


Distribution of Dental Fluorosis in the Southern Zone of Ecuador: An Epidemiological Study

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Calibration
2.6. Examination
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carey, C.M. Focus on Fluorides: Update on the Use of Fluoride for the Prevention of Dental Caries. J. Evid.-Based Dent. Pract. 2014, 14, 95–102. [Google Scholar] [CrossRef]
- de Almeida, B.S.; da Silva Cardoso, V.E.; Buzalaf, M.A.R. Fluoride Ingestion from Toothpaste and Diet in 1- to 3-Year-Old Brazilian Children. Community Dent. Oral Epidemiol. 2007, 35, 53–63. [Google Scholar] [CrossRef]
- Revelo-Mejía, I.A.; Hardisson, A.; Rubio, C.; Gutiérrez, Á.J.; Paz, S. Dental Fluorosis: The Risk of Misdiagnosis—A Review. Biol. Trace. Elem. Res. 2021, 199, 1762–1770. [Google Scholar] [CrossRef]
- Mohd Nor, N.A.; Chadwick, B.L.; Farnell, D.J.J.; Chestnutt, I.G. Factors Associated with Dental Fluorosis among Malaysian Children Exposed to Different Fluoride Concentrations in the Public Water Supply. J. Public Health Dent. 2021, 81, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Tamer, M.N. Sources of Fluoride for Human Exposure; Elsevier: Amsterdam, The Netherlands, 2018; pp. 786–791. [Google Scholar] [CrossRef]
- Do, L.G.; Ha, D.H.; Roberts-Thomson, K.F.; Spencer, A.J. Dental Fluorosis in the Australian Adult Population. Aust. Dent. J. 2020, 65, S47–S51. [Google Scholar] [CrossRef] [PubMed]
- Zohoori, F.V.; Moynihan, P.J.; Omid, N.; Abuhaloob, L.; Maguire, A. Impact of Water Fluoride Concentration on the Fluoride Content of Infant Foods and Drinks Requiring Preparation with Liquids before Feeding. Community Dent. Oral Epidemiol. 2012, 40, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Del Carmen Aguilar-Díaz, F.; Morales-Corona, F.; Cintra-Viveiro, A.C.; de la Fuente-Hernández, J. Prevalence of Dental Fluorosis in Mexico 2005–2015: A Literature Review. Salud Publica Mex. 2017, 59, 306–313. [Google Scholar] [CrossRef]
- Cuenca-León, K.; Pacheco-Quito, E.-M.; Granda-Granda, Y.; Vélez-León, E.; Zarzuelo-Castañeda, A. Phytotherapy. A Solution to Decrease Antifungal Resistance in the Dental Field. Biomolecules 2022, 12, 789. [Google Scholar] [CrossRef]
- Livia, M.; Andalo, T.; Noronha, S.; Myaki, I.; Martins Paiva, S. Uso de Fluoruros. Man. De Ref. Para Proced. Clínicos En Odontopediatría 2014, 57–66. [Google Scholar]
- Iheozor-Ejiofor, Z.; Worthington, H.V.; Walsh, T.; O’Malley, L.; Clarkson, J.E.; Macey, R.; Alam, R.; Tugwell, P.; Welch, V.; Glenny, A.M. Water Fluoridation for the Prevention of Dental Caries. Cochrane Database Syst. Rev. 2015, 2015, CD010856. [Google Scholar] [CrossRef]
- Mclaren, L.; Singhal, S. Does Cessation of Community Water Fluoridation Lead to an Increase in Tooth Decay? A Systematic Review of Published Studies. J. Epidemiol. Community Health 2016, 70, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Adas, C.; Garbin, S.; Felipe, L.; José, A.; Garbin, I.; Adas, S.; Moimaz, S.; Saliba, O. La Fluoración Del Agua de Abastecimiento Público: Abordaje Bioético, Legal y Político. Rev. Bioét. 2017, 25, 328–337. [Google Scholar]
- Vélez-León, E.; Albaladejo-Martínez, A.; Pacheco-Quito, E.-M.; Armas-Vega, A.; Delgado-Gaete, A.; Pesántez-Ochoa, D.; Melo, M. Developmental Enamel Defects in Children from the Southern Region of Ecuador. Children 2022, 9, 1755. [Google Scholar] [CrossRef]
- Ramires, I.; Buzalaf, M.A.R. A Fluoretação Da Água de Abastecimento Público e Seus Benefícios No Controle Da Cárie Dentária: Cinqüenta Anos No Brasil. Cien. Saude Colet. 2007, 12, 1057–1065. [Google Scholar] [CrossRef]
- Whelton, H.P.; Spencer, A.J.; Do, L.G.; Rugg-Gunn, A.J. Fluoride Revolution and Dental Caries: Evolution of Policies for Global Use. J. Dent. Res. 2019, 98, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, F.R.; Aljohani, M.; Botev, L.; O’malley, L.; Glenny, A.M. Dental Fluorosis Prevalence in Saudi Arabia. Saudi Dent. J. 2021, 33, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Zohoori, F.V.; Omid, N.; Sanderson, R.A.; Valentine, R.A.; Maguire, A. Fluoride Retention in Infants Living in Fluoridated and Non-Fluoridated Areas: Effects of Weaning. Br. J. Nutr. 2019, 121, 74–81. [Google Scholar] [CrossRef]
- Maguire, A.; Omid, N.; Abuhaloob, L.; Moynihan, P.J.; Zohoori, F.v. Fluoride Content of Ready-to-Feed (RTF) Infant Food and Drinks in the UK. Community Dent. Oral Epidemiol. 2012, 40, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Molina-Frechero, N.; Castañeda-Castaneira, E.; Bologna-Molina, R.; Carlos, J.; Juárez-López, L.A. Fluorosis Endémica En Una Población Asentada a La Altitud de 2,100 M§. Rev. Mex. Pediatr. 2006, 73, 220–224. [Google Scholar]
- Sharma, D.; Singh, A.; Verma, K.; Paliwal, S.; Sharma, S.; Dwivedi, J. Fluoride: A Review of Pre-Clinical and Clinical Studies. Environ. Toxicol. Pharmacol. 2017, 56, 297–313. [Google Scholar] [CrossRef]
- Gu, L.S.; Wei, X.; Ling, J.Q. Etiology, Diagnosis, Prevention and Treatment of Dental Fluorosis. Zhonghua Kou Qiang Yi Xue Za Zhi 2020, 55, 296–301. [Google Scholar] [CrossRef]
- Programa Nacional de Fluoracion Del Agua. Available online: https://aplicaciones.msp.gob.ec/salud/archivosdigitales/documentosDirecciones/dnvcs/archivos/PROGRAMA%20NACIONAL%20DE%20FLUORURACION.pdf (accessed on 23 January 2023).
- OPS/OMS|Flúor En El Agua de Consumo. Available online: https://www3.paho.org/hq/index.php?option=com_content&view=article&id=8193:2013-fluor-agua-consumo&Itemid=39798&lang=es#gsc.tab=0 (accessed on 23 January 2023).
- Pan American Health Organization; Organización Panamericana de la Salud. Programa Nacional de Fluoruración de La Sal En Ecuador: Presupuesto de Gastos de Operación Para: 1. Estudio de Concentración de Flúor En Agua de Consumo Humano; 2. Estudio de Concentración de Flúor En Orina, 3. Estudio Epidemiológico de Salud Bucal, 4. Programa de Capacitación y Comunicación. 1994. Available online: https://iris.paho.org/handle/10665.2/36699 (accessed on 15 September 2022).
- Reglamento de La Ley de Yodizacion y Fluorización Para La Sal de Consumo Humano. Available online: https://aplicaciones.msp.gob.ec/salud/archivosdigitales/documentosDirecciones/dnvcs/archivos/REGLAMENTO%20LEY%20DE%20YODIZACION%20DE%20SAL.pdf (accessed on 23 January 2023).
- León, E.V.; Flores, M.J.R.; Guzmán, M.A.G.; León, K.C. Análisis de La Concentración de Flúor En El Agua de Abastecimiento Público Del Cantón Cuenca, Como Posible Factor Que Contribuye al Desarrollo de Fluorosis Dental. Anal. Claves Pensam. Contemp. 2019, 23, 6. [Google Scholar] [CrossRef]
- Vélez-León, E.; Albaladejo, A.; Cuenca-León, K.; Jiménez-Romero, M.; Armas-Vega, A.; Melo, M. Prevalence of Caries According to the ICDAS II in Children from 6 and 12 Years of Age from Southern Ecuadorian Regions. Int. J. Environ. Res. Public Health 2022, 19, 7266. [Google Scholar] [CrossRef] [PubMed]
- Parra, J.; Astudillo, D.; Cedillo, N.; Ordoñez, G.; Sempértegui, F. Fluorosis Dental: Prevalencia, Grados de Severidad y Factores de Riesgo En Niños de 7 a 13 Años Del Cantón Cuenca. Maskana 2012, 3, 41–49. [Google Scholar] [CrossRef]
- Del, A.; Armas-Vega, C.; González-Martínez, F.-D.; Rivera-Martínez, M.-S.; Mayorga-Solórzano, M.-R.-F.; Banderas-Benítez, V.-E.; Guevara-Cabrera, O.-F. Factors Associated with Dental Fluorosis in Three Zones of Ecuador. J. Clin. Exp. Dent. 2019, 11, 42–50. [Google Scholar] [CrossRef]
- Moimaz, S.A.S.; Saliba, O.; Marques, L.B.; Garbin, C.A.S.; Saliba, N.A. Dental Fluorosis and Its Influence on Children’s Life. Braz. Oral Res. 2015, 29, S1806-S1806-83242015000100214. [Google Scholar] [CrossRef] [PubMed]
- Yeung, C.A. Book Review: Oral Health Surveys: Basic Methods, 5th Edition. Br. Dent. J. 2014, 217, 333. [Google Scholar] [CrossRef]
- Petersen, P.E. Changing Oral Health Profiles of Children in Central and Eastern Europe-Challenges for the 21st Century; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Dean, H.T. Classification of Mottled Enamel Diagnosis. J. Am. Dent. Assoc. 1934, 21, 1421–1426. [Google Scholar] [CrossRef]
- Griffin, S.O.; Beltrán, E.D.; Lockwood, S.A.; Barker, L.K. Esthetically Objectionable Fluorosis Attributable to Water Fluoridation. Community Dent. Oral Epidemiol. 2002, 30, 199–209. [Google Scholar] [CrossRef]
- Saldarriaga, A.; Restrepo, M.; Rojas-Gualdrón, D.F.; Gualdrón, G.; De, T.; Carvalho, S.; Afonso, M.; Buzalaf, R.; Santos-Pinto, L.; Jeremias, F. Dental Fluorosis According to Birth Cohort and Fluoride Markers in an Endemic Region of Colombia. Sci. World J. 2021, 2021, 6662940. [Google Scholar] [CrossRef]
- de Lourdes Azpeitia-Valadez, M.; Ángel Sánchez-Hernández, M.; Rodríguez-Frausto, M.; Ángel, M.; Tel, S.-H. Factores de Riesgo Para Fluorosis Dental En Escolares de 6 a 15 Años de Edad. Rev. Med. Inst. Mex. Seguro Soc. 2009, 47, 265–270. [Google Scholar]
- Perez, A.G.; Perez, N.G.P.; Rojas, A.I.F.; Ortega, C.C.B.; Pineda, A.E.G.A.; Gutierrez, T.V. Marginalization and Fluorosis Its Relationship with Dental Caries in Rural Children in Mexico: A Cross-Sectional Study. Community Dent. Health 2020, 37, 216–222. [Google Scholar] [CrossRef]
- Agudelo, D.; Gómez, P.; Parra, Y.; Jiménez, L.; Cristancho, G. Factores Asociados a La Fluorosis Dental En Niños De 8 a 12 Años En El Municipio Restrepo Meta. Pain Clin. Soc. Trat. Directriz 2019, 2, 1–13. [Google Scholar]
- Michel-Crosato, E.; Raggio, D.P.; Coloma-Valverde, A.N.D.J.; Lopez, E.F.; Alvarez-Velasco, P.L.; Medina, M.V.; Balseca, M.C.; Quezada-Conde, M.D.C.; de Almeida Carrer, F.C.; Romito, G.A.; et al. Oral Health of 12-Year-Old Children in Quito, Ecuador: A Population-Based Epidemiological Survey. BMC Oral Health 2019, 19, 184. [Google Scholar] [CrossRef] [PubMed]
- Viteri-García, A.; Parise-Vasco, J.M.; Cabrera-Dávila, M.J.; Zambrano-Bonilla, M.C.; Ordonez-Romero, I.; Maridueña-León, M.G.; Caiza-Rennella, A.; Zambrano-Mendoza, A.; Ponce-Faula, C.; Pérez-Granja, M.; et al. Prevalencia e Incidencia de Caries Dental y Efecto Del Cepillado Dental Acompañado de Barniz de Flúor En Escolares de Islas Galápagos, Ecuador: Protocolo Del Estudio EESO-Gal. Medwave 2020, 20, e7974. [Google Scholar] [CrossRef] [PubMed]
- Maita Sarango, D.; Vélez León, E.; Sarmiento Criollo, P.; Jiménez Romero, M. FLUOROSIS DENTAL EN LA ETNIA SARAGURO, LOJA-ECUADOR 2018. Revista Científica UOD: Universidad Odontológica Dominicana 2021, 9, 1–6. [Google Scholar]
- Filho, A.P.R.; Chávez, B.A.; Giacaman, R.A.; Frazão, P.; Cury, J.A. Community Interventions and Strategies for Caries Control in Latin American and Caribbean Countries. Braz. Oral Res. 2021, 35, e054. [Google Scholar] [CrossRef] [PubMed]
- Cardenas, A.F.M.; Armas-Veja, A.; Villarreal, J.P.R.; de Siqueira, F.S.F.; Muniz, L.P.; Campos, V.S.; Reis, A.; Loguercio, A.D. Influence of the Mode of Application of Universal Adhesive Systems on Adhesive Properties to Fluorotic Enamel. Braz. Oral Res. 2019, 33, e120. [Google Scholar] [CrossRef]
- McGrady, M.G.; Ellwood, R.P.; Maguire, A.; Goodwin, M.; Boothman, N.; Pretty, I.A. The Association between Social Deprivation and the Prevalence and Severity of Dental Caries and Fluorosis in Populations with and without Water Fluoridation. BMC Public Health 2012, 12, 1122. [Google Scholar] [CrossRef]
- Ganta, S.; Yousuf, A.; Nagaraj, A.; Pareek, S.; Sidiq, M.; Singh, K.; Vishnani, P. Evaluation of Fluoride Retention Due to Most Commonly Consumed Estuarine Fishes Among Fish Consuming Population of Andhra Pradesh as a Contributing Factor to Dental Fluorosis: A Cross-Sectional Study. J. Clin. Diagn. Res. 2015, 9, ZC11–ZC15. [Google Scholar] [CrossRef]
- Jiménez-zabala, A.; Santa-marina, L.; Otazua, M.; Ayerdi, M.; Galarza, A.; Gallastegi, M.; Ulibarrena, E.; Molinuevo, A.; Anabitarte, A.; Ibarluzea, J. Ingesta de Flúor a Través Del Consumo de Agua de Abastecimiento Público En La Cohorte INMA-Gipuzkoa. Gac. Sanit. 2018, 32, 418–424. [Google Scholar] [CrossRef]
- Portella, P.D.; Dias, B.C.; Ferreira, P.; de Souza, J.F.; Wambier, L.; da Silva Assunção, L.R. The Association of Developmental Dental Defects and the Clinical Consequences in the Primary Dentition: A Systematic Review of Observational Studies. Pediatr. Dent. 2022, 44, 330–341. [Google Scholar] [PubMed]
- Cury, J.A.; Ricomini-Filho, A.P.; Perecin Berti, F.L.; Tabchoury, C.P.M. Systemic Effects (Risks) of Water Fluoridation. Braz. Dent. J. 2019, 30, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Mier, E.A.; Lippert, F. Teeth with Mild and Moderate Enamel Fluorosis Demonstrate Increased Caries Susceptibility In Vitro. J. Evid. Based Dent. Pract. 2017, 17, 293–295. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vélez-León, E.M.; Albaladejo-Martínez, A.; Cuenca-León, K.; Encalada-Verdugo, L.; Armas-Vega, A.; Melo, M. Caries Experience and Treatment Needs in Urban and Rural Environments in School-Age Children from Three Provinces of Ecuador: A Cross-Sectional Study. Dent. J. 2022, 10, 185. [Google Scholar] [CrossRef] [PubMed]
- Barathi, M.; Krishna, A.S.; Rajesh, N. Impact of Fluoride in Potable Water—An Outlook on the Existing Defluoridation Strategies and the Road Ahead. Coord. Chem. Rev. 2019, 387, 121–128. [Google Scholar] [CrossRef]
- di Giovanni, T.; Eliades, T.; Papageorgiou, S.N. Interventions for Dental Fluorosis: A Systematic Review. J. Esthet. Restor. Dent. 2018, 30, 502–508. [Google Scholar] [CrossRef]
- Bergamo, E.T.P.; Barbana, M.; Terada, R.S.S.; Cury, J.A.; Fujimaki, M. Fluoride Concentrations in the Water of Maringá, Brazil, Considering the Benefit/Risk Balance of Caries and Fluorosis. Braz. Oral Res. 2015, 29, 47. [Google Scholar] [CrossRef]
- Ling, Y.; Podgorski, J.; Sadiq, M.; Rasheed, H.; Eqani, S.A.M.A.S.; Berg, M. Monitoring and Prediction of High Fluoride Concentrations in Groundwater in Pakistan. Sci. Total Environ. 2022, 839, 156058. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
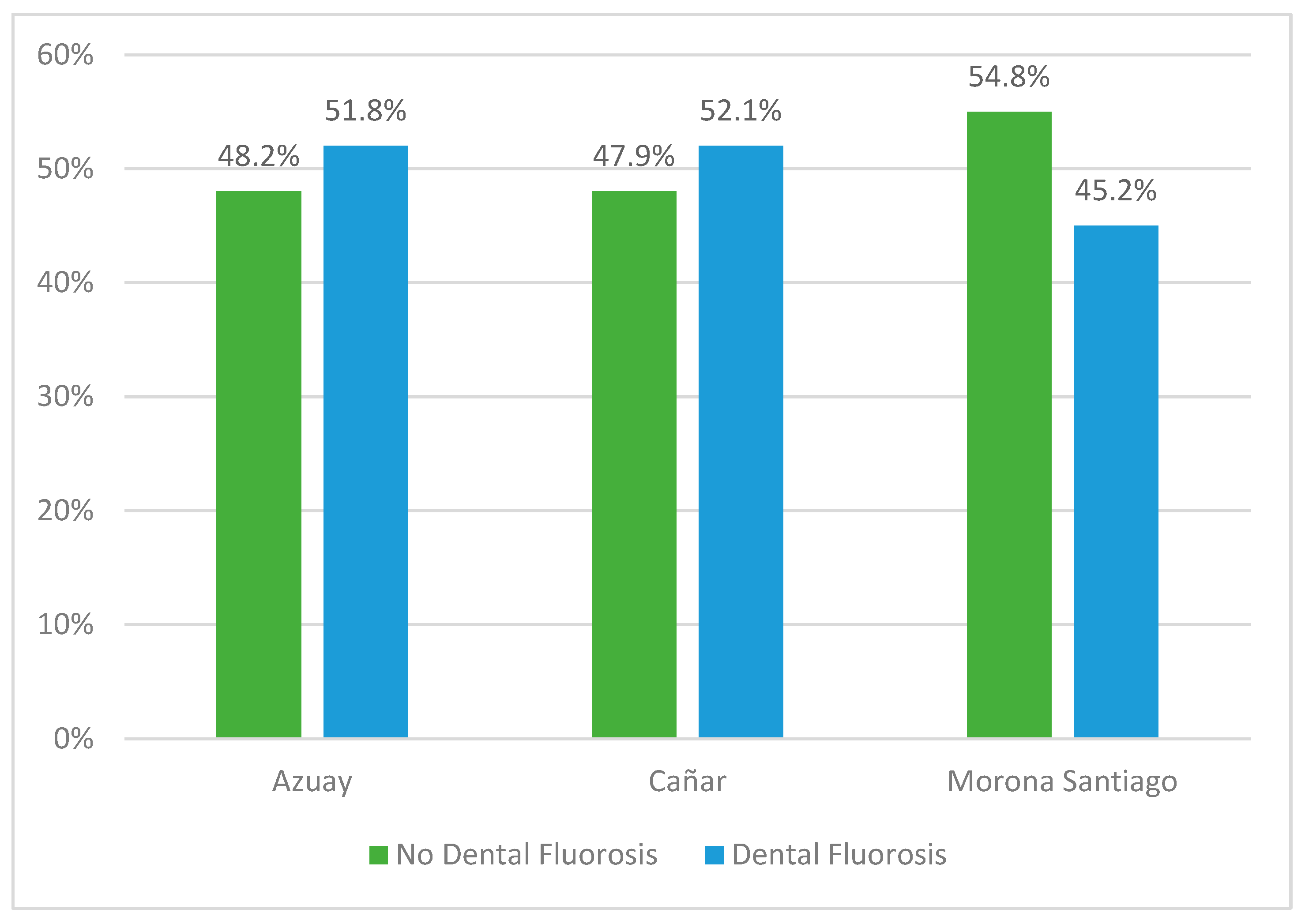
| Fluorosis | Azuay | Cañar | Morona Santiago | Total | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Normal | 276 | 48.2 | 292 | 47.9 | 232 | 54.8 | 800 | 49.8 |
| Debatable | 2 | 0.3 | 0 | 0.0 | 0 | 0.0 | 2 | 0.1 |
| Very slight | 116 | 20.2 | 105 | 17.2 | 73 | 17.3 | 294 | 18.3 |
| Slight | 113 | 19.7 | 108 | 17.7 | 64 | 15.1 | 285 | 17.7 |
| Moderate | 61 | 10.6 | 104 | 17.0 | 51 | 12.1 | 216 | 13.4 |
| Intense | 5 | 0.9 | 0 | 0.0 | 3 | 0.7 | 8 | 0.5 |
| Excluded | 0 | 0.0 | 1 | 0.2 | 0 | 0.0 | 1 | 0.1 |
| Fluorosis | Azuay | Cañar | Morona Santiago | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Urban | Rural | Urban | Rural | Urban | Rural | |||||||
| n | % | n | % | N | % | n | % | n | % | n | % | |
| Normal | 168 | 44.2 | 108 | 37.6 | 110 | 39.9 | 182 | 38.1 | 128 | 46.5 | 104 | 43.0 |
| Debatable | 2 | 0.7 | ||||||||||
| Very slight | 66 | 17.4 | 50 | 17.4 | 40 | 14.5 | 65 | 13.6 | 44 | 16.0 | 29 | 12.0 |
| Slight | 63 | 16.6 | 50 | 17.4 | 36 | 13.0 | 72 | 15.1 | 34 | 12.4 | 30 | 12.4 |
| Moderate | 45 | 11.8 | 16 | 5.6 | 35 | 12.7 | 69 | 14.4 | 27 | 9.8 | 24 | 9.9 |
| Intense | 3 | 0.8 | 2 | 0.7 | 2 | 0.7 | 1 | 0.4 | ||||
| Excluded | 1 | 0.2 | ||||||||||
| x2 | 26.400 | 1.866 | 6.300 | |||||||||
| p | <0.001 | 0.087 | 0.275 | |||||||||
| Debatable | Very Light | Light | Moderate | Intense | Exclude | x2 (p) | |||
|---|---|---|---|---|---|---|---|---|---|
| Sex | Men | n | 0 | 144 | 134 | 125 | 4 | 1 | 9.37 (0.095) |
| % | 0.0 | 35.3 | 32.8 | 30.6 | 1.0 | 0.2 | |||
| Woman | n | 2 | 150 | 151 | 91 | 4 | 0 | ||
| % | 0.5 | 37.7 | 37.9 | 22.9 | 1.0 | 0.0 | |||
| Age | 6 | n | 0 | 11 | 8 | 2 | 0 | 0 | 103.6 (0.000 **) |
| % | 0.0 | 52.4 | 38.1 | 9.5 | 0.0 | 0.0 | |||
| 7 | n | 1 | 41 | 58 | 14 | 0 | 0 | ||
| % | 0.9 | 36.0 | 50.9 | 12.3 | 0.0 | 0.0 | |||
| 8 | n | 0 | 58 | 55 | 22 | 2 | 0 | ||
| % | 0.0 | 42.3 | 40.1 | 16.1 | 1.5 | 0.0 | |||
| 9 | n | 1 | 50 | 47 | 32 | 3 | 1 | ||
| % | 0.7 | 37.3 | 35.1 | 23.9 | 2.2 | 0.7 | |||
| 10 | n | 0 | 38 | 43 | 42 | 0 | 0 | ||
| % | 0.0 | 30.9 | 35.0 | 34.1 | 0.0 | 0.0 | |||
| 11 | n | 0 | 47 | 50 | 25 | 2 | 0 | ||
| % | 0.0 | 37.9 | 40.3 | 20.2 | 1.6 | 0.0 | |||
| 12 | n | 0 | 49 | 24 | 79 | 1 | 0 | ||
| % | 0.0 | 32.0 | 15.7 | 51.6 | 0.7 | 0.0 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vélez-León, E.M.; Albaladejo-Martínez, A.; Ortíz-Ortega, P.; Cuenca-León, K.; Armas-Vega, A.; Melo, M. Distribution of Dental Fluorosis in the Southern Zone of Ecuador: An Epidemiological Study. Dent. J. 2023, 11, 71. https://doi.org/10.3390/dj11030071
Vélez-León EM, Albaladejo-Martínez A, Ortíz-Ortega P, Cuenca-León K, Armas-Vega A, Melo M. Distribution of Dental Fluorosis in the Southern Zone of Ecuador: An Epidemiological Study. Dentistry Journal. 2023; 11(3):71. https://doi.org/10.3390/dj11030071
Chicago/Turabian StyleVélez-León, Eleonor María, Alberto Albaladejo-Martínez, Paulina Ortíz-Ortega, Katherine Cuenca-León, Ana Armas-Vega, and María Melo. 2023. "Distribution of Dental Fluorosis in the Southern Zone of Ecuador: An Epidemiological Study" Dentistry Journal 11, no. 3: 71. https://doi.org/10.3390/dj11030071
APA StyleVélez-León, E. M., Albaladejo-Martínez, A., Ortíz-Ortega, P., Cuenca-León, K., Armas-Vega, A., & Melo, M. (2023). Distribution of Dental Fluorosis in the Southern Zone of Ecuador: An Epidemiological Study. Dentistry Journal, 11(3), 71. https://doi.org/10.3390/dj11030071