
Clinical Performance Comparing Titanium and Titanium–Zirconium or Zirconia Dental Implants: A Systematic Review of Randomized Controlled Trials

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Data Sources
2.1. Focused Question
2.2. Information Sources and Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
3. Resources Selection
3.1. Studies Selection
3.2. Data Extraction and Method of Analysis
3.3. Risk of Bias and Quality Assessment
4. Review
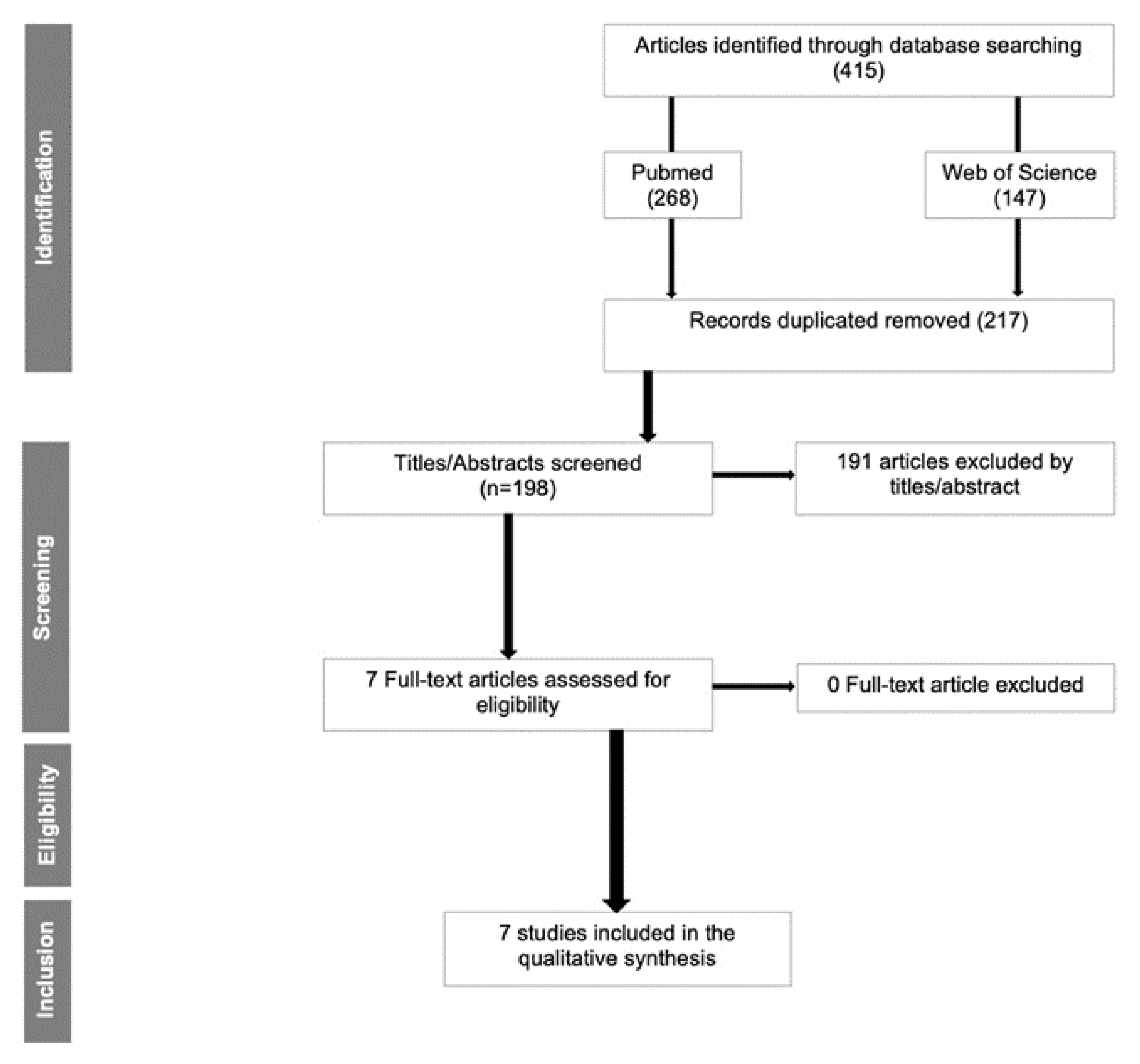
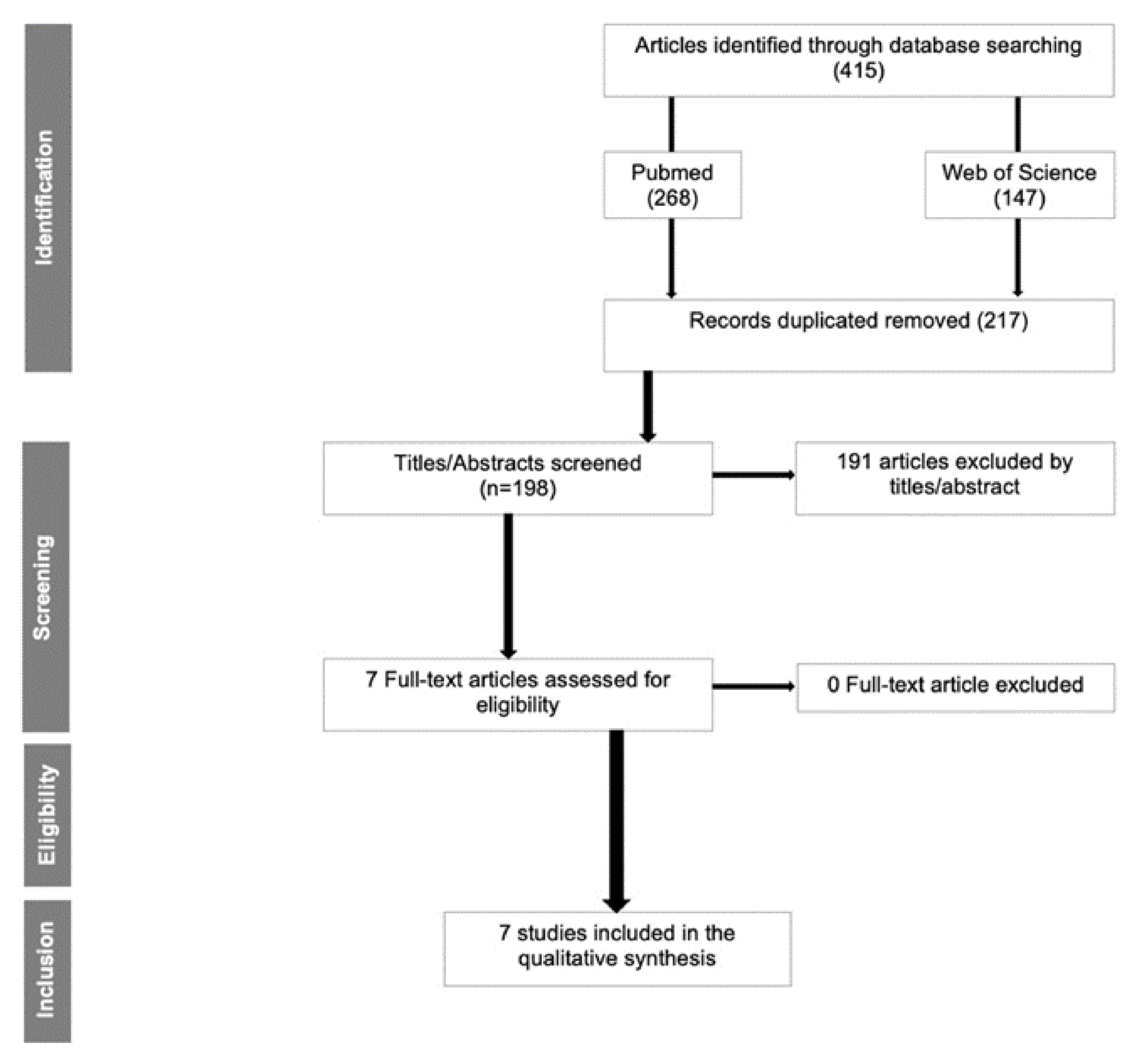
4.1. Study Selection
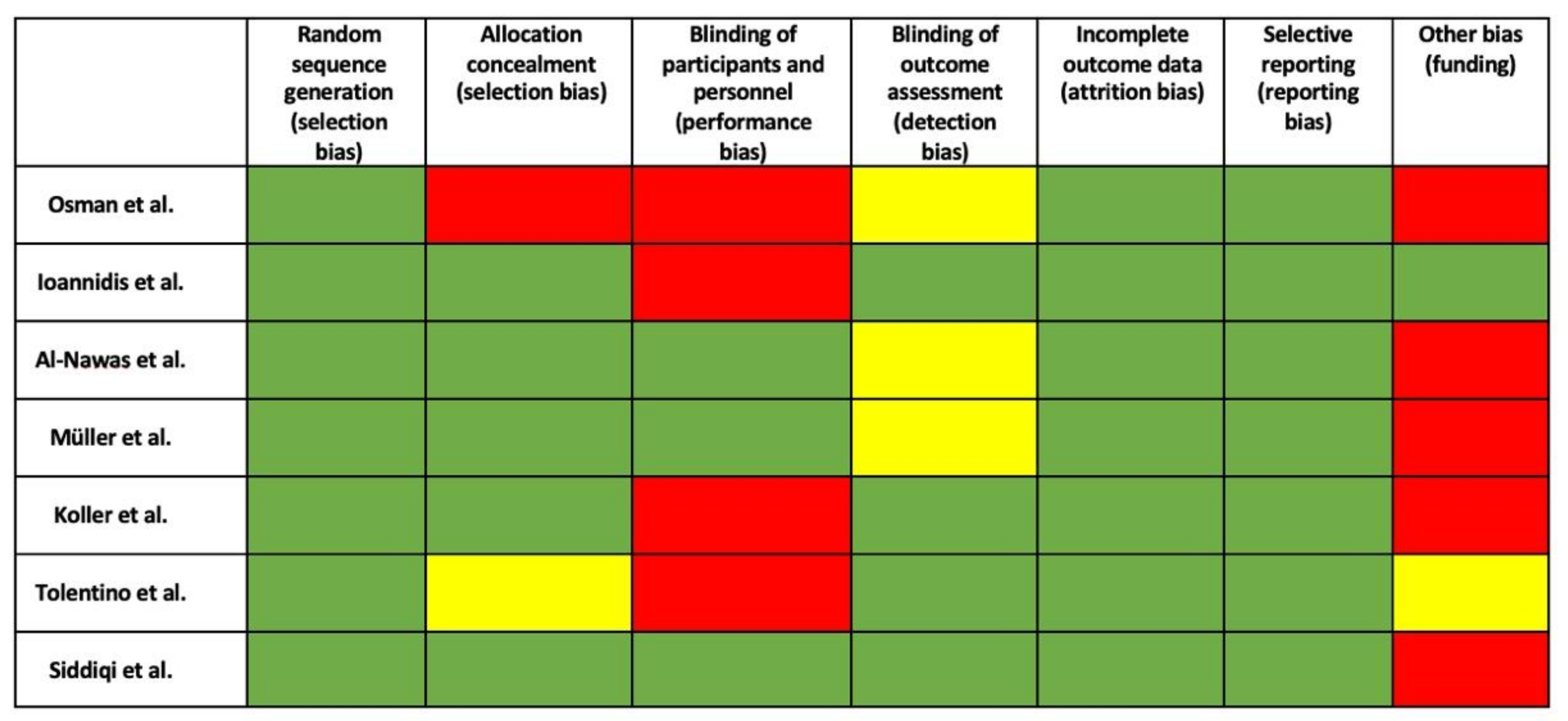
4.2. Risk of Bias
4.3. Study Characteristics
4.4. Smokers
4.5. Implant Features
4.6. Survival Rate (SR)
4.7. Peri-Implant Mucositis and Peri-Implantitis
4.8. Bleeding on Probing (BoP)
4.9. Probing Depth (PD)
5. Discussion
5.1. Smoking History
5.2. Survival Rate (SR)
5.3. Marginal Bone Loss (MBL)
5.4. Mucositis/Peri-Implantitis
5.5. Bleeding on Probing (BoP) and Probing Depth (PD)
5.6. Study Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Karoussis, I.K.; Salvi, G.E.; Heitz-Mayfield, L.J.; Brägger, U.; Hämmerle, C.H.; Lang, N.P. Long-term implant prognosis in patients with and without a history of chronic periodontitis: A 10-year prospective cohort study of the ITI® Dental Implant System. Clin. Oral Implant. Res. 2003, 14, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontol. 2000 2017, 73, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Borges, H.; Correia, A.; Castilho, R.; Fernandes, G. Zirconia Implants and Marginal Bone Loss: A Systematic Review and Meta-Analysis of Clinical Studies. Int. J. Oral Maxillofac. Implant. 2020, 35, 707–720. [Google Scholar] [CrossRef] [PubMed]
- Howe, M.-S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, P.-I.; Breine, U.; Adell, R.; Hansson, B.O.; Lindström, J.; Ohlsson, Å. Intra-Osseous Anchorage of Dental Prostheses: I. Experimental Studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar] [CrossRef]
- Schroeder, A.; Sutter, F.; Ledermann, P.D.; Stich, H. Current experience with the ITI double hollow cylinder implant type K. Internationales Team für orale Implantologie. Schweiz. Mon. Zahnmed. 1984, 94, 503–510. [Google Scholar]
- Buser, D.; Schenk, R.K.; Steinemann, S.; Fiorellini, J.P.; Fox, C.H.; Stich, H. Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. J. Biomed. Mater. Res. 1991, 25, 889–902. [Google Scholar] [CrossRef]
- Buser, D. Effects of various titanium surface configurations on osseointegration and clinical implant stability. In Proceedings of the 3rd European Workshop on Periodontology: Implant Dentistry; Lang, N.P., Karring, T., Lindhe, J., Eds.; Quintessence: Berlin, Germany, 1999; pp. 88–101. [Google Scholar]
- Chaturvedi, T.P. An overview of the corrosion aspect of dental implants (titanium and its alloys). Indian J. Dent. Res. 2009, 20, 91–98. [Google Scholar] [CrossRef]
- Cionca, N.; Hashim, D.; Mombelli, A. Zirconia dental implants: Where are we now, and where are we heading? Periodontol. 2000 2017, 73, 241–258. [Google Scholar] [CrossRef]
- Kelly, J.R.; Denry, I. Stabilized zirconia as a structural ceramic: An overview. Dent. Mater. 2008, 24, 289–298. [Google Scholar] [CrossRef]
- Lughi, V.; Sergo, V. Low temperature degradation-aging- of zirconia: A critical review of the relevant aspects in dentistry. Dent. Mater. 2010, 26, 807–820. [Google Scholar] [CrossRef]
- Kohal, R.-J.; Knauf, M.; Larsson, B.; Sahlin, H.; Butz, F. One-piece zirconia oral implants: One-year results from a prospective cohort study. 1. Single tooth replacement. J. Clin. Periodontol. 2012, 39, 590–597. [Google Scholar] [CrossRef]
- Oliva, J.D.; Oliva, X. Five-year success rate of 831 consecutively placed Zirconia dental implants in humans: A comparison of three different rough surfaces. Int. J. Oral Maxillofac. Implant. 2010, 25, 336–344. [Google Scholar]
- Osman, R.B.; Swain, M.V.; Atieh, M.; Ma, S.; Duncan, W. Ceramic implants (Y-TZP): Are they a viable alternative to titanium implants for the support of overdentures? A randomized clinical trial. Clin. Oral Implant. Res. 2014, 25, 1366–1377. [Google Scholar] [CrossRef]
- Rocchietta, I.; Fontana, F.; Addis, A.; Schupbach, P.; Simion, M. Surface-modified zirconia implants: Tissue response in rabbits. Clin. Oral Implant. Res. 2009, 20, 844–850. [Google Scholar] [CrossRef]
- Akagawa, Y.; Hosokawa, R.; Sato, Y.; Kamayama, K. Comparison between freestanding and tooth-connected partially stabilized zirconia implants after two years’ function in monkeys: A clinical and histologic study. J. Prosthet. Dent. 1998, 80, 551–558. [Google Scholar] [CrossRef]
- Lorusso, F.; Noumbissi, S.; Francesco, I.; Rapone, B.; Khater, A.G.A.; Scarano, A. Scientific Trends in Clinical Research on Zirconia Dental Implants: A Bibliometric Review. Materials 2020, 13, 5534. [Google Scholar] [CrossRef]
- Reis, R.; Nicolau, P.; Calha, N.; Messias, A.; Guerra, F. Immediate versus early loading protocols of titanium-zirconium narrow-diameter implants for mandibular overdentures in edentulous patitents: 1-year results from a randomized controlled trial. Clin. Oral Implant. Res. 2019, 30, 953–961. [Google Scholar] [CrossRef]
- Quirynen, M.; Al-Nawas, B.; Meijer, H.J.A.; Razavi, A.; Reichert, T.E.; Schimmel, M.; Storelli, S.; Romeo, E.; The Roxolid Study Group. Small-diameter titanium Grade IV and titanium-zirconium implants in edentulous mandibles: Three-year results from a double-blind, randomized controlled trial. Clin. Oral Implant. Res. 2015, 26, 831–840. [Google Scholar] [CrossRef]
- Cruz, R.S.; Lemos, C.A.A.; Oliveira, H.F.F.; Batista, V.E.S.; Pellizzer, E.P.; Verri, F.R. Comparison of the Use of Titanium–Zirconium Alloy and Titanium Alloy in Dental Implants: A Systematic Review and Meta-Analysis. J. Oral Implantol. 2018, 44, 305–312. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Ioannidis, A.; Gallucci, G.O.; Jung, R.E.; Borzangy, S.; Hämmerle, C.H.F.; Benic, G.I. Titanium-zirconium narrow-diameter versus titanium regular-diameter implants for anterior and premolar single crowns: 3-year results of a randomized controlled clinical study. J. Clin. Periodontol. 2015, 42, 1060–1070. [Google Scholar] [CrossRef]
- Siddiqi, A.; Kieser, J.A.; De Silva, R.K.; Thomson, W.M.; Duncan, W.J. Soft and Hard Tissue Response to Zirconia versus Titanium One-Piece Implants Placed in Alveolar and Palatal Sites: A Randomized Control Trial. Clin. Implant Dent. Relat. Res. 2015, 17, 483–496. [Google Scholar] [CrossRef]
- Al-Nawas, B.; Brägger, U.; Meijer, H.J.; Naert, I.; Persson, R.; Perucchi, A.; Quirynen, M.; Raghoebar, G.M.; Reichert, T.E.; Romeo, E.; et al. A double-blind randomized controlled trial (RCT) of Titanium-13Zirconium versus. Clin. Implant Dent. Relat. Res. 2012, 14, 896–904. [Google Scholar] [CrossRef] [Green Version]
- Koller, M.; Steyer, E.; Theisen, K.; Stagnell, S.; Jakse, N.; Payer, M. Two-piece zirconia versus titanium implants after 80 months: Clinical outcomes. Clin. Oral Implant. Res. 2020, 31, 388–396. [Google Scholar] [CrossRef] [Green Version]
- Müller, F.; On behalf of the Roxolid Study Group; Al-Nawas, B.; Storelli, S.; Quirynen, M.; Hicklin, S.; Castro-Laza, J.; Bassetti, R.; Schimmel, M. Small-diameter titanium grade IV and titanium-zirconium implants in edentulous mandibles: Five-year results from a double-blind, randomized controlled trial. BMC Oral Health 2015, 15, 123. [Google Scholar] [CrossRef] [Green Version]
- Tolentino, L.; Sukekava, F.; Garcez-Filho, J.; Tormena, M.; Lima, L.A.; Araújo, M.G. One-year follow-up of titanium/zirconium alloy X commercially pure titanium. Clin. Oral Implant. Res. 2016, 27, 393–398. [Google Scholar] [CrossRef]
- Alfadda, A.S. Current Evidence on Dental Implants Outcomes in Smokers and Nonsmokers: A Systematic Review and Meta-Analysis. J. Oral Implantol. 2018, 44, 390–399. [Google Scholar] [CrossRef]
- Hashim, D.; Cionca, N.; Courvoisier, D.S.; Mombelli, A. A systematic review of the clinical survival of zirconia implants. Clin. Oral Investig. 2016, 20, 1403–1417. [Google Scholar] [CrossRef] [Green Version]
- Elnayef, B.; Lázaro, A.; Del Amo, F.S.L.; Galindo-Moreno, P.; Wang, H.L.; Gargallo-Albiol, J.; Hernandéz-Alfaro, F. Zirconia implants as an alternative to titanium: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implant. 2017, 32, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roehling, S.; Woelfler, H.; Hicklin, S.; Kniha, H.; Gahlert, M. A Retrospective Clinical Study with Regard to Survival and Success Rates of Zirconia Implants up to and after 7 Years of Loading. Clin. Implant Dent. Relat. Res. 2016, 18, 545–558. [Google Scholar] [CrossRef] [PubMed]
- Roehling, S.; Schlegel, K.A.; Woelfler, H.; Gahlert, M. Performance and outcome of zirconia dental implants in clinical studies: A meta-analysis. Clin. Oral Implant. Res. 2018, 29, 135–153. [Google Scholar] [CrossRef] [PubMed]
- Altuna, P.; Lucas-Taulé, E.; Gargallo-Albiol, J.; Figueras-Álvarez, O.; Hernandéz-Alfaro, F.; Nart, J. Clinical evidence on titanium-zirconium dental implants: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 842–850. [Google Scholar] [CrossRef]
- Badran, Z.; Struillou, X.; Strube, N.; Bourdin, D.; Dard, M.; Soueidan, A.; Hoornaert, A. Clinical Performance of Narrow-Diameter Titanium-Zirconium Implants: A Systematic Review. Implant Dent. 2017, 26, 316–323. [Google Scholar] [CrossRef]
- Pozzan, M.C.; Grande, F.; Zamperoli, E.M.; Tesini, F.; Carossa, M.; Catapano, S. Assessment of Preload Loss after Cyclic Loading in the OT Bridge System in an “All-on-Four” Rehabilitation Model in the Absence of One and Two Prosthesis Screws. Materials 2022, 15, 1582. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| MEDLINE (PubMed) | Web of Science (WoS) | |
|---|---|---|
| #1 | P—Edentulous patients treated with dental implants | |
| ((“Dental Implants” (MeSH Terms)) OR (Dental Implant † (Supplementary Concept))) | ‘tooth implantation’ OR ‘tooth implant’ OR ‘dental implant’ OR ‘dental implants’ | |
| #2 | I—Rehabilitation with zirconia or titanium–zirconium dental implants | |
| ((“Zirconium” (MeSH Terms)) OR (Zirconium Oxide (Supplementary Concept)) OR (Zirconia (Supplementary Concept)) OR (Yttria Stabilized Tetragonal Zirconia (Supplementary Concept)) OR (“Ceramics” (MeSH Terms))) | ‘zirconium oxide’ OR ‘zirconium’ OR ‘ceramics’ OR ‘yttria stabilized tetragonal zirconia’ | |
| #3 | C—Rehabilitation with titanium dental implants | |
| #4 | O—Clinical outcomes (survival rate, success rate, marginal bone loss, probing in-depth, bleeding on probing, and osseointegration level) | |
| #5 | T—At least 6 months | |
| Search Combination | (#1 AND #2) No combination conducted done with #3, and #4 since most of the papers on dental implants are about titanium, and the combination with keywords related to outcome would limit the search even more. Item #5 was manually evaluated. | |
| Filters | English, humans, 10 years | |
| Author | Year | Patients | Period | Mean Age | Gender | Dropout | Titanium Implant (n) | Zirconia Implant (n) | Connection | Company | Implant Lost | Type of Rehabilitation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Koller et al. | 2020 | 22 | 80 months | 46 | 13M/9F | 0 | 15 | 16 (Zr) | Morse-taper | Ziterion® (Vario T; Ziterion) | 1 Ti/2 Zr | All ceramic (lithium disilicate) single restorations |
| Müller et al. | 2015 | 47 | 5 years | 72 | 24M/23F | 16 | 47 | 47 (TZ) | Morse-taper | Straumann (Bone Level) | 1 Ti/1 TZ | Overdentures |
| Ioannidis et al. | 2015 | 40 | 3 years | NR | Not clear | NR | 20 | 20 (TZ) | Morse-taper | Straumann | NR | Single-implant crown (porcelain-fused-to-metal crowns) in the anterior or premolar regions |
| Tolentino et al. | 2016 | 12 | 1 year | 43.3 | 4M/8F | 0 | 5 | 5 (TZ) | Morse-taper | Straumann | 0 | Screw-retained single metal-ceramic crown in the mandible |
| Osman et al. | 2013 | 24 | 1 year | 62 | 15M/4F | 5 | 56 | 73 (Zr) | External hexagon | Southern Implants | 10 Ti/21 Zr | Overdentures |
| Al-Nawas et al. | 2011 | 91 | 1 year | 65.8 | NR | 21 | 70 | 70 (TZ) | Morse-taper | Straumann (Bone Level) | 2 Ti/1 TZ | Overdentures |
| Siddiqi et al. | 2015 | 24 | 1 year | 62 | 15M/4F | 3 | 70 | 80 (Zr) | External hexagon | Southern Implants | 10 Ti/21 Zr | Overdentures |
| Study | Follow-Up | SR Ti (%) | SR Zr/TZ (%) | MBL Ti (mm) | MBL Zr or TZ (mm) | 1 or 2 Pieces | BoP Ti (%) | BoP TZ/Zr (%) | Mucositis | Peri-Implantitis | PD Ti | PD Zr |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Koller et al., 2020 | 80 m | 93.3 | 87.5 (Zr) | −1.17 | −1.38 (Zr) | 2 | 12.6 | 16.4 (Zr) | NR | 1 Ti was removed after 80 m | NR | NR |
| Muller et al., 2015 | 5 y | 92.6 | 95.8 (TZ) | −0.61 | −0.60 (TZ) | 2 | NR | NR | NR | 1 Ti/1 TZ | NR | NR |
| Ioannidis et al., 2015 | 3 y | 97.3 | 98.7 (TZ) | −0.31 | −0.40 (TZ) | 2 | 20 | 13.8 (TZ) | 10 Ti/8 TZ | 2 TZ | 2.9 mm | 2.6 mm |
| Tolentino et al., 2015 | 1 y | 100 | 100 (TZ) | −0.35 | −0.32 (TZ) | NR | 10 | 10 (TZ) | NR | NR | 3.051 mm | 3.1 mm (TZ) |
| Osman et al., 2013 | 1 y | 95.8 | 90.9 (Zr) | −0.18 | −0.42 (Zr) | 1 | NR | NR | NR | NR | NR | NR |
| Al-Nawas et al., 2011 | 1 y | 97.8 | 98.9 (TZ) | −0.31 | −0.34 (ZT) | NR | 94.5 | 97.7 (TZ) | NR | 1 Ti/1 TZ | NR | NR |
| Siddiqi et al., 2013 | 1 y | 98.6 | 91.2 (Zr) | −0.125 | −0.25 (Zr) | 1 | NR | NR | 0 | 0 | 1.6 mm | 2.2 mm |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, P.R.E.; Otero, A.I.P.; Fernandes, J.C.H.; Nassani, L.M.; Castilho, R.M.; de Oliveira Fernandes, G.V. Clinical Performance Comparing Titanium and Titanium–Zirconium or Zirconia Dental Implants: A Systematic Review of Randomized Controlled Trials. Dent. J. 2022, 10, 83. https://doi.org/10.3390/dj10050083
Fernandes PRE, Otero AIP, Fernandes JCH, Nassani LM, Castilho RM, de Oliveira Fernandes GV. Clinical Performance Comparing Titanium and Titanium–Zirconium or Zirconia Dental Implants: A Systematic Review of Randomized Controlled Trials. Dentistry Journal. 2022; 10(5):83. https://doi.org/10.3390/dj10050083
Chicago/Turabian StyleFernandes, Paulo Rafael Esteves, Ada Isis Pelaez Otero, Juliana Campos Hasse Fernandes, Leonardo Mohamad Nassani, Rogerio Moraes Castilho, and Gustavo Vicentis de Oliveira Fernandes. 2022. "Clinical Performance Comparing Titanium and Titanium–Zirconium or Zirconia Dental Implants: A Systematic Review of Randomized Controlled Trials" Dentistry Journal 10, no. 5: 83. https://doi.org/10.3390/dj10050083
APA StyleFernandes, P. R. E., Otero, A. I. P., Fernandes, J. C. H., Nassani, L. M., Castilho, R. M., & de Oliveira Fernandes, G. V. (2022). Clinical Performance Comparing Titanium and Titanium–Zirconium or Zirconia Dental Implants: A Systematic Review of Randomized Controlled Trials. Dentistry Journal, 10(5), 83. https://doi.org/10.3390/dj10050083