

Oligodontia in the Clinical Spectrum of Syndromes: A Systematic Review

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Collection Process and Data Items
2.5. Risk of Bias within Studies
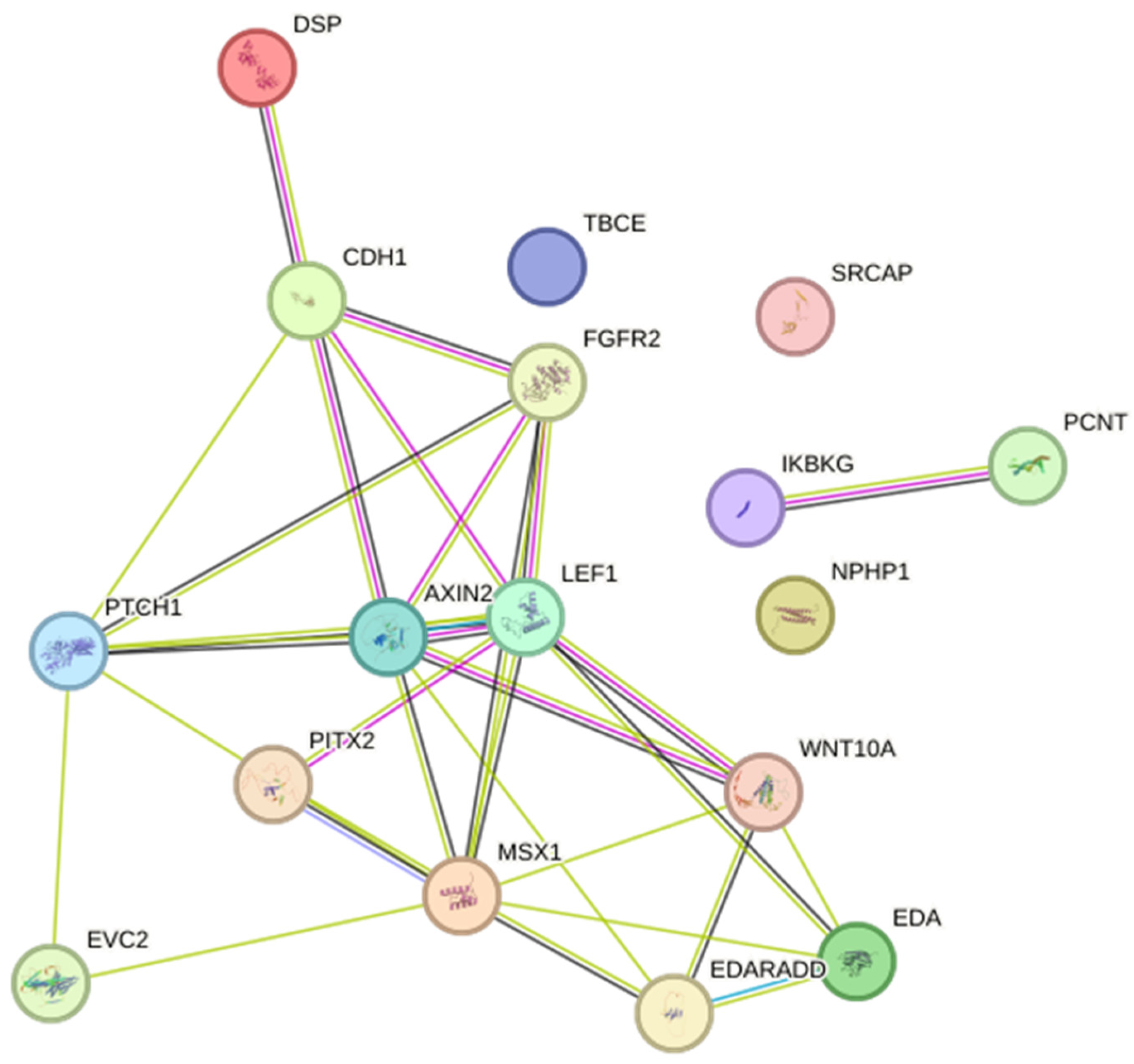
2.6. Interaction Analysis
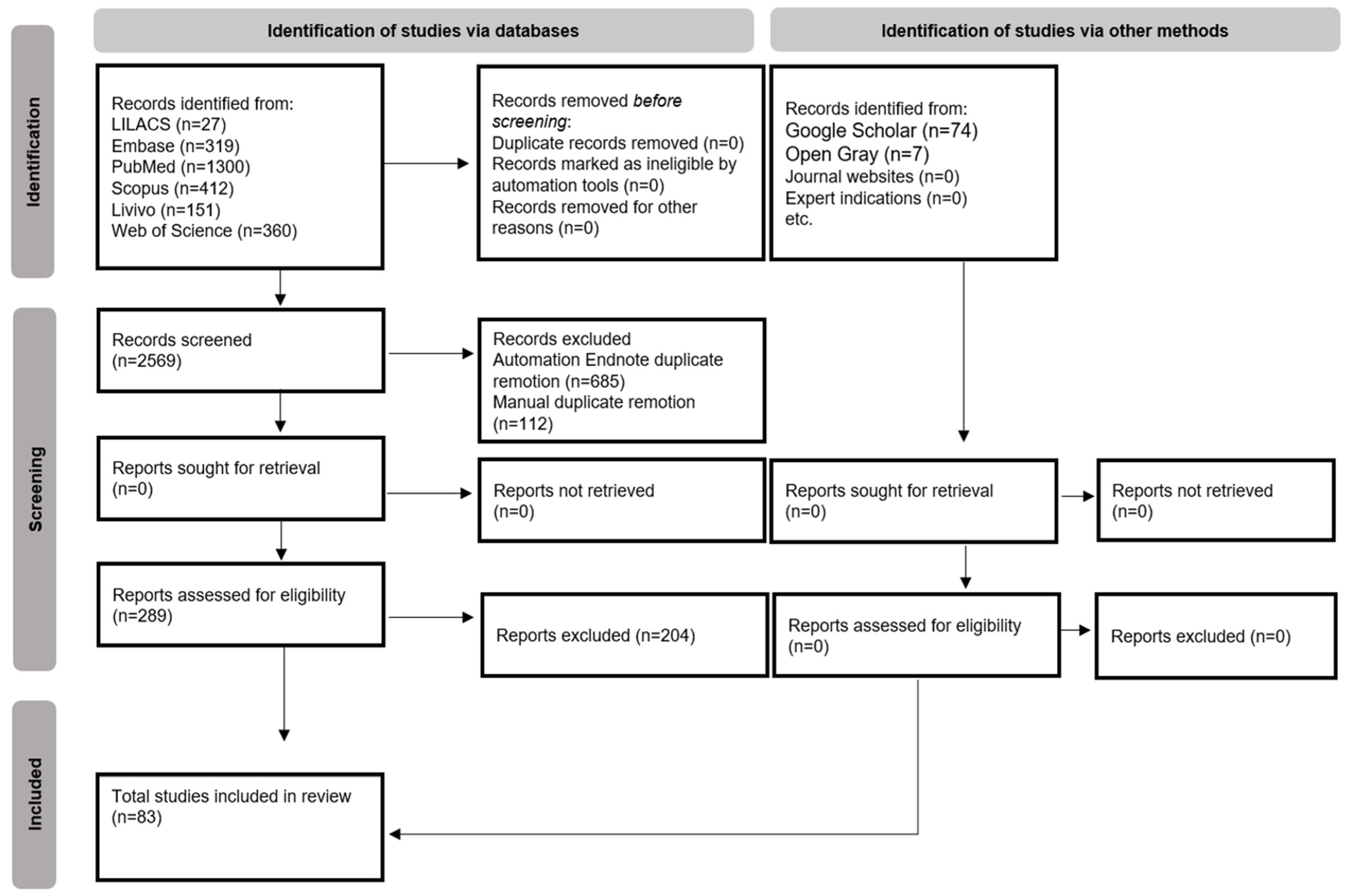
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de La Dure-Molla, M.; Fournier, B.P.; Manzanares, M.C.; Acevedo, A.C.; Hennekam, R.C.; Friedlander, L.; Boy-Lefèvre, M.L.; Kerner, S.; Toupenay, S.; Garrec, P.; et al. Elements of morphology: Standard terminology for the teeth and classifying genetic dental disorders. Am. J. Med. Genet. Part A 2019, 179, 1913–1981. [Google Scholar] [CrossRef] [PubMed]
- Weide, Y.S.; Beemer, F.A.; Faber, J.A.; Bosman, F. Symptomatology of patients with oligodontia. J. Oral Rehabil. 1994, 21, 247–261. [Google Scholar] [CrossRef] [PubMed]
- Zu, X.; Shen, Y.; Zheng, J. [Progress in genetic research on tooth agenesis associated with Wnt/beta-catenin signaling pathway]. Zhonghua Yi Xue Yi Chuan Xue Za Zhi 2021, 38, 506–509. [Google Scholar]
- Al-Ani, A.H.; Antoun, J.S.; Thomson, W.M.; Merriman, T.R.; Farella, M. Hypodontia: An Update on Its Etiology, Classification, and Clinical Management. BioMed Res. Int. 2017, 2017, 9378325. [Google Scholar] [CrossRef]
- Brook, H. Multilevel complex interactions between genetic, epigenetic and environmental factors in the aetiology of anomalies of dental development. Arch. Oral Biol. 2009, 54, S3–S17. [Google Scholar] [CrossRef]
- Nieminen, P.; Arte, S.; Pirinen, S.; Peltonen, L.; Thesleff, I. Gene defect in hypodontia: Exclusion of MSX1 and MSX2 as candidate genes. Hum. Genet. 1995, 96, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Gorlin, R.J. Syndromes of Head and Neck, 2nd ed.; Oxford University Press: Oxford, MS, USA, 2001. [Google Scholar]
- Vieira, A.R. Oral clefts and syndromic forms of tooth agenesis as model for genetics of isolated tooth agenesis. J. Dent. Res. 2003, 82, 162–165. [Google Scholar] [CrossRef]
- Baba, R.; Sato, A.; Arai, K. Consecutive tooth agenesis patterns in non-syndromic oligodontia. Odontology 2022, 110, 183–192. [Google Scholar] [CrossRef]
- Ritwik, P.; Partsson, K.K. Diagnosis of Tooth Agenesis in Childhood and Risk for Neoplasms in Adulthood. Ochsner J. 2018, 18, 345–350. [Google Scholar] [CrossRef]
- Rolling, S.; Poulsen, S. Oligodontia in Danish schoolchildren. Acta Odontol. Scand. 2001, 59, 111–112. [Google Scholar] [CrossRef]
- Nieminen, P. Genetic basis of tooth agenesis. J. Exp. Zool. Part B Mol. Dev. Evol. 2009, 312, 320–342. [Google Scholar] [CrossRef] [PubMed]
- Laganà, G.; Venza, N.; Borzabadi-Farahani, A.; Fabi, F.; Danesi, C.; Cozza, P. Dental anomalies: Prevalence and associations between them in a large sample of non-orthodontic subjects, a cross-sectional study. BMC Oral Health 2017, 17, 62. [Google Scholar] [CrossRef] [PubMed]
- Klein, O.D.; Oberoi, S.; Huysseune, A.; Hovorakova, M.; Peterka, M.; Peterkova, R. Developmental disorders of the dentition: An update. Am. J. Med. Genet. Part C Semin. Med. Genet. 2013, 163, 318–332. [Google Scholar] [CrossRef]
- Adaimy, L.; Chouery, E.; Mégarbané, H.; Mroueh, S.; Delague, V.; Nicolas, E.; Belguith, H.; de Mazancourt, P.; Mégarbané, A. Mutation in WNT10A Is Associated with an Autosomal Recessive Ectodermal Dysplasia: The odonto-onycho-dermal dysplasia. Am. J. Hum. Genet. 2007, 81, 821–828. [Google Scholar] [CrossRef] [PubMed]
- De Coster, P.J.; Marks, L.A.; Martens, L.C.; Huysseune, A. Dental agenesis: Genetic and clinical perspectives. J. Oral Pathol. Med. 2009, 38, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Zhang, H.; Camhi, H.; Seymen, F.; Koruyucu, M.; Kasimoglu, Y.; Kim, J.W.; Kim-Berman, H.; Yuson, N.M.; Benke, P.J.; et al. Analyses of oligodontia phenotypes and genetic etiologies. Int. J. Oral Sci. 2021, 13, 32. [Google Scholar] [CrossRef] [PubMed]
- Nordgarden, H.; Jensen, J.; Storhaug, K. Oligodontia is associated with extra-oral ectodermal symptoms and low whole salivary flow rates. Oral Dis. 2001, 7, 226–232. [Google Scholar] [CrossRef]
- Dhamo, B.; Kuijpers, M.A.R.; Balk-Leurs, I.; Boxum, C.; Wolvius, E.B.; Ongkosuwito, E.M. Disturbances of dental development distinguish patients with oligodontia-ectodermal dysplasia from isolated oligodontia. Orthod. Craniofacial Res. 2018, 21, 48–56. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; Joanna Briggs Institute: Adelaide, Australia, 2017; Chapter 7. [Google Scholar]
- Abdulla, A.M.; Almaliki, A.Y.; Shakeela, N.V.; Alkahtani, Z.; Alqahtani, M.A.; Sainudeen, S.; Shamsuddin, S.V. Prosthodontic Management of a Pediatric Patient with Christ-Siemens-Touraine Syndrome: A Case Report. Int. J. Clin. Pediatr. Dent. 2019, 12, 569–572. [Google Scholar]
- Abs, R.; Raes, D.; Vercruysse, H. Association of isolated hypogonadotropic hypogonadism, pronounced hypodontia and the Wolff-Parkinson-White syndrome. J. Int. Med. 1994, 236, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Aditya, A.; Lele, S.; Aditya, P. Fahr’s disease with oral manifestations: Report of a rare case. Med. Princ. Pract. 2012, 21, 395–397. [Google Scholar] [CrossRef]
- Agarwal, S.S.; Nehra, K.; Jayan, B.; Singh, N.; Thapa, A. Multidisciplinary management of oligodontia polycystic ovarian syndrome: A rare case report. Int. J. Oral Health Sci. Adv. 2014, 2, 33–41. [Google Scholar]
- Aminabadi, N.A.; Ebrahimi, A.; Oskouei, S.G. Chondroectodermal dysplasia (Ellis-van Creveld syndrome): A case report. J. Oral Sci. 2010, 52, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Ann Drum, M.; Kaiser-Kupfer, M.I.; Guckes, A.D.; Roberts, M.W. Oral manifestations of the Rieger syndrome: Report of case. J. Am. Dent. Assoc. (1939) 1985, 110, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Ardila, C.M.; Álvarez-Martínez, E. Dental and Maxillofacial Manifestations of Axenfeld-Rieger Syndrome: Presentation of a Case in a 5-Year-Old Girl. Case Rep. Dent. 2022, 2022, 4348264. [Google Scholar] [CrossRef]
- Arora, V.; Agrawal, K.K.; Mishra, A.; Chandra, A. Witkop’s syndrome: A case report. J. Oral Biol. Craniofacial Res. 2016, 6, 79–81. [Google Scholar] [CrossRef]
- Awadh, W.; Kiukkonen, A.; Nieminen, P.; Arte, S.; Hurmerinta, K.; Rice, D.P. Blepharocheilodontic (BCD) syndrome: New insights on craniofacial and dental features. Am. J. Med. Genet. A 2017, 173, 905–913. [Google Scholar] [CrossRef]
- Barber, S.; Day, P.; Judge, M.; Toole, E.O.; Fayle, S. Variant Carvajal syndrome with additional dental anomalies. Int. J. Paediatr. Dent. 2012, 22, 390–396. [Google Scholar] [CrossRef]
- Bekiesinska-Figatowska, M.; Mierzewska, H.; Kuczynska-Zardzewialy, A.; Szczepanik, E.; Obersztyn, E. Hypomyelination, hypogonadotropic hypogonadism, hypodontia—First Polish patient. Brain Dev. 2010, 32, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Bergendal, B.; Bjerklin, K.; Bergendal, T.; Koch, G. Dental Implant Therapy for a Child with X-linked Hypohidrotic Ectodermal Dysplasia—Three Decades of Managed Care. Int. J. Prosthodont. 2015, 28, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Bergendal, B. Prosthetic habilitation of a young patient with hypohidrotic ectodermal dysplasia and oligodontia: A case report of 20 years of treatment. Int. J. Prosthodont. 2001, 14, 471–479. [Google Scholar]
- Bildik, T.; Ozbaran, B.; Kose, S.; Koturoglu, G.; Gokce, B.; Gunaydin, A.; Altintas, I. Hypohidrotic ectodermal dysplasia: A multidisciplinary approach. Int. J. Psychiatry Med. 2012, 44, 225–240. [Google Scholar] [CrossRef] [PubMed]
- Blankenstein, R.; Brook, A.H.; Smith, R.N.; Patrick, D.; Russell, J.M. Oral findings in Carpenter syndrome. Int. J. Paediatr. Dent. 2001, 11, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Cagetti, M.G.; Camoni, N.; Cetraro, F.; Scanferla, M.; Moretti, G.M. Special-needs patients in pediatric dentistry: Progeroid syndrome. A case of dental management and oral rehabilitation. Pediatr. Rep. 2019, 11, 7951. [Google Scholar] [CrossRef]
- Callanan, A.P.; Anand, P.; Sheehy, E.C. Sotos syndrome with hypodontia. Int. J. Paediatr. Dent. 2006, 16, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, V.M.; Romero, J.S.S.; Paiva Correa de Melo, F.; Fonseca Faro, T.; Nunes Santos, A.C.; Carvalho, S.; Veras Sobral, A.P. Hypohidrotic and hidrotic ectodermal dysplasia: A report of two cases. Dermatol. Online J. 2013, 19, 18985. [Google Scholar]
- Chalabreysse, L.; Senni, F.; Bruyère, P.; Aime, B.; Ollagnier, C.; Bozio, A.; Bouvagnet, P. A new hypo/oligodontia syndrome: Carvajal/Naxos syndrome secondary to desmoplakin-dominant mutations. J. Dent. Res. 2011, 90, 58–64. [Google Scholar] [CrossRef]
- Cho, S.Y.; Lee, C.K.; Drummond, B.K. Surviving male with incontinentia pigmenti: A case report. Int. J. Paediatr. Dent. 2004, 14, 69–72. [Google Scholar] [CrossRef]
- Clauss, F.; Waltmann, E.; Barriere, P.; Hadj-Rabia, S.; Manière, M.C.; Schmittbuhl, M. Dento-maxillo-facial phenotype and implants-based oral rehabilitation in Ectodermal Dysplasia with WNT10A gene mutation: Report of a case and literature review. J. Cranio-Maxillofac. Surg. 2014, 42, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Cogulu, D.; Ertugrul, F. Dental management of a patient with oculo-facio-cardio-dental syndrome. J. Dent. Child. 2008, 75, 306–308. [Google Scholar]
- Cogulu, D.; Oncag, O.; Celen, E.; Ozkinay, F. Kabuki Syndrome with additional dental findings: A case report. J. Dent. Child. 2008, 75, 185–187. [Google Scholar]
- Costa, F.; Sarno, M.; Khouri, R. Emergence of Congenital Zika Syndrome: Viewpoint from the Front Lines. Ann. Intern. Med. 2016, 164, 689–691. [Google Scholar] [CrossRef]
- Dall’Oca, S.; Ceppi, E.; Pompa, G.; Polimeni, A. X-linked hypohidrotic ectodermal dysplasia: A ten-year case report and clinical considerations. Eur. J. Paediatr. Dent. 2008, 9, 14–18. [Google Scholar] [PubMed]
- Devadas, S.; Varma, B.; Mungara, J.; Joseph, T.; Saraswathi, T.R. Witkop tooth and nail syndrome: A case report. Int. J. Paediatr. Dent. 2005, 15, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Downing, A.; Welbury, R.R. The tricho-rhino-phalangeal syndrome—A case report. Int. J. Paediatr Dent. 1992, 2, 35–40. [Google Scholar] [CrossRef]
- Dunbar, A.C.; McIntyre, G.T.; Laverick, S.; Stevenson, B. Axenfeld-Rieger syndrome: A case report. J. Orthod. 2015, 42, 324–330. [Google Scholar] [CrossRef]
- Emral, M.E.; Akcam, M.O. Noonan syndrome: A case report. J. Oral Sci. 2009, 51, 301–306. [Google Scholar] [CrossRef][Green Version]
- Fan, Z.; Sun, S.; Liu, H.; Yu, M.; Liu, Z.; Wong, S.W.; Liu, Y.; Han, D.; Feng, H. Novel PITX2 mutations identified in Axenfeld-Rieger syndrome and the pattern of PITX2-related tooth agenesis. Oral Dis. 2019, 25, 2010–2019. [Google Scholar] [CrossRef]
- Ghosh, S.; Garg, M.; Gupta, S.; Choudhary, M.; Chandra, M. Microcephalic osteodyplastic primordial dwarfism type II: Case report with unique oral findings and a new mutation in the pericentrin gene. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 129, e204–e211. [Google Scholar] [CrossRef]
- Gupta, S.R. Isolated aglossia congenita: A rare case of oromandibular limb hypogenesis syndrome type IB. J. Oral Maxillofac. Pathol. 2012, 16, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.; Govind, M.; Sawai, M.A.; Ansari, M.D. Hypohidrotic ectodermal dysplasia with autosomal recessive inheritance pattern: Report of a rare and unusual case with a brief review of literature. J. Oral Maxillofac. Pathol. 2019, 23, 479. [Google Scholar] [PubMed]
- Hassona, Y.; Rajab, L.; Taimeh, D.; Scully, C. Sanjad-Sakati Syndrome: Oral Health Care. Med. Princ. Pract. 2018, 27, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Hattab, F.N.; Angmar-Månsson, B. Oligodontia of the permanent dentition in two sisters with polycystic ovarian syndrome: Case reports. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 84, 368–371. [Google Scholar] [CrossRef]
- Hattab, F.N.; al-Khateeb, T.; Mansour, M. Oral manifestations of severe short-limb dwarfism resembling Grebe chondrodysplasia: Report of a case. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 81, 550–555. [Google Scholar] [CrossRef]
- Hingston, E.J.; Hunter, M.L.; Hunter, B.; Drage, N. Hurler’s syndrome: Dental findings in a case treated with bone marrow transplantation in infancy. Int. J. Paediatr. Dent. 2006, 16, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Jain, D.; Jain, S.; Kumar, A.; Rahangdale, T. Hypohidrotic Ectodermal Dysplasia: Prosthetic and Endodontic Management. Int. J. Clin. Pediatr. Dent. 2010, 3, 63–67. [Google Scholar] [CrossRef]
- Jain, N.; Naitam, D.; Wadka, A.; Nemane, A.; Katoch, S.; Dewangan, A. Prosthodontic rehabilitation of hereditary ectodermal dysplasia in an 11-year-old patient with flexible denture: A case report. Case Rep. Dent. 2012, 2012, 489769. [Google Scholar] [CrossRef]
- Kale, L.; Khambete, N.; Sodhi, S.; Kumar, R. Achondroplasia with oligodontia: Report of a rare case. J. Oral Maxillofac. Pathol. 2013, 17, 451–454. [Google Scholar]
- Kantaputra, P.; Kaewgahya, M.; Jotikasthira, D.; Kantaputra, W. Tricho-odonto-onycho-dermal dysplasia and WNT10A mutations. Am. J. Med. Genet. Part A 2014, 164, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Kaul, S.; Reddy, R. Prosthetic rehabilitation of an adolescent with hypohidrotic ectodermal dysplasia with partial anodontia: Case report. J. Indian Soc. Pedod. Prev. Dent. 2008, 26, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, T.; Motohashi, N.; Ohyama, K. A case of oculo-facio-cardio-dental syndrome with integrated orthodontic-prosthodontic treatment. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 2004, 41, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Khabour, O.F.; Mesmar, F.S.; Al-Tamimi, F.; Al-Batayneh, O.B.; Owais, A.I. Missense mutation of the EDA gene in a Jordanian family with X-linked hypohidrotic ectodermal dysplasia: Phenotypic appearance and speech problems. Genet. Mol. Res. 2010, 9, 941–948. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Khurana, V.K.; Gupta, R.K.; Kumar, L.P. Witkop syndrome: A case report of an affected family. Dermatol. Online J. 2012, 18, 2. [Google Scholar] [CrossRef] [PubMed]
- Kinyó, A.; Vályi, P.; Farkas, K.; Nagy, N.; Gergely, B.; Tripolszki, K.; Torok, D.; Bata-Csorgo, Z.; Kemény, L.; Szell, M. A newly identified missense mutation of the EDA1 gene in a Hungarian patient with Christ-Siemens-Touraine syndrome. Arch. Dermatol. Res. 2014, 306, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Kishore, M.; Panat, S.R.; Aggarwal, A.; Agarwal, N.; Upadhyay, N.; Ajai, K.; Alok, A. Hypohidrotic Ectodermal Dysplasia (ED): A Case Series. J. Clin. Diagn. Res. 2014, 8, 273–275. [Google Scholar]
- Kobayashi, T.; Iida, A.; Narimatsu, N.; Shimomura, Y. A case of multiple oral cancers in the patient with hypohidrotic ectodermal dysplasia. J. Oral Maxillofac. Surg. Med. Pathol. 2022, 34, 759–763. [Google Scholar] [CrossRef]
- Kozma, C.; Chong, S.S.; Meck, J.M. Interstitial deletion of 4p15.32p16.3 in a boy with minor anomalies, hearing loss, borderline intelligence, and oligodontia. Am. J. Med. Genet. 1999, 86, 316–320. [Google Scholar] [CrossRef]
- Kramer, F.J.; Baethge, C.; Tschernitschek, H. Implants in children with ectodermal dysplasia: A case report and literature review. Clin. Oral Implant. Res. 2007, 18, 140–146. [Google Scholar] [CrossRef]
- Krøigård, A.B.; Thomassen, M.; Lænkholm, A.V.; Kruse, T.A.; Larsen, M.J. Evaluation of Nine Somatic Variant Callers for Detection of Somatic Mutations in Exome and Targeted Deep Sequencing Data. PLoS ONE 2016, 11, e0151664. [Google Scholar] [CrossRef] [PubMed]
- Lévy, J.; Capri, Y.; Rachid, M.; Dupont, C.; Vermeesch, J.R.; Devriendt, K.; Verloes, A.; Tabet, A.C.; Bailleul-Forestier, I. LEF1 haploinsufficiency causes ectodermal dysplasia. Clin. Genet. 2020, 97, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Liedén, A.; Kvarnung, M.; Nilssson, D.; Sahlin, E.; Lundberg, E.S. Intragenic duplication—A novel causative mechanism for SATB2-associated syndrome. Am. J. Med. Genet. Part A 2014, 164, 3083–3087. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.; Liu, Y.; Su, L.; Liu, H.; Feng, H.; Yu, M.; Liu, H. A Novel CDH1 Variant Identified in a Chinese Family with Blepharocheilodontic Syndrome. Diagnostics 2022, 12, 2936. [Google Scholar] [CrossRef] [PubMed]
- Martinho, J.; Ferreira, H.; Paulo, S.; Paula, A.; Marto, C.M.; Carrilho, E.; Marques-Ferreira, M. Oculo-Facio-Cardio-Dental Syndrome: A Case Report about a Rare Pathological Condition. Int. J. Environ. Res. Public Health 2019, 16, 928. [Google Scholar] [CrossRef] [PubMed]
- Marvin, M.L.; Mazzoni, S.M.; Herron, C.M.; Edwards, S.; Gruber, S.B.; Petty, E.M. AXIN2-associated autosomal dominant ectodermal dysplasia and neoplastic syndrome. Am. J. Med. Genet. Part A 2011, 155, 898–902. [Google Scholar] [CrossRef]
- Murata, Y.; Kurosaka, H.; Ohata, Y.; Aikawa, T.; Takahata, S.; Fujii, K.; Miyashita, T.; Morita, C.; Inubushi, T.; Kubota, T.; et al. A novel PTCH1 mutation in basal cell nevus syndrome with rare craniofacial features. Hum. Genome Var. 2019, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, E.M.; Jones, D.C. Dental anomalies in Axenfeld-Rieger syndrome. Int. J. Paediatr. Dent. 2005, 15, 459–463. [Google Scholar] [CrossRef]
- Pipa, A.V.; López, E.M.A.; González, M.G.; Martínez, M.F.; Blanco, F.M.A.B. Treatment with removable prosthesis in hypohidrotic ectodermal dysplasia: A clinical case. Med. Oral Patol. Oral Cir. Bucal 2008, 13, E119–E123. [Google Scholar]
- Reiche, W.; Parkanyi, L.; Braunitzer, G.; Nagy, K.; Karpati, K. Oligodontia in a teenager with Down syndrome—A case study. Klin. Padiatr. 2015, 227, 35–37. [Google Scholar] [CrossRef]
- Retna, R.N.; Sockalingam, S. Clinical manifestation of blepharocheilodontic (BCD) syndrome: A case review. Sains Malays. 2016, 42, 85–88. [Google Scholar]
- Richieri-Costa, A.; Pirolo Júnior, L.; Cohen, M.M., Jr. Carpenter syndrome with normal intelligence: Brazilian girl born to consanguineous parents. Am. J. Med. Genet. 1993, 47, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Rizos, M.; Negrón, R.J.; Serman, N. Möbius syndrome with dental involvement: A case report and literature review. Cleft Palate-Craniofacial J. Off. Publ. Am. Cleft Palate-Craniofacial Assoc. 1998, 35, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Rock, W.P.; McLellan, N.J. Severe hypodontia in association with Klinefelter (47 XXY) syndrome: A case report. Br. J. Orthod. 1990, 17, 321–323. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.; Han, D.; Zhang, J.; Zhao, H.; Feng, H. Two novel heterozygous mutations of EVC2 cause a mild phenotype of Ellis-van Creveld syndrome in a Chinese family. Am. J. Med. Genet. Part A 2011, 155, 2131–2136. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, H.P.; Sennimalai, K.; Samrit, V.D.; Duggal, R.; Yadav, R. Adjunctive orthodontic therapy for prosthetic rehabilitation in a growing child with Axenfeld-Rieger syndrome: A case report. Spec. Care Dent. 2021, 41, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Sikora, P.; Majewski, M.; Kandzierski, G.; Zajączkowska, M.; Borzęcka, H.; Korolczuk, A.; Kozlowski, K. Juvenile nephronophtisis, short stature, partial adontia and skeletal abnormalities—A new syndromic association. Nephrol. Dial. Transplant. 2006, 21, 2335–2336. [Google Scholar] [CrossRef][Green Version]
- Singh, A.; Bhatia, H.P.; Sood, S.; Sharma, N.; Mohan, A. A novel finding of oligodontia and ankyloglossia in a 14-year-old with Floating-Harbor syndrome. Spec. Care Dent. Off. Publ. Am. Assoc. Hosp. Dent. Acad. Dent. Handicap. Am. Soc. Geriatr. Dent. 2017, 37, 318–321. [Google Scholar] [CrossRef]
- Subramaniam, P.; Neeraja, G. Witkop’s tooth and nail syndrome: A multifaceted approach to dental management. J. Indian Soc. Pedod. Prev. Dent. 2008, 26, 22–25. [Google Scholar]
- Suda, N.; Bazar, A.; Jigjid, B.; Garidkhuu, A.; Ganburged, G.; Moriyama, K. A Mongolian patient with hypohidrotic ectodermal dysplasia with a novel P121S variant in EDARADD. Orthod. Craniofacial Res. 2010, 13, 114–117. [Google Scholar] [CrossRef]
- Sultan, A.; Juneja, A.; Bhaskar, S. Co-morbidity of down syndrome with autism spectrum disorder: Dental implications. J. Oral Biol. Craniofacial Res. 2020, 10, 146–148. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Li, F.; Liu, Y.; Qu, H.; Wong, S.W.; Zeng, L.; Yu, M.; Feng, H.; Liu, H.; Han, D. A novel inhibitor of nuclear factor kappa-B kinase subunit gamma mutation identified in an incontinentia pigmenti patient with syndromic tooth agenesis. Arch. Oral Biol. 2019, 101, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Talasila, J.; Pachigolla, R.; Yarlagadda, K.V.S.N.; Vuppala, R.; Grzeschik, K.H.; Kiran, S.; Rose, C.M.; Gottesman, G.S.; Urban, Z. Acromelia-oligodontia syndrome. Clin. Case Rep. 2017, 5, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Tanboga, I.; Kargul, B.; Ergeneli, S.; Aydin, M.Y.; Atasu, M. Clinical features of incontinentia pigmenti with emphasis on dermatoglyphic findings. J. Clin. Pediatr. Dent. 2001, 25, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Tanboga, I.; Pinçe, S.; Düzdar, L. Dental management of a child with EEC syndrome. Int. J. Paediatr. Dent. 1992, 2, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.C.; Slavatinek, A.M.; Vargervik, K.; Oberoi, S. Hypodontia in Beare-Stevenson syndrome: An example of dental anomalies in FGFR-related craniosynostosis syndromes. Cleft Palate-Craniofacial J. 2010, 47, 253–258. [Google Scholar] [CrossRef]
- Tosun, G.; Sener, Y. Apert syndrome with glucose-6-phosphate dehydrogenase deficiency: A case report. Int. J. Paediatr. Dent. 2006, 16, 218–221. [Google Scholar] [CrossRef]
- Tuna, E.B.; Sulun, T.; Rosti, O.; El Abdallah, F.; Kayserili, H.; Aktoren, O. Craniodentofacial manifestations in Hallermann-Streiff syndrome. Cranio J. Craniomandib. Pract. 2009, 27, 33–38. [Google Scholar]
- Tuna, E.B.; Marşan, G.; Gençay, K.; Seymen, F. Craniofacial and dental characteristics of Kabuki syndrome: Nine years cephalometric follow-up. J. Clin. Pediatr. Dent. 2012, 36, 393–400. [Google Scholar] [CrossRef]
- Vasudevan, B.; Sinha, A. A Rare Case of Odonto-Onycho-Dermal-Dysplasia with WNT10a Mutation. Indian J. Dermatol. 2023, 68, 355. [Google Scholar]
- Waldron, J.M.; McNamara, C.; Hewson, A.R.; McNamara, C.M. Axenfeld-Rieger syndrome (ARS): A review and case report. Spec. Care Dent. Off. Publ. Am. Assoc. Hosp. Dent. Acad. Dent. Handicap. Am. Soc. Geriatr. Dent. 2010, 30, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Ye, X.; Bian, Z. The second deletion mutation in exon 8 of EDA gene in an XLHED pedigree. Dermatology 2013, 226, 105–110. [Google Scholar] [CrossRef]
- Zidane, F.E.; El Alloussi, M. Oligodontia and Facial Phenotype Associated with a Rare Syndrome. Case Rep. Dent. 2022, 2022, 1045327. [Google Scholar] [CrossRef] [PubMed]
- Galluccio, G.; Castellano, M.; La Monaca, C. Genetic basis of non-syndromic anomalies of human tooth number. Arch. Oral Biol. 2012, 57, 918–930. [Google Scholar] [CrossRef] [PubMed]
- Ogaard, B.; Krogstad, O. Craniofacial structure and soft tissue profile in patients with severe hypodontia. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Zeng, B.; Lu, H.; Xiao, X.; Zhou, L.; Lu, J.; Zhu, L.; Yu, D.; Zhao, W. Novel EDA mutation in X-linked hypohidrotic ectodermal dysplasia and genotype-phenotype correlation. Oral Dis. 2015, 21, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Moura, E.; Rotenberg, I.S.; Pimpão, C.T. X-Linked Hypohidrotic Ectodermal Dysplasia-General Features and Dental Abnormalities in Affected Dogs Compared With Human Dental Abnormalities. Top. Companion Anim. Med. 2019, 35, 11–17. [Google Scholar] [CrossRef]
- Reyes-Reali, J.; Mendoza-Ramos, M.I.; Garrido-Guerrero, E.; Méndez-Catalá, C.F.; Méndez-Cruz, A.R.; Pozo-Molina, G. Hypohidrotic ectodermal dysplasia: Clinical and molecular review. Int. J. Dermatol. 2018, 57, 965–972. [Google Scholar] [CrossRef]
- Aubert-Mucca, M.; Huber, C.; Baujat, G.; Michot, C.; Zarhrate, M.; Bras, M.; Boutaud, L.; Malan, V.; Attie-Bitach, T.; Cormier-Daire, V. Ellis-Van Creveld Syndrome: Clinical and Molecular Analysis of 50 Individuals. J. Med. Genet. 2023, 60, 337–345. [Google Scholar] [CrossRef]
- Hu, Q.; Mai, J.; Xiang, Q.; Zhou, B.; Liu, S.; Wang, J. A novel deletion mutation in the BCOR gene is associated with oculo-facio-cardio-dental syndrome: A case report. BMC Pediatr. 2022, 22, 82. [Google Scholar] [CrossRef]
- McMillan, K.B.; McMillan, D.C.; Arce, K.; Salinas, T. Surgical and prosthetic rehabilitation of siblings with Witkop tooth and nail syndrome using zygomatic implants: A familial case series of 3 patients with up to 15-year follow-up. Oral Maxillofac. Surg. 2023, 27, 711–719. [Google Scholar] [CrossRef]
- Reis, L.M.; Maheshwari, M.; Capasso, J.; Atilla, H.; Dudakova, L.; Thompson, S.; Zitano, L.; Lay-Son, G.; Lowry, R.B.; Black, J.; et al. Axenfeld-Rieger syndrome: More than meets the eye. J. Med. Genet. 2023, 60, 368–379. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, S.; Naveen, D.; Haan, E.; Barnett, C. CDH1-related blepharocheilodontic syndrome is associated with diffuse gastric cancer risk. Am. J. Med. Genet. A 2020, 182, 1780–1784. [Google Scholar] [CrossRef] [PubMed]
- Arzoo, P.S.; Klar, J.; Bergendal, B.; Norderyd, J.; Dahl, N. WNT10A mutations account for (1/4) of population-based isolated oligodontia and show phenotypic correlations. Am. J. Med. Genet. A 2014, 164, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Tuzoff, D.V.; Tuzova, L.N.; Bornstein, M.M.; Krasnov, A.S.; Kharchenko, M.A.; Nikolenko, S.I.; Sveshnikov, M.M.; Bednenko, G.B. Tooth detection and numbering in panoramic radiographs using convolutional neural networks. Dentomaxillofacial Radiol. 2019, 48, 20180051. [Google Scholar] [CrossRef] [PubMed]
- Román, J.C.M.; Fretes, V.R.; Adorno, C.G.; Silva, R.G.; Noguera, J.L.V.; Legal-Ayala, H.; Mello-Román, J.D.; Torres, R.D.E.; Facon, J. Panoramic Dental Radiography Image Enhancement Using Multiscale Mathematical Morphology. Sensors 2021, 21, 3110. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.C.; Line, S.R. The genetics of amelogenesis imperfecta: A review of the literature. J. Appl. Oral Sci. 2005, 13, 212–217. [Google Scholar] [CrossRef]
- Vastardis, H. The genetics of human tooth agenesis: New discoveries for understanding dental anomalies. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 650–655. [Google Scholar] [CrossRef]
- Zeng, B.; Zhao, Q.; Li, S.; Lu, H.; Lu, J.; Ma, L.; Zhao, W.; Yu, D. Novel EDA or EDAR Mutations Identified in Patients with X-Linked Hypohidrotic Ectodermal Dysplasia or Non-Syndromic Tooth Agenesis. Genes 2017, 8, 259. [Google Scholar] [CrossRef]
- Andreoni, F.; Sgattoni, C.; Bencardino, D.; Simonetti, O.; Forabosco, A.; Magnani, M. Missense mutations in EDA and EDAR genes cause dominant syndromic tooth agenesis. Mol. Genet. Genom. Med. 2020, 9, 1555. [Google Scholar] [CrossRef]
- Mues, G.; Tardivel, A.; Willen, L.; Kapadia, H.; Seaman, R.; Frazier-Bowers, S.; Schneider, P.; D’souza, R.N. Functional analysis of ectodysplasin—A mutations causing selective tooth agenesis. Eur. J. Hum. Genet. 2010, 18, 19–25. [Google Scholar] [CrossRef]
- Peck, J.; Douglas, G.; Wu, C.H.; Burbelo, P.D. Human RhoGAP domain-containing proteins: Structure, function and evolutionary relationships. FEBS Lett. 2002, 528, 27–34. [Google Scholar] [CrossRef]
- Schalk-van der Weide, Y.; Steen, W.H.; Bosman, F. Distribution of missing teeth and tooth morphology in patients with oligodontia. ASDC J. Dent. Child. 1992, 59, 133–140. [Google Scholar]
- Schalk-van der Weide, Y.; Prahl-Andersen, B.; Bosman, F. Tooth formation in patients with oligodontia. Angle Orthod. 1993, 63, 31–37. [Google Scholar]
- Polder, B.J.; Van’t Hof, M.A.; Van der Linden, F.P.; Kuijpers-Jagtman, A.M. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent. Oral Epidemiol. 2004, 32, 217–226. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author Year/Country | Geographic Origin | Type of Study (CR/SC) | Syndrome Name (#OMIM) | Sex (M/F) | Age (Yrs) | Mode of Inheritance (AD/AR/X-LINKED) | Causative Gene | Dentition | Number of Teeth | Affected Teeth | Systemic Manifestations | Craniofacial Manifestations |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abdulla et al., 2019 [23]/Kingdom of Saudi Arabia | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 7 | NR | NR | Permanent | 14 | 12,14, 15, 22, 24, 25, 31, 32, 34, 35, 41, 42, 44, 45 | No production of tears, sweat pores were poorly visible | Hair over the scalp was sparsely distributed, scanty eyebrows and eyelashes, hyperpigmentation around the eyes, depressed nasal bridge, prominent supraorbital ridge, everted dry lips, delayed eruption of permanent dentition, bone ridge on the mandibular anterior region was very thin, cone-shaped crowns, conical maxillary anterior teeth, oligodontia |
| Abs et al., 1994 [24]/Belgium | NR | CR | Wolff–Parkinson–White syndrome (#194200) | F | 22 | NR | NR | Permanent | 11 | 14, 15, 17, 12, 22, 25, 27, 35, 37, 45, 47 | Discrete cubitus valgus, hygonadotropic hypogonadism, ovaries had a prepubertal aspect without stigmata of ovulation, negative T-waves in leads 111 and AVF, low level of luteinizing hormone (LH), gonadotropinreleasing hormone (GnRH), folliclestimulating hormone (FSH). | Microdontia, retention of deciduous teeth, oligodontia |
| Aditya et al., 2012 [25]//India | NR | CR | Fahr’s syndrome (#213600) | F | 23 | NR | NR | Permanent | 14 | 11, 14, 15, 17, 21, 35, 36, 37, 42, 43, 44, 45, 46, 47 | Short toes and fingers, seizure, short of stature, short digits, several hypopigmented to depigmented macules on the face, multiple slightly hyperpigmented plaques on the abdomen, right arm, left thigh and leg, and right calf, multiple small hard paules on the extremities, osteoporosis with cupping deformity at articular surfaces, thyroid stimulating hormone and parathyroid hormone levels very high, calcifications in the bilateral caudate nucleus, putamen, glubus pallidus, thalamus, basal ganglia, cerebral hemipheres and cortical white matter, severe mental retardation | Bilateral cataracts and oligodontia |
| Agarwal et al., 2014 [26]/India | NR | CR | Polycistic ovarian syndrome (#184700) | F | 21 | NR | NR | Permanent | 22 | 12, 13, 14, 15, 16, 17, 22, 23, 25, 27, 31, 32, 33, 34, 35, 37, 41, 42, 44, 45, 46, 47 | NR | Slight reduction in lower anterior facial height, straight profile, mildly protuberant lips, normal nasolabial angle, deep mentolabial sulcus and hyperactivity of the mentalis muscle, oligodontia |
| Aminabadi et al., 2010 [27]/Iran | NR | CR | Ellis–van Creveld syndrome (#225500) | F | 5 | NR | NR | Primar /Permanent | 6/9 | 52, 53, 63, 71, 73, 83/12, 31, 32, 33, 35, 41, 42, 43, 45 | Short stature, extremities were plump, shortness of the limbs, hands and feet were wide and markedly deformed with sausage-shaped fingers and dysplastic fingernails, bimanual hexadactyly on the ulnar side | Hair was fine and straight, fusion of the middle portion of the upper lip to the maxillary gingival mucosal margin with absence of the mucobuccal fold, multiple accessory labiogingival frenula, conical anterior teeth, oligodontia, multiple small alveolar notches on the crest of a thin alveolar ridge, serrated appearance of the gingiva, supernumerary tooth |
| Ann Drum et al., 1985 [28]//United States of America | NR | CR | Rieger syndrome (#602482) | F | NR | NR | NR | Permanent | 17 | 11, 12, 13, 14, 16, 21, 22, 23, 26, 31, 32, 33, 36, 41, 42, 45, 46 | Bilateral microcornea with nasally displaced oval-shaped pupils, peripheral iris adhesions to the cornea | Oligodontia, microdontia, hypoplastic enamel, hyperplastic tissue was present where the maxillary labial frenum |
| Ardila and Álvarez-Martínez, 2022 [29]/Colombia | Colombia | CR | Axenfeld–Rieger syndrome (#180500) | F | 5 | AD | NR | Permanent | 22 | 16, 15, 14, 13, 12, 21, 22, 25, 26, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46 | Pupillary dyscoria, corectopia, blepharitis, abnormalities in the iris, and posterior embryotoxon. In profile analysis, there is a greater predominance of the upper third of the face with respect to the middle and lower thirds. A slightly flattened infraorbital area, prominent cheekbones, straight nasolabial angle, superior rretrochelia, resting labial seal, inferior normochelia, and a slightly flattened mentolabial angle are observed. | Hyperplastic upper labial frenulum, enamel hypoplasia, hypodontia, oligodontia, microdontia, taurodontism, conical teeth, short roots, and delayed eruption |
| Arora et al., 2016 [30]/India | NR | CR | Witkop’s syndrome (#189500) | M | 23 | NR | NR | Permanent | 22 | 11, 12, 14, 15, 16, 17, 21, 23, 24, 25, 26, 27, 31, 32, 33, 34, 37, 41, 42, 43, 44, 47 | Marked longitudinal ridging of the nail plates of the fingers, onychorrhexis, toenails affected with koilonychia, thin nail plates | Oligodontia, root stumps, deciduous dentition was hypoplastic, conical teeth |
| Awadh et al., 2016 [31]/Finland | Finland | CR | Blepharocheilodontic syndrome (#119580) | 1: M 2: M 3: F 4: M | 7.8–8.2 | AD | NR | Primary/Permanent | 1. 13/17 2. 6/7 3. 8/14 4. 7/17 | 1. 51, 52, 53, 54, 55, 61, 62, 63, 64, 65, 73, 74, 84/11, 12, 13, 14, 21, 22, 23, 24, 25, 27, 33, 34, 35, 41, 43, 44, 45 2. 51, 52, 73, 74, 75, 84/11, 12, 13, 21, 22, 34, 44 3. 51, 52, 54, 61, 62, 64, 74, 84/11, 12, 13, 14, 15, 21, 22, 23, 24, 25, 33, 34, 43, 44 4. 54, 62, 63, 64, 71, 81, 84/11, 12, 14, 15, 21, 22, 23, 24, 25, 31, 32, 33, 35, 41, 42, 43, 44 | NR | Eyelash abnormalities, ectropion of the lower eyelids, bilateral cleft lip and palate, severe skeletal III malocclusion, oligodontia of primary and permanent teeth |
| Barber et al., 2012 [32]/United Kingdom | NR | CR | Carvajal syndrome (#605676) | F | 15 | NR | NR | Permanent | 9 | 15, 17, 24, 25, 27, 35, 37, 45, 47 | Hyperkeratotic skin on palms and soles, patchy dry, scaly skin, linear palmar and diffuse keratoderma with episodic plantar fissures, small white fingernails and thickened toenails. | Sparse eyebrows and eyelashes, premature root resorption with loss of primary teeth, microdontia incisors, recurrent angular cheilitis, granulomatous, furrowed, folded and cobblestone appearance of bilateral mucosa and fissured dorsum of tongue, episodes of generalized oral soreness twice a year, oligodontia |
| Bekiesinska-Figatowska et al., 2009 [33]/Poland | NR | CR | 4H syndrome (#612440) | F | 25 | NR | NR | Permanent | 8 | 12, 15, 22, 24, 34, 35, 44, 45 | Intellectual development was mildly delayed, hypogonadotropid hypogonadism, low level of LH and FSH | Cerebellum was atrophic, corpus callosum was thin, subarachnoid cyst in the middle cranial fossa, and oligodontia |
| Bergendal, 2001 [34]/Sweden | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | F | 6 | NR | NR | Permanent | 15 | 13, 14, 15, 24, 25, 31, 32, 33, 34, 35, 41, 42, 43, 44, 45 | Capacity to sweat is reduced | Fine sparse hair, dry and thin skin, frontal bossing, cherub-like lips, no body hair on arms and legs |
| Bergendal et al., 2015 [35]/Sweden | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 32 | X-linked | NR | Permanent | 24 | 11, 12, 14, 15, 17, 21, 22, 24, 25, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 | Decreased sweating capacity, hoarse voice | Light sparse hair, marked oral dryness, conical teeth, mandibular anodontia, and maxillary oligodontia |
| Bildik et al., 2012 [36]/Turkey | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 14 | NR | NR | Permanent | 26 | 12, 13, 14, 15, 16, 17, 22, 23, 24, 25, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 | Pervasive dryness on skin, excoriated papules, attention deficits, anxiety symptoms | Slimming on hairs, maxillary hypoplasia and sunken cheeks |
| Blankenstein et al., 2001 [37]/United Kingdom | NR | CR | Carpenter syndrome (#201000) | M | 14 | AR | NR | Permanent | 18 | 12, 14, 15, 17, 22, 24, 25, 27, 31, 32, 34, 35, 37, 41, 42, 44, 45, 47 | Clinodactyly and syndactyly of the fingers, preaxial polysyndactyly of the feet, hypospadias and undescended testicles, talipes equinovarus, ventriculoseptal defect, asthma | Acrocephaly, low-set ears with malformed pinnae, flattened nasal bridge, epicanthal folds, dystopia canthorum, short neck, class III malloclusion with no crowding, and oligodontia |
| Cagetti et al., 2019 [38]/Italy | NR | CR | Progeroid syndrome (#612289) | F | 8 | NR | NR | Permanent | 22 | 11, 12, 14, 15, 16, 17, 21, 22, 23, 24, 25, 26, 27, 33, 34, 36, 37, 43, 44, 45, 46, 47 | Brachycephaly, dural malformations and vascular developmental variations, hemangioma of the cephalic segment, scoliosis, skin xerosis, onychodystrophy with hypoplasia of the distal phalanx of the finger, hypertrichosis, skin laxity and wrinkles of the neck | Prominent eyebrows, misshapen teeth with radicular anomalies, condyles appeared dysmorphic and flattened, class III occlusion, and oligodontia |
| Callanan et al., 2006 [39]/United Kingdom | NR | CR | Sotos syndrome (#117550) | M | 10 | NR | NR | Permanent | 11 | 12, 14, 15, 22, 24, 25, 34, 35, 37, 44, 45 | Atrioventricular septal defect, asthma, learning disability, and behavioural problems | Macrocrania, frontal bossing, thin receding hairline, down-slanting palpebral fissures, large ears, a flat nasal bridge, pointed chin, epicanthal folds, class I malocclusion, and oligodontia |
| Carvalho et al., 2013 [40]/Brazil | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | 1: M 2:M | 1:29 2:14 | NR | NR | Permanent | 1.22 2. 13 | 1.13, 14, 15, 16, 17, 23, 24, 25, 26, 27, 31, 32, 34, 35, 36, 37, 41, 42, 44, 45, 46, 47 2.12, 15, 16, 22, 23, 31, 32, 34, 35, 41, 42, 44, 45 | Thin and dry skin, and palmoplantar hyperkeratosis | 1: Sparse hair, frontal bossing, hyperpigmentation in the periorbital region, low implantation of the ear, saddle nose, and oligodontia; 2: Low implantation of the ear, scanty eyebrows, and oligodontia. |
| Chalabreysse et al., 2011 [41]/France | NR | CR | Carvajal/Naxos syndrome (#605676/#601214) | M | 21 | AD | DSP | Permanent | 11 | 12, 15, 17, 22, 25, 27, 35, 37, 44, 45, 47 | Palmoplantar keratoderma, dilated cardiomyopathy, membranous ventricular septal defect | Wooly hair and oligodontia |
| Cho et al., 2004 [42]/China | China | CR | Incontinentia pigmenti/Block–Sulzberger syndrome (#308300) | M | 8 | X-linked dominant | NR | Permanent | 6 | 15, 21, 25, 31, 44, 45 | Typical inflammatory vesicles on the extremities shortly, linear verrucous, hyperkeratocic lesions on the extremities, hyperactivity, pigmentation on his trunk and limbs | Hypodontia deciduous, notch-shaped maxillary incisor, and oligodontia. |
| Clauss et al., 2014 [43]/France | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | NR | NR | WNT10A | Permanent | 15 | 13, 14, 15, 16, 17, 23, 24, 25, 26, 27, 34, 35, 43, 44, 45 | NR | Dry eyes, otitis, microdontia, cone-shaped teeth, and oligodontia |
| Cogulu and Ertugrul, 2008 [44]/Turkey | NR | CR | Oculofaciocardiodental syndrome (#300166) | F | 12 | X-linked dominant | NR | Permanent | 10 | 12, 15, 22, 25, 31, 32, 35, 41, 42, 45 | Mild cardiomegaly | Bilateral congenital cataracts, microphtalmia in the right eye, left exotropia at birth, bulbous and bifid nose, delayed eruption of the primary and permanent dentition, retained primary teeth, radiculomegaly in permanent maxillary incisorsa, and oligodontia |
| Cogulu et al., 2008 [45]/Turkey | NR | CR | Kabuki syndrome (#147920) | F | 11 | NR | NR | Permanent | 18 | 13, 14, 15, 17, 22, 23, 24, 25, 27, 32, 33, 35, 37, 42, 43, 44, 45, 47 | Mental retardation, skeletal anomalies, atrial septal defect. | Highly arched eyebrows, long palpebral fissures, eversion of the lower eyelids, large ears, flat nasal tip, cleft palate, abnormal tooth shape, widely spaced teeth, taurodont molar, and oligodontia |
| Costa et al., 2016 [46]/Brazil | Brazilian | CR | Zika virus syndrome (#448237) | M | 3-5 | NR | NR | Primary/Permanent | 12 20 | 1.51, 53, 55, 61, 63, 64, 65, 71,73,75, 81, 85 2.13, 14, 15, 17, 22, 24, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 47 | Cerebral palsy, foot syndactyly, and ventriculomegaly. | Mild epicanthal folds with triangular shaped facies, mild frontal bossing, fine lips, midface hypoplasia with shortened philtrum, bilateral and low- set posteriorly rotated ears small chin, and oligodontia |
| Dall’oca et al., 2008 [47]/Italy | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 11 | X-linked dominant | NR | Primary | 17 | 51, 52, 53, 55, 61, 62, 63, 65, 71, 72, 73, 74, 75, 81, 82, 83, 85 | Dry skin, delicate and prone rashes, thin, light blond and wooly hair, poor eyelashes and eyebrows, heat intolerance, hyper-pigmented in the periocular area and around the mouth | Slight depression of the bridge of the nose, malformed upper molars, conoid cusps and oligodontia |
| Devadas et al., 2005 [48]/India | India | CR | Witkop’s syndrome (#189500) | F | 5 | NR | NR | Permanent | 10 | 12, 22, 23, 25, 31, 32, 33, 41, 42, 43 | Short stature, hypoplastic fingernails, thin and easily chipped toenails | Scanty eyebrows, slightly drooping eyelids, prominent epicanthal folds, microdontia, and oligodontia |
| Downing and Welbury, 1992 [49]/United Kingdom | NR | CR | Trichorhinophalangeal syndrome (#190350) | M | 8 | NR | NR | Permanent | 8 | 12, 16, 22, 26, 31, 32, 41, 42 | Soft nails, dry skin, broad terminal phalanges of fingers and toes, short stature, cone-shaped epiphyses | Sparse blond hair, prominent ears, broad pear-shaped nose, a long philtrum, thin upper lip, class III malocclusion, and oligodontia |
| Dunbar et al., 2015 [50]/United Kingdom | NR | CR | Axenfeld–Rieger syndrome (#180500) | M | 10 | NR | NR | Permanent | 8 | 11, 12, 13, 21, 22, 32, 35, 45 | NR | Class III malocclusion and oligodontia |
| Emral and Akcam, 2009 [51]/Turkey | NR | CR | Noonan syndrome (#163950) | M | 13 | AD | NR | Permanent | 7 | 12, 22, 27, 34, 35, 45, 46 | Short stature, asymmetry between the left and right thorax, pectus excavatum, widely spaced nipples | Facial dismorphism, bilateral telecanthus, myopia, 13 diopter, low neck-hair line, mane neck, high palatal vault, drooping eyelids, asymmetric smile, low-set ears, thick helix of the ear, small, upturned nose, broad forehead, deeply grooved philtrum, and oligodontia |
| Fan et al., 2019 [52]/China | NR | CR | Axenfeld–Rieger syndrome (#180500) | 1:F 2:F 3:F 4:F | 7-29 | AD | PITX2 | Primary/Permanent | 1. 10 2. 9 3. 22 4. 9/19 | 1. 11, 12, 13, 14, 21, 22, 23, 27, 33, 43 2.11, 13, 21, 23, 31, 41, 42, 43, 45 3.11, 12, 13, 14, 15, 17, 21, 22, 23, 24, 25, 27, 31, 32, 33, 34, 35, 41, 42, 43, 44, 45 4.51, 52, 54, 55, 61, 62, 63, 64, 65/11, 12, 13, 14, 15, 16, 17, 21, 22, 23, 24, 25, 27, 31, 33, 35, 41, 45, 47 | Umbilical stump abnormality | Severe ocular anterior chamber anomalies, corneal opacity, iridocorneal adhesion, angle cosure, iris hypoplasia, corectopia, glaucoma, complete blindness, and oligodontia |
| Ghosh et al., 2019 [53]/India | India | CR | Microcephalic osteofysplastic dwarfism type II (#210720) | M | 8 | AR | PCNT | Permanent | 14 | 12, 13, 14, 15, 17, 22, 24, 31, 33, 34, 35, 43, 44, 45 | Hyperpigmented skin, hypotrichosis of scalp, eyebrow, eyelashes, thin upper and lower extremities with clinodactyly, bilateral flat foot, high-pitched voice, mild thracolumbar scoliosis | Micrognathia, large prominent eyes, beak-shaped nose with deviated nasal septum, conical roots, horizontal growth pattern with skeletal deep bite, craniostenosis, and oligodontia. |
| Gupta, 2012 [54]/India | India | CR | Oromandibular limb hypogenesis syndrome type I B (#103300) | M | 28 | NR | NR | Permanent | 10 | 12, 15, 22, 25, 31, 32, 35, 41, 42, 45 | Oropharyngeal isthmus absence of the palatoglossal arches | Medium height with a long narrow face, fused eyebrows, low-set ears, broad nasal alae, saddle nose, pointy tapering chin, thin lips, complete absence of tongue, and oligodontia |
| Hasan et al., 2019 [55}/India | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | F | 19 | AR | NR | Permanent | 15 | 11, 12, 21, 22, 23, 31, 32, 35, 36, 41, 42, 43, 44, 45, 46 | Heat intolerance with raised body temperature and reduced perspiration, short stature, normal-shaped fingers, and broad, short, and wide-spaced toes | Reduced anterior facial height and mild hyperpigmented, wrinkled periorbital skin, receding hairline, thin, lusterless hair with premature graying, prognathic mandible, and oligodontia |
| Hassona et al., 2018 [56]/Jordan | NR | CR | Sanjad–Sakati syndrome (#241410) | F | 15 | NR | TBCE | Permanent | 14 | 12, 13, 14, 15, 22, 23, 24, 25, 33, 34, 35, 42, 44, 45 | Hypocalcemia, hyperphosphatemia, low parathyroid hormone level, small hands and feet with short and thin digits, microcephaly | Low set ears, beaked nose, retrognathic mandible, thin lips, incomplete root formation, taurodontism, and oligodontia |
| Hattab et al., 1996 [57]/Iran | Jordan | CR | Grebe chondrodysplasia (#200700) | M | 9 | NR | NR | Permanent | 25 | 11, 12, 13, 14, 15, 17, 21, 22, 23, 24, 25, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 47 | Short stature, deformed limbs, difficulty walking, short and deformed arms, disproportionately short fingers, fingertips were budlike, small, and with dysplastic nails, markedly short and asymmetric legs, talipes equinovarus, irregular and bulbous toes, left ulna and fibula were hypoplastic, right fibula absent | Asymmetric and dysmorphic with a prominent forehead, flat occiput, depressed middle third of the face, ocular hypertelorism with antimongoloid slanting, severe loss of hearing, depressed bridge of the nose, frontal bossing, angular highly set orbital plates, hypoplastic maxilla, prognathic mandible, and oligodontia. |
| Hattab et al., 1997 [58]/Sweden | NR | CR | Polycystic ovarian syndrome (#184700) | 1: F 2: F | 1:21 2:18 | NR | NR | Permanent | 1.26 2.22 | 1. 12, 13, 14, 15, 16, 17, 22, 23, 24, 25, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 2.12, 13, 15, 16, 17, 22, 23, 24, 25, 26, 27, 31, 32, 33, 34, 35, 37, 41, 42, 44, 45, 46 | Enlarged ovaries with multiple cystic-like lesions | Long and coarse hair and oligodontia |
| Hingston et al., 2006 [59]/United Kingdom | NR | CR | Hurler’s syndrome (#607014) | F | 11 | NR | NR | Permanent | 8 | 14, 15, 24, 25, 34, 35, 44, 45 | Short stature | Large head, short neck, corneal clouding, depressed nasal bridge, broad nasal tip, long upper lip with relative flattening of the philtrum, and oligodontia |
| Jain et al., 2010 [60]/India | NR | CR | Hypohidrotic ectordemal dysplasia (#305100) | M | 13 | NR | NR | Permanent | 21 | 12, 13, 14, 15, 17, 22, 23, 24, 25, 27, 31, 32, 34, 35, 36, 37, 41, 42, 43, 44, 45 | Maculopapular eruptions, onchodysplasia | Protuberant supraorbital ridge, frontal bossing, sparse hairs, scant eyelashes and eyebrows, saddle nose, conical-shaped teeth, hypoplastic teeth, and oligodontia |
| Jain et al., 2012 [61]/India | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 11 | NR | NR | Permanent | 25 | 13, 14, 15, 16, 17, 21, 22, 24, 25, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 | Lack of sweating, dryness of skin, raised body temperature | Sparse hair, frontal bossing, prominent supra orbital ridges, depressed nasal bridge, sunken cheeks, protuberant lips, decreased lower facial height, absence of saliva, dry oral mucosa, and oligodontia |
| Kale et al., 2013 [62]/India | NR | CR | Achondroplasia (#100800) | F | 16 | NR | NR | Permanent | 18 | 12, 14, 16, 22, 24, 26, 31, 32, 33, 34, 35, 37, 41, 42, 43, 44, 45, 47 | Short stature, rhizomelic shortening of the arms and legs, lumbar lordosis, prominent buttocks, stubby fingers with trident hand, brachycephaly | Shortening of the skull base with frontal bossing, flat nasal bridge, retruded maxilla, hypertonic lips, and oligodontia |
| Kantaputra et al., 2014 [63]/Thailand | Thailand | CR | Tricho-odonto-onychodermal dysplasia (#275980) | 1: F 2: F 3: F | 16-27 | AR | WNT10A | Permanent | 1.26 2.21 3.12 | 1. 11, 12, 13, 14, 16, 17, 21, 22, 23, 24, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 2.12, 13, 14, 15, 17, 22, 23, 24, 25, 31, 32, 33, 34, 37, 41, 42, 43, 44, 45, 46, 47 3. 12, 14, 16, 22, 27, 31, 32, 35, 41, 42, 45, 46 | Dystrophic fingernails and toenails, palmoplantar keratoderma, dry skin, skin improved with age | Straight hair during childhood, slow growing scalp hair, dysplastic hair follicle, trichorrhexis nodosa-like hair anomaly, facial freckles, barrel-shaped mandibular incisors, and oligodontia |
| Kaul and Reddy, 2008 [64]/India | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 14 | NR | NR | Permanent | 24 | 12, 13, 14, 15, 16, 17, 22, 23, 24, 25, 26, 27, 31, 32, 33, 34, 35, 37, 41, 42, 43, 44, 45, 47 | Dry skin, frequent bouts of fever, intolerant to heat, scanty body hair | Frontal bossing, scanty scalp hair, periorbital pigmentation, low-set ears, depressed nasal, protuberant lips, dry mucosa, malformed incisors impacted, and oligodontia |
| Kawamoto, Motohashi and Ohyama, 2004 [65]/Japan | Japan | CR | Oculofaciocardiodental syndrome (#300166) | F | 13 | X-linked dominant | NR | Permanent | 7 | 12, 15, 24, 31, 32, 35, 41 | Cardiac anomalies | Congenital cataract, dental root gigantism, and oligodontia |
| Khabour et al., 2010 [66]/Jordan | Jordan | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 11 | X-linked | EDA | Permanent | 17 | 12, 14, 15, 17, 22, 24, 25, 27, 32, 34, 35, 36, 37, 42, 44, 45, 47 | Damaged eccrine glands (anhidrosis) | Sparse scalp hair, absent eyebrows and eyelashes, periorbital wrinkling, saddle nose, protuberant lips, abnormally shaped upper and lower permanent teeth, and oligodontia. |
| Khurana et al., 2012 [67]/Jordan | NR | CR | Witkop syndrome (#189500) | M | 20 | AD | MSX1 | Permanent | 11 | 11, 12, 17, 21, 22, 27, 31, 35, 37, 44, 47 | Abnormalities of both toenails and fingernails | Sparse scalp hair, smaller mandibles, and oligodontia |
| Kinyó et al., 2014 [68]/Hungary | Hungary | CR | Christ–Siemens–Touraine syndrome (#305100) | M | 35 | X-linked | EDA | Permanent | 25 | 11, 14, 15, 16, 17, 21, 22, 24, 25, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 | Dryness of the skin, eyes, airways, and mucous membranes | Missing eyebrows and eyelashes, sparse hair, and oligodontia |
| Kishore et al., 2014 [69]/India | India | CR | Hypohidrotic ectodermal dysplasia (#305100) | 1: M 2: M | 1:20 2:25 | X-linked recessive | NR | Permanent | 24 | 17, 16, 15, 14, 13, 23, 24, 25, 26, 27, 37, 36, 35, 34, 33, 32, 31, 41, 42, 43, 44, 45, 46, 47 | Skin was dry and wrinkled with no nail dystrophy | Frontal bossing, scarce eyebrows and eyelashes, thinning of scalp hair, prominent supraorbital ridges, depressed nasal bridge, thick and prominent lips with a concave profile, and oligodontia |
| Kobayashi et al., 2022 [70]/Japan | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | F | 24 | AD | EDA | Permanent | 25 | 11, 12, 13, 14, 15, 17, 21, 22, 23, 24, 25, 27, 31, 32, 33, 34, 35, 37, 41, 42, 43, 44, 45, 46, 47 | Mammary glands hypoplastic and the surfaces of her palms and soles glossy and partially eroded | The lower face was short, the oral fissure was narrow, the middle face sank, and the lips protruded, resembling the so-called prematurely aged face in the profile, scalp hair thin and soft, and oligodontia |
| Kozma, et al., 1999 [71]/United States of America | Saudia Arabia | CR | Wolf–Hirschhorn syndrome (#194190) | M | 11 | NR | NR | Permanent | 9 | 14, 24, 31, 34, 35, 37, 41, 44, 45 | NR | Oligodontia |
| Kramer et al., 2005 [72]/Germany | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 3 | NR | NR | Primary /Permanent | 1. 18/26 | 52, 53, 54, 55, 62, 63, 64, 65, 71, 72, 73, 74, 75, 81, 82, 83, 84, 85 / 12, 13, 14, 15, 16, 17, 22, 23, 24, 25, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 | Dry hypopigmented scaly skin | Hair was thin, sparse, and blond with sparse eyelashes and eyebrows, as well as oligodontia |
| Kroigard et al., 2016 [73]/Denmark | NR | CR | Odonto-onychodermal dysplasia (#257980) | F | 75 | NR | WNT10A | Permanent | 26 | 12, 13, 14, 15, 16, 17, 22, 23, 24, 25, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 | Dry skin, slightly dystrophic and brittle finger and toe nails with spooning. | Erythematous plaques on both cheeks and the nose, facial basal cell carcinomas, and oligodontia |
| Levy et al., 2020 [74]/France | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | 1: F 2:M | 1:23 2:6 | X-linked | LEF1 | Primary/Permanent | 1. 7/19 2. 19 | 1. 55, 53, 63, 65, 73, 74, 75/17, 16, 15, 14, 13, 24, 25, 26, 27, 35, 34, 33, 32, 31, 41, 42, 43, 44, 45 2. 16, 15, 14, 12, 22, 24, 27, 37, 35, 34, 33, 32, 31, 41, 42, 43, 44, 45, 47 | NR | 1: Sparse, fine hair, sparse eyelashes and eyebrows, and oligodontia; 2: Sparse, fine hair, sparse eyelashes and eyebrows, microdontia, and oligodontia. |
| Liedén et al., 2014 [75]/Sweden | NR | CR | AT-rich sequence-binding protein 2 gene (#608148) | M | 20 | NR | NR | Permanent | 10 | 11, 12, 13, 14, 24, 25, 33, 35, 43, 44 | Impairment of fine and gross motor skills, left-sided mild hemiparesis, and spasticity with increased reflexes in the upper and lower extremities bilaterally, mild–moderate osteoporosis | Tall forehead, bushy eyebrows, a prominent nose, cleft palate was noted early, with surgical correction at the age of 11 months, conical front teeth, generally large teeth crowns and with extremely short, malformed roots and oligodontia |
| Lin et al., 2022 [76]/China | NR | CR | Blepharocheilodontic syndrome (#119580) | 1:M 2:F | 9 35 | AD | CDH1 | Permanent | 1.14 2.19 | 1. 11, 12, 13, 14, 15, 21, 22, 23, 24, 25, 31, 34, 41, 44 2. 11, 12, 13, 15, 21, 22, 23, 24, 25, 31, 32, 33, 34, 35, 41, 42, 43, 44, 45 | Euryblepharon, ectropion, distichiasis | High frontal hairline, broad forehead, and oligodontia |
| Martinho, et al., 2019 [77]/Portugal | NR | CR | Oculofaciocardiodental syndrome (#300166) | F | 26 | X-linked dominant | NR | Permanent | 10 | 13, 15, 16, 22, 24, 26, 27, 36, 37, 46 | Mild cardiomegaly, a misalignment of her thumbs, valgus foot, and prolapsed mitral valve | Long, narrow face (dolichocephalous) with a bifid tip of the nose and very deep-set eyes with cataract, and oligodontia |
| Marvin et al., 2011 [78]/United States of America | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | F | 35 | NR | AXIN2 | Permanent | 11 | 13, 17, 23, 27, 31, 32, 37, 41, 42, 43, 47 | NR | Hypognathia, fine scalp hair, very sparse eyebrows, slightly up-slanting palpebral fissures, malar hypoplasia, broad nasal bridge, fine scalp hair, slightly up-slanting palpebral fissure, and oligodontia |
| Murata et al., 2019 [79]/Japan | Japan | CR | Basal cell nevus syndrome (#109400) | F | 6 | NR | PTCH1 | Permanent | 10 | 12, 14, 15, 22, 24, 25, 31, 34, 35, 45 | Cheiloplasty, palatoplasty, and surgical excision of cardiac fibroma and palmar pits | Ocular hypertelorism, bilateral cleft lip and palate, and oligodontia |
| O’Dwyer and Jones, 2005 [80]/United Kingdom | NR | CR | Axenfeld–Rieger syndrome (#180500) | F | 10 | NR | NR | Permanent | 11 | 11, 12, 13, 21, 22, 23, 27, 32, 35, 42, 45 | NR | Severe hypodontia, microdontia, short root, and oligodontia |
| Pipa Vallejo et al., 2008 [81]/Turkey | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 5 | X-linked recessive | NR | Primary | 15 | 54, 53, 51, 63, 64, 65, 75, 74, 73, 72, 71, 81, 83, 84, 85 | Fine dry skin on the palms and soles | Parse, fine silky hair, thinly covering the scalp, thin eyebrows, folded lower eyelid, narrow nose at the tip, thick lower lip, and oligodontia |
| Reiche et al., 2014 [82]/United States of America | NR | CR | Down’s syndrome (#190685) | NR | 18 | NR | NR | Permanent | 6 | 12, 17, 22, 27, 31, 41 | NR | Macroglossia and oligodontia |
| Retna and Sockalingam, 2003 [83]/Malaysia | China | CR | Blepharocheilodontic syndrome (#119580) | F | 5 | NR | NR | Permanent | 20 | 11, 13, 14, 15, 17, 21, 22, 24, 25, 31, 32, 33, 34, 35, 37, 41, 42, 43, 44, 45 | Bilateral eye anomalies that include ectropion of the lower eyelids, lagophthalmos, hypertelorism, distichiasis and euryblepharon, and scalp hair was sparse and straight | Bilateral cleft lip and palate, microstomia, and oligodontia and microdontia with conical-shaped teeth |
| Richieri-Costa et al.,1993 [84]/Canada | NR | CR | Carpenter syndrome (#201000) | F | 6 | NR | NR | Permanent | 26 | 12, 13, 14, 15, 16, 17, 22, 23, 24, 25, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 | Hypertelorism, small hands, brachydactyly, camptodactyly of the left third finger, small feet, proximal cutaneous syndactyly of toes, and clinodactyly of toes | Thick neck, dolichoplagiomacrocephaly, prominent forehead, blow nasal bridge, hypoplastic alveolar ridges, and oligodontia |
| Rizos et al., 1998 [85]/United States of America | NR | CR | Mobius syndrome (#157900) | F | 17 | NR | NR | Permanent | 8 | 11, 17, 23, 24, 25, 26, 27, 32 | NR | Facial hemiplegia and oligodontia |
| Rock and McLellan, 1990 [86]/United Kingdom | NR | CR | Klinefelter syndrome (NR) | M | 8 | NR | NR | Permanent | 11 | 12, 14, 15, 22, 24, 25, 34, 35, 37, 44, 45 | NR | Broad nasal bridge and hypertelorism |
| Shen et al., 2011 [87]/China | China | CR | Ellis–van Creveld syndrome (#225500) | F | 6 | AR | EVC2 | Permanent | 8 | 12, 13, 22, 23, 31, 32, 41, 42 | Postaxial polydactyly of both hands, syndactyly of the toes and nail dysplasia, and abnormalities of the knee joints | Hipodontia and oligodontia |
| Siddiqui et al., 2021 [88]/India | NR | CR | Axenfeld–Rieger syndrome(#180500) | F | 11 | AD | PITX2 | Permanent | 14 | 11, 12, 14, 15, 16, 17, 21, 22, 25, 31, 32, 35, 41, 42 | Ophthalmic records revealed anterior segment dysgenesis with corectopia (displacement of the pupil) and polycoria (multiple pupils) | Maxillary hypoplasia with poor upper lip support and thick everted lower lip and oligodontia |
| Sikora et al., 2016 [89]/Australia | NR | CR | Juvenile nephronophtisis (#256100) | F | 11 | NR | NPHP1 | Permanent | 12 | 12, 17, 23, 26, 27, 31, 32, 33, 37, 41, 42, 47 | Short hands and feet and genu valgum | Dysmorphic face—broad nose, large mouth, small chin, bilateral fusion of the 1 and 2 upper teeth, and oligodontia |
| Singh et al., 2001 [90]/India | India | CR | Floating-Harbor syndrome (#136140) | M | 14 | NR | SRCAP | Permanent | 8 | 12, 22, 23, 31, 32, 33, 41, 43 | Bilateral inguinal testis, cryptorchidism, hypospadias, and congenital absence of right kidney | Leptoproscopic facial form, deep-set eyes, long eyelashes, ptosis of upper eyelids, reduced malar prominence, low-set ears with outwardly rotated ear lobes, broad and bulbous nose, low-hanging columella, smooth philtrum, reduced dry vermilion of the upper lip, slightly everted lower lip, ankyloglossia with thick frenum and restricted tongue movements, and oligodontia |
| Subramaniam and Neeraja, 2008 [91]/India | NR | CR | Witkop’s syndrome (#189500) | M | 14 | NR | NR | Permanent | 24 | 12, 13, 14, 15, 17, 22, 23, 24, 25, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 | NR | Oligodontia |
| Suda et al., 2010 [92]/Japan | NR | CR | Hypohidrotic Ectodermal dysplasia (#305100) | M | 5 | NR | EDARADD | Permanent | 27 | 11, 12, 13, 14, 15, 16, 17, 21, 22, 23, 24, 25, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 47 | Unable to sweat | Hair and eyebrows were sparse, oligondontia |
| Sultan et al., 2020 [93]/India | NR | CR | Down syndrome (#190685) | M | 12 | NR | NR | Permanent | 8 | 12, 22, 31, 35, 37, 41, 42, 45 | Short stature and mentally challenged | Saddle nose deformity, hypertelorism, midface hypoplasia with retruded maxilla and protruded mandible, including the intra-oral aspects of the high arch palate, macroglossia of the tongue, and oligodontia |
| Sun et al., 2019 [94]/China | China | CR | Incontinentia pigmenti (#308300) | F | 15 | X-linked dominant | IKBKG | Permanent | 11 | 15, 17, 22, 24, 25, 34, 35, 37, 44, 45, 46 | NR | Oligodontia |
| Talasila et al., 2017 [95]/India | India | CR | Acromelia-oligodontia syndrome (NR) | M | 18 | NR | NR | Permanent | 6 | 31, 33, 35, 36, 37, 41 | The forelimbs show rudimentary thumbs and acromelia | High forehead, zygomatic and mandibular hypoplasia on the left, deviation of the chin to the left, blepharophimosis, ankyloglossia, and oligodontia |
| Tanboga et al., 2001 [96]/Turkey | India | CR | Incontinentia pigmenti (#308300) | F | 6 | X-linked dominant | NR | Primary/Permanent | 8/17 | 52, 62, 64, 72, 75, 81, 82, 85/12, 13, 14, 15, 17, 22, 23, 24, 25, 27, 32, 35, 37, 41, 42, 45, 47 | NR | Oligodontia |
| Tanboga, et al., 1992 [97]/Turkey | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 7 | NR | NR | Permanent | 8 | 11, 16, 21, 26, 32, 36, 42, 46 | Hands and feet characterized by syndactyly of the digits and absent, hypoplastic, or fused phalanges and metacarpals | Hair and eyebrows were sparse, oligondontia |
| Tao et al., 2010 [98]/United States of America | NR | CR | Beare–Stevenson syndrome (#123790) | M | 6 | AD | FGFR2 | Permanent | 9 | 15, 25, 31, 32, 35, 41, 42, 44, 45 | Cutis gyrate, acanthosis nigricans, skin tags, ear defects, anogenital anomalies, and a prominent umbilical stump | Midface hypoplasia, natal teeth, and oligodontia |
| Tosun et al., 2006 [99]/Turkey | NR | CR | Apert syndrome (#101200) | M | 4 | AD | NR | Primary/ Permanent | 8/8 | 52, 55, 62, 65, 72, 75, 82, 85/14, 15, 24, 25, 34, 35, 44, 45 | Syndactyly of hands and feet digit | Displayed midface hypoplasia, a flat/steep forehead, an extremely short, depressed nose, proptosis, trapezoidal shape of mouth, tongue appeared excessively large, pseudo cleft palate, and oligodontia |
| Tuna et al., 2009 [100]/Istanbul | NR | CR | Hallermann–Streiff (HSS) syndrome (#234100) | F | 10 | NR | NR | Permanent | 16 | 12, 14, 15, 22, 24, 25, 31, 32, 33, 34, 35, 41, 42, 43, 44, 45 | Decreased oropharyngeal airway | Micrognathia, sparse hair, eyebrows, eyelashes, cutaneous atrophy, congenital bilateral cataracts, ptosis, horizontal nystagmus, blue sclera, mildly down-slanting palpebral fissures, lateral collapse of the middle and lower lateral cartilages at the nose, hypertrophy of the turbinates, excessive long soft palate, nasal septum deviated, open bite, moderate anterior crowding and malformed teeth, bilateral posterior crossbite, prominent tongue-thrust swallowing, excessive vertical dimension of the lower third of the face, and oligodontia |
| Tuna et al., 2012 [101]/Turkey | NR | CR | Kabuki syndrome (#147920) | M | 5 | AD | NR | Permanent | 10 | 12, 14, 22, 24, 32, 33, 35, 42, 43, 45 | Short fifth finger, small middle phalanges, and hyperelastic finger joints | Long and everted lateral and palpebral fissures, dysplastic prominent ears, blue sclera, a short nasal septum, depressed nasal tip, hypermobility of the joints, and oligodontia |
| Vasudevan and Sinha, 2023 [102]/India | NR | CR | Odonto-onychiadermal dysplasia (#257980) | M | 19 | NR | NR | Permanent | 24 | 11, 12, 13, 14, 15, 16, 17, 22, 23, 24, 25, 26, 31, 32, 33, 34, 35, 37, 41, 42, 43, 44, 45, 47 | Hyperkeratosis on the pal mar aspect of both hands, dystrophy of the toe nails, and ichthyosis of posterior aspect of legs | Oligodontia |
| Waldron et al., 2010 [103]/Ireland | Ireland | CR | Axenfeld–Rieger syndrome (#180500) | F | 7 | AD | NR | Permanent | 14 | 11, 12, 13, 21, 22, 23, 31, 32, 33, 35, 41, 42, 43, 45 | NR | Oligodontia |
| Yin et al., 2013 [104]/China | NR | CR | Hypohidrotic ectodermal dysplasia (#305100) | M | 5 | NR | EDA | Permanent | 26 | 12, 13, 14, 15, 16, 17, 22, 23, 24, 25, 26, 27, 31, 32, 33, 34, 35, 36, 37, 41, 42, 43, 44, 45, 46, 47 | NR | Oligodontia |
| Zidane and Alloussi, 2022 [105]/Marrocos | NR | CR | Dubowitz syndrome (#223370) | M | 6 | AR | NR | Permanent | 15 | 15, 14, 13, 12, 22, 23, 24, 25, 35, 34, 32, 31, 41, 44, 45 | NR | Had a high-pitched voice, mild mental retardation, and oligodontia |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castilho, N.L.; Resende, K.K.M.; Santos, J.A.d.; Machado, R.A.; Coletta, R.D.; Guerra, E.N.S.; Acevedo, A.C.; Martelli-Junior, H. Oligodontia in the Clinical Spectrum of Syndromes: A Systematic Review. Dent. J. 2023, 11, 279. https://doi.org/10.3390/dj11120279
Castilho NL, Resende KKM, Santos JAd, Machado RA, Coletta RD, Guerra ENS, Acevedo AC, Martelli-Junior H. Oligodontia in the Clinical Spectrum of Syndromes: A Systematic Review. Dentistry Journal. 2023; 11(12):279. https://doi.org/10.3390/dj11120279
Chicago/Turabian StyleCastilho, Natália Lopes, Kêmelly Karolliny Moreira Resende, Juliana Amorim dos Santos, Renato Assis Machado, Ricardo D. Coletta, Eliete Neves Silva Guerra, Ana Carolina Acevedo, and Hercílio Martelli-Junior. 2023. "Oligodontia in the Clinical Spectrum of Syndromes: A Systematic Review" Dentistry Journal 11, no. 12: 279. https://doi.org/10.3390/dj11120279
APA StyleCastilho, N. L., Resende, K. K. M., Santos, J. A. d., Machado, R. A., Coletta, R. D., Guerra, E. N. S., Acevedo, A. C., & Martelli-Junior, H. (2023). Oligodontia in the Clinical Spectrum of Syndromes: A Systematic Review. Dentistry Journal, 11(12), 279. https://doi.org/10.3390/dj11120279