
A Systematic Review of Stem Cell Applications in Maxillofacial Regeneration




Abstract

1. Introduction
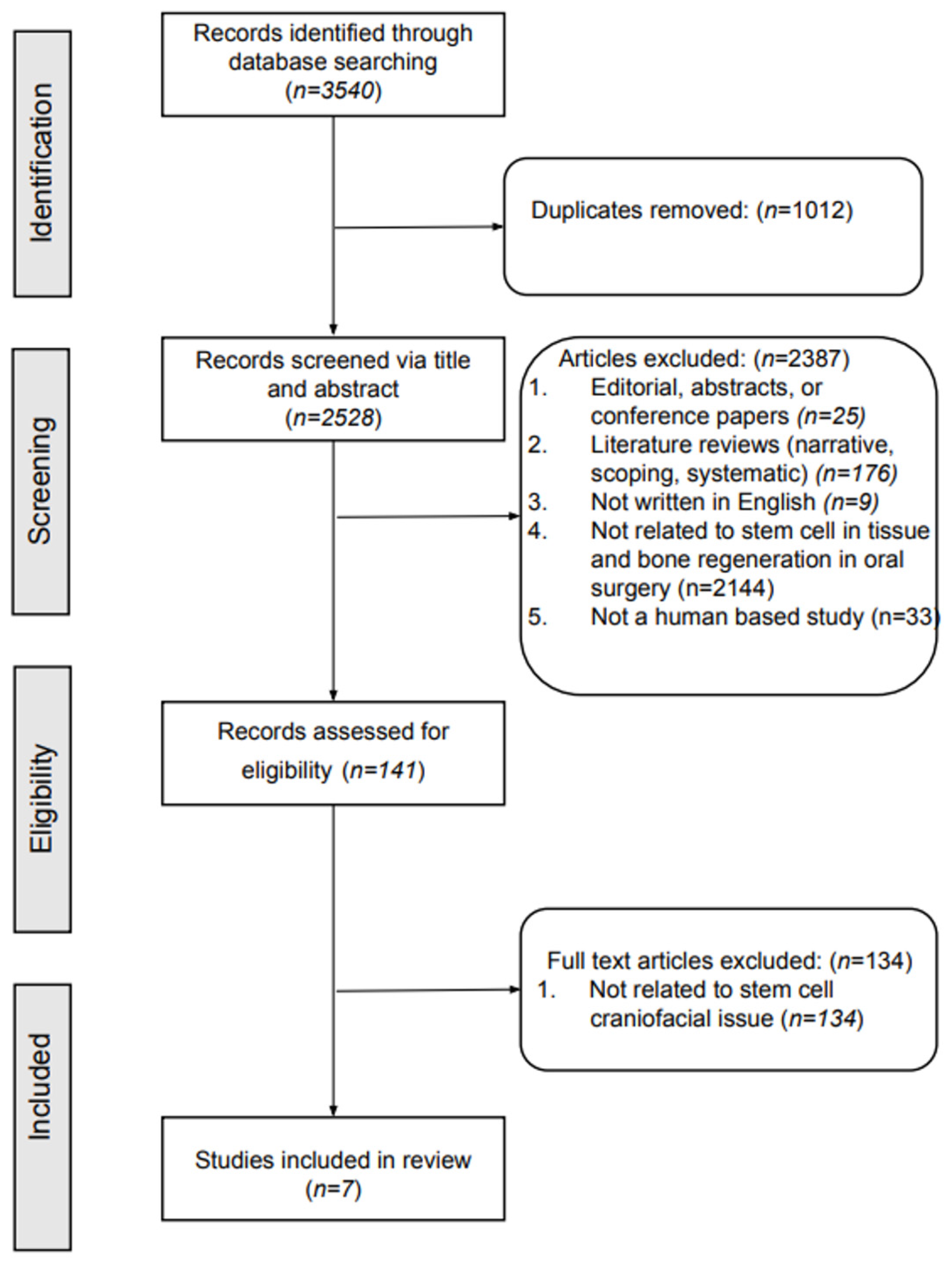
2. Methods
3. Results
3.1. Safety and Efficacy of Stem Cell Therapy
3.2. Bone Regeneration and Quality
3.3. Risk of Bias Assessment
3.4. Limitations of Included Studies
4. Discussion
4.1. Safety and Immune Modulation
4.2. Efficacy and Quality of Regenerated Bone
4.3. Clinical Implications and Future Directions
4.4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mao, A.S.; Mooney, D.J. Regenerative medicine: Current therapies and future directions. Proc. Natl. Acad. Sci. USA 2015, 112, 14452–14459. [Google Scholar] [CrossRef] [PubMed]
- Sunil, P.; Manikandhan, R.; Muthu, M.; Abraham, S. Stem cell therapy in oral and maxillofacial region: An overview. J. Oral Maxillofac. Pathol. 2012, 16, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Fortier, L.A. Stem Cells: Classifications, Controversies, and Clinical Applications. Vet. Surg. 2005, 34, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Bluteau, G.; Luder, H.-U.; De Bari, C.; Mitsiadis, T. Stem cells for tooth engineering. Eur. Cells Mater. 2008, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Piera-Velazquez, S.; Jimenez, S.A. Endothelial to Mesenchymal Transition: Role in Physiology and in the Pathogenesis of Human Diseases. Physiol. Rev. 2019, 99, 1281–1324. [Google Scholar] [CrossRef]
- Rowe, R.G.; Daley, G.Q. Induced pluripotent stem cells in disease modelling and drug discovery. Nat. Rev. Genet. 2019, 20, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Yamanaka, S. Induction of Pluripotent Stem Cells from Mouse Embryonic and Adult Fibroblast Cultures by Defined Factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef]
- Patel, D.M.; Shah, J.; Srivastava, A. Therapeutic Potential of Mesenchymal Stem Cells in Regenerative Medicine. Stem Cells Int. 2013, 2013, 496218. [Google Scholar] [CrossRef] [PubMed]
- Bose, S.; Vahabzadeh, S.; Bandyopadhyay, A. Bone Tissue Engineering Using 3D Printing. Mater. Today 2013, 16, 496–504. [Google Scholar] [CrossRef]
- Pedroni, A.C.F.; Sarra, G.; de Oliveira, N.K.; Moreira, M.S.; Deboni, M.C.Z.; Marques, M.M. Cell sheets of human dental pulp stem cells for future application in bone replacement. Clin. Oral Investig. 2019, 23, 2713–2721. [Google Scholar] [CrossRef]
- Simion, M.; Baldoni, M.; Rasperini, G.; Zaffe, D. Vertical Bone Augmentation with Simultaneous Implant Placement Using Membrane Technique. J. Oral Implantol. 2013, 39, 3–18. [Google Scholar]
- Soufizadeh, P.; Mansouri, V.; Ahmadbeigi, N. A review of animal models utilized in preclinical studies of approved gene therapy products: Trends and insights. Lab. Anim. Res. 2024, 40, 17. [Google Scholar] [CrossRef] [PubMed]
- Margiana, R.; Markov, A.; Zekiy, A.O.; Hamza, M.U.; Al-Dabbagh, K.A.; Al-Zubaidi, S.H.; Hameed, N.M.; Ahmad, I.; Sivaraman, R.; Kzar, H.H.; et al. Clinical application of mesenchymal stem cell in regenerative medicine: A narrative review. Stem Cell Res. Ther. 2022, 13, 366. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Mao, H.Q. Electrospun scaffolds for stem cell engineering. Adv. Drug Deliv. Rev. 2009, 61, 1084–1096. [Google Scholar] [CrossRef] [PubMed]
- Rizk, A.; Rabie, A.B. Human dental pulp stem cells expressing transforming growth factor β3 transgene for cartilage-like tissue engineering. Cytotherapy 2013, 15, 712–725. [Google Scholar] [CrossRef] [PubMed]
- Khojasteh, A.; Estaminejad, M.B. Vertical Bone Augmentation with Simultaneous Implant Placement Using Particulate Min-eralized Bone and Mesenchymal Stem Cells: A Preliminary Study in Rabbit. J. Oral Implantol. 2013, 39, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomized Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Asahina, I.; Kagami, H.; Agata, H.; Honda, M.J.; Sumita, Y.; Inoue, M.; Nagamura-Inoue, T.; Tojo, A. Clinical Outcome and 8-Year Follow-Up of Alveolar Bone Tissue Engineering for Severely Atrophic Alveolar Bone Using Autologous Bone Marrow Stromal Cells with Platelet-Rich Plasma and β-Tricalcium Phosphate Granules. J. Clin. Med. 2021, 10, 5231. [Google Scholar] [CrossRef]
- Feng, S.-W.; Su, Y.-H.; Lin, Y.-K.; Wu, Y.-C.; Huang, Y.-H.; Yang, F.-H.; Chiang, H.-J.; Yen, Y.; Wang, P.D.-Y. Small blood stem cells for enhancing early osseointegration formation on dental implants: A human phase I safety study. Stem Cell Res. Ther. 2021, 12, 380. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, W.; Osugi, M.; Kawai, T.; Hibi, H. First-in-human study and clinical case reports of the alveolar bone regeneration with the secretome from human mesenchymal stem cells. Head Face Med. 2016, 12, 5. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, W.; Watanabe, J.; Toyama, N.; Osugi, M.; Sakaguchi, K.; Hibi, H. Clinical Study of Bone Regeneration by Conditioned Medium from Mesenchymal Stem Cells after Maxillary Sinus Floor Elevation. Implant. Dent. 2017, 26, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, A.; Manescu, A.; Langer, M.; Rustichelli, F.; Desiderio, V.; Paino, F.; De Rosa, A.; Laino, L.; D’Aquino, R.; Tirino, V.; et al. Three Years after Transplants in Human Mandibles, Histological and In-Line Holotomography Revealed That Stem Cells Regenerated a Compact Rather Than a Spongy Bone: Biological and Clinical Implications. Stem Cells Transl. Med. 2013, 2, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Gjerde, C.; Mustafa, K.; Hellem, S.; Rojewski, M.; Gjengedal, H.; Yassin, M.A.; Feng, X.; Skaale, S.; Berge, T.; Rosen, A.; et al. Cell therapy induced regeneration of severely atrophied mandibular bone in a clinical trial. Stem Cell Res. Ther. 2018, 9, 213. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.S.; Aurora, J.K.; Dubey, K.N.; Chauhan, H.; Saxena, M.; Ganvir, S.R. A comparative evaluation of bone regeneration using mesenchymal stem cells versus blood coagulum in sinus augmentation procedures. Natl. J. Maxillofac. Surg. 2021, 12, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Trounson, A.; McDonald, C. Stem Cell Therapies in Clinical Trials: Progress and Challenges. Cell Stem Cell 2015, 17, 11–22. [Google Scholar] [CrossRef]
- Madrigal, M.; Rao, K.S.; Riordan, N.H. A review of therapeutic effects of mesenchymal stem cell secretions and induction of secretory modification by different culture methods. J. Transl. Med. 2014, 12, 260. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, Y.; Li, Q.; Liu, K.; Hou, J.; Shao, C.; Wang, Y. Immunoregulatory mechanisms of mesenchymal stem and stromal cells in inflammatory diseases. Nat. Rev. Nephrol. 2018, 14, 493–507. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Romanos, G.E. The role of primary stability for successful immediate loading of dental implants. A literature review. J. Dent. 2010, 38, 612–620. [Google Scholar] [CrossRef]
- Caplan, A.I. Mesenchymal Stem Cells: Time to Change the Name! Stem Cells Transl. Med. 2017, 6, 1445–1451. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Databases Database Link Search Date | Search Strategies | Number of Articles Found |
|---|---|---|
| Scopus https://www.scopus.com/home.uri (accessed on 2 February 2024) | (TITLE-ABS-KEY (“stem cell*”) AND TITLE-ABS-KEY (“bone regeneration” OR “tissue regeneration” OR “tissue engineering” OR “bone graft*”) AND TITLE-ABS-KEY (dent*)) AND PUBYEAR > 2013 AND PUBYEAR < 2023 AND (EXCLUDE (EXACTKEYWORD, “Animals”) OR EXCLUDE (EXACTKEYWORD, “Nonhuman”) OR EXCLUDE (EXACTKEYWORD, “Animal”) OR EXCLUDE (EXACTKEYWORD, “Animal Experiment”) OR EXCLUDE (EXACTKEYWORD, “Mouse”) OR EXCLUDE (EXACTKEYWORD, “Animal Tissue”) OR EXCLUDE (EXACTKEYWORD, “Animal Cell”) OR EXCLUDE (EXACTKEYWORD, “Rat”) OR EXCLUDE (EXACTKEYWORD, “Mice”) OR EXCLUDE (EXACTKEYWORD, “Animal Model”) OR EXCLUDE (EXACTKEYWORD, “Rats”)) | 1897 |
| PubMed https://pubmed.ncbi.nlm.nih.gov (accessed on 2 February 2024) | ((“stem cell*” [Title/Abstract]) AND (“bone regeneration” [Title/Abstract] OR “tissue regeneration” [Title/Abstract] OR “tissue engineering” [Title/Abstract] OR “bone graft*” [Title/Abstract]) AND “dent*” [Title/Abstract]) AND ((humans[Filter]) | 980 |
| WoS https://access.clarivate.com/login?app=wos (accessed on 2 February 2024) | ((TS = (“stem cell*”)) AND TS = (“bone regeneration” OR “tissue regeneration” OR “tissue engineering” OR “bone graft*”)) AND TS = (dent*) AND ((ALL = ((“population groups” not “animal models”))) OR ALL = (men OR women OR patient OR female OR male OR subjects OR adult)) NOT ALL = (“animal models”) AND (PY = (“2023” OR “2022” OR “2021” OR “2020” OR “2019” OR “2018” OR “2017” OR “2016” OR “2015” OR “2014” OR “2013”)) | 488 |
| OVID https://ovidsp.ovid.com/ (accessed on 2 February 2024) | ((stem cell*.ti,ab) AND ((bone regeneration.ti,ab) OR (tissue regeneration.ti,ab) OR (tissue engineering.ti,ab) OR (bone graft*.ti,ab)) AND (dent*.ti,ab) AND ((men) OR (women) OR (patient) OR (female) OR (male) OR (subjects) OR (adult)) NOT (animal models)) limit to yr = “2013–2023” | 108 |
| Cochrane Library https://www.cochranelibrary.com/advanced-search (accessed on 2 February 2024) | Title Abstract Keyword—((stem cell*) AND ((bone regeneration) OR (tissue regeneration) OR (tissue engineering) OR (bone graft *)) AND (dent*) AND ((men) OR (women) OR (patient) OR (female) OR (male) OR (subjects) OR (adult)) NOT (animal models)) | 65 |
| Dentistry & Oral Sciences Source—Ebscohost https://www.ebsco.com/products/research-databases/dentistry-oral-sciences-source (accessed on 2 February 2024) | TI(((stem cell*) AND ((bone regeneration) OR (tissue regeneration) OR (tissue engineering) OR (bone graft*)) AND (dent*))) AND AB(((stem cell*) AND ((bone regeneration) OR (tissue regeneration) OR (tissue engineering) OR (bone graft*)) AND (dent*))) AND ((men) OR (women) OR (patient) OR (female) OR (male) OR (subjects) OR (adult)) NOT (animal models) | 2 |
| Author (Year) | Country | Study Aim | Study Design | Stem Cell Type | Dental Surgical Procedures | Outcomes |
|---|---|---|---|---|---|---|
| Asahina et al. (2021) [20] | Japan | Examine the safety and efficacy of bone tissue engineering for patients with a severely atrophic alveolar bone | Cohort study | Bone marrow stem cells | Sinus lift | During treatment and follow-ups for 66 months, no side effects or health concerns were noted. Therapy was safe and effective. |
| Feng et al. (2021) [21] | Taiwan | Assess safety and efficacy of regeneration in the case of large bony defects | Phase I study | Small blood stem cells | Various types | All implants were implanted successfully. Elevated levels of eotaxin, fibroblast growth factor, monocyte chemoattractant protein 1, macrophage-derived chemokine, and interleukin-17A found in patients after small blood cell treatment. |
| Giuliani et al. (2013) [24] | Italy | Assess the stability and quality of regenerated bone and vessel network | Cohort study | Dental pulp stem cells | Bone graft | Three years after grafting in the mandible, the regenerated bone was uniformly vascularized and exhibited a compact structure, rather than a cancellous one. |
| Gjerde et al. (2018) [25] | Norway | Evaluate bone regeneration using marrow-derived mesenchymal stromal cells | Clinical Trial | Bone marrow-derived stromal cells | Sinus augmentation | The bone marrow cells induced significant new bone formation. |
| Gupta et al. (2021) [26] | India | Evaluate quality and quantity of bone formation in maxillary sinus lift and implant stability of atrophic maxilla | Case–control | Mesenchymal stem cells | Sinus augmentation | Of the 40 sinus lifts performed and 42 implants placed, all showed primary stability. |
| Katagiri et al. (2016) [22] | Japan | Examine safety and osteogenic potential of mesenchymal stem cells in bone | Case–control | Mesenchymal stem cells | Bone graft | Bone marrow-derived mesenchymal stem cells were used safely with less inflammation and showed great osteogenic potential. |
| Katagiri et al. (2017) [23] | Japan | Evaluate safety of secretome of bone marrow-derived mesenchymal stem cells for maxillary sinus lift | Case–control | Mesenchymal stem cells | Bone graft | Bone formation was clinically confirmed in all cases. The secretome of bone marrow-derived mesenchymal stem cells was used safely. |
| Author (Year) | Selection Bias a | Performance Bias b | Detection Bias c | Attrition Bias d | Reporting Bias e | Other Bias f | Overall Risk of Bias g |
|---|---|---|---|---|---|---|---|
| Asahina et al. (2021) [20] | Low | High | Low | Low | Low | Medium | Moderate |
| Feng et al. (2021) [21] | Medium | High | Medium | Medium | Low | High | High |
| Giuliani et al. (2013) [24] | Low | Medium | Low | Medium | Medium | Medium | Moderate |
| Gjerde et al. (2018) [25] | Medium | High | Medium | High | Medium | Low | High |
| Gupta et al. (2021) [26] | Low | Medium | Low | Low | Low | Low | Low |
| Katagiri et al. (2016) [22] | High | High | High | Medium | High | Medium | High |
| Katagiri et al. (2017) [23] | High | High | Medium | Medium | Medium | Medium | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, M.; Sadri, M.; Katz, M.; Schwartz, C.; Mohajeri, A. A Systematic Review of Stem Cell Applications in Maxillofacial Regeneration. Dent. J. 2024, 12, 315. https://doi.org/10.3390/dj12100315
Hung M, Sadri M, Katz M, Schwartz C, Mohajeri A. A Systematic Review of Stem Cell Applications in Maxillofacial Regeneration. Dentistry Journal. 2024; 12(10):315. https://doi.org/10.3390/dj12100315
Chicago/Turabian StyleHung, Man, Mahsa Sadri, Melanie Katz, Connor Schwartz, and Amir Mohajeri. 2024. "A Systematic Review of Stem Cell Applications in Maxillofacial Regeneration" Dentistry Journal 12, no. 10: 315. https://doi.org/10.3390/dj12100315
APA StyleHung, M., Sadri, M., Katz, M., Schwartz, C., & Mohajeri, A. (2024). A Systematic Review of Stem Cell Applications in Maxillofacial Regeneration. Dentistry Journal, 12(10), 315. https://doi.org/10.3390/dj12100315