
Root Fractures in the Primary Teeth and Their Management: A Scoping Review

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Questions
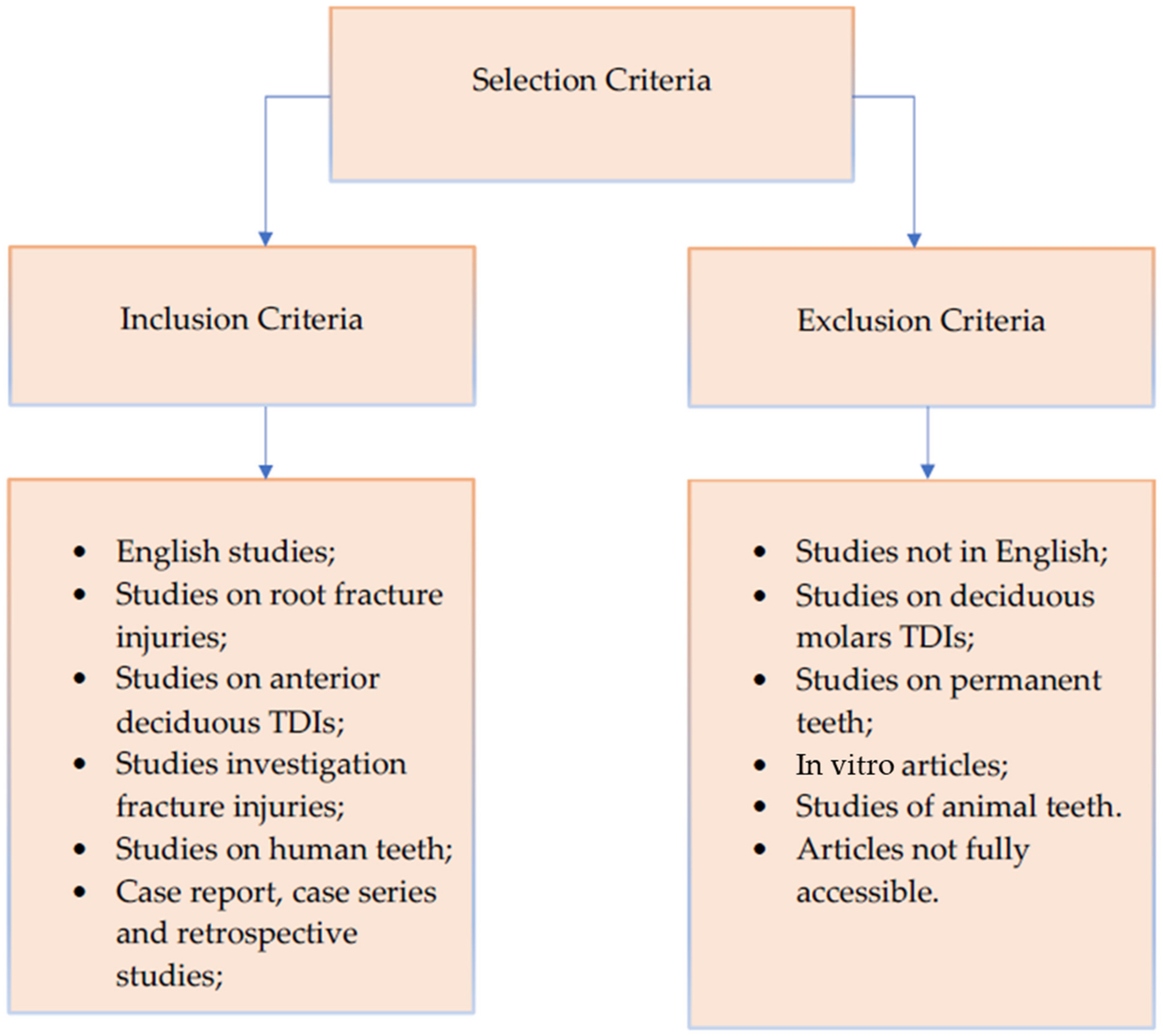
2.2. Selection Criteria
2.3. Search Strategy
2.4. Study Quality Assessment
2.5. Data Extraction
3. Results
3.1. General Data of the Selected Patients
3.2. Type of Root Fracture
3.3. Further Trauma and/or Dislocation Suffered
3.4. Time to Treatment
3.5. Intraoral Diagnostic Tests Performed
3.6. Treatment
3.7. Follow-Up
4. Discussion
- The root fracture of primary teeth is a rare injury predominantly found in the upper incisors of children aged 3 to 4 which, if not managed properly, can cause numerous complications, including premature tooth loss and altered eruption of the permanent teeth, as well as possible psychological repercussions.
- During the first diagnostic check, we would emphasize the need for greater attention to the interpretation of the radiographic images regarding the early resorption of the apical root, which generally should be interpreted as a physiological response.
- Regarding treatment, repositioning and splinting of the coronal fragment does not damage the permanent germ [42]. As explained above, this occurs because the apical fragment remains in the same position. So, the conservative treatment of the root fractures of primary teeth is highly beneficial. Tooth repositioning and semi-rigid splinting therapy could be conservative methods to avoid extraction in pediatric patients.
- Manual repositioning of the dislocated coronal fragment and subsequent splinting immediately after the trauma gave positive long-term results. The use of orthodontic splinting techniques is poorly described in the literature, but this could be a useful method when manual tooth repositioning is difficult and should therefore be further investigated.
- PCO of the crown of tooth affected by the root fracture is frequent and should not be understood as a pathological phenomenon. This response from the dental pulp is often underestimated, or not properly investigated in clinical studies.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holan, G.; Needleman, H.L. Premature loss of primary anterior teeth due to trauma—Potential short- and long-term sequelae. Dent. Traumatol. 2014, 30, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Kramer, P.F.; Feldens, C.A.; Ferreira, S.H.; Bervian, J.; Rodrigues, P.H.; Peres, M.A. Exploring the impact of oral diseases and disorders on quality of life of preschool children. Community Dent. Oral Epidemiol. 2013, 41, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Viegas, C.M.; Paiva, S.M.; Carvalho, A.C.; Scarpelli, A.C.; Ferreira, F.M.; Pordeus, I.A. Influence of traumatic dental injury on quality of life of Brazilian preschool children and their families. Dent. Traumatol. 2014, 30, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Abanto, J.; Tello, G.; Bonini, G.C.; Oliveira, L.B.; Murakami, C.; Bönecker, M. Impact of traumatic dental injuries and malocclusions on quality of life of preschool children: A population-based study. Int. J. Paediatr Dent. 2015, 25, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, M.; de Carvalho Rocha, M.J. Traumatized primary teeth in children assisted at the Federal University of Santa Catarina, Brazil. Dent. Traumatol. 2002, 18, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Bhayya, D.P.; Shyagali, T.R. Traumatic injuries in the primary teeth of 4- to 6-year-old school children in gulbarga city, India. A prevalence study. Oral Health Dent. Manag. 2013, 12, 17–23. [Google Scholar]
- Petti, S.; Glendor, U.; Andersson, L. World traumatic dental injury prevalence and incidence, a meta-analysis-One billion living people have had traumatic dental injuries. Dent. Traumatol. 2018, 34, 71–86. [Google Scholar] [CrossRef]
- Kratunova, E.; Silva, D. Pulp therapy for primary and immature permanent teeth: An overview. Gen. Dent. 2018, 66, 30–38. [Google Scholar]
- Flores, M.T.; Onetto, J.E. How does orofacial trauma in children affect the developing dentition? Long-term treatment and associated complications. Dent. Traumatol. 2019, 35, 312–323. [Google Scholar] [CrossRef]
- Day, P.F.; Flores, M.T.; O’Connell, A.C.; Abbott, P.V.; Tsilingaridis, G.; Fouad, A.F.; Cohenca, N.; Lauridsen, E.; Bourguignon, C.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 3. Injuries in the primary dentition. Dent. Traumatol. 2020, 36, 343–359. [Google Scholar] [CrossRef]
- Feldens, C.A.; Borges, T.S.; Vargas-Ferreira, F.; Kramer, P.F. Risk factors for traumatic dental injuries in the primary dentition: Concepts, interpretation, and evidence. Dent. Traumatol. 2016, 32, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Andreasen, F.M.; Andersson, L. Textbook and Color Atlas of Traumatic Injuries to the Teeth; John Wiley & Sons: Hoboken, NJ, USA, 2019; pp. 34–68. [Google Scholar]
- Borum, M.K.; Andreasen, J.O. Therapeutic and economic implications of traumatic dental injuries in Denmark: An estimate based on 7549 patients treated at a major trauma centre. Int. J. Paediatr. Dent. 2001, 11, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Bonanato, K.; Sardenberg, F.; Santos, E.R.; Ramos-Jorge, M.L.; Zarzar, P.M. Horizontal root fracture with displacement in the primary dentition. Gen. Dent. 2009, 57, e31–e34. [Google Scholar] [PubMed]
- Abbott, P.V. Diagnosis and management of transverse root fractures. Dent. Traumatol. 2019, 35, 333–347. [Google Scholar] [CrossRef] [PubMed]
- Bourguignon, C.; Cohenca, N.; Lauridsen, E.; Flores, M.T.; O’Connell, A.C.; Day, P.F.; Tsilingaridis, G.; Abbott, P.V.; Fouad, A.F.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent. Traumatol. 2020, 36, 314–330. [Google Scholar] [CrossRef]
- Andreasen, F.M.; Andreasen, J.O. Diagnosis of luxation injuries: The importance of standardized clinical, radiographic and photographic techniques in clinical investigations. Endod. Dent. Traumatol. 1985, 1, 160–169. [Google Scholar] [CrossRef]
- Liu, X.; Huang, J.; Bai, Y.; Wang, X.; Baker, A.; Chen, F.; Wu, L.A. Conservation of root-fractured primary teeth—Report of a case. Dent. Traumatol. 2013, 29, 498–501. [Google Scholar] [CrossRef]
- Majorana, A.; Pasini, S.; Bardellini, E.; Keller, E. Clinical and epidemiological study of traumatic root fractures. Dent. Traumatol. 2002, 18, 77–80. [Google Scholar] [CrossRef]
- Borum, M.K.; Andreasen, J.O. Sequelae of trauma to primary maxillary incisors. I. Complications in the primary dentition. Endod. Dent. Traumatol. 1998, 14, 31–44. [Google Scholar] [CrossRef]
- Santos, B.Z.; Cardoso, M.; Almeida, I.C. Pulp canal obliteration following trauma to primary incisors: A 9-year clinical study. Pediatr Dent. 2011, 33, 399–402. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics 1977, 33, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Gadicherla, P.; Devi, M.M. Root fracture in primary teeth. J. Dent. Oro. Facial. Res. 2016, 12, 33–35. [Google Scholar]
- Richa, M.C.; Kumar, N. Management of intra alveolar root fracture in primary incisor: A conservative approach and review of literature. J. Dent. Spec. 2017, 5, 156–160. [Google Scholar]
- Bruzda-Zwiech, A.; Ciesielska, N.; Szczepańska, J. Conservative management of root-fractured primary incisor—Case report. Nowa. Stomatol. 2018, 23, 153–158. [Google Scholar] [CrossRef]
- Di Giorgio, G.; Zumbo, G.; Saccucci, M.; Luzzi, V.; Ierardo, G.; Biagi, R.; Bossù, M. Root Fracture and Extrusive Luxation in Primary Teeth and Their Management: A Case Report. Dent. J. 2021, 9, 107. [Google Scholar] [CrossRef]
- Cho, W.C.; Nam, O.H.; Kim, M.S.; Lee, H.S.; Choi, S.C. A retrospective study of traumatic dental injuries in primary dentition: Treatment outcomes of splinting. Acta Odontol. Scand. 2018, 76, 253–256. [Google Scholar] [CrossRef]
- Flores, M.T. Traumatic injuries in the primary dentition. Dent Traumatol. 2002, 18, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Spinas, E.; Pipi, L.; Mezzena, S.; Giannetti, L. Use of Orthodontic Methods in the Treatment of Dental Luxations: A Scoping Review. Dent. J. 2021, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Andreasen, F.M.; Skeie, A.; Hjørting-Hansen, E.; Schwartz, O. Effect of treatment delay upon pulp and periodontal healing of traumatic dental injuries—A review article. Dent. Traumatol. 2002, 18, 116–128. [Google Scholar] [CrossRef] [PubMed]
- Goswami, M.; Eranhikkal, A. Management of Traumatic Dental Injuries Using Different Types of Splints: A Case Series. Int. J. Clin. Pediatr. Dent. 2020, 13, 199–202. [Google Scholar] [PubMed]
- Spinas, E.; Deias, M.; Mameli, A.; Giannetti, L. Pulp canal obliteration after extrusive and lateral luxation in young permanent teeth: A scoping review. Eur. J. Paediatr. Dent. 2021, 22, 55–60. [Google Scholar]
- Spinas, E.; Melis, A.; Savasta, A. Therapeutic approach to intrusive luxation injuries in primary dentition. A clinical follow-up study. Eur. J. Paediatr. Dent. 2006, 7, 179–186. [Google Scholar]
- Andreasen, F.M.; Andreasen, J.O. Resorption and mineralization processes following root fracture of permanent incisors. Endod. Dent. Traumatol. 1988, 4, 202–214. [Google Scholar] [CrossRef]
- Andreasen, F.M. Transient root resorption after dental trauma: The clinician’s dilemma. J. Esthet. Restor. Dent. 2003, 15, 80–92. [Google Scholar] [CrossRef]
- Nam, O.H.; Kim, M.S.; Kim, G.T.; Choi, S.C. Atypical root resorption following root fractures in primary teeth. Quintessence Int. 2017, 48, 793–797. [Google Scholar]
- Costa, V.P.; Oliveira, L.J.; Rosa, D.P.; Cademartori, M.G.; Torriani, D.D. Crown-Root Fractures in Primary Teeth: A Case Series Study of 28 Cases. Braz. Dent. J. 2016, 27, 234–238. [Google Scholar] [CrossRef][Green Version]
- Cho, J.; Sachs, A.; Cunningham, L.L., Jr. Dental Trauma and Alveolar Fractures. Facial Plast. Surg. Clin. N. Am. 2022, 30, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Cunha, R.F.; Pugliesi, D.M.; de Mello Vieira, A.E. Oral trauma in Brazilian patients aged 0–3 years. Dent. Traumatol. 2001, 17, 210–212. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author and Year | Type of Article | N◦ of Samples | N◦ of Dental Fracture | Traumatized Tooth | Localization of Fracture | Any Other Trauma | Permanent Germs Maturation Stage | Tests Performed | Range Time after the Detected Trauma | Age | Gender | Therapeutic Intervention | Follow-Up | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bonanato et al., 2009 [14] | Case report | 1 | 1 | 61 | AT | Extrusive luxation vestibularly | ns | IPR | 1 day | 3 | F | Repositioning and splint (semi-rigid containment with a 0.5 orthodontic wire affixed with photopolymerizable resin) for 3 weeks | 12 months | Permanence of the apical fragment and reduction in the separation between the root fragments, no discoloration |
| Liu et al., 2013 [18] | Case report | 1 | 2 | 51 61 | AT MD | Grade II mobility Gum bleeding Extrusive Luxation of 1 mm palatally Grade II mobility Gum bleeding | Crown 3/4 complete | IPR | Same day | 3.5 | F | Splint (orthodontic brackets and 0.5 mm stainless steel wire) for 3 months. Repositioning and splint (orthodontic brackets and 0.5 mm stainless steel wire) for 3 months | 2.5 years | After 3 months the root resorption of both apical fragments was almost completed |
| Gadicherla et al., 2016 [27] | Case report | 1 | 1 | 51 | AT | No mobility | Crown 3/4 complete | IPR | 3 days | 3.5 | F | Any treatment | 4 months | No complications |
| Kumari et al., 2017 [28] | Case report | 2 | 1 1 | 51 51 | AT MD | Grade II mobility Grade II mobility | Crown 3/4 complete | IPR | Same day Same day | 4 4 | M M | Splint (semi rigid wire-composite splint) for 2 months. Splint (semi-rigid wire composite) for 4 weeks | 36 months 24 months | Resorption of the apical fragment and apical root after 2.5 years. Resorption of the apical fragment and apical root after 1 year |
| Bruzda-Zwiech et al., 2018 [29] | Case report | 1 | 1 | 61 | AT | Mobility | ns | IPR | Same day | 3 | M | Any treatment | 3.5 years | At the 8-month follow-up there was evidence of healing of the root fracture with calcified tissue, at 3.5 years there was a complete resorption of the apical fragment and of the entire root |
| Di Giorgio et al., 2021 [30] | Case report | 1 | 1 | 51 | AT | Extrusive luxation of 3 mm | ns | IPR | Same day | 3,5 | M | Repositioning and splint (orthodontic flexible splint) for four weeks | 3 years | After 1 year there was pulp canal obliteration and resorption of the apical fragment |
| Cho et al., 2017 [31] | Retrospective study | 38 | 53 | ns | ns | ns | ns | ns | <24 h 14 >24 h 19 | ns | 30 M 8 F | Any treatment: 20 Splinting: 33 | 6 months | Any treatment: failure 14 Splinting: failure 11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinas, E.; Di Giorgio, G.; Murgia, M.S.; Garau, V.; Pinna, M.; Zerman, N. Root Fractures in the Primary Teeth and Their Management: A Scoping Review. Dent. J. 2022, 10, 74. https://doi.org/10.3390/dj10050074
Spinas E, Di Giorgio G, Murgia MS, Garau V, Pinna M, Zerman N. Root Fractures in the Primary Teeth and Their Management: A Scoping Review. Dentistry Journal. 2022; 10(5):74. https://doi.org/10.3390/dj10050074
Chicago/Turabian StyleSpinas, Enrico, Gianni Di Giorgio, Martina Salvatorina Murgia, Valentino Garau, Mara Pinna, and Nicoletta Zerman. 2022. "Root Fractures in the Primary Teeth and Their Management: A Scoping Review" Dentistry Journal 10, no. 5: 74. https://doi.org/10.3390/dj10050074
APA StyleSpinas, E., Di Giorgio, G., Murgia, M. S., Garau, V., Pinna, M., & Zerman, N. (2022). Root Fractures in the Primary Teeth and Their Management: A Scoping Review. Dentistry Journal, 10(5), 74. https://doi.org/10.3390/dj10050074