDT | 660 + MB (10 mg/mL) | Two minutes incubation time, wash with distilled water, dry, 100 mW, 60 s irradiation time, 450 μm diffusor tip/1 session: day 0 | Bacteria before/after | Chemomechanical preparation + aPDT vs. chemome-chanical preparation alone, significant difference in bacteria: Gram-positive (p = 0.02) Gram-negative (p = 0.005) facultative anaerobes (p = 0.013) obligate anaerobes (p = 0.007) |
| Garcez et al. (2010) [47] | Repeated measures/30 teeth of 21 patients with periapical periodontitis, endo retreatment previously with antibiotic resistance and apical bone lesion. Microbiological samples: 1. after access of canal 2. after endo re-treatment 3. after aPDT Rubber dam used | Conventional endo re-treatment + aPDT Sampling before + after aPDT Placing Ca(OH)2 for 7 days and then second aPDT session without sampling | 660 nm + polyethylenimine chlorin(e6) (3.6 mg/mL) | Two minutes incubation time, wash with distilled water, dry 40 mW, 240 s irradiation time, 9.6 J, 200 μm tip, spiral movement/1 session: day 0 | Bacteria before/after | The combination of endodontic therapy and aPDT killed all 9 multi-drug resistant bacterial species found in root canal infections No p-values available |
| Citation [ref] | Type of Study/Number of Samples | Test/Control Groups | Laser + PS Used (PS Concentration) | aPDT Protocol/Number of Sessions | Follow-Up | Outcome |
|---|---|---|---|---|---|---|
| Alves et al. (2019) [48] | Split mouth RCT/20 patients (6–8 yrs)/occlusal surfaces homologous primary molars (20 teeth per group) (microbiological repeated measurements before/after) Rubber Dam used | Selective caries removal + aPDT/Selective caries removal Deep restoration Dycal and Ketac Molar in both groups | 660 nm + MB (0.05 mg/mL) | Five minutes incubation time, wash with water, 100 mW, 180 s irradiation time, 640 J/cm2/1 session: day 0 | 6 months | After caries removal S.mutans 76% reduction (p = 0.04) After caries removal + aPDT S.mutans 92.6% reduction (p = 0.01) p < 0.05 between groups, no secondary caries in either group |
| Bargrizan et al. (2019) [49] | Parallel control RCT/56 patients (5–6 y) severe early childhood caries (Salivary S.mutans) | aPDT (14 patients)/TBO alone (14 patients), Laser alone (14 patients), Negative control (14 patients) | 633 nm + TBO (0.1 mg/mL) | Kept in mouth for 5 min incubation time, spit, 20 mW, 5 min total irradiation (60 s tongue 60 s palate 90 s maxilla buccal mucosa 90 s mandibula buccal mucosa, klo4 output nozzle 1 cm2 area, 6 J/cm2/2 sessions: day 0, 3 | 2 weeks | Significant reduction in Salivary S.mutans in test group compared to all groups. Before second intervention S.mutans levels rising. Two interventions advisable |
| Ornellas et al. (2018) [50] | Microbiological repeated measurements/18 primary molars | Selective caries removal + aPDT/Selective caries removal Sampling before + after aPDT | 660 nm + MB (0.1 mg/mL) | Five minutes incubation time, removal with sterile cotton, 100 mW, 90 s irradiation time, 3 mm2 spot, 300 J/cm2/1 session: day 0 | Bacteria before/after | Reduction of log1 in Strep spp., Lactobacillus spp. and mutans streptococci Not significant |
| Steiner-Oliveira et al. (2015) [51] | Parallel-control RCT/32 patients (5–7 y) with partial caries removal in primary molars Rubber Dam used | aPDT (10 patients)/LED aPDT (10 patients)/CHX (12 patients) Sampling before/after partial caries removal | 660 nm + MB (0.1 mg/mL) | Five minutes incubation time, wash with water, 100 mW, 90 s irradiation time, 320 J/cm2, Powermeter used/1 session: day 0 | 12 months | No significant difference between groups aPDT group: Log1 reduction in total bacteria count |
| Guglielmi et al. (2011) [52] | Microbiological repeated measurements/26 permanent molars Rubber Dam used | Selective caries removal + aPDT/Selective caries removal Sampling before + after aPDT | 660 nm + MB (0.1 mg/mL) | Five minutes incubation time, no wash, 100 mW, 0.028 cm2 spot size, 9 J, 90 s irradiation, perpendicular to occlusal surface, one point to the center, 320 J/cm2, Power meter used/1 session: day 0 | Bacteria before/after | Log10 reduction: 1.38 for mutans streptococci (p < 0.0001), 0.93 for Lactobacillus spp. (p < 0.0001), 0.91 for total viable bacteria (p < 0.0001) |
| Citation [ref] | Type of Study/Number of Samples | Test/Control Groups | Laser + PS Used (PS Concentration) | aPDT Protocol/Number of Sessions | Follow-Up | Outcome |
|---|---|---|---|---|---|---|
| Afroozi et al. (2019) [53] | Parallel-control RCT/56 patients with denture stomatitis (candida spp) | aPDT + Nystatin (28 patients)/Nystatin (28 patients) Both groups received nystatin tx 3 times per day for 15 days | 810 nm + ICG (1 mg/mL) | Palatal application 10 min incubation time, no wash, 30 s irradiation time per point, 56 J/cm2/2 sessions: day 0, 7 (tx of denture not mentioned) | 60 days | aPDT + nystatin group significant difference in candida CFU reduction After 15 days p = 0.013 After 60 days (p < 0.0001) Significant difference in reduction in lesion extension after 15 days p = 0.005 and in Newton’s classification (p = 0.007) after 60 days |
| de Senna et al. (2018) [54] | Parallel-control RCT/36 patients with denture stomatitis (candida spp) | aPDT (18 patients)/Miconazol (18 patients) | 660 nm + MB (0.45 mg/mL) | Palatal + prosthesis: 10 min incubation time, no wash, 100 mW, 280 s irradiation time per cm2, dose 28 J/cm2/8 sessions: twice a week for 4 weeks | 30 days | aPDT group significant reduction in erythema after 15 days (after 30 days no significant difference) No difference in candida CFU reduction |
| da Mota et al. (2016) [55] | Parallel-control RCT/46 patients with halitosis | aPDT (15 patients)/aPDT + tongue scraper (15 patients), tongue scraper alone (16 patients) | 660 nm + MB (0.05 mg/mL) | Five minutes incubation time, no wash, 100 mW, 90 s irradiation time per point (6 points), 1 cm distance from each other, 9 J, fluence 320 J/cm2, irradiance 3.5 W/cm2, spot area 0.028 cm2, power meter used/1 session: day 0 | 7 days | aPDT significantly better immediate CFU results No significant differences in CFU or H2S results between groups after 7 days |
| Citation [ref] | Type of Study/Number of Samples | Test/Control Groups | Laser + PS Used (PS Concentration) | aPDT Protocol/Number of Sessions | Follow-Up | Outcome |
|---|---|---|---|---|---|---|
| Mirza et al. (2018) [56] | Parallel-control RCT/45 patients with erosive atrophic OLP tongue, buccal mucosa ≤3 cm | aPDT (15 patients)/LLLT (15 patients), Topical corticosteroid: dexamethasone + nystatin (15 patients) | 630 nm + TBO (1 mg/mL) | Ten minutes incubation time, no wash, 10 mW, 10 mW/cm2, 150 s irradiation time per point, spot size 1 cm2, fluence 1.5 J/cm2/8 sessions: 2 times weekly for a month | 7 days after completion of tx | Efficacy index: aPDT significant different compared to LLLT (p = 0.001) and corticosteroid group (p = 0.001) Pain control (VAS): Control group significantly better. Corticosteroids still gold standard in tx of clinical signs and symptoms |
| Mostafa et al. (2017) [57] | Parallel-control RCT/20 patients with oral erosive lesions | aPDT (10 patients)/Topical corticosteroid: triamcinolone (10 patients) | 660 nm + MB (50 mg/mL) | Five minutes incubation time (gargle), no wash, 100–130 mW/cm2, 70 s irradiation time/8 sessions: Once a week for two months | 2 months after completion of tx | aPDT group: VAS and lesion size decreased significantly in all follow up sessions until 2 months |
| Jajarm et al. (2015) [58] | Parallel-control RCT/25 patients with erosive atrophic OLP tongue, buccal mucosa ≤3 cm | aPDT (11 patients)/Topical corticosteroid: dexamethasone + nystatin (14 patients) | 630 nm + TBO (1 mg/mL) | Ten minutes incubation time, no wash, 10 mW, 10 mW/cm2, 150 s irradiation time per point, spot size 1 cm2, dose 1.5 J/cm2/8 sessions: 2 times weekly for a month | 4 weeks after completion of tx | Pain control (VAS) and Efficacy Index: Control group significantly better. No relapse (100% control group 72.7% aPDT group) |
| Citation [ref] | Type of Study/Number of Samples | Test/Control Groups | Laser + PS Used (PS Concentration) | aPDT Protocol/Number of Sessions | Follow-Up | Outcome |
|---|---|---|---|---|---|---|
| Eroglu et al. (2019) [59] | Parallel-control RCT/40 patients with pericoronitis region of mandibular third molars | aPDT + Amoxicillin (20 patients)/Amoxicillin (20 patients) 2 Biopsies: day 0 and day of extraction-day 2 | 810 nm + ICG (0.1 mg/mL) | Incubation time unknown, no wash, 300 mW, 40 s irradiation time per area (operculum, distal, buccal and lingual pockets, 200 μm tip/2 sessions: day 0, 1 | 7 days | aPDT group: Histologically significantly better for inflammatory cell scores Day 6 (4 days after surgery): aPDT VAS = 0 vs control VAS = 1 statistically significant (but not clinical) |
| Citation [ref] | Randomization | Sample Size Calculation and Required Number Included | Baseline Situation Similar | Blinding | Parameters of Laser Use Described Appropriately and Calculations Correct | Power Meter Used | Numerical Results Available (Statistics) | No Missing Outcome Data | All Samples/Patients Completed the Follow-Up | Correct Interpretation of Data | Total Score/10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Periodontitis | |||||||||||
| Grzech-Leśniak et al. (2019) [22] | yes | no | yes | no | yes | no | yes | yes | yes | yes | 7 |
| Gandhi et al. (2019) [23] | yes | yes | yes | yes | no | no | yes | yes | yes | yes | 8 |
| Hill et al. (2019) [24] | yes | yes | yes | yes | yes | no | yes | yes | yes | yes | 9 |
| Bechara et al. (2018) [25] | yes | yes | yes | yes | no | no | yes | yes | yes | yes | 8 |
| Theodoro et al. (2018) [26] | yes | yes | yes | yes | yes | no | yes | yes | yes | yes | 9 |
| Segarra et al. (2017) [27] | yes | yes | no | yes | no | no | yes | yes | yes | yes | 7 |
| Tabenski et al. (2017) [28] | yes | yes | yes | yes | yes | no | yes | yes | yes | yes | 9 |
| Da Cruz Andrade et al. (2017) [29] | yes | no | yes | yes | yes | yes | yes | yes | yes | yes | 9 |
| Skurska et al. (2015) [30] | yes | no | no | yes | no | no | yes | yes | yes | yes | 6 |
| Carvalho et al. (2015) [31] | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | 10 |
| Alwaeli et al. (2015) [32] | yes | no | yes | yes | no | no | yes | yes | yes | yes | 7 |
| Mueller et al. (2015) [33] | yes | no | yes | yes | no | no | yes | yes | yes | yes | 7 |
| Betsy et al. (2014) [34] | yes | yes | yes | yes | no | no | yes | yes | yes | yes | 8 |
| Luchesi et al. (2013) [35] | yes | yes | yes | yes | no | no | yes | yes | yes | yes | 8 |
| Balata et al. (2013) [36] | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | 10 |
| Cappuyns et al. (2012) [37] | yes | yes | yes | yes | no | no | yes | yes | yes | yes | 8 |
| Filho et al. (2012) [38] | yes | yes | yes | yes | yes | no | yes | yes | yes | yes | 9 |
| Peri-Implantitis | |||||||||||
| Albaker et al. (2018) [39] | yes | no | no | yes | yes | no | yes | yes | yes | yes | 7 |
| Abduljabbar (2017) [40] | yes | no | yes | no | no | no | yes | yes | yes | yes | 6 |
| Romeo et al. (2016) [41] | yes | no | yes | no | yes | no | no | yes | yes | yes | 6 |
| Bassetti et al. (2014) [42] | yes | no | yes | yes | no | no | yes | yes | yes | yes | 7 |
| Endo | |||||||||||
| Coelho et al. (2019) [43] | yes | yes | yes | yes | yes | no | yes | yes | yes | yes | 9 |
| de Miranda et al. (2018) [44] | yes | yes | yes | yes | yes | no | yes | yes | yes | yes | 9 |
| Garcez et al. (2015) [45] | yes | no | yes | no | no | no | yes | yes | yes | yes | 6 |
| Juric et al. (2014) [46] | yes | no | yes | yes | yes | no | yes | yes | yes | yes | 8 |
| Garcez et al. (2010) [47] | yes | no | yes | yes | yes | no | no | yes | yes | yes | 7 |
| Caries | |||||||||||
| Alves et al. (2019) [48] | yes | yes | yes | no | yes | no | yes | yes | yes | yes | 8 |
| Bargrizan et al. (2019) [49] | yes | yes | yes | yes | yes | no | yes | yes | yes | yes | 9 |
| Ornellas et al. (2018) [50] | yes | no | yes | yes | yes | no | yes | yes | yes | yes | 8 |
| Steiner-Oliveira et al. (2015) [51] | yes | no | yes | yes | yes | yes | yes | yes | yes | yes | 9 |
| Guglielmi et al. (2011) [52] | yes | yes | yes | no | yes | yes | yes | yes | yes | yes | 9 |
| Candida/Halitosis | |||||||||||
| Afroozi et al. (2019) [53] | yes | no | yes | yes | no | no | yes | yes | yes | yes | 7 |
| de Senna et al. (2018) [54] | yes | no | yes | no | no | no | yes | yes | yes | yes | 6 |
| da Mota et al. (2016) [55] | yes | no | yes | yes | yes | yes | yes | yes | yes | yes | 9 |
| OLP | |||||||||||
| Mirza et al. (2018) [56] | yes | no | yes | yes | yes | no | yes | no | no | yes | 6 |
| Mostafa et al. (2017) [57] | yes | no | yes | no | no | no | yes | yes | yes | yes | 6 |
| Jajarm et al. (2015) [58] | yes | no | yes | no | yes | no | yes | yes | yes | yes | 7 |
| Healing | |||||||||||
| Eroglu et al. (2018) [59] | yes | no | yes | yes | no | no | yes | yes | yes | yes | 7 |
| MB-Perio/Peri-Implantitis 8 Papers | MB-Endo 3 Papers | MB-Caries 4 Papers | MB-Halitosis 1 Paper | |
|---|---|---|---|---|
| Photosensitizer concentration (mg/mL) | 0.05–10 10 * | 5, 10, 25 | 0.05–0.1 0.1 * | 0.05 |
| Incubation time (min) | 1–5 | 2, 5, 2 * | 5 | 5 |
| Power (mW) | 60–150 100 * | 100 | 100 | 100 |
| Irradiation time (s) | 48–133 60 * or 90 * | 60, 180, 300 | 90–180 90 * | 90 |
| Tip (μm) | 200–600 600 * | 200, 300, 450 | 1900 | 1900 |
| Number of sessions | 1–3 1 * | 1 | 1 | 1 |
| TBO-Perio 1 Paper | TBO-Caries 1 Paper | TBO-Olp 2 Papers | |
|---|---|---|---|
| Photosensitizer concentration (mg/mL) | 1 | 0.1 | 1 |
| Incubation time (min) | 1 | 5 | 10 |
| Power (mW) | 200 | 20 | 10 |
| Irradiation time (s) | 30 | 90 | 150 |
| Tip/spot size | 800 μm diffusor | 1 cm2 | 1 cm2 |
| Number of sessions | 3 | 2 | 8 |
| ICG-Perio 1 Paper | |
|---|---|
| Photosensitizer concentration (mg/mL) | 0.1 |
| Incubation time (min) | 1 |
| Power (mW) | 100 |
| Irradiation time (s) | 20 |
| Tip (μm) | 300 |
| Number of sessions | 1 |
| PEI-ce6-Endo 1 Paper | |
|---|---|
| Photosensitizer concentration (mg/mL) | 3.6 |
| Incubation time (min) | 2 |
| Power (mW) | 40 |
| Irradiation time (s) | 240 |
| Tip (μm) | 200 |
| Number of sessions | 1 |
| Photosensitizer | Laser | ||
|---|---|---|---|
| Type | Power | Tip Diameter | Trans-gingival Use or Not |
| Concentration | Emission Mode | Diffusor Tip or Not | Energy Distribution |
| Incubation Time | Irradiation Time | Tip-To-Tissue Distance | Speed of Movement |
| Wash/No Wash before Illumination | Total Energy Delivered | Spot Size at Tissue |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mylona, V.; Anagnostaki, E.; Parker, S.; Cronshaw, M.; Lynch, E.; Grootveld, M. Laser-Assisted aPDT Protocols in Randomized Controlled Clinical Trials in Dentistry: A Systematic Review. Dent. J. 2020, 8, 107. https://doi.org/10.3390/dj8030107
Mylona V, Anagnostaki E, Parker S, Cronshaw M, Lynch E, Grootveld M. Laser-Assisted aPDT Protocols in Randomized Controlled Clinical Trials in Dentistry: A Systematic Review. Dentistry Journal. 2020; 8(3):107. https://doi.org/10.3390/dj8030107
Chicago/Turabian StyleMylona, Valina, Eugenia Anagnostaki, Steven Parker, Mark Cronshaw, Edward Lynch, and Martin Grootveld. 2020. "Laser-Assisted aPDT Protocols in Randomized Controlled Clinical Trials in Dentistry: A Systematic Review" Dentistry Journal 8, no. 3: 107. https://doi.org/10.3390/dj8030107
APA StyleMylona, V., Anagnostaki, E., Parker, S., Cronshaw, M., Lynch, E., & Grootveld, M. (2020). Laser-Assisted aPDT Protocols in Randomized Controlled Clinical Trials in Dentistry: A Systematic Review. Dentistry Journal, 8(3), 107. https://doi.org/10.3390/dj8030107