Biomodification of a Class-V Restorative Material by Incorporation of Bioactive Agents

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Material Formulation
- (a)
- Hydroxyapatite (CAPTAL, London, UK).
- (b)
- Chitosan (Sigma-Aldrich Company Ltd., Dorset, UK).
- (c)
- Chondroitin sulphate (Sigma-Aldrich Company Ltd., Dorset, UK).
- (d)
- Bioglass (Sigma-Aldrich Company Ltd., Dorset, UK).
- (e)
- Gelatine (Sigma Aldrich Company Ltd., Dorset, UK).
- (f)
- Processed bovine dentin [24], prepared according to the following protocol:
2.2. Specimen Fabrication
2.3. Sample Size
2.4. Mechanical Tests
2.4.1. Working and Setting Time Determination
2.4.2. Biaxial Flexural Strength Test
2.4.3. Vickers Hardness Test
2.4.4. Compressive Strength Test
2.5. Biological Tests
2.5.1. Cell Culture
2.5.2. Investigation of Cell Viability in the Monolayer Culture System
2.5.3. Investigation Biocompatibility of the Modified GIC Discs Using 3D-OMM Model
2.6. Statistical Analysis
3. Results
3.1. Mechanical Tests
3.1.1. Working and Setting Time
3.1.2. Biaxial Flexural Strength (BFS)
3.1.3. Vickers Hardness
3.1.4. Compressive Strength
3.2. Biological Tests
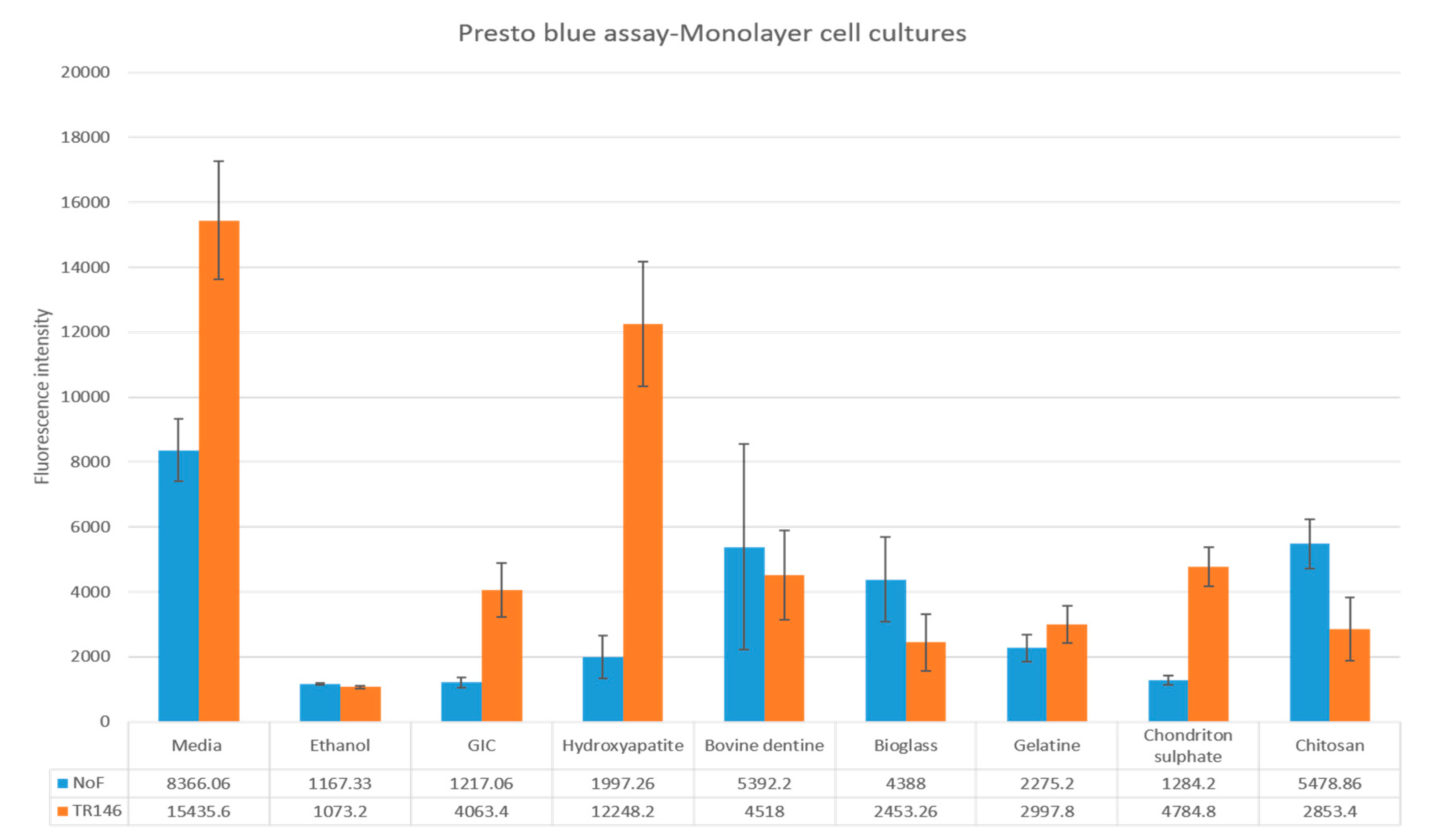
3.2.1. NOF Monolayer Viability Assay
3.2.2. TR146 Monolayer Viability Assay
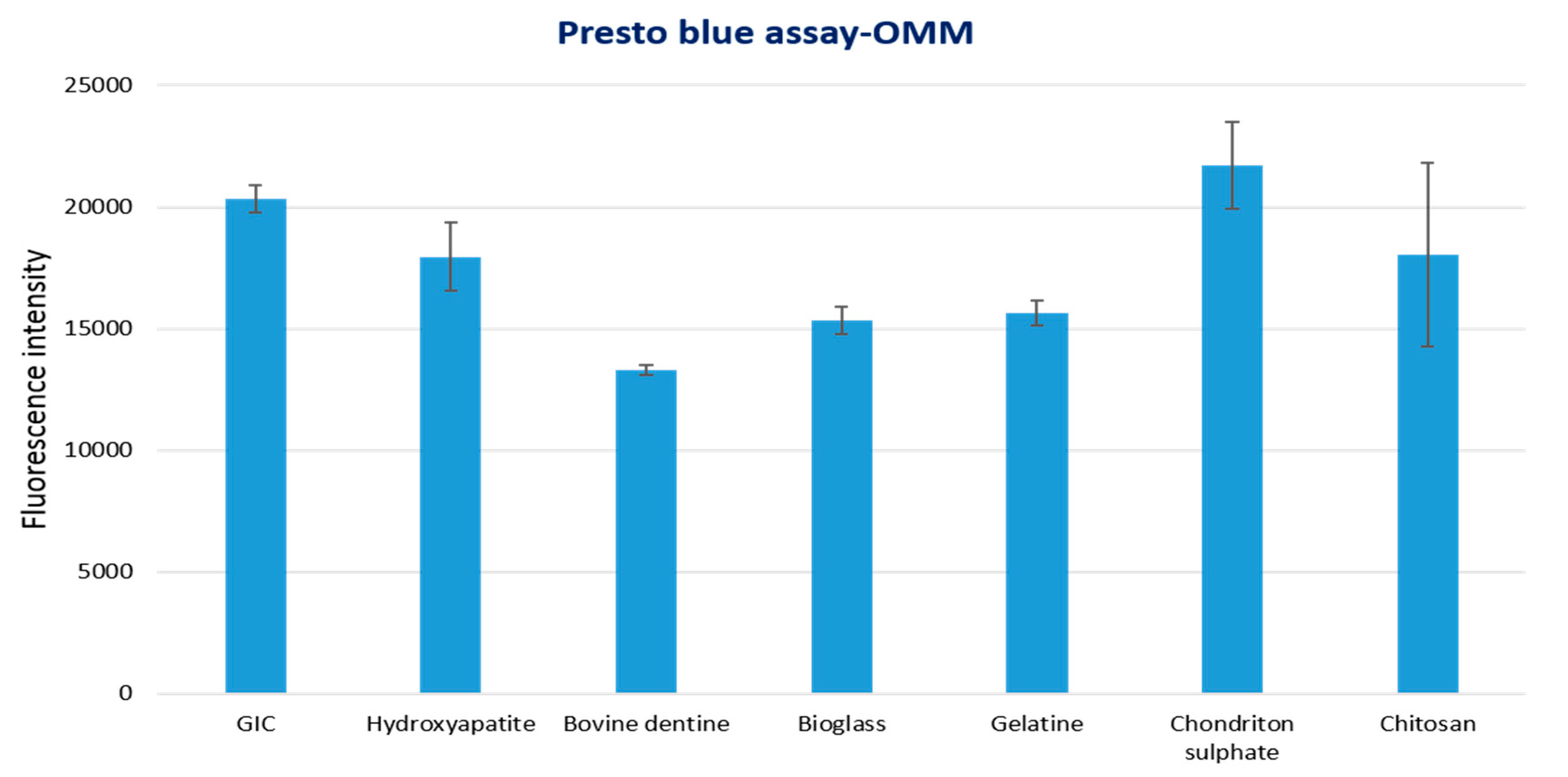
3.2.3. 3D-OMM Model Tissue Viability Assay
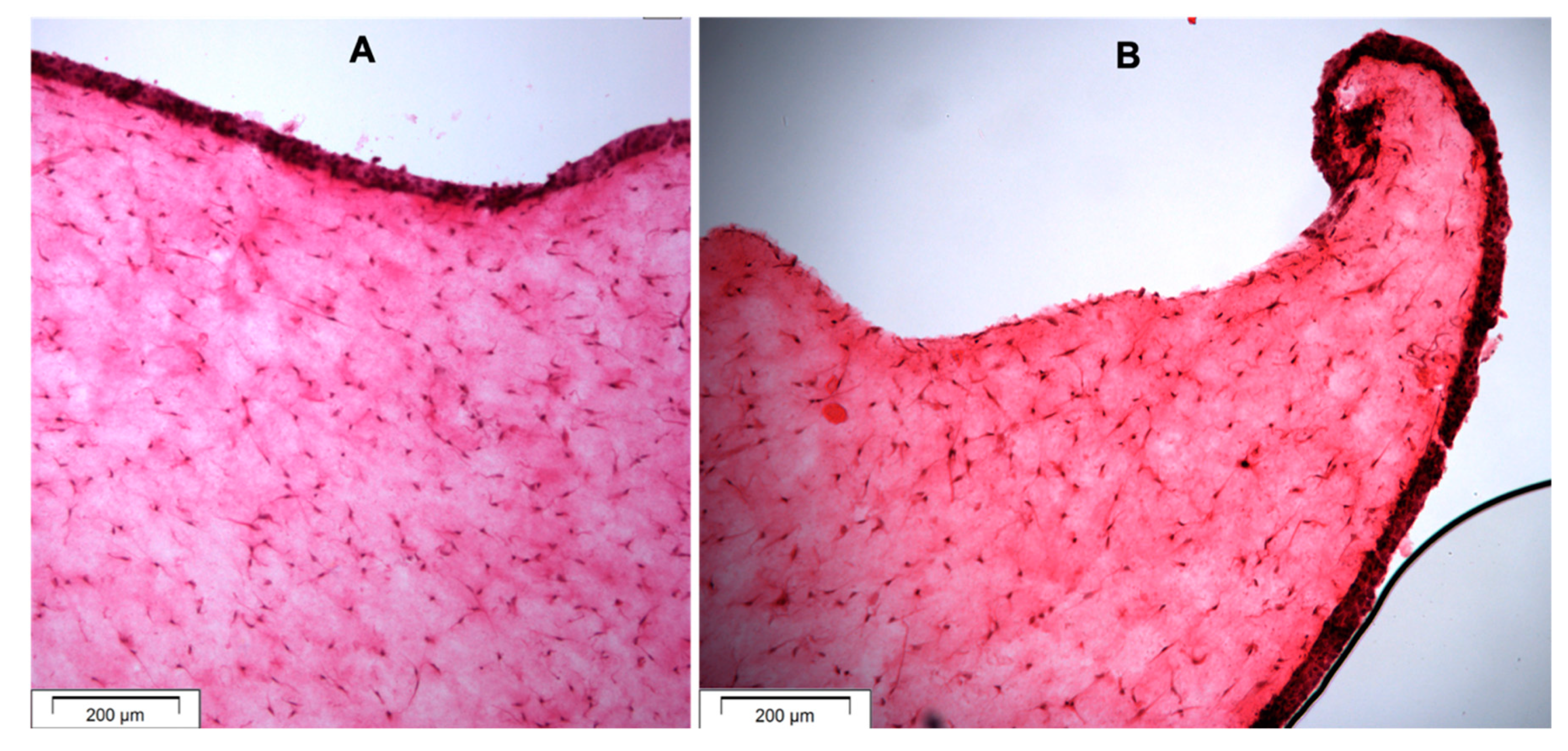
3.2.4. Histological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chi, D.L.; Berg, J.H.; Kim, A.S.; Scott, J. Northwest Practice-Based Research Collaborative in Evidence-Based Dentistry. Correlates of root caries experience in middle-aged and older adults in the northwest practice-based research collaborative in evidence-based dentistry research network. J. Am. Dent. Assoc. 2013, 144, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.O.; Griffin, P.M.; Swann, J.L.; Zlobin, N. Estimating rates of new root caries in older adults. J. Dent. Res. 2004, 83, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Stewardson, D.; Creanor, S.; Thornley, P.; Bigg, T.; Bromage, C.; Browne, A.; Cottam, D.; Dalby, D.; Gilmour, J.; Horton, J.; et al. The survival of Class V restorations in general dental practice: Part 3, five-year survival. Br. Dent. J. 2012, 212, E14. [Google Scholar] [CrossRef] [PubMed]
- Van Dijken, J.W.; Pallesen, U. Long-term dentin retention of etch-and-rinse and self-etch adhesives and a resin-modified glass ionomer cement in non-carious cervical lesions. Dent. Mater. 2008, 24, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Peumans, M.; De Munck, J.; Mine, A.; Van Meerbeek, B. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dent. Mater. 2014, 30, 1089–1103. [Google Scholar] [CrossRef] [PubMed]
- Heintze, S.D.; Ruffieux, C.; Rousson, V. Clinical performance of cervical restorations—A meta-analysis. Dent. Mater. 2010, 26, 993–1000. [Google Scholar] [CrossRef]
- Shubhashini, N.; Meena, N.; Ashish Shetty, A.K.; Naveen, D.N. Finite element analysis of stress concentration in Class V restorations of four groups of restorative materials in mandibular premolar. J. Conserve. Dent. JCD 2008, 11, 121–126. [Google Scholar]
- Yannas, I.V.; Burke, J.F.; Orgill, D.P.; Skrabut, E.M. Wound tissue can utilize a polymeric template to synthesize a functional extension of skin. Science 1982, 215, 174–176. [Google Scholar] [CrossRef]
- Heintze, S.D.; Rousson, V. Clinical effectiveness of direct class II restorations-a meta-analysis. J. Adhes. Dent. 2012, 14, 407–431. [Google Scholar]
- Giachetti, L.; Scaminaci Russo, D.; Bambi, C.; Grandini, R. A review of polymerization shrinkage stress: Current techniques for posterior direct resin restorations. J. Contemp. Dent. Pract. 2006, 7, 79–88. [Google Scholar] [CrossRef]
- Moharamzadeh, K.; Van Noort, R.; Brook, I.M.; Scutt, A.M. Cytotoxicity of resin monomers on human gingival fibroblasts and HaCaT keratinocytes. Dent. Mater. 2007, 23, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Moharamzadeh, K.; Brook, I.M.; Scutt, A.M.; Thornhill, M.H.; Van Noort, R. Mucotoxicity of dental composite resins on a tissue-engineered human oral mucosal model. J. Dent. 2008, 36, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Yan, F.; Xiao, Y.; Li, H.; Haase, H.; Bartold, P.M. A comparison of the effects of two kinds of glass-ionomer cement on human gingival fibroblast attachment, proliferation and morphology in vitro. J. Int. Acad. Periodontol. 2000, 2, 14–18. [Google Scholar] [PubMed]
- Subbarao, C.; Neelakantan, P.; Subbarao, C.V. In vitro biocompatibility tests of glass ionomer cements impregnated with collagen or bioactive glass to fibroblasts. J. Clin. Pediatric Dent. 2012, 36, 269–274. [Google Scholar] [CrossRef]
- Balto, H.A. Attachment and morphological behavior of human periodontal ligament fibroblasts to mineral trioxide aggregate: A scanning electron microscope study. J. Endod. 2004, 30, 25–29. [Google Scholar] [CrossRef]
- Czarnecka, B.; Deręgowska-Nosowicz, P.; Limanowska-Shaw, H.; Nicholson, J.W. Shear bond strengths of glass-ionomer cements to sound and to prepared carious dentine. J. Mater. Sci. Mater. Med. 2007, 18, 845–849. [Google Scholar] [CrossRef]
- Rodriguez, I.A.; Rozas Ferrara, C.A.; Campos-Sanchez, F.; Alaminos, M.; Uribe Echevarría, J.; Campos, A. An in vitro biocompatibility study of conventional and resin-modified glass ionomer cements. J. Adhes. Dent. 2013, 15, 541–546. [Google Scholar]
- Mickenautsch, S.; Mount, G.; Yengopal, V. Therapeutic effect of glass-ionomers: An overview of evidence. Aust. Dent. J. 2011, 56, 10–15. [Google Scholar] [CrossRef]
- Sidhu, S.K.; Carrick, T.E.; McCabe, J.F. Temperature mediated coefficient of dimensional change of dental tooth-colored restorative materials. Dent. Mater. 2004, 20, 435–440. [Google Scholar] [CrossRef]
- Van Noort, R. Introduction to Dental Materials, 4th ed.; Elsevier Health Sciences: London, UK, 2013. [Google Scholar]
- Heintze, S.D.; Roulet, J.F. Glass ionomer derivates have better retention rates in cervical restorations compared to self-etching adhesive systems. J. Evid. Based Dent. Pract. 2010, 10, 18–20. [Google Scholar] [CrossRef]
- Moharamzadeh, K.; Brook, I.M.; Van Noort, R.; Scutt, A.M.; Smith, K.G.; Thornhill, M.H. Development, optimization and characterization of a full-thickness tissue engineered human oral mucosal model for biological assessment of dental biomaterials. J. Mater. Sci. Mater. Med. 2008, 19, 1793–1801. [Google Scholar] [CrossRef] [PubMed]
- Chai, W.L.; Moharamzadeh, K.; Brook, I.M.; Emanuelsson, L.; Palmquist, A.; van Noort, R. Development of a novel model for the investigation of implant–soft tissue interface. J. Periodontol. 2010, 81, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Moharamzadeh, K.; Freeman, C.; Blackwood, K. Processed bovine dentine as a bone substitute. Br. J. Oral Maxillofac. Surg. 2008, 46, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.S.; Ravikumar, N.; Kavitha, S.; Mahalaxmi, S.; Jayasree, R.; Kumar, T.S.; Haneesh, M. Nanochitosan modified glass ionomer cement with enhanced mechanical properties and fluoride release. Int. J. Boil. Macromol. 2017, 104, 1860–1865. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Cai, Y.; Engqvist, H.; Xia, W. Enhanced bioactivity of glass ionomer cement by incorporating calcium silicates. Biomatter 2016, 6, e1123842. [Google Scholar] [CrossRef]
- Fathi, H.; Johnson, A.; Van Noort, R.; Ward, J.M. The influence of calcium fluoride (CaF2) on biaxial flexural strength of apatite-mullite glass-ceramic materials. Dent. Mater. 2005, 21, 846–851. [Google Scholar] [CrossRef]
- Johnson, A.; Shareef, M.Y.; Van Noort, R.; Walsh, J.M. Effect of furnace type and ceramming heat treatment conditions on the biaxial flexural strength of a canasite glass-ceramic. Dent. Mater. 2000, 16, 280–284. [Google Scholar] [CrossRef]
- Almela, T.; Brook, I.M.; Moharamzadeh, K. Development of three-dimensional tissue engineered bone-oral mucosal composite models. J. Mater. Sci. Mater. Med. 2016, 27, 65. [Google Scholar] [CrossRef]
- Tayebi, L.; Moharamzadeh, K. (Eds.) Biomaterials for Oral and Dental Tissue Engineering; Woodhead: Duxford, UK, 2017; pp. 3–18. [Google Scholar]
- Prosser, H.J.; Powis, D.R.; Wilson, A.D. Glass-ionomer cements of improved flexural strength. J. Dent. Res. 1986, 65, 146–148. [Google Scholar] [CrossRef]
- Xie, D.; Brantley, W.A.; Culbertson, B.M.; Wang, G. Mechanical properties and microstructures of glass-ionomer cements. Dent. Mater. 2000, 16, 129–138. [Google Scholar] [CrossRef]
- Yap, A.U.; Wang, X.; Wu, X.; Chung, S.M. Comparative hardness and modulus of tooth-colored restoratives: A depth-sensing microindentation study. Biomaterials 2004, 25, 2179–2185. [Google Scholar] [CrossRef] [PubMed]
- Yip, H.K.; Smales, R.J.; Ngo, H.C.; Tay, F.R.; Chu, F.C. Selection of restorative materials for the atraumatic restorative treatment (ART) approach: A review. Spec. Care Dent. 2001, 21, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Bali, P.; Prabhakar, A.R.; Basappa, N. An in vitro comparative evaluation of compressive strength and antibacterial activity of conventional GIC and hydroxyapatite reinforced GIC in different storage media. J. Clin. Diagn. Res. 2015, 9, ZC51–ZC55. [Google Scholar] [PubMed]
- Arita, K.; Yamamoto, A.; Shinonaga, Y.; Harada, K.; Abe, Y.; Nakagawa, K.; Sugiyama, S. Hydroxyapatite particle characteristics influence the enhancement of the mechanical and chemical properties of conventional restorative glass ionomer cement. Dent. Mater. J. 2011, 30, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Alatawi, R.A.; Elsayed, N.H.; Mohamed, W.S. Influence of hydroxyapatite nanoparticles on the properties of glass ionomer cement. J. Mater. Res. Technol. 2019, 8, 344–349. [Google Scholar] [CrossRef]
- De Caluwé, T.; Vercruysse, C.W.; Ladik, I.; Convents, R.; Declercq, H.; Martens, L.C.; Verbeeck, R.M. Addition of bioactive glass to glass ionomer cements: Effect on the physico-chemical properties and biocompatibility. Dent. Mater. 2017, 33, e186–e203. [Google Scholar] [CrossRef]
- Berrington, D. Viability reagent, prestoblue, in comparison with other available reagents, utilized in cytotoxicity and antimicrobial assays. Int. J. Microbiol. 2013, 2013, 420601. [Google Scholar]
- Choi, Y.S.; Hong, S.R.; Lee, Y.M.; Song, K.W.; Park, M.H.; Nam, Y.S. Study on gelatin-containing artificial skin: I. Preparation and characteristics of novel gelatin-alginate sponge. Biomaterials 1999, 20, 409–417. [Google Scholar] [CrossRef]
- Hong, S.R.; Lee, S.J.; Shim, J.W.; Choi, Y.S.; Lee, Y.M.; Song, K.W.; Park, M.H.; Nam, Y.S.; Lee, S.I. Study on gelatin-containing artificial skin IV: A comparative study on the effect of antibiotic and EGF on cell proliferation during epidermal healing. Biomaterials 2001, 22, 2777–2783. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Working Time (Minutes) | Setting Time (Minutes) | BFS (MPa) | Hardness (MPa) | Compressive Strength (MPa) | |
|---|---|---|---|---|---|
| GIC | 5.1 (0.5) | 1.6 (0.5) | 33.1 (6.8) | 49.5 (6.8) | 112.3 (17.1) |
| Hydroxyapatite | 6.6 (0.5) | 1.6 (0.4) | 31.4 (5.1) | 52.6 (13.1) | 129.5 (26.5) |
| Bovine dentine | 5.9 (0.5) | 1.7 (0.3) | 31.0 (4.0) | 47.9 (13.9) | 111.3 (25.9) |
| Bioglass | 6.7 * (1.2) | 2.0 (0.3) | 32.0 (2.1) | 46.3 (15.6) | 91.0 (14.9) |
| Gelatine | 6.0 (0.3) | 2.4 (0.5) | 21.8 (6.3) | 41.4 (18.7) | 44.2 * (16.6) |
| Chondroitin sulphate | 6.2 (0.7) | 2.2 (0.8) | 35.0 (4.4) | 37.5 (11.8) | 50.5 * (10.8) |
| Chitosan | 4.9 (0.3) | 1.2 (0.3) | 35.0 (4.4) | 49.1 (23.3) | 97.1 (14.7) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Binaljadm, T.; Moorehead, R.; Almela, T.; Franklin, K.; Tayebi, L.; Moharamzadeh, K. Biomodification of a Class-V Restorative Material by Incorporation of Bioactive Agents. Dent. J. 2019, 7, 110. https://doi.org/10.3390/dj7040110
Binaljadm T, Moorehead R, Almela T, Franklin K, Tayebi L, Moharamzadeh K. Biomodification of a Class-V Restorative Material by Incorporation of Bioactive Agents. Dentistry Journal. 2019; 7(4):110. https://doi.org/10.3390/dj7040110
Chicago/Turabian StyleBinaljadm, Tahani, Robert Moorehead, Thafar Almela, Kirsty Franklin, Lobat Tayebi, and Keyvan Moharamzadeh. 2019. "Biomodification of a Class-V Restorative Material by Incorporation of Bioactive Agents" Dentistry Journal 7, no. 4: 110. https://doi.org/10.3390/dj7040110
APA StyleBinaljadm, T., Moorehead, R., Almela, T., Franklin, K., Tayebi, L., & Moharamzadeh, K. (2019). Biomodification of a Class-V Restorative Material by Incorporation of Bioactive Agents. Dentistry Journal, 7(4), 110. https://doi.org/10.3390/dj7040110