Foreign-Trained Dentists in the United States: Challenges and Opportunities


Abstract
:1. Introduction
“Since I recognize that graduates of foreign dental schools, US citizens or not, might make a worthwhile contribution to dentistry in this country … Still we must be careful to uphold standards of US Dentistry—the best in the world—and, therefore, should take a good look at foreign-trained dentists to be sure they measure up our standards before granting them licensure”.[1]
2. Materials and Methods
3. Results
3.1. Study Selection
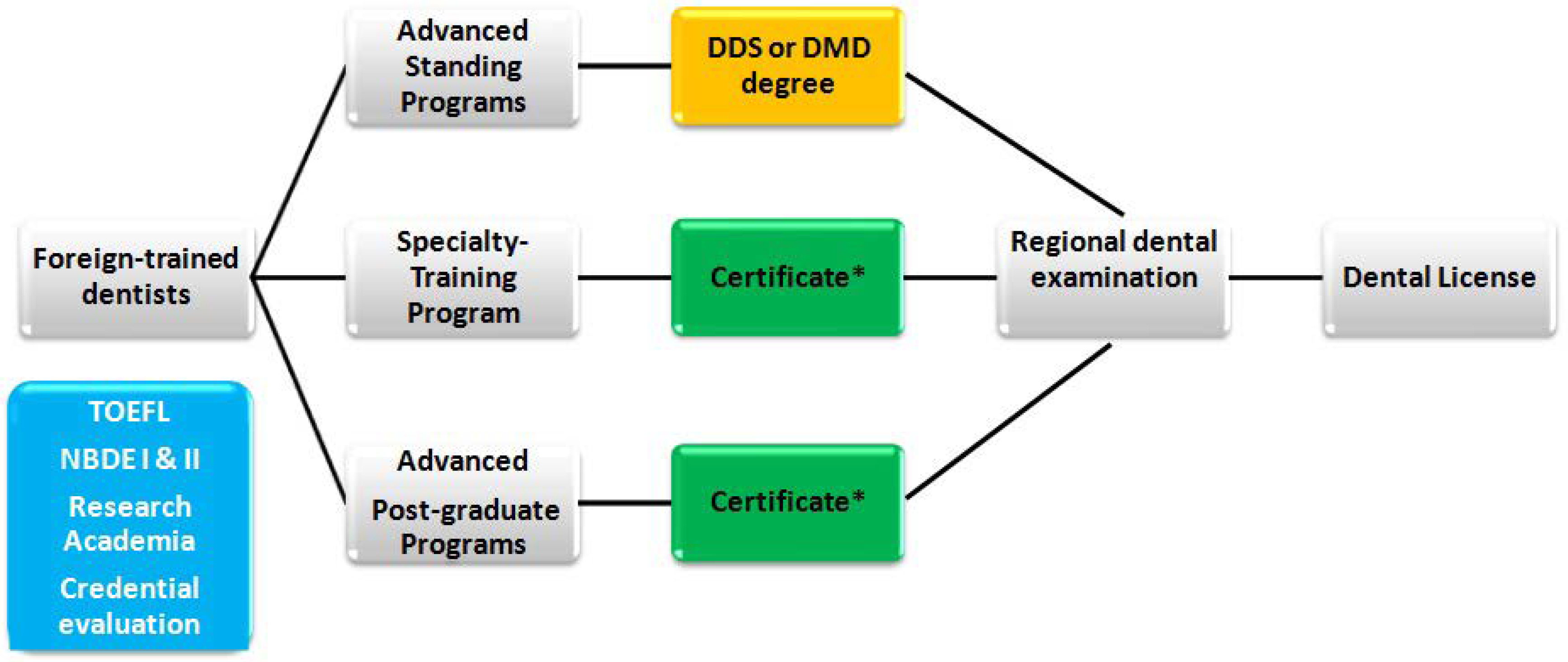
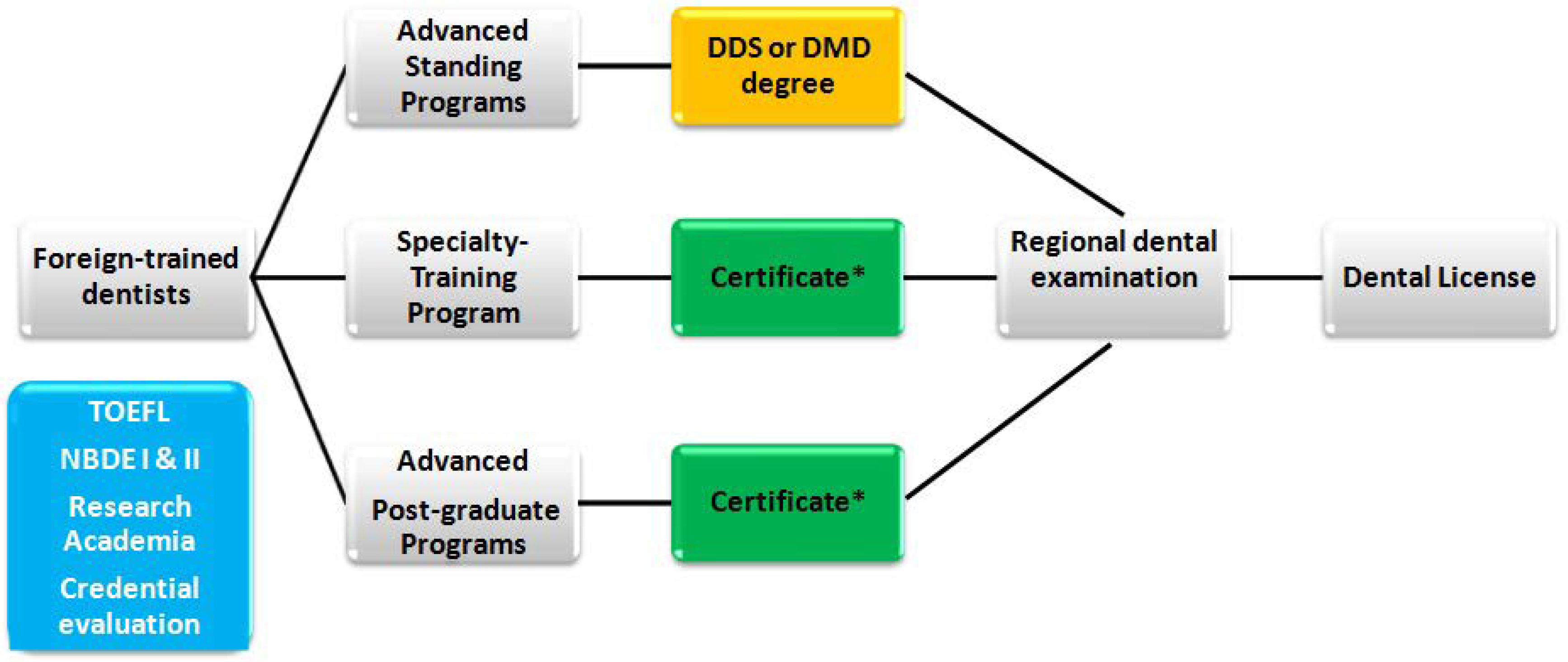
3.2. Pathway to Licensing
3.2.1. Advanced Standing Programs
3.2.2. Specialty Training Programs
3.2.3. Advanced Post-Graduate Education Programs
3.3. Challenges
3.3.1. Admission Process
3.3.2. Tuition Costs
3.3.3. Immigration Barriers
3.3.4. Cultural Differences
3.4. Opportunities
3.4.1. Underserved Communities
3.4.2. Diversity
3.4.3. Expertise and Experience
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Butts, H.C. Foreign-trained practitioners should meet our standards to be licensed [editiorial]. J. Am. Dent. Assoc. 1977, 94, 417. [Google Scholar] [PubMed]
- Rubin, M.K. Foreign-trained dentists—A problem in licensure. N. Y. State Dent. J. 1982, 48, 704. [Google Scholar] [PubMed]
- Welie, J.V. Is dentistry a profession? Part 2. The hallmarks of professionalism. J. Can. Dent. Assoc. 2004, 70, 599–602. [Google Scholar] [PubMed]
- Holmboe, E.S. Maintenance of certification, revalidation, and professional self-regulation. J. Contin. Educ. Health Prof. 2013, 33 (Suppl. S1), S63–S66. [Google Scholar] [CrossRef] [PubMed]
- Welie, J.V. Is dentistry a profession? Part 3. Future challenges. J. Can. Dent. Assoc. 2004, 70, 675–678. [Google Scholar] [PubMed]
- Welie, J.V. Is dentistry a profession? Part 1. Professionalism defined. J. Can. Dent. Assoc. 2004, 70, 529–532. [Google Scholar] [PubMed]
- Mertz, E.; Wides, C.; Cooke, A.; Gates, P.E. Tracking workforce diversity in dentistry: Importance, methods, and challenges. J. Public Health Dent. 2016, 76, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Sweis, L.E.; Guay, A.H. Foreign-trained dentists licensed in the United States: Exploring their origins. J. Am. Dent. Assoc. 2007, 138, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Boorberg, N.B.; Schonwetter, D.J.; Swain, V.L. Advanced placement, qualifying, and degree completion programs for internationally trained dentists in canada and the United States: An overview. J. Dent. Educ. 2009, 73, 399–415. [Google Scholar] [PubMed]
- Pannu, V.; Thompson, A.L.; Pannu, D.S.; Collins, M.A. Education for foreign-trained dentists in the United States: Currently available findings and need for further research. J. Dent. Educ. 2013, 77, 1521–1524. [Google Scholar] [PubMed]
- Pitigoi-Aron, G.; King, P.A.; Chambers, D.W. Predictors of academic performance for applicants to an international dental studies program in the United States. J. Dent. Educ. 2011, 75, 1577–1582. [Google Scholar] [PubMed]
- Rhodes, D. Transnational licensure: View from texas. J. Am. Coll. Dent. 2003, 70, 4–7. [Google Scholar] [PubMed]
- Rother, E.T. Systematic literature review x narrative review. Acta Paulista de Enfermagem 2007, 20, 5–6. [Google Scholar] [CrossRef]
- Garcia, R.I.; Blue Spruce, G.; Sinkford, J.C.; Lopez, M.J.; Sullivan, L.W. Workforce diversity in dentistry—Current status and future challenges. J. Public Health Dent. 2017, 77, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Aziz, S.R. Racial diversity in american oral and maxillofacial surgery. J. Oral Maxillofac. Surg. 2010, 68, 1723–1731. [Google Scholar] [CrossRef] [PubMed]
- Al-Sowygh, Z.H.; Sukotjo, C. Foreign-trained dentists in advanced education in prosthodontics programs in the United States: Demographics, perspectives on current training, and future goals. J. Prosthodont. 2011, 20, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Lacy, E.S.; McCann, A.L.; Miller, B.H.; Solomon, E.; Reuben, J.S. Achieving student diversity in dental schools: A model that works. J. Dent. Educ. 2012, 76, 523–533. [Google Scholar] [PubMed]
- Ramesh, A.; Ganguly, R.; Qualters, D.M. An interdisciplinary, team-based design for an oral and maxillofacial radiology course for postdoctoral dental students. J. Dent. Educ. 2014, 78, 1339–1345. [Google Scholar] [PubMed]
- Mertz, E.; Wides, C.; Calvo, J.; Gates, P. The hispanic and latino dentist workforce in the United States. J. Public Health Dent. 2017, 77, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Casamassimo, P.S.; Feigal, R.; Adair, S.M.; Berg, J.; Stewart, R. A snapshot of the U.S. Postdoctoral pediatric dentistry faculty workforce, 2002. J. Dent. Educ. 2004, 68, 823–828. [Google Scholar] [PubMed]
- Bazargan, N.; Chi, D.L.; Milgrom, P. Exploring the potential for foreign-trained dentists to address workforce shortages and improve access to dental care for vulnerable populations in the United States: A case study from washington state. BMC Health Serv. Res. 2010, 10, 336. [Google Scholar] [CrossRef] [PubMed]
- Allareddy, V.; Elangovan, S.; Nalliah, R.P.; Chickmagalur, N.; Allareddy, V. Pathways for foreign-trained dentists to pursue careers in the United States. J. Dent. Educ. 2014, 78, 1489–1496. [Google Scholar] [PubMed]
- Catalanotto, F.A. Expected changes in regulation and licensure: Influence on future education of dentists. J. Dent. Educ. 2017, 81, eS11–eS20. [Google Scholar] [CrossRef] [PubMed]
- Itaya, L.E.; Chambers, D.W.; King, P.A. Analyzing the influence of admissions criteria and cultural norms on success in an international dental studies program. J. Dent. Educ. 2008, 72, 317–328. [Google Scholar] [PubMed]
- Vujicic, M. Will we see more foreign-trained dentists in the United States? J. Am. Dent. Assoc. 2017, 148, 538–540. [Google Scholar] [CrossRef] [PubMed]
- National Matching Services Inc. Postdoctoral Dental Matching Program for Positions Beginning in 2018. Available online: https://www.natmatch.com/dentres/statistics.html (accessed on 6 June 2018).
- Redden, E. Fee for Being Foreign. Available online: https://www.insidehighered.com/news/2015/05/08/some-public-universities-are-charging-differentiated-tuition-rates-or-raising-fees (accessed on 6 June 2018).
- School of Dental Medicine, University of Colorado. International Student Program. Tuition and Financial Information. Available online: http://www.ucdenver.edu/academics/colleges/dentalmedicine/ProgramsAdmissions/InternationalStudentProgram/Pages/ISP.aspx (accessed on 6 June 2018).
- School of Dental Medicine, University of Buffalo. 2018–2019 Estimated Cost of Attendance. Available online: https://dental.buffalo.edu/education/dds-program/dds-program/international-dentist-program/costs--financial-aid-and-scholarships.html (accessed on 6 June 2018).
- Eastman Institute for Oral Health, University of Rochester. Advanced Education in General Dentistry. Available online: https://www.urmc.rochester.edu/dentistry/education/advanced-ed.aspx (accessed on 6 June 2018).
- U.S. Citizenship and Inmigration Services. H-1B Fiscal Year (FY) 2018 Cap Season. Available online: https://www.uscis.gov/working-united-states/temporary-workers/h-1b-specialty-occupations-and-fashion-models/h-1b-fiscal-year-fy-2018-cap-season (accessed on 6 June 2018).
- Lopez, N.; Berthold, P. Transnational licensure: Foreign dentists in america reclaim their profession through the program for advanced standing students (pass). J. Am. Coll. Dent. 2003, 70, 15–17. [Google Scholar] [PubMed]
- Okunseri, C.; Bajorunaite, R.; Abena, A.; Self, K.; Iacopino, A.M.; Flores, G. Racial/ethnic disparities in the acceptance of medicaid patients in dental practices. J. Public Health Dent. 2008, 68, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Komaromy, M.; Grumbach, K.; Drake, M.; Vranizan, K.; Lurie, N.; Keane, D.; Bindman, A.B. The role of black and hispanic physicians in providing health care for underserved populations. N. Engl. J. Med. 1996, 334, 1305–1310. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Articles Discussing Dental Workforce Diversity in the U.S. | |||
|---|---|---|---|
| Author | Publication Year | Journal | Aim of the Study |
| Casamassimo et al. [20] | 2004 | Journal of Dental Education | Describes the changes in pediatric dentistry faculty numbers and teaching loads between 1995 and 2002 for postdoctoral pediatric dentistry education. |
| Aziz [15] | 2010 | Journal of Oral and Maxillofacial Surgery | Reviews the racial demographic of American oral and maxillofacial surgery as it compares with the racial demographic of the U.S. |
| Bazargan et al. [21] | 2010 | BMC Health Services Research | Describes the potential impact of foreign-trained dentists have on improving access to dental care for vulnerable populations. |
| Al-Sowygh & Sukotjo [16] | 2011 | Journal of Prosthodontics | Reviews perspectives of foreign-trained dentists in comparison with U.S.-trained Dentists in Advanced Education in Prosthodontics programs on their current clinical training and future goals. |
| Lacy et al. [17] | 2012 | Journal of Dental Education | Describes an educational program implemented in Texas A & M Health Science Center Baylor College of Dentistry, to increase the number of underrepresented minorities dental students. |
| Ramesh et al. [18] | 2014 | Journal of Dental Education | Describes the transition of an oral and maxillofacial radiology course from a traditional lecture format to an interactive case-based, team-based, interdisciplinary, and intra-professional learning model in advanced dental education. |
| Mertz et al. [7] | 2016 | Journal of Public Health Dentistry | Describes sources of data on underrepresented minority dental providers in the U.S. |
| Garcia et al. [14] | 2017 | Journal of Public Health Dentistry | Reviews the underrepresented minority dentists in the U.S. workforce. |
| Mertz et al. [19] | 2017 | Journal of Public Health Dentistry | Describes the Hispanic/Latino dentist workforce in the U.S., their general practice patterns, and their contributions to oral health care for Hispanic and underserved patients. |
| Articles Discussing the Licensing Process for Foreign-Trained Dentists in the U.S. | |||
|---|---|---|---|
| Author | Publication Year | Journal | Aim of the Study |
| Butts [1] | 1977 | Journal of the American Dental Association | Reviews the concerns regarding the incorporation of foreign-trained dentists as dental providers in the U.S. |
| Rubin [2] | 1982 | The New York State Dental Journal | Reviews the concerns regarding the licensure process for foreign-trained dentists to practice clinical dentistry in the State of New York. |
| Sweis & Guay [8] | 2007 | Journal of the American Dental Association | Describes the origins of foreign-trained dentists seeking licensure in the U.S. |
| Itaya et al. [24] | 2008 | Journal of Dental Education | Describes the influence of admissions criteria and cultural norms on success in an international dental studies program |
| Boorberg et al. [9] | 2009 | Journal of Dental Education | Reviews the different types of programs available to foreign-trained dentists seeking to practice in either Canada or the U.S. |
| Pannu et al. [10] | 2013 | Journal of Dental Education | Reviews the current trends in education for foreign-trained dentists in the U.S. |
| Allaredy et al. [22] | 2014 | Journal of Dental Education | Reviews the different pathways for foreign-trained dentists to pursue career in the U.S. |
| Catalanotto [23] | 2017 | Journal of Dental Education | Reviews expected changes in regulation and licensure, and its influence on future education of dentists in the U.S. |
| Vujicic [25] | 2017 | Journal of the American Dental Association | Describes future perspectives for foreign-trained dentists in the U.S. |
| Year Training | Matched | Unmatched | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| GPR | AEGD | OMFS | PEDS | ORTHO | ANES | PERIO | PROS | ||||
| 2018 | U.S./Canada | 682 (97.7%) | 232 (95%) | 222 (99.5%) | 391 (96.7%) | 256 (90.4%) | 21 (100%) | 93 (66.4%) | 70 (60.8%) | 715 (26.6%) | 2682 |
| Non-U.S. | 16 (2.2%) | 12 (4.9%) | 1 (0.4%) | 13 (3.2%) | 27 (9.5%) | 0 (0%) | 47 (33.5%) | 45 (39.1%) | 362 (69.2%) | 523 | |
| 2017 | U.S./Canada | 716 (97.4%) | 243 (94.1%) | 216 (96.8%) | 384 (96.9%) | 255 (90.4%) | 27 (100%) | NA | NA | 733 (28.4%) | 2574 |
| Non-U.S. | 19 (2.5%) | 15 (5.8%) | 7 (3.1%) | 12 (3%) | 27 (9.5%) | 0 (0%) | 246 (75.4%) | 326 | |||
| 2016 | U.S. | 596 (95%) | 212 (89%) | 213 (96.3%) | 355 (93.9%) | 234 (90%) | 30 (93.7%) | NA | NA | 645 (28.2%) | 2285 |
| Non-U.S. | 31 (4.9%) | 26 (10.9%) | 8 (3.6%) | 23 (6%) | 26 (10%) | 2 (6.2%) | 221 (65.5%) | 337 | |||
| 2015 | U.S. | 591 (95.0%) | 182 (79.8%) | 209 (97.2%) | 359 (93.4%) | 237 (88.4%) | 22 (88%) | NA | NA | 639 (28.5%) | 2239 |
| Non-U.S. | 31 (4.9%) | 46 (20.1%) | 6 (2.7%) | 25 (6.5%) | 31 (11.5%) | 3 (12%) | 283 (66.5%) | 425 | |||
| 2014 | U.S. | 619 (95.6%) | 164 (84.1%) | 216 (96.8%) | 357 (95.9%) | 218 (86.1%) | 27 (87%) | NA | NA | 693 (30.2%) | 2294 |
| Non-U.S. | 28 (4.3%) | 31 (15.8%) | 7 (3.1%) | 15 (4%) | 35 (13.8%) | 4 (12.9%) | 285 (70.3%) | 405 | |||
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kellesarian, S.V. Foreign-Trained Dentists in the United States: Challenges and Opportunities. Dent. J. 2018, 6, 26. https://doi.org/10.3390/dj6030026
Kellesarian SV. Foreign-Trained Dentists in the United States: Challenges and Opportunities. Dentistry Journal. 2018; 6(3):26. https://doi.org/10.3390/dj6030026
Chicago/Turabian StyleKellesarian, Sergio Varela. 2018. "Foreign-Trained Dentists in the United States: Challenges and Opportunities" Dentistry Journal 6, no. 3: 26. https://doi.org/10.3390/dj6030026
APA StyleKellesarian, S. V. (2018). Foreign-Trained Dentists in the United States: Challenges and Opportunities. Dentistry Journal, 6(3), 26. https://doi.org/10.3390/dj6030026