1. Introduction
Although oral health is an inseparable part of total health, dental diseases are the most neglected of most prevalent chronic diseases [
1]. The increase of dental caries prevalence has been noted, especially in developing countries, which fall behind developed countries in preventing dental caries and protecting oral health [
2]. During the last decade, a significant increase in dental caries in Saudi children has been observed, which has been attributed to several factors, including [
3,
4]:
increased sugar consumption;
high consumption of carbonated soft drinks;
inadequate oral hygiene practices;
lack of organized prevention, promotion, and education programs; and
poor awareness to the importance of oral health in children.
This paper describes oral health among a group of children in a city in Saudi Arabia, a proposed community health intervention to improve the oral health, and an overview of a pilot phase program.
3. Risk Factors and Causal Theory
As a semi-urban area in northwestern Saudi Arabia, Tabuk has a population of 450,000. Thirty-eight percent of the population is under the age of 15. Children in Tabuk have the same risk factors, resultant nutritional problems, and health disorders, including dental caries, compared to other areas of Saudi Arabia [
3]. To formulate a conceptual framework to serve as a scaffold in oral health program planning, development, and evaluation, a thorough understanding of the factors contributing to oral health status is required, including social factors, cultural values and beliefs, dental workforce, and the current healthcare system. The mission of the program is to improve the oral health status of children in Tabuk, Saudi Arabia.
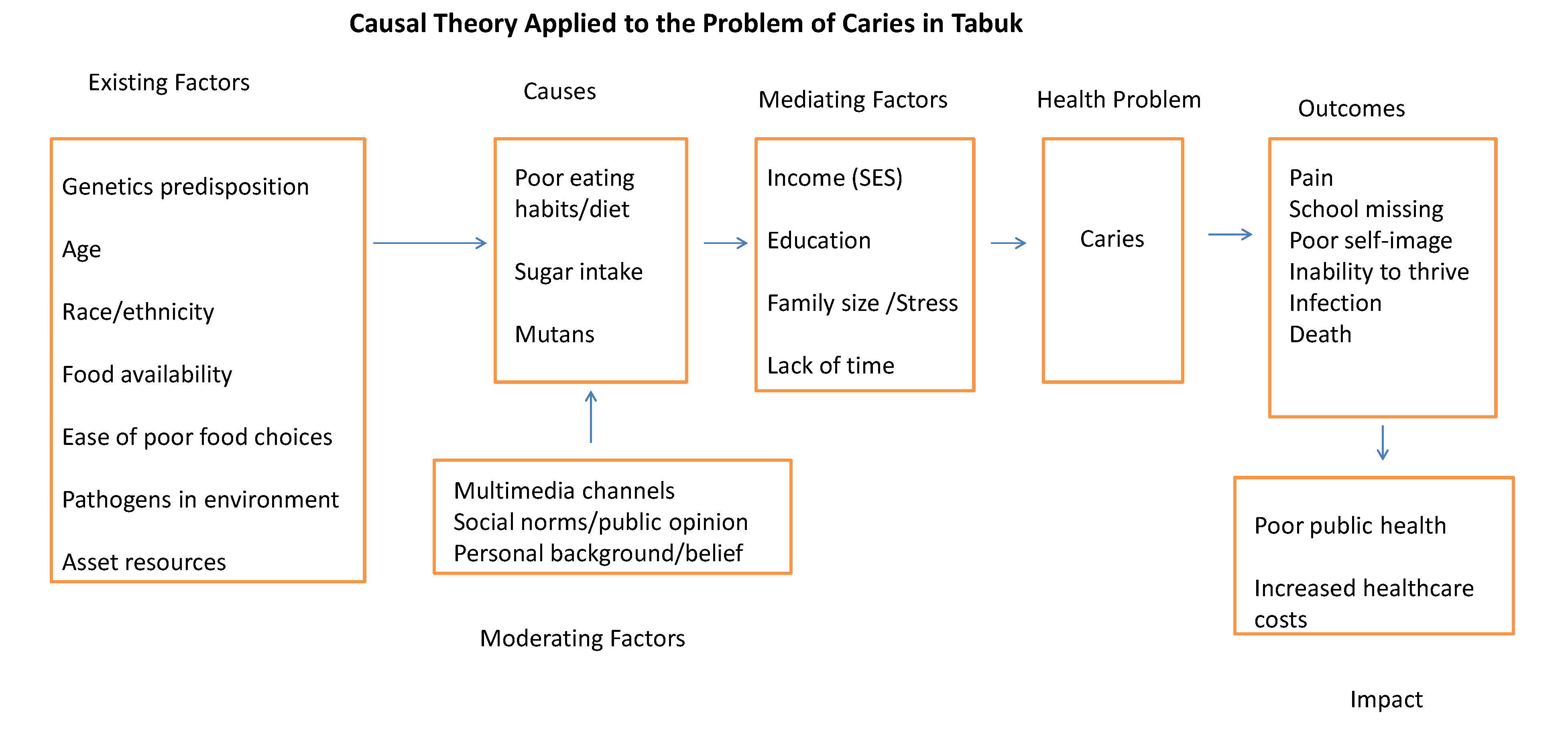
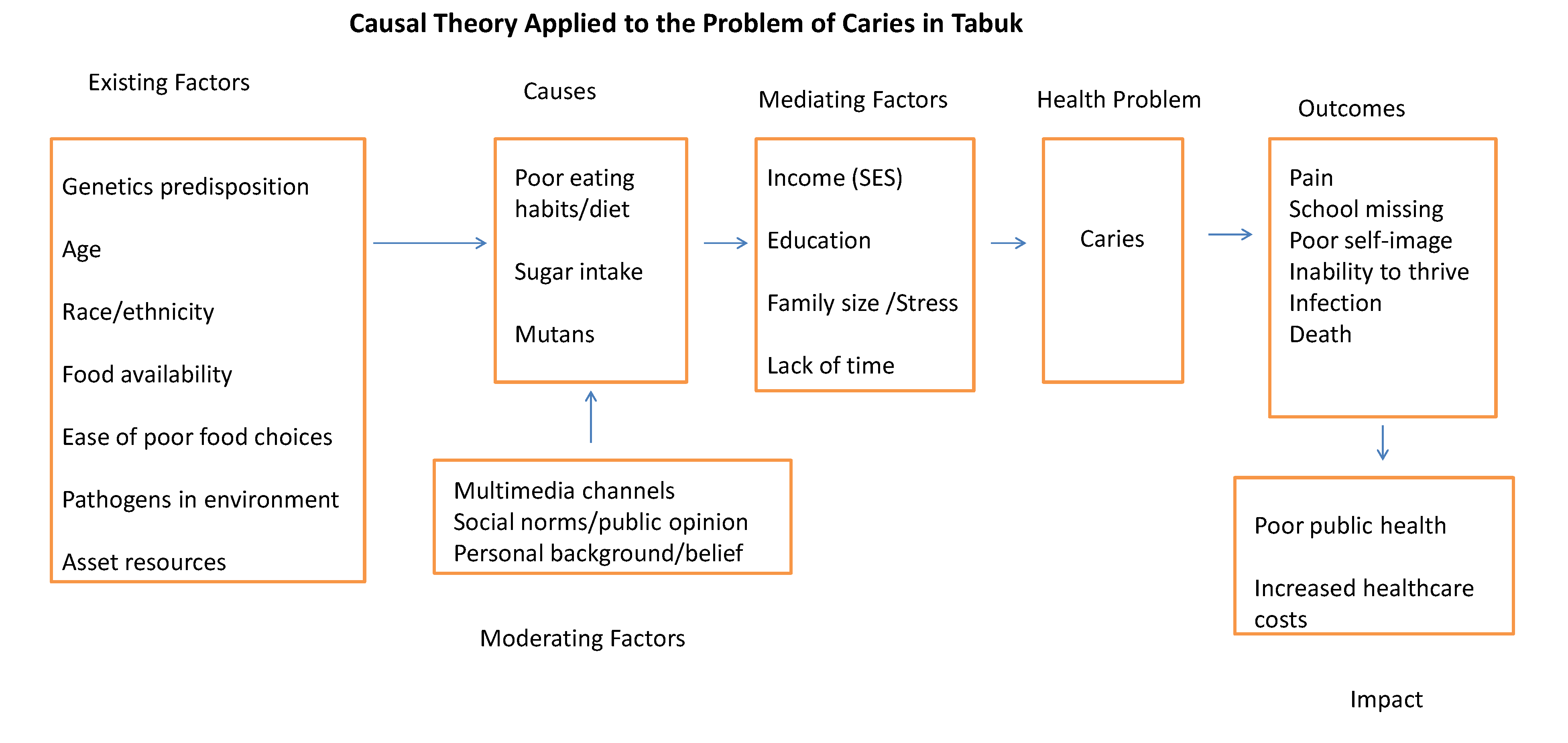
Causal theory hypothesizes the causes of a health problem by identifying factors contributing to a specific problem and resulting outcomes [
6]. Elements of causal theory guide the intervention choice and the parameters for the evaluation of program effects. Implementing causal theory to identify factors contributing to caries in Tabuk schoolchildren revealed specific factors leading to the health problem, mediating factors between causes and outcomes, moderating factors with the potential to exaggerate or lessen the problem, and existing factors (known as required antecedent factors) underlie the causal factors [
6].
Figure 1 depicts the causal model of the caries problem in children in Tabuk, Saudi Arabia.
Figure 1.
Causal theory applied to the problem of caries in Tabuk, Saudi Arabia.
Figure 1.
Causal theory applied to the problem of caries in Tabuk, Saudi Arabia.
4. Description of the Program: Evidence-Based Interventions
4.1. Strategies: Rationale and Evidence
As dental caries is a multifactorial disease, several strategies are needed to control progression or, preferably, prevent initiation. Preventive measures with demonstrated efficacy should be collectively considered in the fight against dental disease. According to Topaloglu, Eden, and Frencken (2009), there are three primary means to control dental caries [
7]. The first is by weakening caries’ promoting factors, such as non-milk extrinsic sugars and cariogenic bacteria [
8]. The second is reinforcing protective factors, such as fluoride with its various modalities, both topical and systemic, and dental sealant. Fluoride has made an enormous contribution to the decline in dental caries, particularly in industrialized countries, and fissure sealant is a proven preventive agent [
9]. As caries are etiologically complex, the third, and most recommended means, to address dental caries is through a combination of weakening those factors, which promote caries and reinforcing those factors, which protect against the disease.
Several international programs (European, New Zealand, Australia, U.S., China) and diagnostic measures have been developed and applied to improve the oral health status in children with varying evidence [
10]. In the U.S., for example, a number of federally funded organizations have been working for decades to address the carious disease in U.S. populations. The Federal Head Start had a preventive dentistry program with mass sealant application to the appropriate age groups. In addition, fluoridation experts have been managing reservation and pueblo fluoride levels into the drinking water. Several community-based and school-based educational programs in which oral health and disease prevention series of lectures and hands-on, including tooth brushing with a fluoridated toothpaste, have helped populations to improve oral health. Several comprehensive papers and systematic reviews support sealant and fluoride, both topical and systemic, applications [
10,
11,
12,
13]. While the current proposed program fits alongside such international programs, the suggestion of the 1998 World Development Reports of the United Nations Development Program, “Think Globally, but Act Locally,” should be considered [
14].
Because the ramifications of dental caries adversely affect patient health, psychosocial environment, and finances, it must be addressed as a community health problem, not just biologic one. Engaging and empowering members of the community to identify the problem and its potential causes and search for tailored solutions to a community is a prerequisite for a sustained, successful community program. Poor habits (e.g., diet and nutritional habits) and life-styles (e.g., sedentary) that eventually lead to most of the chronic diseases humanity suffers from, including dental caries, are initiated during youth and reinforced by sociopolitical policies and environmental conditions [
15]. A recent study found that the Saudi Arabian children’s caries experiences and related behaviors are similar to those of mothers (DMFT/dmft of mothers and children were high: 12.4 and 9, respectively) [
16]. DMFT describes the prevalence of dental caries in an individual by calculating the number of Decayed (D), Missing (M), and Filled (F) Teeth (T). For the primary dentition, the corresponding designations are dmft. Acknowledging and tackling these conditions will reduce risk factors for chronic diseases, including the most common, dental caries. Increasing social capital will aid in translating concepts of health education and promotion into action within the community, providing the prevention program the supportive environment needed for success.
4.2. Strategies and Activities Lists
Strategy 1. Create school oral health surveillance systemActivity 1.1. Conduct visual dental screening of children at school.
Activity 1.2. Identifying the presence of dental disease and condition.
Activity 1.3. Identify children according to their caries risk classification.
Activity 1.4. Inform parents of children who screened positive and seek informed consent for further actions.
Strategy 2. Provide the supportive environment for optimal oral health Activity 2.1. Reduce consumption of refined sugar at the school.
Activity 2.2. Ban carbonated beverages in the school canteen and vending machines.
Activity 2.3. Provide children a healthy diet, including less sugary foods and acidic soft drinks and more fresh fruit and vegetables.
Activity 2.4. Ensure equitable access to safe fluoridated drinking water at the school.
Activity 2.5. Conduct periodic oral hygiene educational programs for children and families.
Activity 2.6. Distribute free toothbrushes and fluoridated toothpastes.
Activity 2.7. Arrange for supervised tooth brushing (toothbrush drills).
Strategy 3. Apply fluoride varnish and dental sealants on high- and medium-caries risk children in school-based setting Activity 3.1. Contract well-trained dental hygienists for fluoride and sealant application.
Activity 3.2. Apply fluoride varnish four times per year.
Activity 3.3. Apply dental sealants on first permanent molars of first-grade children and second permanent molars of sixth-grade children.
Activity 3.4. Re-evaluate sealants every six-month interval and re-apply, if necessary.
Strategy 4. Provide treatment for existing dental diseasesActivity 4.1. Contract dental professionals (general practitioners, dental therapists, pediatric dentists).
Activity 4.2. Purchase a mobile dental clinic for providing on-site dental care to children.
Activity 4.3. Start with atraumatic restorative treatment (ART) or interim therapeutic restorations (ITR) to meet the basic service required and achieve caries control.
Activity 4.4. Refer advanced cases of dental needs to contracted specialized dental clinics in school-linked settings.
Strategy 5. Increase awareness of opportunities for organized actionsActivity 5.1. Build relationships with local people who will benefit from the program and understand their realities.
Activity 5.2. Conduct society needs assessments through an epidemiologic survey.
Activity 5.3. Create a dialogue, asking people their opinions concerning the oral health program and their perceived priorities.
Activity 5.4. Cooperate with groups already working in the area to benefit from their knowledge and experience.
Activity 5.5. Integrate parents in the school program as auxiliaries.
Activity 5.6. Integrate dental school programs into the curriculum.
Activity 5.7. Integrate oral health into maternal and child health programs.
Activity 5.8. Work with the official figures to create food legislation to better label of products, increase the cost of highly-carbonated beverages, and reduce the price of healthy alternatives.
Strategy 6. Monitor, evaluate, and revise the program Activity 6.1. Create a surveillance system for all program’s activities.
Activity 6.2. Monitor program progress meeting stated objectives, how well personnel are doing their jobs, and how well equipment and facilities are operating.
Activity 6.3. Measure the progress of each activity.
Activity 6.4. Identify problems in carrying out the activities and plan revision and modification.
Activity 6.5. Plan for summative evaluation at the end of the program to evaluate its impact outcome.
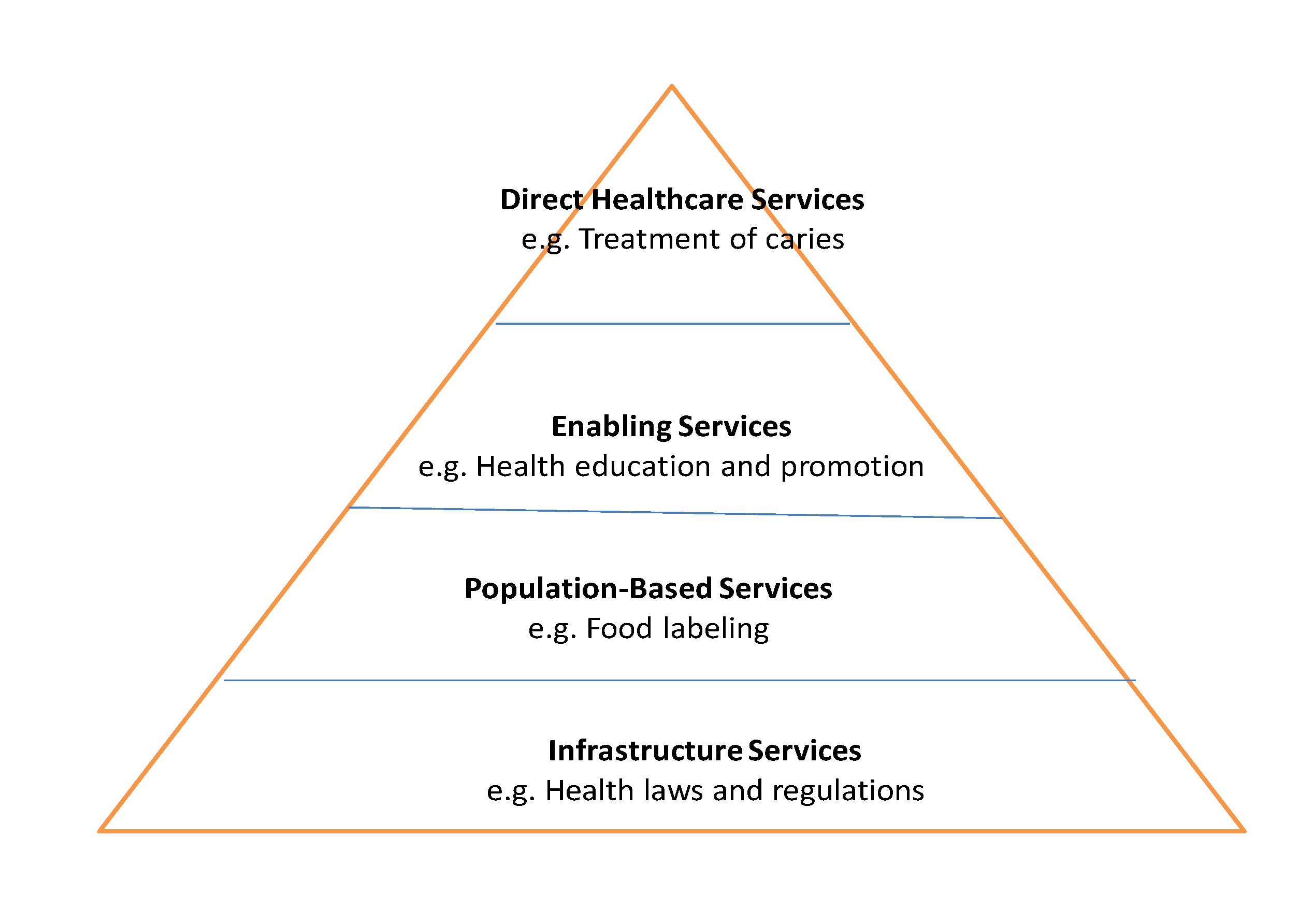
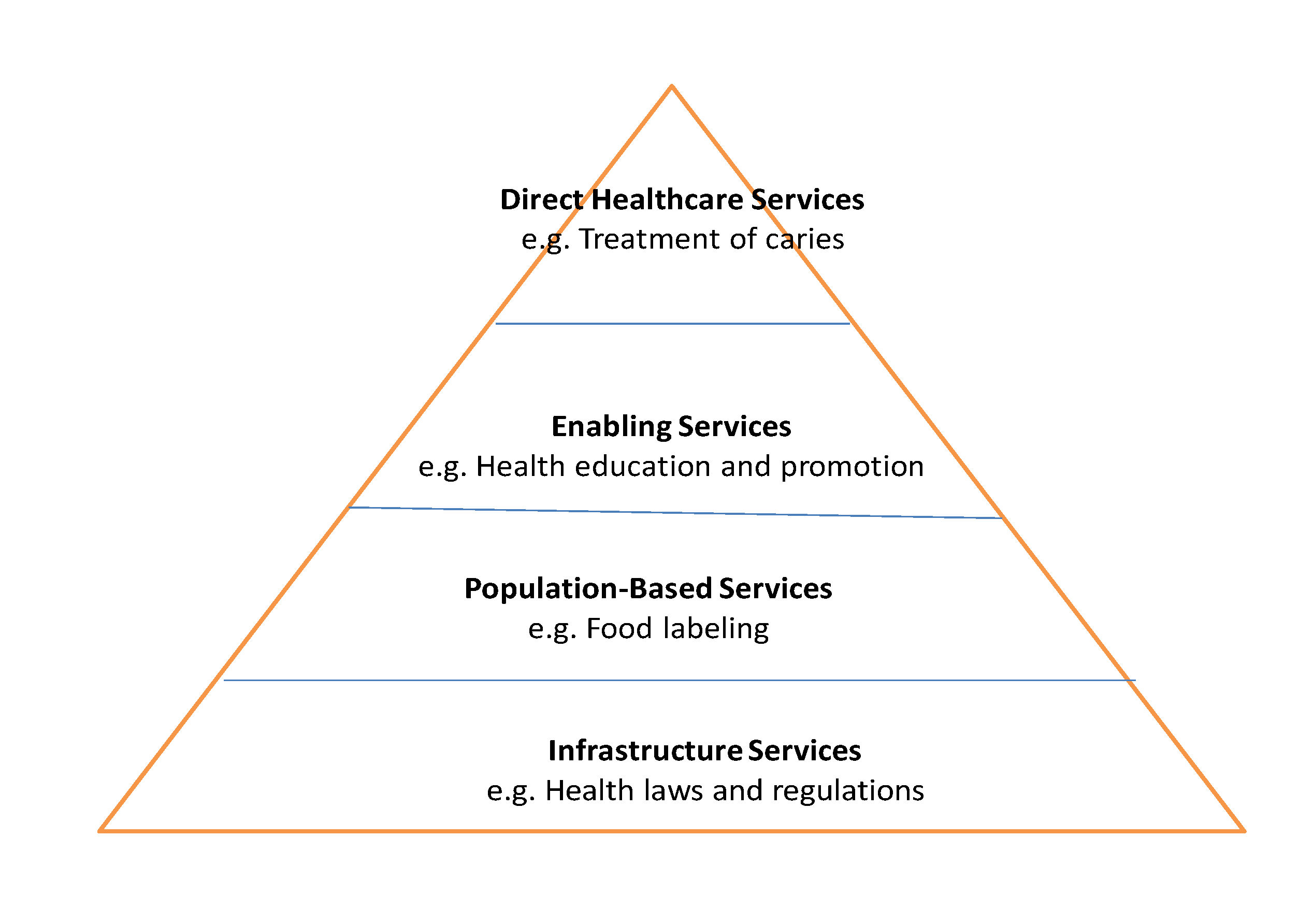
Program strategies and activities support the public health pyramid (
Figure 2) [
6]. For example, the top of the pyramid (direct healthcare services) contains services directed to individuals (students), which have immediate effects on the health of participants (e.g., treatment of carious lesions). The next level, enabling services, contains health and social services supporting or supplementing the health of students, such as a nutritional education program provided at the school. The next level, population-based services, offers services, such as food labeling. Finally, base of the pyramid contains the infrastructure of the health program, such as laws and regulations pertinent to the health of the people.
Figure 2.
The program health pyramid.
Figure 2.
The program health pyramid.
4.3. Specific Interventions
Provision of dental treatment to increase the percentage of fillings in primary teeth (F) and in primary teeth (f) components to 90%. Pediatric dentists and general practitioners collaborate to achieve this goal.
Increasing the awareness of children and their parents toward the importance of oral health through organizing oral health education and promotion programs [
17]. Schools teachers and dental health educators will collaborate to promote the importance of oral health in children.
Preventive measures including oral hygiene instructions and fluoride varnish to all children. Dental hygienists and therapists are responsible for achieving this goal.
Identification of early signs of dental disease in infants, toddlers, and preschoolers should be sought by targeting parents through dental health education sessions, emphasizing diet modifications to reduce sugar consumption and encourage supervised tooth brushing with fluoridated toothpaste, systemic fluoride supplements to children (the fluoride level in Tabuk’s drinking water is well below the recommended level), professional fluoride varnish application, and sealants for primary molars [
18].
4.4. Program Goals and Objectives
The program goals and objectives are linked to causal theory (
Figure 1) and specific interventional plans listed above. The program goals will be achieved when corresponding process and outcome objectives are met.
Goal 1: Meeting the restorative dental needs of grades one and six Tabuk schoolchildrenObjective 1.1: Screening all available children in grades one and six to identify oral health needs and define teeth restoration needs.
Objective 1.2: Recruiting practicing dentists, pediatric dentists, dental assistants, dental hygienists, and dental therapists to provide children with the needed restorative care.
Objective 1.3: Providing restorative treatment for grades one and six children (whose parents signed the informed consent forms).
Goal 2: Promoting and applying evidence-based preventive activities that sustain oral health and prevent dental caries Objective 2.1: Adding fluoride to school public drinking water by the recommended level (0.7 ppm).
Objective 2.2: Applying dental sealants on fully erupted first permanent molars of grade one students and second permanent molars of grade six students.
Objective 2.3: Applying fluoride varnish on at least 90% of children.
Objective 2.4: Contacting the Ministry of Education to ban carbonated soft drinks and other junk foods in the school’s canteen and vending machines.
Goal 3: Mobilizing and empowering the public and community organizations to recognize and apply solutions for the problem of caries in children Objective 3.1: Establishing community groups to identify oral health needs and define solutions through advocacy and promotion of oral health.
Objective 3.2: Organizing oral health campaigns in schools, hospitals, and work settings advocating a healthy diet that includes fresh fruits and vegetables instead of sugar and processed foods.
4.5. Program Resources
To implement the current program adequate resources must be specified and acquired. The resources required to meet the program’s needs and successes encompass a variety of elements, including human resources, physical resources, transportation, informational resources, time, managerial resources, and monetary resources [
6].
Human resources are the cornerstone in planning, implementing, and evaluating a program, and encompass the expertise, experience, and capabilities of personnel. Personnel costs often constitute the largest portion of any program budget. The program’s personnel can be divided into two types: dental staff and administrative staff. The program will be directed by a public health dentist and managed by the director of the program, who has several years of experience in school-based and school-linked dental programs. Additional personnel include dental assistants, dental hygienists, and a dentist, all holding current licenses from the Saudi Commission of Health Specialties and Ministry of Health. Riyadh College of Dentistry (RCD) has promised to provide this program with these personnel. The dental students from RCD will serve as dental educators and will help the licensed dental staff in screening, fluoride varnishing, and applying sealant, and administrative work. The program plans to hire an evaluation specialist with a lump sum and a program secretary on a wage basis. Off-site personnel include postgraduate students and academic instructors in RCD pediatric dental clinics who will provide specialized dental care for a portion of schoolchildren referred to receive advanced restorative care. The program has a plan to recruit volunteers from the local community, such as schoolteachers and a school nurse.
Physical and Informational Resources include material resources, facilities, supplies, hardware and software, and equipment. The dental mobile van, provided by the SDS, is equipped to provide basic dental care such as simple restorations and simple extractions. Taking radiographs are also possible, if needed. On-site materials and equipment to provide the intervention include fluoride varnish, dental sealants, disposable screening tools, personal protective equipment, and educational materials and handouts. Ministry of Defense Medical Services Division (MDMSD) will provide office equipment, such as computers, fax machines, and photocopiers, by using their well-equipped offices, which also include staff members who will bring informational knowledge to the program.
Transportation. The program staff members will be compensated for transportation expenses from and to the target school. Families will be responsible for taking their referred schoolchildren to RCD facilities.
A timeline for each goal and objective has been provided in the ‘program goals and objectives’ section.
Monetary Resources: Aside from the services, facilities, personnel, and equipment RCD and SDS pledged to offer, MDMSD has offered to provide successive grants to our program to meet its financial requirements based on balance sheets and budget.
4.6. Budget
The total cost of this program is divided into direct costs (personnel and non-personnel) and indirect costs. The personnel costs are salaries and wages, fringe benefits and consultants and contractual costs. The non-personnel costs are materials and supplies, equipment, communications, travel (domestic and foreign), and other expenses, such as those related to arranging or attending a symposium. Indirect costs are intangible costs, such as lights and maintenance.
4.7. Program Partners
For achieving the program's objectives, partners from several units and organizations will be included. As Tabuk is in a primarily military area, we start with Ministry of Defense Medical Services Division because it has the proper authority to approve and assist the program. As military personnel and their dependents are medically and dentally served via Northwest Armed Forces Hospitals, we need to include these facilities as network partners. King Adulaziz Military City should be contacted also for potential appointments or contracts with specialists/consultants in public health dentistry, hygienists, and dental health educators, as there is a lack of personnel in these fields. Ministry of Education should be contacted to provide schoolchildren with fluoridated toothpastes and brushes, non-cariogenic snacks, and drinks, and oral health education sessions in schools. In addition, Saudi Dental Society (SDS) represented by the Saudi National Campaign against Tooth Decay among Children will be contacted to raise awareness toward these groups of children, and seek help by providing the project with one of their mobile dental vans. The SDS, in collaboration with several leading manufacturers of oral care products such as Oral-B and Colgate, conducts school-based oral health education to promote behavior conducive to health among schoolchildren, and distributes free fluoridated toothpastes and brushes in addition to educational materials and motivational stickers.
Another partner, which showed a keen interest in pursuing this project, is Riyadh College of Dentistry (RCD). RCD has generously offered to provide the program with two portable dental units, one dentist, three dental assistants, three dental hygienists, and an indefinite number of dental students. It also offers treatment for children in need of advanced restorative care in its pediatric dentistry unit. Based on that, the program activities will take place in the school, including screening, oral health education, sealants and fluoride varnish application, and ART (or ITR). Other advanced restorative treatment, including extraction and/or pulp therapy, will be referred to RCD’s clinics. Students, parents, and school staff members are the cornerstone of any successful program targeting schoolchildren and, therefore, their understanding of the importance of the program and their willingness to help is a prerequisite to a fruitful outcome.
4.8. Program Outlines and Logistics
The program outline was as the following:
5. Pilot Program Implementation and Assessment
As mentioned previously, the dental department in a private dental college (RCD) and oral health product manufacturers (Colgate-Palmolive and GlaxoSmithKline) agreed to be part of the project. They helped meet the goals of applying fluoride varnish and dental sealants on high- and medium-caries risk children in school-linked settings, providing treatment for existing dental diseases either under local anesthesia or in the operatory room under general anesthesia, and increasing awareness of children and their parents toward the importance of oral health through organizing education and promotion programs and distributing free toothbrushes and/or fluoridated toothpastes. Dental treatments were provided under substantial discounted fees or by accepting most insurance plans. Other services were provided at no charge.
Forms including appraisal of children’s nutritional intake, oral hygiene status, and parents’ perceptions toward the importance of the children’s oral health status to general health and well-being were constructed. These forms were completed at baseline and after providing oral health education/promotion and dental treatment to ascertain the impact of the program’s interventions on the oral health status of children and their families.
The WHO standard for surveying caries that is based on dmft/DMFT (Decayed, Missing, or Filled Primary and Permanent Teeth) was followed [
19]. Further, children were classified according to need for dental care: children who were in urgent treatment need (children who are in obvious pain at the time of examination, visible infection, gross swelling, or presence of pus), and those who had visible decays but without urgent treatment needs. Diet evaluation forms were also distributed for recording everything the child eats or drinks within five days. The ADA’s Risk Assessment forms were used as a tool to evaluate a patient’s risk of developing caries.
Oral hygiene was assessed using the Debris Index, the most common index used to evaluate children’s oral hygiene practices [
20]. Each child was given a disclosing tablet to chew for visualization of soft and hard deposits. Using age appropriate language, the composition, distribution, and effects of plaque were explained and methods for daily removal were demonstrated. Parents were invited to take an effective responsibility toward their children’s oral-health care. One-to-one education to parents emphasizes key messages, including regular dental visits, signs of early carious lesions, tooth brushing, use of fluoride toothpaste, feeding practices, and reduced cost treatment options. Forms for documenting oral hygiene instructions were given verbally and/or along with printed materials.
The debris from six preselected tooth surfaces was scored as the following: 0 no debris or stain present; 1 soft debris, covering not more than 1/3 of tooth surface; 2 soft debris, covering more than 1/3 but not more than 2/3 of the tooth surface; 3 soft debris covering more than 2/3 of tooth surface. After the scores for debris are calculated, the debris scores were totaled and divided by 6, the number of segments scored [
21].
Each child received professional oral cleaning with fluoridated prophylaxis paste followed by fluoride varnish application (Clinpro White Varnish, 3M ESPE). The varnish takes a few minutes to put on the teeth. It helps prevent initiation of dental caries and slow down progression of existing decay. In addition, each child was given a kit, containing a toothbrush, fluoridated toothpaste, and a dental floss. Hand-outs and flyers emphasizing the importance of oral-health care and how it can be achieved were distributed to children and families. An important segment of this project was to explore oral-health-related quality of life (OHRQoL) of children as reported by parents. OHRQoL is a concept that was originally conceptualized in 1978 in a discussion of the relationship between the mouth and patient quality of life [
22]. It is defined as that part of a person’s quality of life affected by the oral health. This concept focuses on the patient as a whole and, therefore, emphasizes the holistic model of oral health.
More recently, a number of oral-health-related quality of life (OHRQoL) scales have been developed and validated [
23]. As children—very young children, in particular—are often not reliable sources of information for medical purposes (e.g., diagnosis), parents are relied on as informants for measuring child OHRQoL [
22]. The instrument used here consists of four sections.
Section 1 consists of two items, asking about the oral health status in general (item 1) and how much the child’s overall wellbeing is affected by the condition of his oral health (item 2).
Section 2 consists of 14 items, focusing on the signs and symptoms of oral disease the child experienced during the last three months.
Section 3 consists of 19 items, on the effects of oral disease on the child’s feelings and everyday activities.
Section 2 and
Section 3 comprise a Parental-Caregivers Perceptions Questionnaire (P-CPQ).
Section 4 consists of 14 items, focusing on the effects of child’s oral disease on parents and other family members; this is known as a Family Impact Scale (FIS). All items are scored using 5-point Likert-type response options. A P-CPQ consists of 33 items, measuring certain domains: oral symptoms (six items), functional limitations (eight items), emotional well-being (nine items), and social well-being (ten items). A FIS scale consists of 14 items, measuring certain domains: parental/family activity (five items), parental emotions (four items), and family conflict (four items).
The remainder of this document presents comprehensive data on the sample of schoolchildren who received comprehensive dental treatments at the referral center.
6. Results
6.2. Dental Reimbursement
Health services, including oral healthcare, are mainly provided by the Ministry of Health hospitals and its primary and specialized health centers. Those services are provided free of charge to Saudi nationals (23.5 million people) and with fees to non-nationals (5.5 million) [
24]. It is admitted, however, that the organization of health service delivery needs to be improved [
25]. There is an increased participation from the private sector in the provision of medical and dental healthcare, particularly with the recent large number of companies specializing in health insurance [
1]. It is evident from
Table 2 that all children had private or public dental insurance.
Table 2 demonstrates number of children according to their types of health insurance. There were six health insurers providing dental coverage along the health coverage with different benefits. The majority of children are covered by public insurance known as SCECO (28 patients or 58.3%). While SCECO reimbursement rates are lower than other health insurance companies, it has two advantages to beneficiaries: no deductibles and no annual maximum limits. Many health-care providers do not accept SCECO enrollees; however, RCD accepted them as part of its service to society through the current program.
Table 2.
Types of Health Insurance
Table 2.
Types of Health Insurance
| Insurers | SCECO | Bupa | NCCI | Shield | Medi-Visa | GlobMed |
|---|
| No. patients (%) | 28 (58.3%) | 4 (8.3%) | 8 (16.7%) | 2 (4.2%) | 4 (8.3%) | 2 (4.2%) |
6.3. Oral Health and Quality of Life
Forty-eight OHRQoL questionnaires were completed by 48 children’s parents (26 father and 22 mother; average age 43.3 [
SD 9.8]). The two general questions asked how parents would rate the health of their child’s teeth, lips, jaws and mouth and how much parents believed a child’s overall wellbeing was affected by the condition of his/her teeth, lips, jaws or moth.
Table 3 and
Table 4 present the distribution of scores.
Table 3.
Distribution of Parents’ Answers to the Global Question: How would you rate the health of your child’s teeth, lips, jaws, and mouth?
Table 3.
Distribution of Parents’ Answers to the Global Question: How would you rate the health of your child’s teeth, lips, jaws, and mouth?
| | Answers |
|---|
| | Poor (0) | Fair (1) | Good (2) | V. Good (3) | Excellent (4) |
| Number | 24 | 10 | 12 | 2 | 0 |
| Percentage | 50% | 20.8% | 25% | 4.2% | 0% |
Table 4.
Distribution of Parents’ Answers to the Global Question: How much is your child’s overall wellbeing affected by the condition of his/her teeth, lips, jaws, or mouth?
Table 4.
Distribution of Parents’ Answers to the Global Question: How much is your child’s overall wellbeing affected by the condition of his/her teeth, lips, jaws, or mouth?
| | Answers |
|---|
| | Not at all (0) | Very little (1) | Some (2) | A lot (3) | Very much (4) |
| Number | 4 | 10 | 8 | 8 | 18 |
| Percentage | 8.3% | 20.8% | 16.7% | 16.7% | 37.5% |
It is evident that half of the parents rated their children’s oral health as poor, with 21% and 25% as fair and good, respectively. More than one third of the parents indicated they believe that there is a “very much” relationship between overall wellbeing and the condition of the child’s oral health. Interestingly, 8.3% believe there is no relationship between the two; 21%, 17%, and 17% think the relationship is “very little,” “some,” or “a lot,” respectively.
The question asked parents about pain in the teeth, lips, jaws or mouth (question number 3) was important because pain is usually the driving reason to seek medical/dental help. Twelve (25%) parents reported their children as having “every day or almost every day” pain related to oral cavity, while eight (16.7%) reported “often,” 18 (37.5%) reported “sometimes,” 6 (12.5%) reported “once or twice,” and four (8.3%) reported “never.” Pearson correlation between oral health status and pain (1st item and 3rd item) was found to be 0.417 (P = 0.003), which is medium in strength. This suggested that pain is an important factor in parents’ estimation of the status of their children’s oral health.
Section 2 of the questionnaire focuses on the signs and symptoms the child experiences due to his oral health condition. The mean score was 19.70 (
SD 8.79), which compares very well with that reported in another study using the same tool (21.02 ± 18.14) [
23].
Section 3 of the questionnaire focuses on the effects of oral health status on children’s feelings and everyday activities while section 4 focuses on the effects of oral health on parents and other family members. The mean scores for these two sections were 15.34 (
SD 11.12) and 17.41 (
SD 11.47), respectively. These findings suggest that parents considered the signs and symptoms of the oral/dental disease that children manifest with the highest magnitude while considered the effects of oral disease on children and families’ quality of life with less magnitude. The differences in scores were not statistically significant, however.
The responses to item 49 which asked whether “the oral health condition of the child caused financial difficulties for your family,” indicated that negligence of oral health condition is unrelated to financial difficulties as 38 (79.2%) parent reported “Never,” six (12.5%) reported “One or twice,” and four (8.3%) reported “sometimes.”
7. Program Evaluation: Process and Outcome
The program’s main evaluation effort focused on the process and outcome objectives, outlined in its proposal.
7.1. Oral Health Assessment: A Pre-Post Design
Table 5 shows the Debris Index (DI) scores of the patients at baseline and at the follow-up appointment, after about one week.
Table 5.
Debris Index (DI) Mean Scores at Baseline and After One-Week of Oral Health Education
Table 5.
Debris Index (DI) Mean Scores at Baseline and After One-Week of Oral Health Education
| | DI (Baseline) | DI (Follow-up) | t | P |
|---|
| DI mean (SD) | 3.74 (0.61) | 3.12 (0.70) | 9.86 | 0.000 |
The mean DI score was 3.74 (
SD 0.61) at baseline and decreased to 3.12 (
SD 0.70) at follow-up sessions. Paired-samples
t-test found the difference to be significant (mean difference 0.61 (
SD 0.42),
t 9.86,
df 47,
P < 0.001). However, the post-oral health instruction DI scores were higher than those reported in Saudi children in the same age group (mean 2.34) [
20]. All children were classified as high-caries risk, based on their dental clinical condition and poor dietary habits. The current results are in agreement with those of Al-Wazzan (2004) who found a mean dmft score of 7.34 (
SD 4.02) in school-aged children [
20]. He also reported that 88% of children were consuming sweetened snacks three to four times per day, and 41% were not brushing their teeth. These results are consistent with the findings reported here and convey the importance of developing approaches to improve the oral hygiene and compliance with dietary recommendations.
Self-efficacy, as proposed by Bandura, plays an important role in determinant of behavior [
15]. It is the conviction that a person is able to accomplish a behavior needed to bring about certain outcome. The approach, based on self-efficacy, involves the following:
The patient accomplishes a large part of dental care, thus he/he plays an important role in controlling and making decisions on his own dental care.
The dental provider has the task of providing knowledge and psychosocial support.
Changing behavior is more likely to start and be maintained if freely chosen and were personally reasonable.
Based on this, a dentist helps the patients to find their own competence to solve their problems, emphasizing self-efficacy and individual responsibility.
7.2. Dental Sealants: Short-term Quality Evaluation
Monitoring quality of provided services is an essential component of process evaluation. Resin-based dental sealants (Fisseal, Promedica) were provided to 11 patients and 28 first permanent molars were sealed. The remaining permanent teeth were found to be carious and in need of restorative care. Sealed molars were inspected by an experienced pediatric dentist about one-week after placement by another pediatric dentist. All sealants were found to adequately cover the occulsal pits and fissures, intact, and have marginal integrity, conforming to the requirements of sealant short-term retention checks.
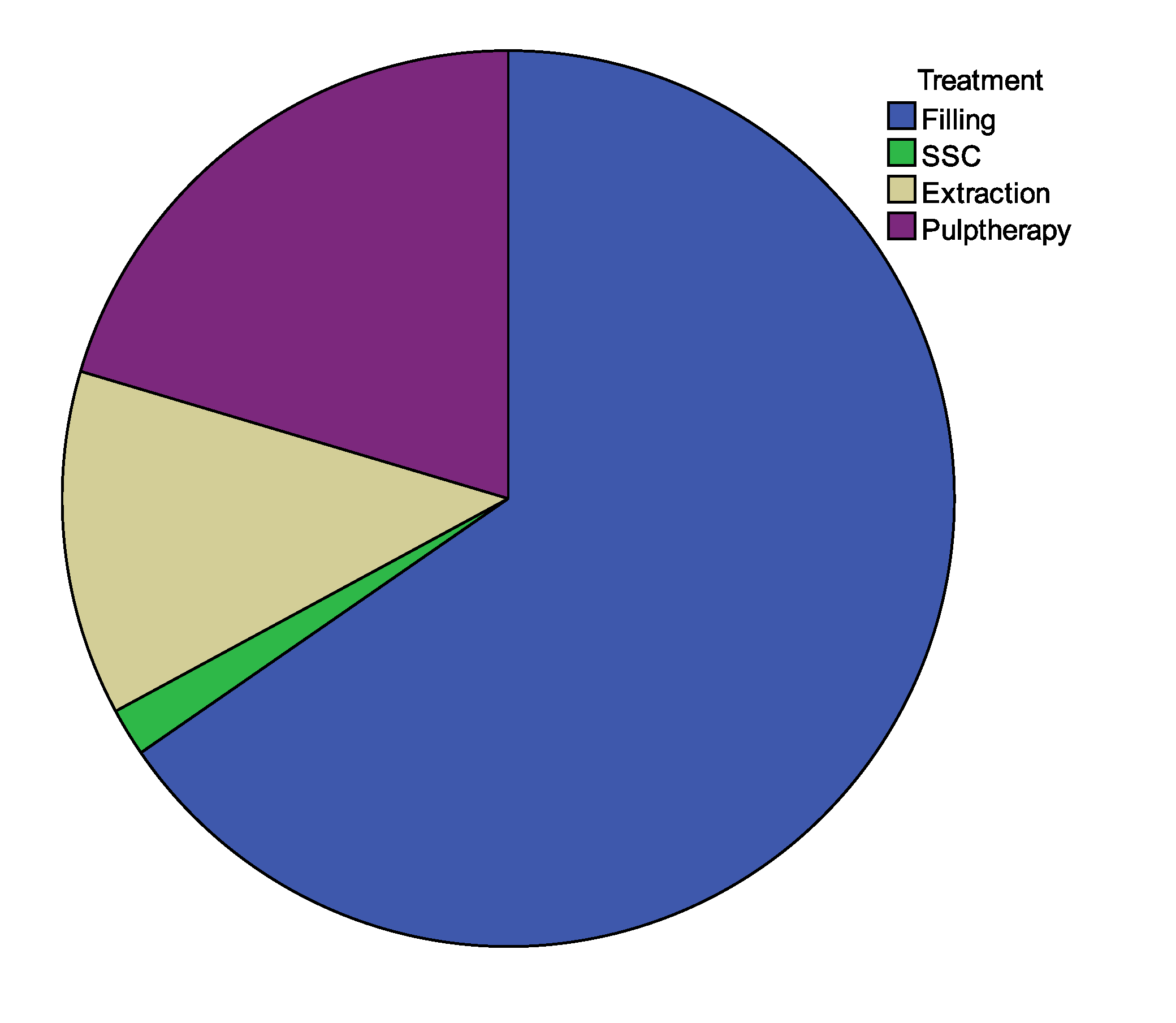
7.3. Dental Treatment Provided: An Audit
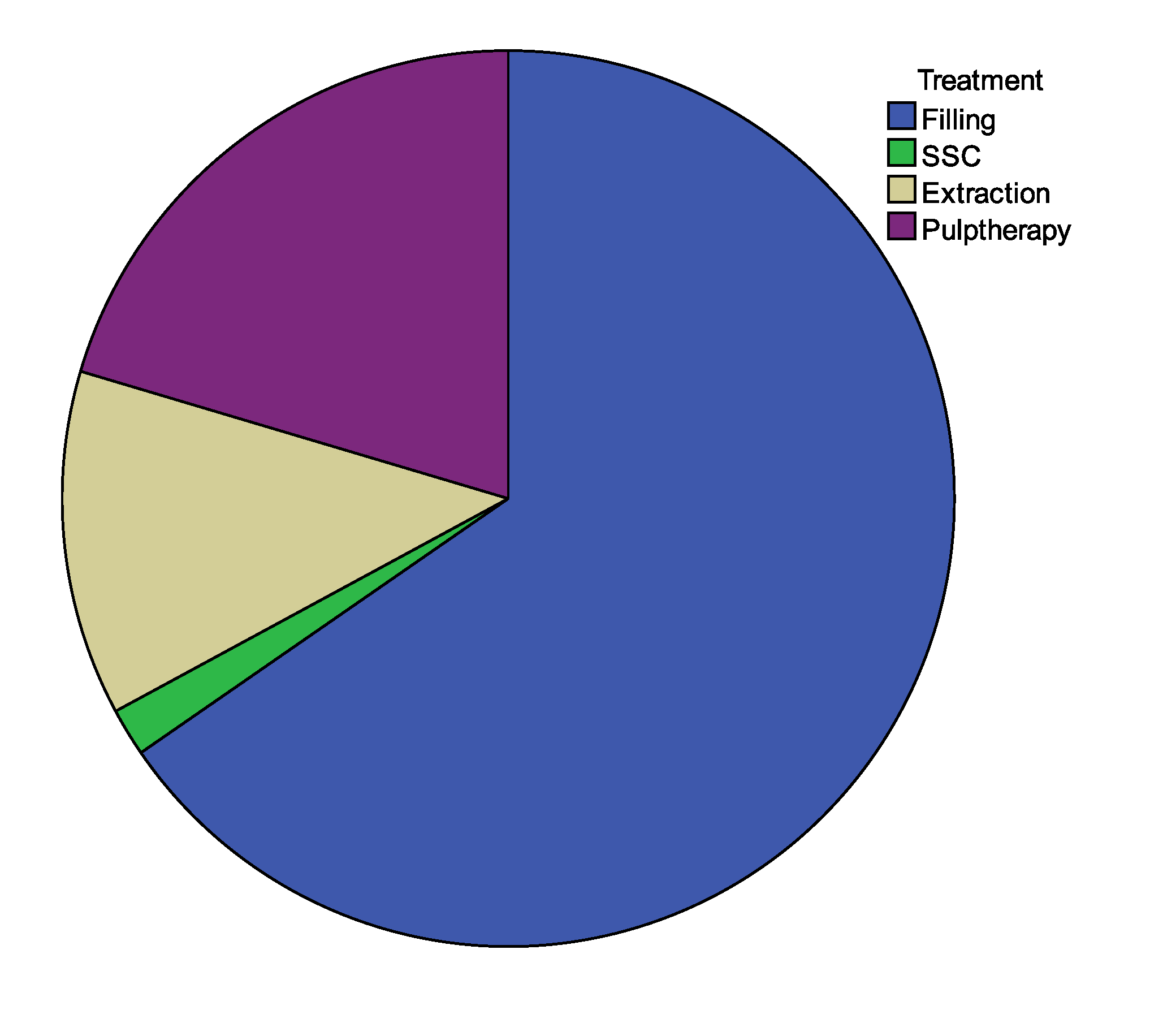
Auditing implemented interventions is an essential part of process evaluation, and meeting restorative needs of the program’s patients fulfill its immediate outcomes. Forty-eight patients received dental care during the course of the program; 378 composite resin (Filtek Z250, 3M ESPE) or resin-modified light-cured glass ionomer (Riva, SDI) restorations were placed. One-hundred and eighteen teeth received pulp therapy (pulpotomy or pulpectomy), ten of which received stainless steel crowns (SSCs). Seventy-two teeth were extracted due to caries.
Figure 3 shows the distribution of dental treatments provided. It is evident that SSCs were the least and this is explained by two reasons. First, many parents objected the metallic color of the crowns and preferred tooth-colored restoration. Second, and perhaps more importantly, no health insurance companies cover SSCs although they are the most durable restorations for primary teeth. The relative large numbers of teeth in need of pulp therapy or extraction indicate the advanced carious lesions due to negligence.
Figure 3.
Distribution of treatment provided.
Figure 3.
Distribution of treatment provided.
8. Limitations, Lessons Learned, and Future Plans
The most significant limitation to this project was its short-term nature; longer-term project at the national level is needed to fully meet the restorative and preventive dental needs of Saudi Arabian children. Another limitation was that we do not have postoperative data for OHRQoL; the study would have been strengthened had we made a postoperative assessment. We are considering distribution of post-operative OHRQoL questionnaires to parents of children who completed dental treatment. This would enable the investigator to evaluate the effects of treatment on children’s wellbeing and general health by comparing pre-operative findings to post-operative ones. Comparing pre-operative scores to post-operative scores for each domain (i.e., oral symptoms, functional limitations, emotional well-being, etc.) would reveal which domain is affected the most with dental treatment. Finally, the findings from this sample of children cannot by generalized because the sample is not necessarily representative of Saudi Arabian schoolchildren. It includes children who were referred to a specialized dental center and, therefore, can be considered as representing the children who are severely affected by dental disease.
The program intends to expand its services during the Academic year 2013-2014 to include children in other grades as well as add other schools.


{kind=link}
{kind=link}
{kind=link}