Inspection of the Microbiota in Endodontic Lesions

 ,
,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
- Inclusion criteria: All scientific studies or systematic reviews investigating the bacterial associations with persistent endodontic lesions where the bacterial identification method was clearly described (PCR 16s rDNA, PCR 16s rRNA, test culture) were considered, with priority given to the most recent and updated studies. The most appropriate scientific studies on the oral microbiota in healthy tissues were identified using the most exhaustive and updated systematic revision present in the literature.
- Exclusion criteria: All articles that only considered the microbiological aspects of endodontics in a marginal way were excluded, along with case reports.
3. Results
4. Discussion
4.1. Penetration and Invasion of the Endodontic Space
4.2. Microbiological Differences between Bacterial Flora in Endodontically Treated Canals and in Untreated Canals
4.3. Gut Microbiome Inside the Oral Cavity. A Possible Explanation
4.4. The Role of Enterococcus Faecalis in Chronic Apical Periodontitis
5. Conclusions
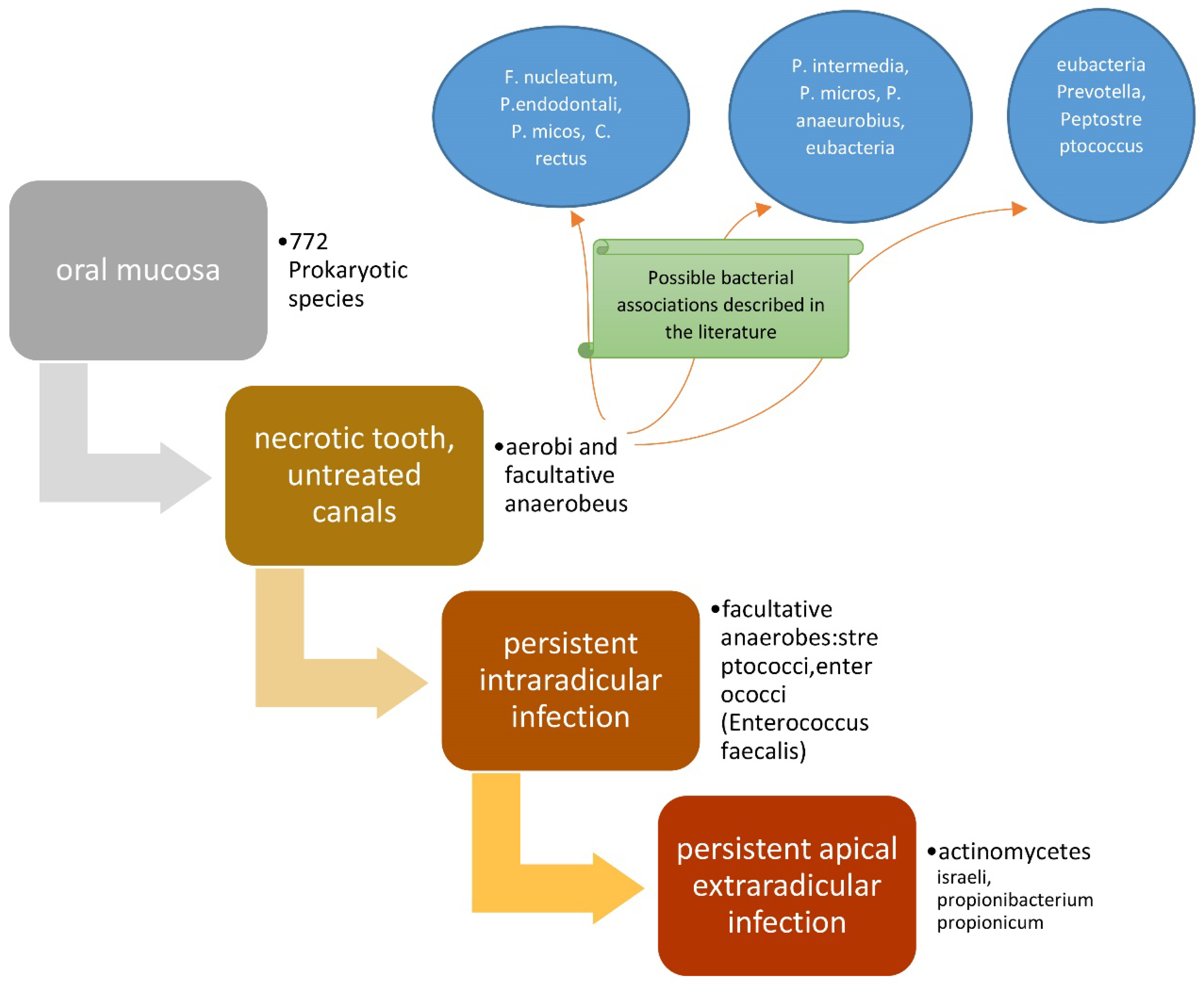
- Several microbes can be identified depending on the health status of the tooth (caries, pulpitis, necrotic tooth, acute/chronic parodontitis, persistent extra/intra-radicular infections);
- In endodontic failures, the most involved bacterial species are facultative anaerobes with predominance in recurrent forms of apical periodontitis of Enterococcus faecalis;
- In persistent extra-radicular infections, the bacteria mainly involved are A. israeli and Propionibacterium propionicum;
- The presence of intestinal microbiome in the oral cavity and consequently inside the tooth is due to food contamination by enterococci.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saito, D.; Leonardo Rde, T.; Rodrigues, J.L.; Tsai, S.M.; Hofling, J.F.; Goncalves, R.B. Identification of bacteria in endodontic infections by sequence analysis of 16S rDNA clone libraries. J. Med. Microbiol. 2006, 55, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi, M.; Troiano, G.; Laino, L.; Lo Russo, L.; Giannatempo, G.; Lauritano, F.; Cicciu, M.; Lo Muzio, L. ProTaper and WaveOne systems three-dimensional comparison of device parameters after the shaping technique. A micro-CT study on simulated root canals. Int. J. Clin. Exp. Med. 2015, 8, 17830–17834. [Google Scholar] [PubMed]
- Troiano, G.; Dioguardi, M.; Cocco, A.; Zhurakivska, K.; Ciavarella, D.; Muzio, L.L. Increase the glyde path diameter improves the centering ability of F6 Skytaper. Eur. J. Dent. 2018, 12, 89–93. [Google Scholar] [CrossRef]
- Troiano, G.; Dioguardi, M.; Cocco, A.; Giannatempo, G.; Laino, L.; Ciavarella, D.; Berutti, E.; Lo Muzio, L. Influence of Operator’s Experience on the Shaping Ability of Protaper Universal and Waveone Systems: A Comparative Study on Simulated Root Canals. Open Dent. J. 2016, 10, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Buonavoglia, A.; Lauritano, D.; Perrone, D.; Ardito, F.; Troiano, G.; Dioguardi, M.; Candotto, V.; Silvestre, F.J.; Lo Muzio, L. Evaluation of chemical-physical properties and cytocompatibility of TheraCal LC. J. Biol. Regul. Homeost. Agents 2017, 31, 1–9. [Google Scholar] [PubMed]
- Troiano, G.; Perrone, D.; Dioguardi, M.; Buonavoglia, A.; Ardito, F.; Lo Muzio, L. In vitro evaluation of the cytotoxic activity of three epoxy resin-based endodontic sealers. Dent. Mater. J. 2018, 37, 374–378. [Google Scholar] [CrossRef]
- Assed, S.; Ito, I.Y.; Leonardo, M.R.; Silva, L.A.; Lopatin, D.E. Anaerobic microorganisms in root canals of human teeth with chronic apical periodontitis detected by indirect immunofluorescence. Endod. Dent. Traumatol. 1996, 12, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Swimberghe, R.C.D.; Coenye, T.; De Moor, R.J.G.; Meire, M.A. Biofilm model systems for root canal disinfection: A literature review. Int. Endod. J. 2018, 52. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi, M.; Di Gioia, G.; Illuzzi, G.; Laneve, E.; Cocco, A.; Troiano, G. Endodontic irrigants: Different methods to improve efficacy and related problems. Eur. J. Dent. 2018, 12, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi, M.; Perrone, D.; Troiano, G.; Laino, L.; Ardito, F.; Lauritano, F.; Cicciu, M.; Muzio, L.L. Cytotoxicity evaluation of five different dual-cured resin cements used for fiber posts cementation. Int. J. Clin. Exp. Med. 2015, 8, 9327–9333. [Google Scholar]
- Chevalier, M.; Ranque, S.; Precheur, I. Oral fungal-bacterial biofilm models in vitro: A review. Med. Mycol. 2018, 56, 653–667. [Google Scholar] [CrossRef]
- Ducret, M.; Fabre, H.; Celle, A.; Mallein-Gerin, F.; Perrier-Groult, E.; Alliot-Licht, B.; Farges, J.C. Current challenges in human tooth revitalization. Biomed. Mater. Eng. 2017, 28, S159–S168. [Google Scholar] [CrossRef]
- Haapasalo, M.; Orstavik, D. In vitro infection and disinfection of dentinal tubules. J. Dent. Res. 1987, 66, 1375–1379. [Google Scholar] [CrossRef] [PubMed]
- Braz-Silva, P.H.; Bergamini, M.L.; Mardegan, A.P.; De Rosa, C.S.; Hasseus, B.; Jonasson, P. Inflammatory profile of chronic apical periodontitis: A literature review. Acta Odontol. Scand. 2019, 77, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Parhizkar, A.; Nojehdehian, H.; Asgary, S. Triple antibiotic paste: Momentous roles and applications in endodontics: A review. Restor. Dent. Endod. 2018, 43, e28. [Google Scholar] [CrossRef]
- Trusewicz, M.; Buczkowska-Radlinska, J.; Giedrys-Kalemba, S. The effectiveness of some methods in eliminating bacteria from the root canal of a tooth with chronic apical periodontitis. Ann. Acad. Med. Stetin. 2005, 51, 43–48. [Google Scholar] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Verma, D.; Garg, P.K.; Dubey, A.K. Insights into the human oral microbiome. Arch. Microbiol. 2018, 200, 525–540. [Google Scholar] [CrossRef]
- Hirai, K.; Tagami, A.; Okuda, K. Isolation and classification of anaerobic bacteria from pulp cavities of nonvital teeth in man. Bull. Tokyo Dent. Coll. 1991, 32, 95–98. [Google Scholar]
- Grenier, D.; Mayrand, D. Nutritional relationships between oral bacteria. Infect. Immun. 1986, 53, 616–620. [Google Scholar]
- Foster, K.R.; Bell, T. Competition, not cooperation, dominates interactions among culturable microbial species. Curr. Biol. 2012, 22, 1845–1850. [Google Scholar] [CrossRef] [PubMed]
- Kwang, S.; Abbott, P. The presence and distribution of bacteria in dentinal tubules of root filled teeth. Int. Endod. J. 2014, 47, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Love, R.M.; Jenkinson, H.F. Invasion of dentinal tubules by oral bacteria. Crit. Rev. Oral Biol. Med. 2002, 13, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Siqueira, J.F., Jr.; Loghin, S.; Berman, L.H. The cracked tooth: Histopathologic and histobacteriologic aspects. J. Endod. 2015, 41, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Fabricius, L.; Dahlen, G.; Ohman, A.E.; Moller, A.J. Predominant indigenous oral bacteria isolated from infected root canals after varied times of closure. Scand. J. Dent. Res. 1982, 90, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Sundqvist, G. Taxonomy, ecology, and pathogenicity of the root canal flora. Oral Surg. Oral Med. Oral Pathol. 1994, 78, 522–530. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rocas, I.N.; Alves, F.R.; Silva, M.G. Bacteria in the apical root canal of teeth with primary apical periodontitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 721–726. [Google Scholar] [CrossRef]
- Chavez de Paz, L.E.; Hamilton, I.R.; Svensater, G. Oral bacteria in biofilms exhibit slow reactivation from nutrient deprivation. Microbiology 2008, 154, 1927–1938. [Google Scholar] [CrossRef]
- Ingar, O. Open access to oral microbiology. J. Oral Microbiol. 2009, 1. [Google Scholar] [CrossRef]
- Fouad, A.F.; Kum, K.Y.; Clawson, M.L.; Barry, J.; Abenoja, C.; Zhu, Q.; Caimano, M.; Radolf, J.D. Molecular characterization of the presence of Eubacterium spp and Streptococcus spp in endodontic infections. Oral Microbiol. Immunol. 2003, 18, 249–255. [Google Scholar] [CrossRef]
- Narayanan, L.L.; Vaishnavi, C. Endodontic microbiology. J. Conserv. Dent. 2010, 13, 233–239. [Google Scholar] [CrossRef]
- Love, R.M. Bacterial adhesins—Their role in tubule invasion and endodontic disease. Aust. Endod. J. 2002, 28, 25–28. [Google Scholar] [CrossRef]
- Venkatesan, N.; Perumal, G.; Doble, M. Bacterial resistance in biofilm-associated bacteria. Future Microbiol. 2015, 10, 1743–1750. [Google Scholar] [CrossRef]
- Al-Ahmad, A.; Ameen, H.; Pelz, K.; Karygianni, L.; Wittmer, A.; Anderson, A.C.; Spitzmuller, B.; Hellwig, E. Antibiotic resistance and capacity for biofilm formation of different bacteria isolated from endodontic infections associated with root-filled teeth. J. Endod. 2014, 40, 223–230. [Google Scholar] [CrossRef]
- Raslan, N.; Mansour, O.; Assfoura, L. Evaluation of antibiotic mix in Non-instrumentation Endodontic Treatment of necrotic primary molars. Eur. J. Paediatr. Dent. 2017, 18, 285–290. [Google Scholar] [CrossRef]
- Lee, L.W.; Lee, Y.L.; Hsiao, S.H.; Lin, H.P. Bacteria in the apical root canals of teeth with apical periodontitis. J. Formos. Med. Assoc. 2017, 116, 448–456. [Google Scholar] [CrossRef]
- Gomes, B.P.; Drucker, D.B.; Lilley, J.D. Positive and negative associations between bacterial species in dental root canals. Microbios 1994, 80, 231–243. [Google Scholar]
- Siqueira, J.F., Jr.; Rocas, I.N.; Souto, R.; de Uzeda, M.; Colombo, A.P. Actinomyces species, streptococci, and Enterococcus faecalis in primary root canal infections. J. Endod. 2002, 28, 168–172. [Google Scholar] [CrossRef]
- Ruviere, D.B.; Leonardo, M.R.; da Silva, L.A.; Ito, I.Y.; Nelson-Filho, P. Assessment of the microbiota in root canals of human primary teeth by checkerboard DNA-DNA hybridization. J. Dent. Child. 2007, 74, 118–123. [Google Scholar]
- Siqueira, J.F.; Rocas, I.N. Positive and negative bacterial associations involving Dialister pneumosintes in primary endodontic infections. J. Endod. 2003, 29, 438–441. [Google Scholar] [CrossRef]
- Guven, Y.; Ustun, N.; Aksakal, S.D.; Topcuoglu, N.; Aktoren, O.; Kulekci, G. Assessment of the endodontic microbiota of abscessed primary teeth using microarray technology. Indian J. Dent. Res. 2018, 29, 781–786. [Google Scholar] [CrossRef]
- Shin, J.M.; Luo, T.; Lee, K.H.; Guerreiro, D.; Botero, T.M.; McDonald, N.J.; Rickard, A.H. Deciphering Endodontic Microbial Communities by Next-generation Sequencing. J. Endod. 2018, 44, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Cheung, G.S.; Ho, M.W. Microbial flora of root canal-treated teeth associated with asymptomatic periapical radiolucent lesions. Oral Microbiol. Immunol. 2001, 16, 332–337. [Google Scholar] [CrossRef]
- Adib, V.; Spratt, D.; Ng, Y.L.; Gulabivala, K. Cultivable microbial flora associated with persistent periapical disease and coronal leakage after root canal treatment: A preliminary study. Int. Endod. J. 2004, 37, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Sanhueza, G.; Bello-Toledo, H.; Gonzalez-Rocha, G.; Goncalves, A.T.; Valenzuela, V.; Gallardo-Escarate, C. Metagenomic study of bacterial microbiota in persistent endodontic infections using Next-generation sequencing. Int. Endod. J. 2018, 51, 1336–1348. [Google Scholar] [CrossRef] [PubMed]
- Amaral, S.F.D.; Scaffa, P.M.C.; Rodrigues, R.D.S.; Nesadal, D.; Marques, M.M.; Nogueira, F.N.; Sobral, M.A.P. Dynamic Influence of pH on Metalloproteinase Activity in Human Coronal and Radicular Dentin. Caries Res. 2018, 52, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Siqueira, J.F., Jr. Fate of the tissue in lateral canals and apical ramifications in response to pathologic conditions and treatment procedures. J. Endod. 2010, 36. [Google Scholar] [CrossRef] [PubMed]
- Heling, I.; Rotstein, I. A persistent oronasal sinus tract of endodontic origin. J. Endod. 1989, 15, 132–134. [Google Scholar] [CrossRef]
- Taschieri, S.; Torretta, S.; Corbella, S.; Del Fabbro, M.; Francetti, L.; Lolato, A.; Capaccio, P. Pathophysiology of sinusitis of odontogenic origin. J. Investig. Clin. Dent. 2017, 8. [Google Scholar] [CrossRef]
- Brook, I. Sinusitis of odontogenic origin. Otolaryngol. Head Neck Surg. 2006, 135, 349–355. [Google Scholar] [CrossRef]
- Molander, A.; Reit, C.; Dahlen, G.; Kvist, T. Microbiological status of root-filled teeth with apical periodontitis. Int. Endod. J. 1998, 31. [Google Scholar] [CrossRef]
- Love, R.M. Enterococcus faecalis—A mechanism for its role in endodontic failure. Int. Endod. J. 2001, 34, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Sundqvist, G.; Figdor, D.; Persson, S.; Sjogren, U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 86–93. [Google Scholar] [CrossRef]
- Zehnder, M.; Guggenheim, B. The mysterious appearance of enterococci in filled root canals. Int. Endod. J. 2009, 42, 277–287. [Google Scholar] [CrossRef]
- Drucker, D.B.; Green, R.M. The relative cariogenicity of different streptococci in the gnotobiotic WAG/RIJ rat. Arch. Oral Biol. 1981, 26, 599–606. [Google Scholar] [CrossRef]
- Chestnutt, I.G.; MacFarlane, T.W.; Stephen, K.W. An in vitro investigation of the cariogenic potential of oral streptococci. Arch. Oral Biol. 1994, 39, 589–593. [Google Scholar] [CrossRef]
- Gold, O.G.; Jordan, H.V.; van Houte, J. The prevalence of enterococci in the human mouth and their pathogenicity in animal models. Arch. Oral Biol. 1975, 20, 473–477. [Google Scholar] [CrossRef]
- Chu, F.C.; Tsang, C.S.; Chow, T.W.; Samaranayake, L.P. Identification of cultivable microorganisms from primary endodontic infections with exposed and unexposed pulp space. J. Endod. 2005, 31, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D. Experimental bacterial anachoresis in dog dental pulps capped with calcium hydroxide. J. Endod. 1989, 15, 591–595. [Google Scholar] [CrossRef]
- Kaufman, B.; Spangberg, L.; Barry, J.; Fouad, A.F. Enterococcus spp. in endodontically treated teeth with and without periradicular lesions. J. Endod. 2005, 31, 851–856. [Google Scholar] [CrossRef]
- Sjogren, U.; Figdor, D.; Spangberg, L.; Sundqvist, G. The antimicrobial effect of calcium hydroxide as a short-term intracanal dressing. Int. Endod. J. 1991, 24, 119–125. [Google Scholar] [CrossRef]
- Franz, C.M.; Stiles, M.E.; Schleifer, K.H.; Holzapfel, W.H. Enterococci in foods—A conundrum for food safety. Int. J. Food Microbiol. 2003, 88, 105–122. [Google Scholar] [CrossRef]
- Fisher, K.; Phillips, C. The ecology, epidemiology and virulence of Enterococcus. Microbiology 2009, 155, 1749–1757. [Google Scholar] [CrossRef]
- Estrela, C.; Silva, J.A.; de Alencar, A.H.; Leles, C.R.; Decurcio, D.A. Efficacy of sodium hypochlorite and chlorhexidine against Enterococcus faecalis—A systematic review. J. Appl. Oral Sci. 2008, 16, 364–368. [Google Scholar] [CrossRef]
- Marashdeh, M.Q.; Gitalis, R.; Levesque, C.; Finer, Y. Endodontic pathogens possess collagenolytic properties that degrade human dentine collagen matrix. Int. Endod. J. 2019, 52, 416–423. [Google Scholar] [CrossRef]
- Kayaoglu, G.; Orstavik, D. Virulence factors of Enterococcus faecalis: Relationship to endodontic disease. Crit. Rev. Oral Biol. Med. 2004, 15, 308–320. [Google Scholar] [CrossRef]
- Gutmann, J.L.; Manjarres, V. Historical and Contemporary Perspectives on the Microbiological Aspects of Endodontics. Dent. J. 2018, 6, 49. [Google Scholar] [CrossRef]
- Stuart, C.H.; Schwartz, S.A.; Beeson, T.J.; Owatz, C.B. Enterococcus faecalis: Its role in root canal treatment failure and current concepts in retreatment. J. Endod. 2006, 32, 93–98. [Google Scholar] [CrossRef]
- Chercoles-Ruiz, A.; Sanchez-Torres, A.; Gay-Escoda, C. Endodontics, Endodontic Retreatment, and Apical Surgery Versus Tooth Extraction and Implant Placement: A Systematic Review. J. Endod. 2017, 43, 679–686. [Google Scholar] [CrossRef]
- Zhang, C.; Du, J.; Peng, Z. Correlation between Enterococcus faecalis and Persistent Intraradicular Infection Compared with Primary Intraradicular Infection: A Systematic Review. J. Endod. 2015, 41, 1207–1213. [Google Scholar] [CrossRef]
- Signoretti, F.G.; Endo, M.S.; Gomes, B.P.; Montagner, F.; Tosello, F.B.; Jacinto, R.C. Persistent extraradicular infection in root-filled asymptomatic human tooth: Scanning electron microscopic analysis and microbial investigation after apical microsurgery. J. Endod. 2011, 37, 1696–1700. [Google Scholar] [CrossRef]
- Ricucci, D.; Candeiro, G.T.; Bugea, C.; Siqueira, J.F., Jr. Complex Apical Intraradicular Infection and Extraradicular Mineralized Biofilms as the Cause of Wet Canals and Treatment Failure: Report of 2 Cases. J. Endod. 2016, 42, 509–515. [Google Scholar] [CrossRef]
- Xia, T.; Baumgartner, J.C. Occurrence of Actinomyces in infections of endodontic origin. J. Endod. 2003, 29, 549–552. [Google Scholar] [CrossRef]
- Grgurevic, J.; Ivanisevic Malcic, A.; Tambic Andrasevic, A.; Prpic Mehicic, G.; Kuzmac, S.; Jukic, S. Frequency of bacetrial content finding in persistant periapical lesions. Acta Stomatol. Croat. 2017, 51, 217–226. [Google Scholar] [CrossRef]
- Ricucci, D.; Lopes, W.S.P.; Loghin, S.; Rocas, I.N.; Siqueira, J.F., Jr. Large Bacterial Floc Causing an Independent Extraradicular Infection and Posttreatment Apical Periodontitis: A Case Report. J. Endod. 2018, 44, 1308–1316. [Google Scholar] [CrossRef]
- Rochd, T.; Calas, P.; Jabri, M.; Roques, C. Resistance to B-lactamines of bacteria responsible for endodontic root canal infections. Odontostomatol. Trop. 2010, 33, 25–33. [Google Scholar]



{kind=link}
{kind=link}
| Reviewer 2 | Reviewer 2 | Reviewer 2 | |||
|---|---|---|---|---|---|
| Include | Exclude | Unsure | Total | ||
| Reviewer 1 | Include | 9 | 0 | 0 | 9 |
| Reviewer 1 | Exclude | 3 | 268 | 10 | 281 |
| Reviewer 1 | Unsure | 0 | 25 | 35 | 60 |
| Total | 12 | 293 | 45 | 350 |
| Keywords | PubMed | Scopus |
|---|---|---|
| Persistent intra-radicular infection | 6 | 10 |
| Persistent extra-radicular infection | 13 | 2 |
| Endodontic treatment | 4183 | 5225 |
| Endodontic bacteria | 21 | 30 |
| Microbial endodontic | 756 | 0 |
| Endodontic failure | 157 | 290 |
| Total number of records | 5136 | 5557 |
| First Author, Date | Journal | Type of Study | Endodontic Diseases Associated with Bacteria Examined in the Study | Main Bacteria That Are Associated with Pathology Examined in the Study | Characteristics of the Main Bacteria Taken into Consideration | Identification Method |
|---|---|---|---|---|---|---|
| Verma, D., 2018 | Archives of microbiology | Review (data: The expanded Human Oral Microbiome Database) | Normal oral cavity | 772 prokaryotic species (96% six broad phyla: Firmicutes, Actinobacteria, Proteobacteria, Fusobacteria, Bacteroidetes, and Spirochaetes) | Gram-positive, Gram-negative, anaerobic and aerobic. | PCR 16S rDNA |
| Shin, J.M., 2018 | Journal of endodontics | Review (data: PubMed—Next Generation Sequencing Applications) | Necrotic teeth in untreated canals, pulpitis, primary endodontic infections |
|
| PCR 16S rRNA |
| Guven, Y., 2018 | Indian journal of dental research: Official publication of the Indian Society for Dental Research | Clinical study | Necrotic teeth, abscessed primary teeth, primary endodontic infections |
|
| PCR 16S rRNA |
| Siqueira, J.F., 2003 | Journal of endodontics | Clinical study | The necrotic tooth in untreated canals, primary endodontic infections |
|
| PCR 16S rDNA |
| Siqueira, J.F., 2002 | Journal of endodontics | Clinical study | Necrotic teeth in untreated canals, primary endodontic infections |
|
| PCR 16S rRNA |
| Love, R.M., 2001 | International endodontic journal | Clinical study | Persistent intra-radicular infection | Enterococcus faecalis | Gram-positive, facultative anaerobic | Culture |
| Molande, A., 1998 | International endodontic journal | Clinical study | Persistent intra-radicular infection |
|
| Culture |
| Xia, T., 2003 | Journal of endodontics | Clinical study | Persistent apical extra-radicular infection | Actinomycetes (A. israeli) | Gram-positive, anaerobic. | PCR 16S rRNA |
| Grgurevic, J., 2017 | Acta Stomatol Croat | Clinical study | Persistent apical extra-radicular infection | Propionibacterium propionicum | Gram-positive, anaerobic. | PCR 16S rRNA |
| Environment or Pathology | Type of Bacteria | Prevalent Bacteria That to Form the Microbiota |
|---|---|---|
| Oral mucosa | Gram-positive, Gram-negative, anaerobic and aerobic | 772 Prokaryotic species |
| Necrotic tooth, Untreated canals | Gram-positive, Gram-negative, anaerobic and aerobic | Eubacteria Prevotella intermedia Peptostreptococcus Fusobacterium Porphyromonas Parvimonas Streptococcus Campylobacter rectus Dialister pneumosintes Actinomyces species Enterococcus faecalis |
| Persistent intra-radicular infection | Gram-positive, facultative anaerobes | Streptococci Enterococci (Enterococcus faecalis) |
| Persistent extra-radicular infection | Gram-positive, anaerobic | Actinomycetes (A. israeli) Propionibacterium propionicum |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dioguardi, M.; Di Gioia, G.; Illuzzi, G.; Arena, C.; Caponio, V.C.A.; Caloro, G.A.; Zhurakivska, K.; Adipietro, I.; Troiano, G.; Lo Muzio, L. Inspection of the Microbiota in Endodontic Lesions. Dent. J. 2019, 7, 47. https://doi.org/10.3390/dj7020047
Dioguardi M, Di Gioia G, Illuzzi G, Arena C, Caponio VCA, Caloro GA, Zhurakivska K, Adipietro I, Troiano G, Lo Muzio L. Inspection of the Microbiota in Endodontic Lesions. Dentistry Journal. 2019; 7(2):47. https://doi.org/10.3390/dj7020047
Chicago/Turabian StyleDioguardi, Mario, Giovanni Di Gioia, Gaetano Illuzzi, Claudia Arena, Vito Carlo Alberto Caponio, Giorgia Apollonia Caloro, Khrystyna Zhurakivska, Iolanda Adipietro, Giuseppe Troiano, and Lorenzo Lo Muzio. 2019. "Inspection of the Microbiota in Endodontic Lesions" Dentistry Journal 7, no. 2: 47. https://doi.org/10.3390/dj7020047
APA StyleDioguardi, M., Di Gioia, G., Illuzzi, G., Arena, C., Caponio, V. C. A., Caloro, G. A., Zhurakivska, K., Adipietro, I., Troiano, G., & Lo Muzio, L. (2019). Inspection of the Microbiota in Endodontic Lesions. Dentistry Journal, 7(2), 47. https://doi.org/10.3390/dj7020047