

Implementation of Virtual Reality in Preclinical Pediatric Dentistry Learning: A Comparison Between Simodont® and Conventional Methods

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
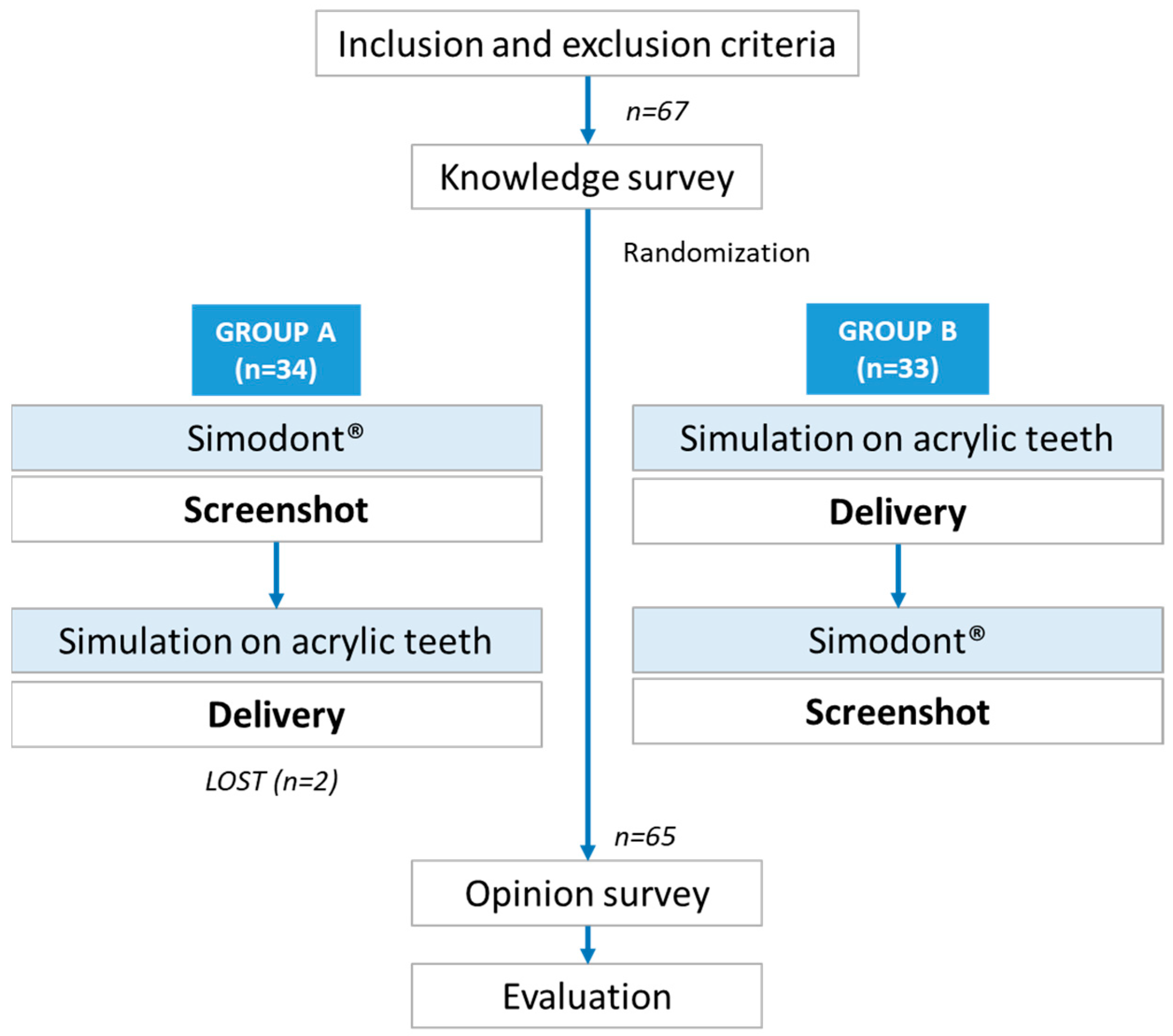
2.1. Study Design and Ethics Statement
2.2. Study Sample and Participants
2.3. Study Procedure and Outcomes
2.4. Randomization
2.5. Statistical Analysis
3. Results
3.1. Participants
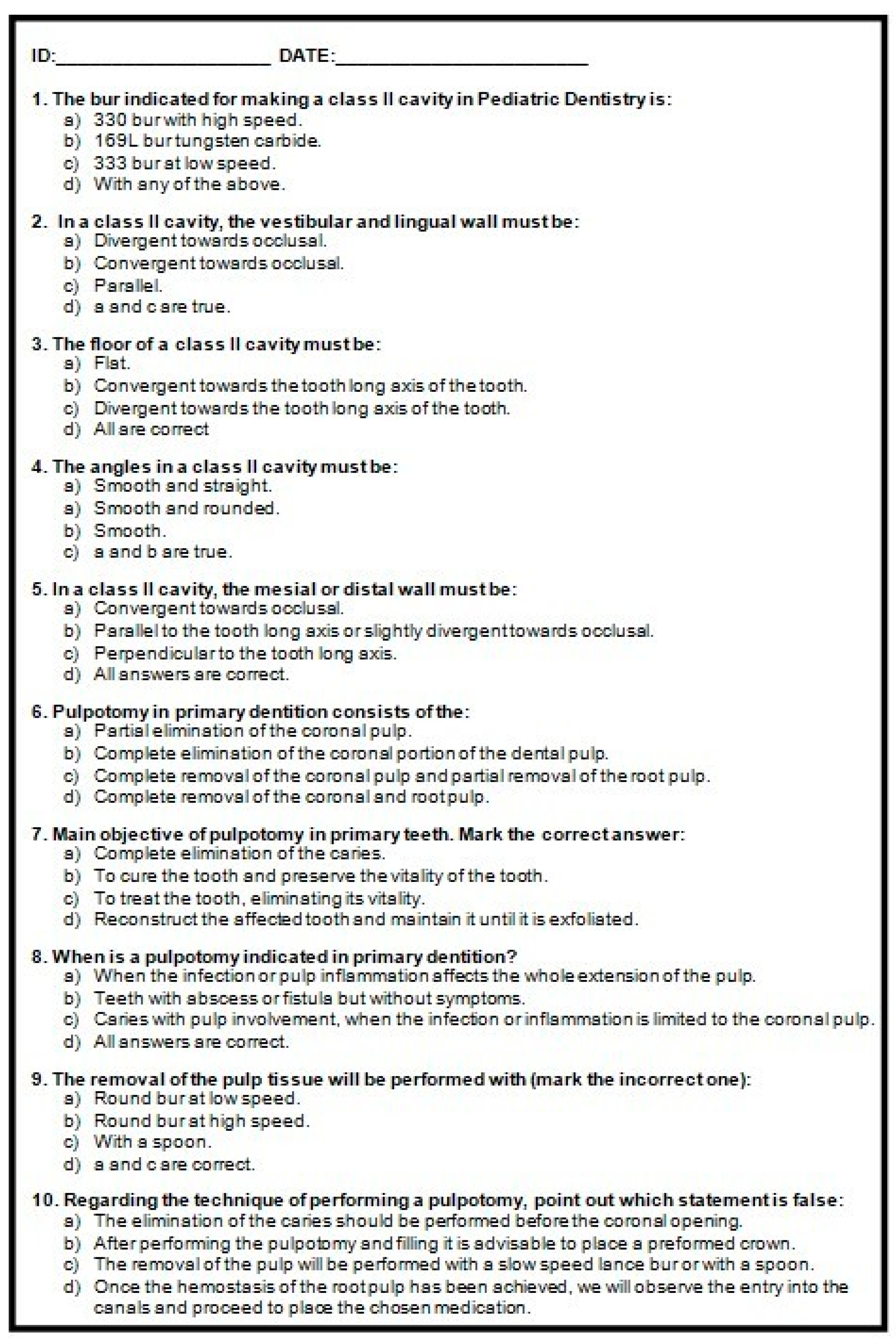
3.2. Influence of Theoretical Knowledge on Preclinical Practices
3.3. Comparison of Scores Obtained in the Simulated Practices with Simodont® and SAT
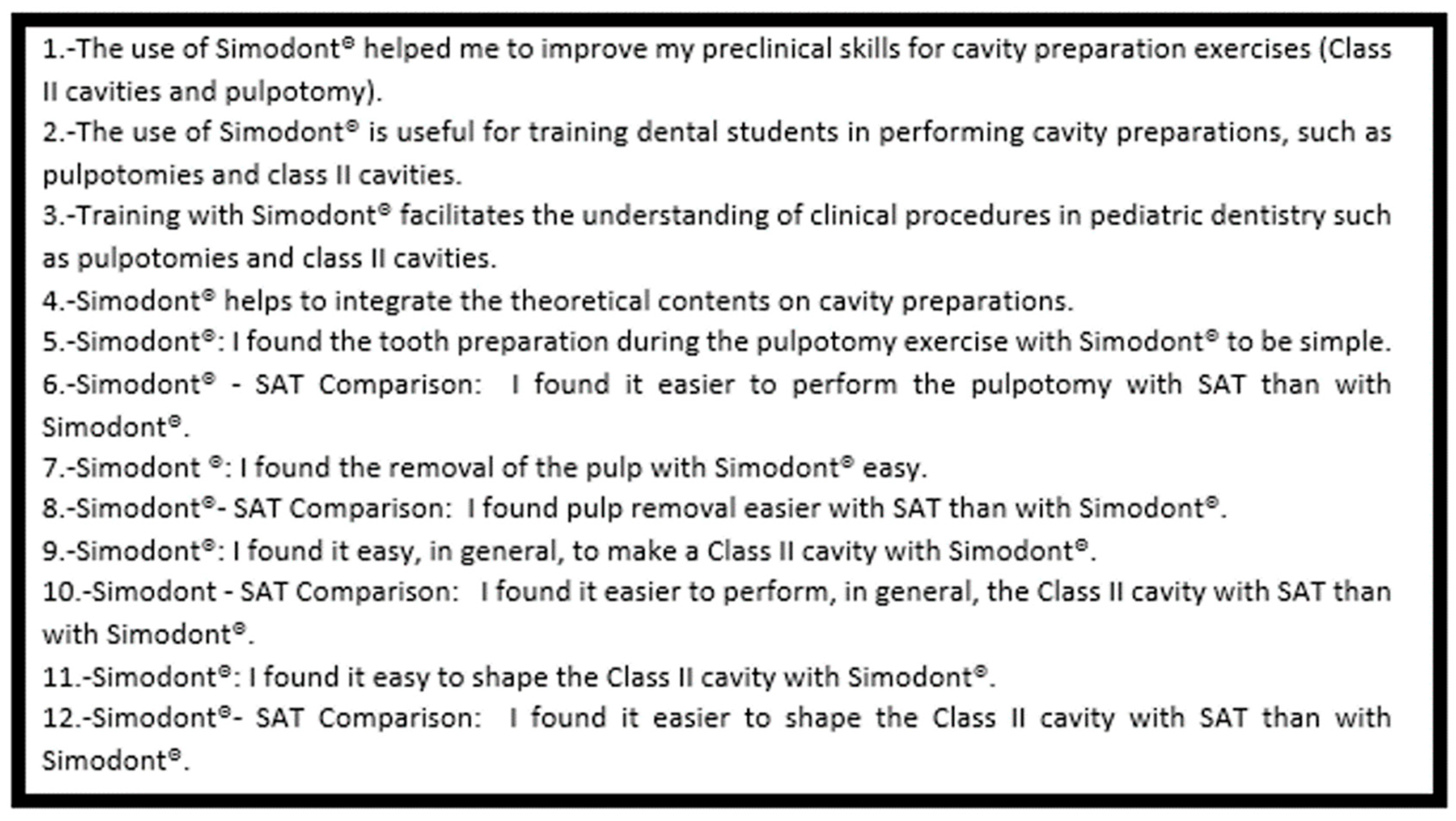
3.4. Assessment of Students’ Perceptions
3.5. Intra- and Inter-Examiner Agreement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B
References
- Escobar-Castillejos, D.; Noguez, J.; Neri, L.; Magan, A.; Benes, B. A review of simulators with haptic devices for medical training. J. Med. Syst. 2016, 40, 104. [Google Scholar] [CrossRef]
- Chan, D.C.; Pruzler, K.B.; Caughman, W.F. Simulation with preclinical operative dentistry courses-3 year retrospective results. J. Dent. Educ. 2000, 64, 224. [Google Scholar]
- Perry, S.; Bridges, S.M.; Burrow, M.F. A review of the use of simulation in dental education. Simul. Healthc. 2015, 10, 31–37. [Google Scholar] [CrossRef]
- Vincent, M.; Joseph, D.; Amory, C.; Paoli, N.; Ambrosini, P.; Mortier, É.; Tran, N. Contribution of Haptic Simulation to Analogic Training Environment in Restorative Dentistry. J. Dent. Educ. 2020, 84, 367–376. [Google Scholar] [CrossRef]
- Leung, A.L.-S.; Yeung, C.; Chu, S.; Wong, A.W.-Y.; Yu, O.Y.; Chu, C.-H. Use of Computer Simulation in Dental Training with Special Reference to Simodont. Dent. J. 2021, 9, 125. [Google Scholar] [CrossRef] [PubMed]
- Jasinevicius, T.R.; Landers, M.; Nelson, S.; Urbankova, A. An evaluation of two dental simulation systems: Virtual reality versus contemporary non-computer-assisted. J. Dent. Educ. 2004, 68, 1151–1162. [Google Scholar] [CrossRef] [PubMed]
- Rhienmora, P.; Haddawy, P.; Suebnukarn, S.; Dailey, M.N. Intelligent dental training simulator with objective skill assessment and feedback. Artif. Intell. Med. 2011, 52, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, J.A. Use of simulation technology in dental education. J. Dent. Educ. 2001, 65, 1225–1231. [Google Scholar] [CrossRef]
- Zafar, S.; Lai, Y.; Sexton, C.; Siddiqi, A. Virtual Reality as a novel educational tool in pre-clinical paediatric dentistry training: Students’ perceptions. Int. J. Paediatr. Dent. 2020, 30, 791–797. [Google Scholar] [CrossRef]
- Makransky, G.; Bonde, M.T.; Wulff, J.S.G.; Wandarl, J.; Hood, M.; Creed, P.; Bache, I.; Silahtaroglu, A.; Nørremølle, A. Simulation based virtual learning environment in medical genetics conunseling: An example of bridging the gap between theory and practice in medical education. BMC Med. Educ. 2016, 16, 98. [Google Scholar] [CrossRef]
- Bakr, M.M.; Massey, W.L.; Alexander, H. Can virtual simulators replace traditional preclinical teaching methods: A students’ perspective? Int. J. Dent. Oral. Health 2015, 2, 1–6. [Google Scholar]
- Söderström, T.; Häll, L.; Nilsson, T.; Ahlqvist, J. Computer simulation training in thealth care education: Fuelling refection-in action? Simul. Gaming 2014, 45, 805–828. [Google Scholar] [CrossRef]
- Aliaga, I.; Pedrera-Canal, M.; Vera, V.; Rico Martín, S.; Garcia Barbero, E.; Leal-Hernández, O.; Moran, J.M. Preclinical assessment methodology using a dental simulator during dental students’ first and third years. J. Oral. Sci. 2020, 62, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Suebnukarn, S.; Haddawy, P.; Rhienmora, P.; Jittimanee, P.; Viratket, P. Augmented kinematic feedback from haptic virtual reality for dental skill acquisition. J. Dent. Educ. 2010, 74, 1357–1366. [Google Scholar] [CrossRef] [PubMed]
- Bakr, M.M.; Massey, W.; Alexander, H. Students’ evaluation of a 3DVR haptic device (Simodont®). Does early exposure to haptic feedback during preclinical dental education enhance the development of psychomotor skills? Int. J. Dent. Clin. 2014, 6, 1–7. [Google Scholar]
- Roy, E.; Bakr, M.M.; George, R. The need for virtual reality simulators in dental education: A review. Saudi Dent. J. 2017, 29, 41–47. [Google Scholar] [CrossRef]
- Zafar, S.; Siddiqi, A.; Yasir, M.; Zachar, J.J. Pedagogical development in local anaesthetic training in paediatric dentistry using virtual reality simulator. Eur. Arch. Paediatr. Dent. 2021, 22, 667–674. [Google Scholar] [CrossRef]
- Plessas, A. Computerized Virtual Reality Simulation in Preclinical Dentistry: Can a Computerized Simulator Replace the Conventional Phantom Heads and Human Instruction? Simul. Healthc. 2017, 12, 332–338. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Murbay, S.; Neelakantan, P.; Chang, J.W.W.; Yeung, S. Evaluation of the introduction of a dental virtual simulator on the performance of undergraduate dental students in the pre-clinical operative dentistry course. Eur. J. Dent. Educ. 2020, 24, 5–16. [Google Scholar] [CrossRef]
- de Boer, I.R.; Bakker, D.R.; Serrano, C.M.; Koopman, P.; Wesselink, P.R.; Vervoorn, J.M. Innovation in dental education: The “On-the-Fly” approach to simultaneous development, implementation and evidence collection. Eur. J. Dent. Educ. 2018, 22, 215–222. [Google Scholar] [CrossRef]
- Mirghani, I.; Mushtaq, F.; Allsop, M.J.; Al-Saud, L.M.; Tickhill, N.; Potter, C.; Keeling, A.; Mon-Williams, M.A.; Manogue, M. Capturing differences in dental training using a virtual reality simulator. Eur. J. Dent. Educ. 2018, 22, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Hattori, A.; Tonami, K.I.; Tsuruta, J.; Hideshima, M.; Kimura, Y.; Nitta, H.; Araki, K. Effect of the haptic 3D virtual reality dental training simulator on assessment of tooth preparation. J. Dent. Sci. 2022, 17, 514–520. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
{kind=link}
| Correct (1 Point) | Incorrect (0 Points) | |
|---|---|---|
| Yes | No |
| Yes | No |
| Yes | No |
| Yes | No |
| Yes | No |
| Correct (1 Point) | Incorrect (0 Points) | |
|---|---|---|
| Yes | No |
| No | Yes |
| No | Yes |
| Yes | No |
| No | Yes |
| Previous Knowledge | Kendall Tau | Spearman Rho | ||
|---|---|---|---|---|
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| Class II Simodont® | −0.007 | 0.948 | −0.006 | 0.959 |
| Class II SAT | 0.130 | 0.198 | 0.177 | 0.156 |
| Pulpotomy Simodont® | −0.014 | 0.891 | −0.017 | 0.890 |
| Pulpotomy SAT | −0.114 | 0.263 | −0.139 | 0.265 |
| Mean | 95% CI | SD | |||
|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||
| Class II | Simodont® | 1.9692 | 1.9889 | 2.2496 | 1.13150 |
| SAT | 2.5692 | 2.2627 | 2.8758 | 1.23705 | |
| Pulpotomy | Simodont® | 2.9231 | 2.6984 | 3.1477 | 0.90671 |
| SAT | 3.6000 | 3.3237 | 3.8763 | 1.11524 | |
| Simodont® vs. Simulation on Acrylic Teeth | Kendall Tau | Spearman Rho | Wilcoxon Rank Test | ||
|---|---|---|---|---|---|
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | p-Value | |
| Class II | 0.289 | 0.005 * | 0.343 | 0.005 * | 0.001 * |
| Pulpotomy | 0.103 | 0.331 | 0.123 | 0.330 | <0.001 * |
| Agree | Neutral | Disagree | ꭓ2 | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | p-Value | ||
| Simodont® Perception | 1 | 28 | 41.8 | 26 | 38.8 | 11 | 16.4 | 0.019 * |
| 2 | 35 | 52.2 | 21 | 31.3 | 9 | 13.4 | <0.001 * | |
| 3 | 40 | 59.7 | 20 | 29.9 | 5 | 7.5 | <0.001 * | |
| 4 | 43 | 64.2 | 20 | 29.9 | 2 | 3 | <0.001 * | |
| Simodont® vs. SAT | 5 | 5 | 7.5 | 23 | 34.3 | 37 | 55.2 | <0.001 * |
| 6 | 49 | 73.1 | 8 | 11.9 | 8 | 11.9 | <0.001 * | |
| 7 | 14 | 20.9 | 19 | 28.4 | 32 | 47.8 | 0.019 * | |
| 8 | 46 | 68.7 | 16 | 23.9 | 3 | 4.5 | <0.001 * | |
| 9 | 21 | 31.3 | 25 | 37.3 | 19 | 28.4 | 0.650 | |
| 10 | 47 | 70.1 | 13 | 19.4 | 5 | 7.5 | <0.001 * | |
| 11 | 20 | 29.9 | 21 | 31.3 | 24 | 35.8 | 0.819 | |
| 12 | 47 | 70.1 | 14 | 20.9 | 4 | 6 | <0.001 * | |
| Inter-Examiner | Intra-Examiner | |||||||
|---|---|---|---|---|---|---|---|---|
| Simodont® | SAT | Simodont® | SAT | |||||
| Kappa Value | Agreement | Kappa Value | Agreement | Kappa Value | Agreement | Kappa Value | Agreement | |
| Question | Class II | |||||||
| 1 | 0.894 | Strong | 1 | Almost perfect | 1 | Almost perfect | 0.900 | Strong |
| 2 | 0.792 | Moderate | 0.700 | Moderate | 0.898 | Strong | 0.900 | Strong |
| 3 | 0.681 | Moderate | 0.898 | Strong | 0.886 | Strong | 0.700 | Moderate |
| 4 | 0.828 | Strong | 1 | Almost perfect | 0.608 | Moderate | 0.659 | Moderate |
| 5 | 0.681 | Moderate | 0.794 | Moderate | 0.898 | Strong | 1.000 | Almost perfect |
| Question | Pulpotomy | |||||||
| 1 | 0.765 | Moderate | 0.692 | Moderate | 1 | Almost perfect | 0.886 | Strong |
| 2 | 0.612 | Moderate | 1 | Almost perfect | 1 | Almost perfect | 1 | Almost perfect |
| 3 | 0.737 | Moderate | 0.773 | Moderate | 1 | Almost perfect | 1 | Almost perfect |
| 4 | 1 | Almost perfect | 0.643 | Moderate | 0.894 | Strong | 0.773 | Moderate |
| 5 | 0.828 | Strong | 0.794 | Moderate | 1 | Almost perfect | 0.900 | Minimal |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caleya, A.M.; Martín-Vacas, A.; Mourelle-Martínez, M.R.; de Nova-Garcia, M.J.; Gallardo-López, N.E. Implementation of Virtual Reality in Preclinical Pediatric Dentistry Learning: A Comparison Between Simodont® and Conventional Methods. Dent. J. 2025, 13, 51. https://doi.org/10.3390/dj13020051
Caleya AM, Martín-Vacas A, Mourelle-Martínez MR, de Nova-Garcia MJ, Gallardo-López NE. Implementation of Virtual Reality in Preclinical Pediatric Dentistry Learning: A Comparison Between Simodont® and Conventional Methods. Dentistry Journal. 2025; 13(2):51. https://doi.org/10.3390/dj13020051
Chicago/Turabian StyleCaleya, Antonia M., Andrea Martín-Vacas, María Rosa Mourelle-Martínez, Manuel Joaquín de Nova-Garcia, and Nuria E. Gallardo-López. 2025. "Implementation of Virtual Reality in Preclinical Pediatric Dentistry Learning: A Comparison Between Simodont® and Conventional Methods" Dentistry Journal 13, no. 2: 51. https://doi.org/10.3390/dj13020051
APA StyleCaleya, A. M., Martín-Vacas, A., Mourelle-Martínez, M. R., de Nova-Garcia, M. J., & Gallardo-López, N. E. (2025). Implementation of Virtual Reality in Preclinical Pediatric Dentistry Learning: A Comparison Between Simodont® and Conventional Methods. Dentistry Journal, 13(2), 51. https://doi.org/10.3390/dj13020051