2.1. Step by Step Process of Implementation of ICDAS
A Task Force was set up in 2011 to undertake a background investigation into the potential of various systems of caries classifications for the implementation of the dental curriculum of IMU. The ICDAS was finally selected.
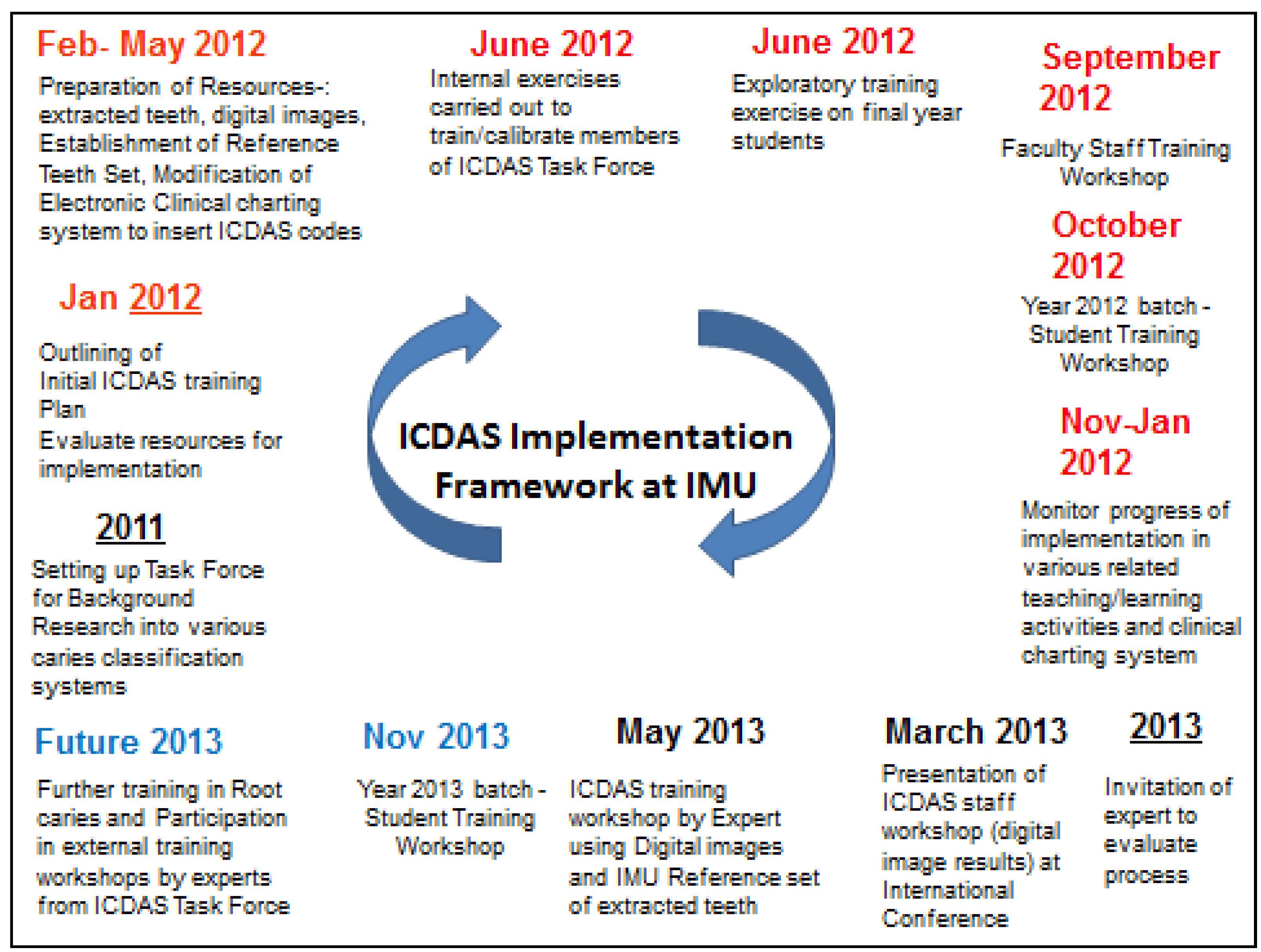
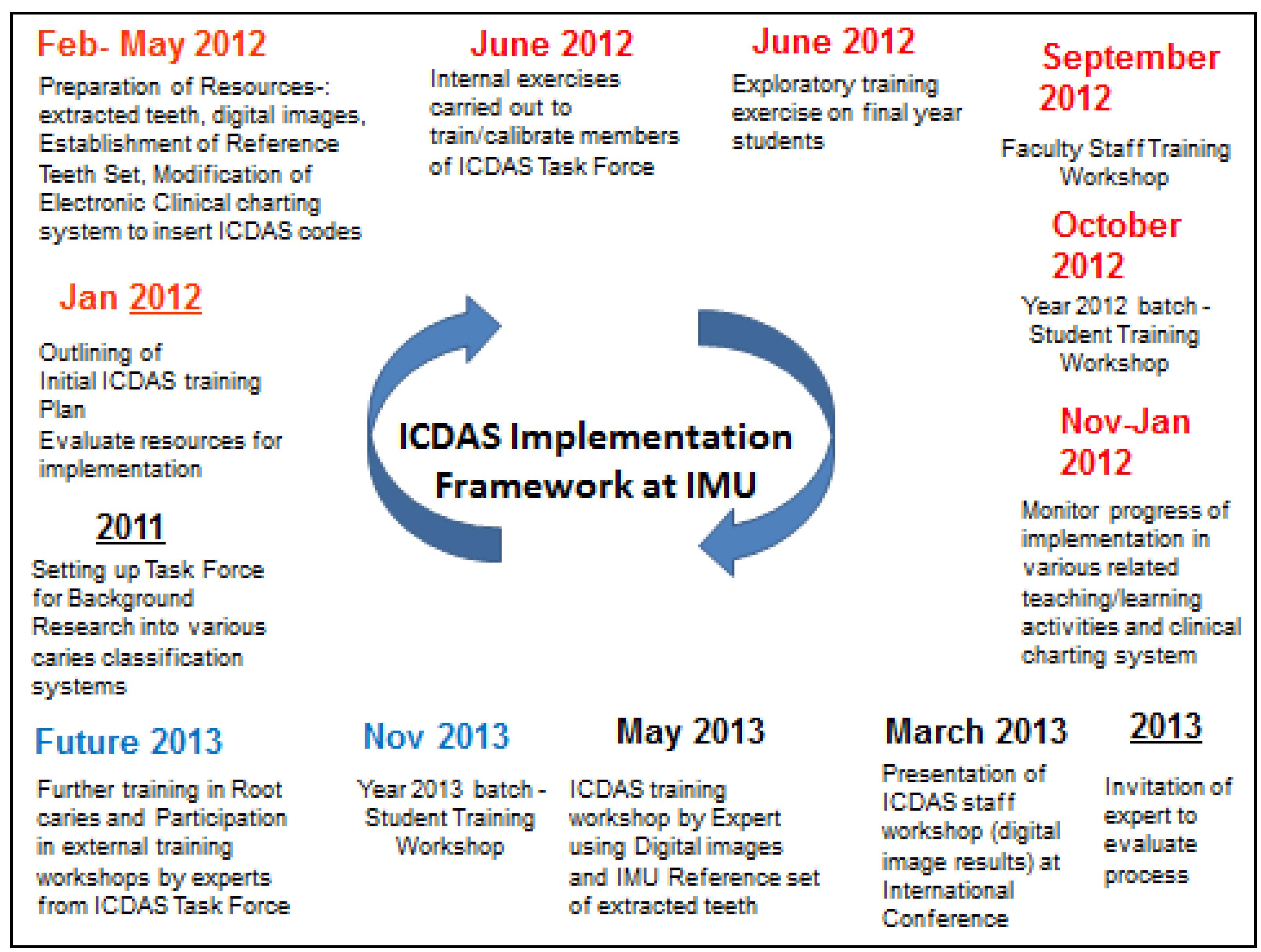
Figure 1 shows the outline framework, charting all the stages in the overall implementation process.
Once the decision was made to implement the ICDAS, an IMU-ICDAS Task Force was formed which established the framework of the implementation process.
An initial search of the literature identified the training resources which already existed and could be used in the training of faculty staff and students of IMU.
The most useful of these was a 90-min free E-learning program which had been developed by the ICDAS foundation to support training. This initial E-learning programme was designed to be a general introduction to the criteria and codes and explained the ICDAS examination protocol and reviewed the coding system. The committee evaluated it for its use in future training [
8,
9].
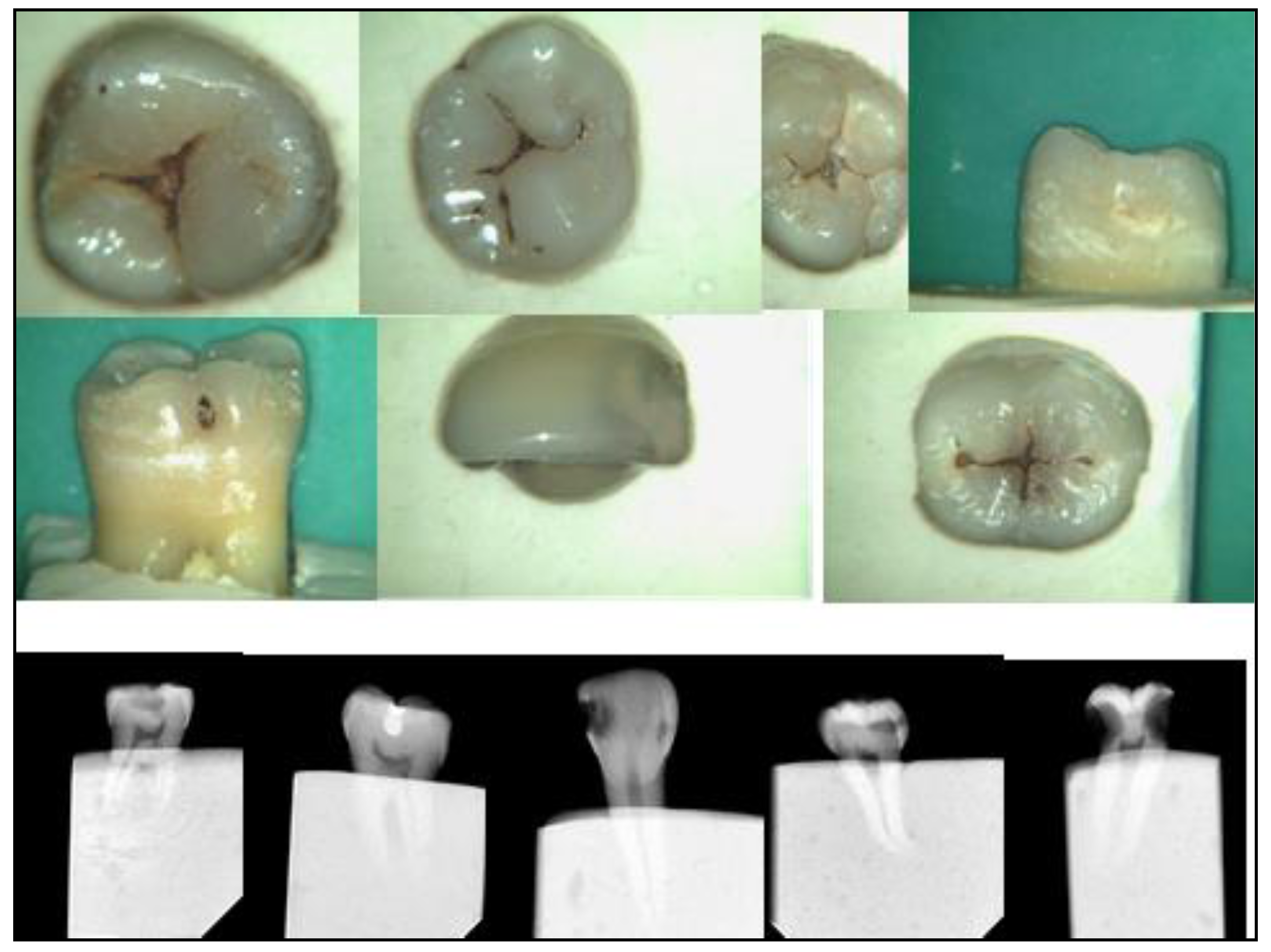
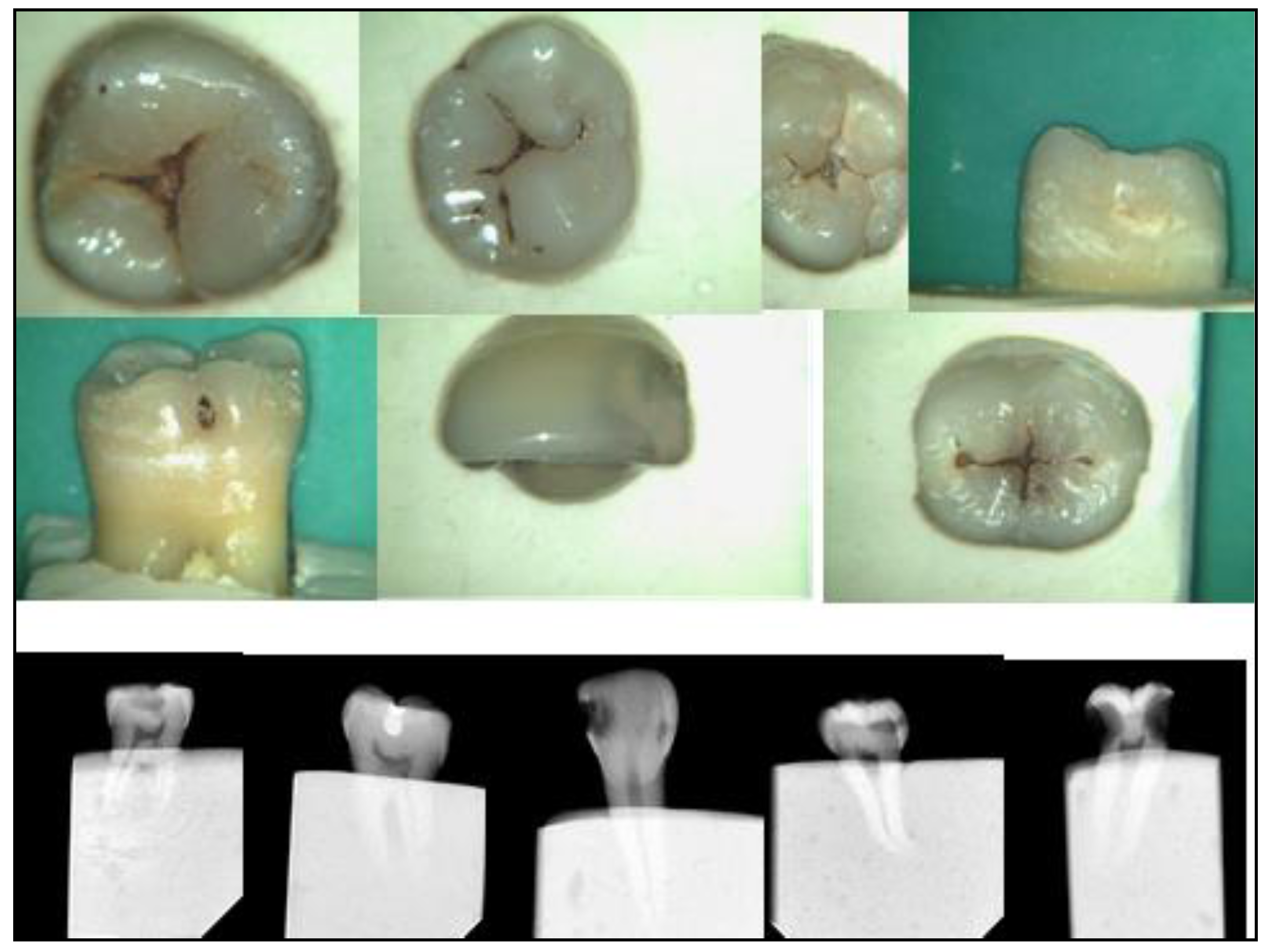
The next step was to start selecting and collecting appropriate extracted teeth with various stages of caries lesions. They were cleaned and their digital images taken with the Camsight digital surgical scope camera (
Figure 2). Photographs were also taken of carious teeth seen clinically in patients’ mouths (
Figure 3). That began the creation of a collection of training resources and tools at IMU.
Figure 1.
International Caries Detection and Assessment System (ICDAS) Implementation Framework at School of Dentistry, International Medical University (IMU).
Figure 1.
International Caries Detection and Assessment System (ICDAS) Implementation Framework at School of Dentistry, International Medical University (IMU).
Figure 2.
Camsight digital images of extracted teeth depicting different ICDAS codes with some radiographs.
Figure 2.
Camsight digital images of extracted teeth depicting different ICDAS codes with some radiographs.
Figure 3.
Camsight digital images of patients’ teeth depicting different ICDAS codes.
Figure 3.
Camsight digital images of patients’ teeth depicting different ICDAS codes.
At the same time, a ‘Reference Set’ of carious extracted teeth exhibiting an adequate number of surfaces with the different ICDAS codes was gradually and carefully examined, graded and collected over a period of several months (
Figure 4). Radiographs were taken of each tooth to eliminate or confirm the presence of deeper carious lesions (
Figure 2). Numerous discussion meetings took place so that the committee could come to an agreement on the ICDAS code given for each of the caries lesions on the surfaces of these teeth.
Figure 4.
The IMU Reference Set of extracted teeth.
Figure 4.
The IMU Reference Set of extracted teeth.
For the next few months, the ICDAS Task Force carried out evaluation exercises amongst themselves using the Reference Set and the Camsight digital images in order to establish which were suitable for calibration. In the event, it was found that not enough information is present in digital images to enable the observers to accurately grade lesions as compared with the actual teeth. However, the images have some use in preliminary discussions in training.
Finally, the Reference Set of teeth was used by the Task Force to train and calibrate its members so as to reach high levels of intra-examiner and inter-examiner agreement.
An exploratory training exercise using the ‘Reference Set’ of extracted teeth for calibrationand digital images for discussion was also carried out with the final year students during this time. It showed they gained a high level of understanding and good acceptance of this classification system.
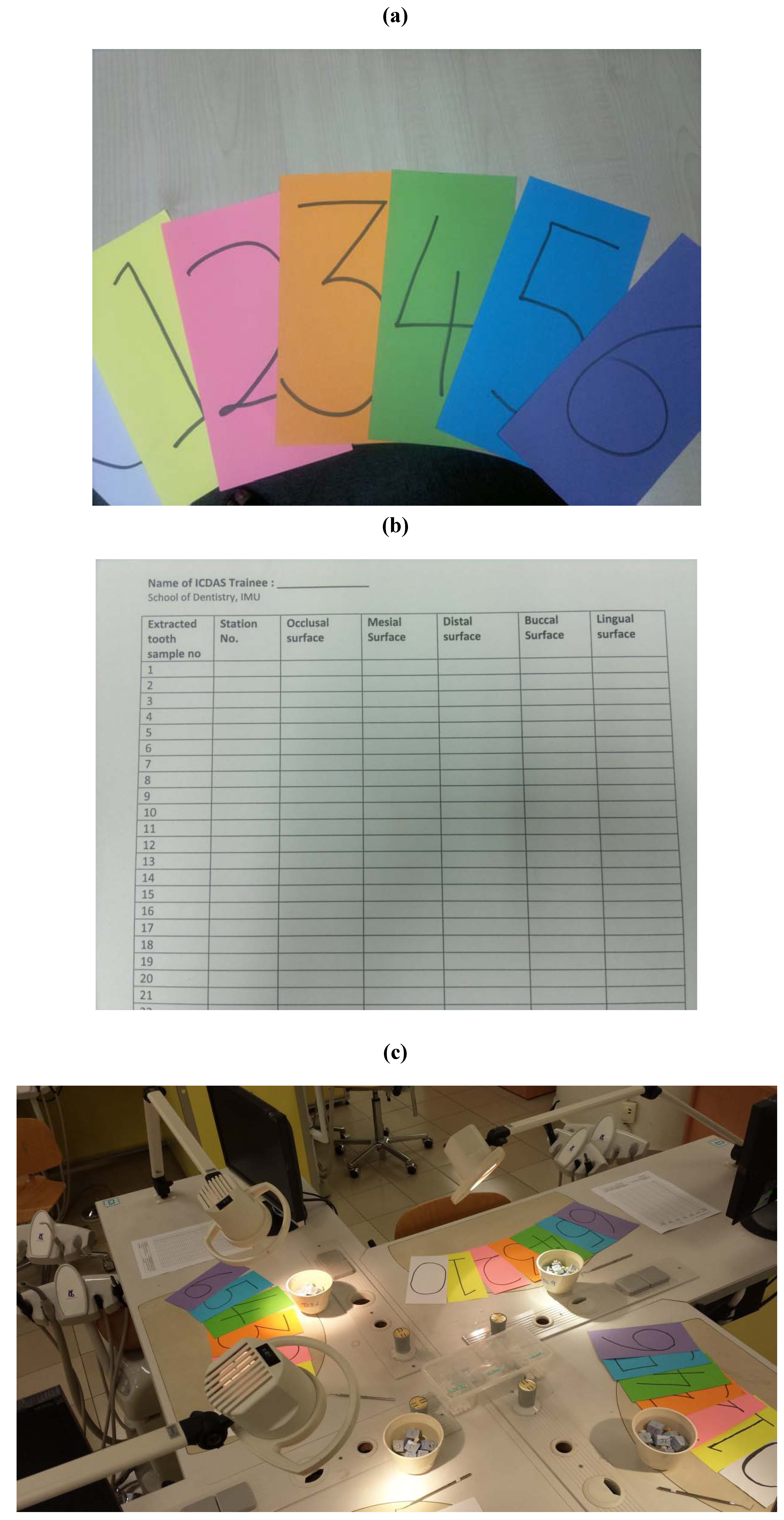
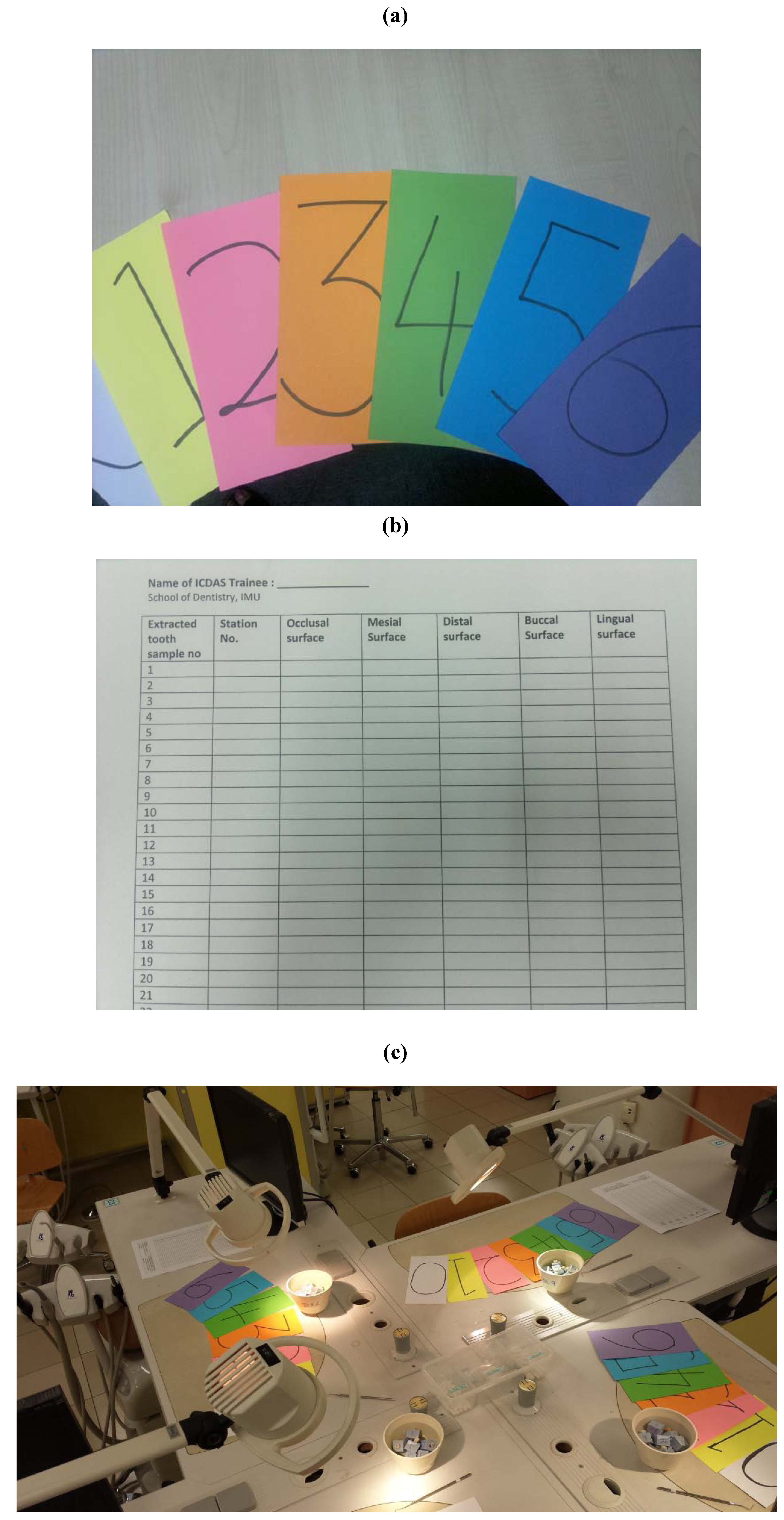
During this time the tools, including support materials for the stations at which the Reference Set would be distributed, were decided upon
. Finally, assessment forms were printed and the date and venue for the first IMU Faculty Staff training workshop was decided upon (
Figure 5a).
Two intensive four-hour half day ICDAS workshops were conducted for all the academic staff with 100% attendance in two groups using a dental simulation laboratory (DSL) as the venue. It was ideal for the purpose as it came equipped with individual light lamps, three way-air spray syringes and computer screen monitors for each staff member (
Figure 5c). These doubled up as seating places for staff during the lecture/discussion components, and as stations, each with a tooth, during the calibration exercises. The staff were tasked with going through the 90-min E-learning program a few days before coming for the workshop [
8].
Figure 5.
Different colored cards depicting the ICDAS codes used for photograph discussion exercise by the trainees (a). Form used by the ICDAS trainees in the extracted teeth exercise (b). Venue set-up for the ICDAS workshop (c).
Figure 5.
Different colored cards depicting the ICDAS codes used for photograph discussion exercise by the trainees (a). Form used by the ICDAS trainees in the extracted teeth exercise (b). Venue set-up for the ICDAS workshop (c).
The workshop consisted of a presentation on ICDAS, its background, coding criteria and its application in management using preventive and minimal invervention by the ICDAS Task Force members. This was followed by a discussion and asessment exercise using Camsight digital images of different ICDAS coded caries lesions (
Figure 5a). Thereafter, a discussion and assessment exercise on selected surfaces of extracted teeth from the Reference Set depicting the ICDAS codes was carried out. The teeth were pre-soaked in water for 12 h and the staff were required to use the 3-way air spray syringe to dry the teeth before coding them [
11]. Periodontal probes were provided to each participant as adjuncts in the assessment exercise, together with admonitions never to cause surface damage with them (
Figure 5c).
Figure 6.
Student Training Workshop: Photo discussion session.
Figure 6.
Student Training Workshop: Photo discussion session.
Two more identical workshops were carried out subsequently in October 2012 for BDS Year One students and more recently for the new batch of students in November 2013 (
Figure 6).
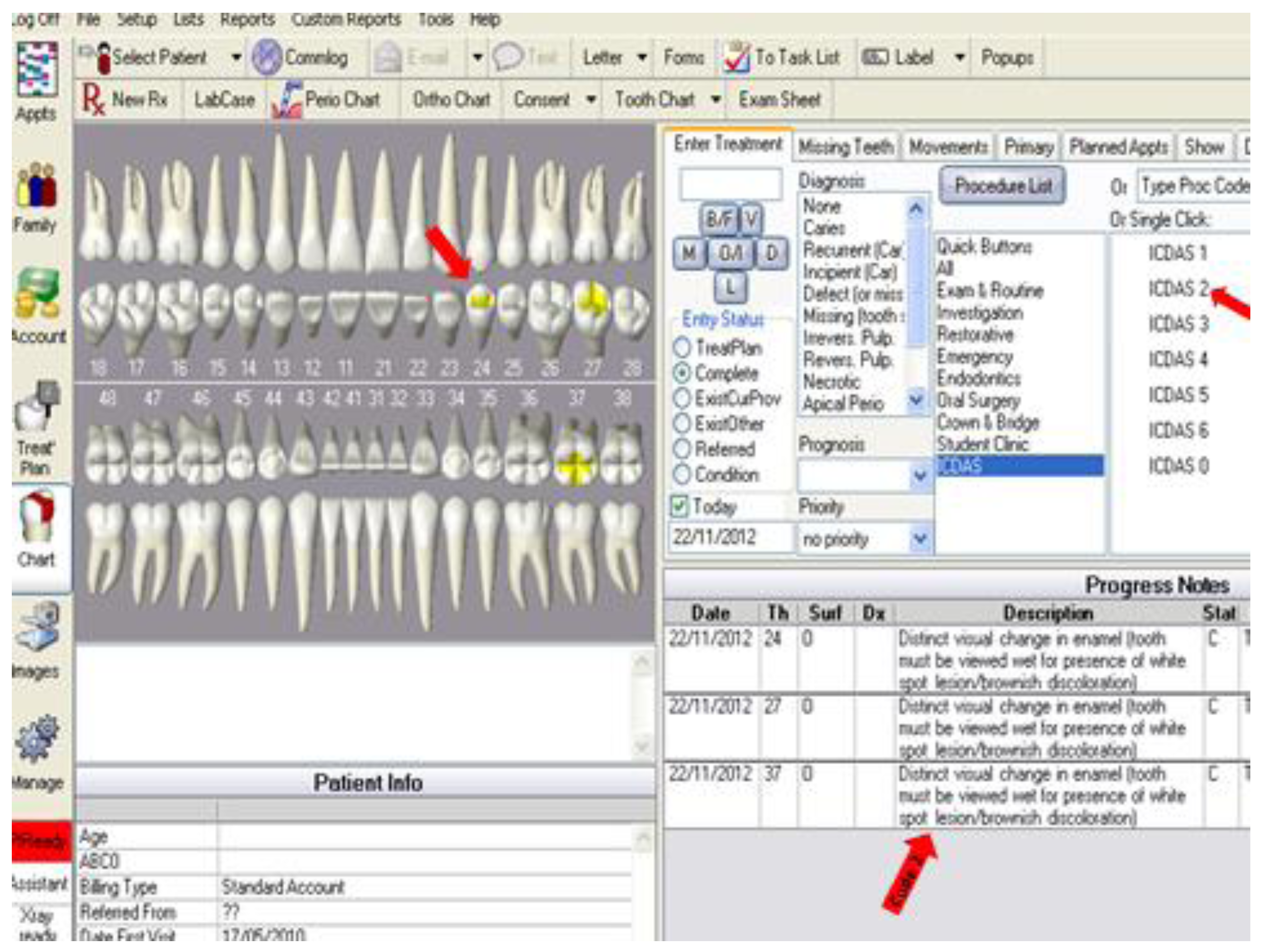
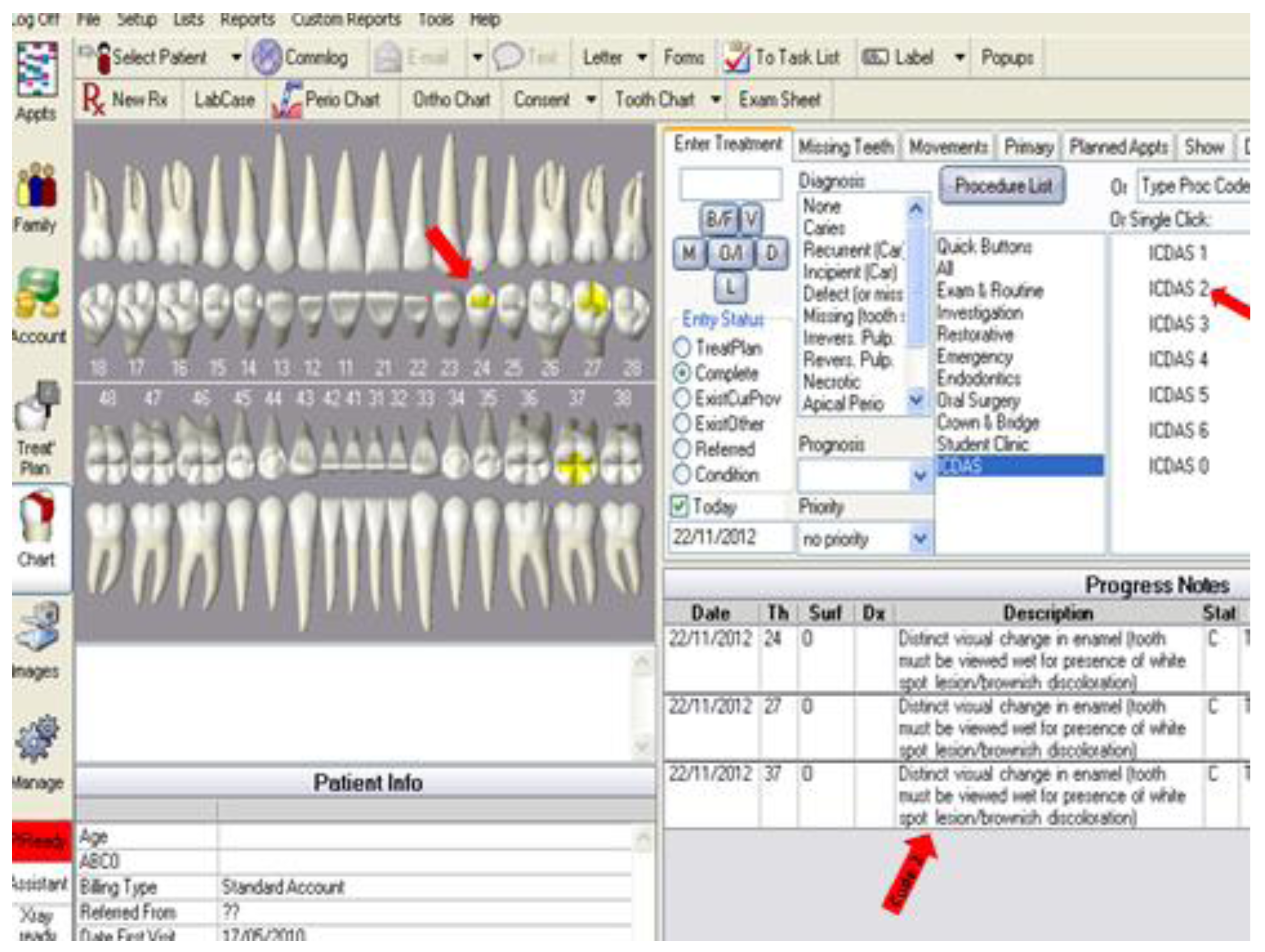
From November to January, all relevant teaching materials including handouts for students and evaluation criteria of caries-related and cavity preparation projects were identified, monitored and modified to accommodate the ICDAS concept. Additionally, documents specifying the methods of evaluation for grading carious lesions and the use of such grades to inform choice of types of management were replaced with ones using the ICDAS system. Finally, simultaneously with those changes the modification of the existing electronic system of clinical charting in patient clinics to allow insertion of ICDAS coding was completed (
Figure 7). The red arrows in this figure show the progression of steps when charting the tooth with its respective ICDAS code. All the ICDAS code criteria have been previously inserted into this charting system during its modification and automatically pops up once the tooth is coded.
Figure 7.
Modification of electronic system of clinical charting.
Figure 7.
Modification of electronic system of clinical charting.
After these changes had been accomplished it was evident that the ICDAS system had achieved a satisfactory level of penetration into the clinical and academic usage of all staff and students. It was noted that the level of calibration was not at a level required for clinical trial, but it was serving the purpose of encouraging early detection and preventive management of initial non-cavitated lesions and eliminating overtreatment of more advanced lesions.
Nevertheless, it was the intention of the Task Force to begin a rolling programme of high level calibration of all staff and students. To initiate that work, an expert (KE) with several years of experience in the system was invited in May 2013 to evaluate the progress of implementation at IMU and begin the high level calibration process.
The calibration process was done at a further half day ICDAS training workshop for staff. That began as previously with a discussion of Camsight digital images followed by scoring the extracted teeth from the IMU Reference set led by the expert.
All staff together with the expert then moved through a series of stations each with an extracted tooth from the IMU Reference Set chosen by the expert. A clearly indicated surface on each tooth was graded by each of those present and the data collected centrally. Following a further discussion, the grading process was repeated in exactly the same way but without those scoring having access to their original scores.
In more detail, 12 members of academic staff and one external ICDAS expert twice graded the surfaces of 30 extracted teeth which had been mounted and stored as described above. The intra-examiner weighted kappa statistics were calculated and are presented with their confidence limits in
Table 1.
Table 1.
The intra-examiner weighted kappa statistics.
Table 1.
The intra-examiner weighted kappa statistics.
Intra-trainee agreement before and after
the training | Weighted Kappa a | Standard error | 95% CI |
|---|
| Trainee 1 | 0.897 | 0.039 | 0.820 to 0.974 |
| Trainee 2 | 0.761 | 0.078 | 0.608 to 0.913 |
| Trainee 3 | 0.820 | 0.060 | 0.702 to 0.937 |
| Trainee 4 | 0.803 | 0.043 | 0.719 to 0.886 |
| Trainee 5 | 0.806 | 0.050 | 0.708 to 0.904 |
| Trainee 6 | 0.817 | 0.042 | 0.734 to 0.899 |
| Trainee 7 | 0.481 | 0.099 | 0.288 to 0.675 |
| Trainee 8 | 0.878 | 0.048 | 0.785 to 0.971 |
| Trainee 9 | 0.829 | 0.060 | 0.712 to 0.946 |
| Trainee 10 | 0.800 | 0.054 | 0.693 to 0.906 |
| Trainee 11 | 0.705 | 0.082 | 0.545 to 0.865 |
| Trainee 12 | 0.734 | 0.088 | 0.562 to 0.905 |
The data obtained by each staff member at the second examination was then analyzed against the same data from the expert using weighted kappa statistics to provide measures on inter-examiner variability. Those values together with their confidence limits are presented in
Table 2.
Table 2.
The inter-examiner weighted kappa statistics (expert versus trainee/staff member).
Table 2.
The inter-examiner weighted kappa statistics (expert versus trainee/staff member).
| Agreement between trainer and trainee after the training | Weighted Kappa a | Standard error | 95% CI |
|---|
| Trainer vs. Trainee 1 | 0.805 | 0.048 | 0.710 to 0.900 |
| Trainer vs. Trainee 2 | 0.795 | 0.064 | 0.670 to 0.920 |
| Trainer vs. Trainee 3 | 0.688 | 0.076 | 0.540 to 0.836 |
| Trainer vs. Trainee 4 | 0.754 | 0.050 | 0.656 to 0.852 |
| Trainer vs. Trainee 5 | 0.782 | 0.058 | 0.668 to 0.896 |
| Trainer vs. Trainee 6 | 0.894 | 0.030 | 0.835 to 0.953 |
| Trainer vs. Trainee 7 | 0.747 | 0.055 | 0.639 to 0.855 |
| Trainer vs. Trainee 8 | 0.707 | 0.062 | 0.586 to 0.828 |
| Trainer vs. Trainee 9 | 0.818 | 0.050 | 0.720 to 0.915 |
| Trainer vs. Trainee 10 | 0.746 | 0.063 | 0.623 to 0.869 |
| Trainer vs. Trainee 11 | 0.636 | 0.091 | 0.458 to 0.814 |
| Trainer vs. Trainee 12 | 0.570 | 0.081 | 0.411 to 0.729 |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}