
Predictability of Invisalign® Clear Aligners Using OrthoPulse®: A Retrospective Study

 ,
,  , , ,
, , ,  ,
,
Abstract

1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mester, A.; Mester, A. The History of Photobiomodulation: Endre Mester (1903–1984). Photomed. Laser Surg. 2017, 35, 393–394. [Google Scholar] [CrossRef]
- Posten, W.; Wrone, D.A.; Dover, J.S.; Arndt, K.A.; Silapunt, S.; Alam, M. Low-level laser therapy for wound healing: Mechanism and efficacy. Derm. Surg. 2005, 31, 334–340. [Google Scholar] [CrossRef]
- Kim, W.S.; Calderhead, R.G. Is light-emitting diode phototherapy (LED-LLLT) really effective? Laser 2011, 20, 205–215. [Google Scholar] [CrossRef]
- Chung, H.; Dai, T.; Sharma, S.K.; Huang, Y.Y.; Carroll, J.D.; Hamblin, M.R. The nuts and bolts of low-level laser (light) therapy. Ann. Biomed. Eng. 2012, 40, 516–533. [Google Scholar] [CrossRef] [PubMed]
- Sommer, A.P.; Pinheiro, A.L.; Mester, A.R.; Franke, R.P.; Whelan, H.T. Biostimulatory windows in low-intensity laser activation: Lasers, scanners, and NASA’s light-emitting diode array system. J. Clin. Laser Med. Surg. 2001, 19, 29–33. [Google Scholar] [CrossRef] [PubMed]
- AlShahrani, I.; Togoo, R.A.; Hosmani, J.; Alhaizaey, A. Photobiomodulation in acceleration of orthodontic tooth movement: A systematic review and meta analysis. Complement. Med. 2019, 47, 102220. [Google Scholar] [CrossRef]
- Kamal, A.; Salman, B.; Ar, N.H.; Samsudin, A.R. Management of dry socket with low-level laser therapy. Clin. Oral Investig. 2021, 25, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Pandeshwar, P.; Roa, M.D.; Das, R.; Shastry, S.P.; Kaul, R.; Srinivasreddy, M.B. Photobiomodulation in oral medicine: A review. J. Investig. Clin. Dent. 2016, 7, 114–126. [Google Scholar] [CrossRef]
- Jiang, Q.; Li, J.; Mei, L.; Du, J.; Levrini, L.; Abbate, G.M.; Li, H. Periodontal health during orthodontic treatment with clear aligners and fixed appliances: A meta-analysis. J. Am. Dent. Assoc. 2018, 149, 712–720.e12. [Google Scholar] [CrossRef]
- Levrini, L.; Carganico, A.; Abbate, L. Maxillary expansion with clear aligners in the mixed dentition: A preliminary study with Invisalign(R) First system. Eur. J. Paediatr. Dent. 2021, 22, 125–128. [Google Scholar] [CrossRef]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Robertson, L.; Kaur, H.; Fagundes, N.C.F.; Romanyk, D.; Major, P.; Flores Mir, C. Effectiveness of clear aligner therapy for orthodontic treatment: A systematic review. Orthod. Craniofac. Res. 2020, 23, 133–142. [Google Scholar] [CrossRef]
- Kravitz, N.D.; Kusnoto, B.; BeGole, E.; Obrez, A.; Agran, B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Houle, J.P.; Piedade, L.; Todescan, R., Jr.; Pinheiro, F.H. The predictability of transverse changes with Invisalign. Angle Orthod. 2017, 87, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Sambevski, J.; Papadopoulou, A.K.; Foley, M.; Dalci, K.; Petocz, P.; Darendeliler, M.A.; Dalci, O. Physical properties of root cementum: Part 29. The effects of LED-mediated photobiomodulation on orthodontically induced root resorption and pain: A pilot split-mouth randomized controlled trial. Eur. J. Orthod. 2022, 44, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Almpani, K.; Kantarci, A. Surgical Methods for the Acceleration of the Orthodontic Tooth Movement. Front. Oral. Biol. 2016, 18, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Kacprzak, A.; Strzecki, A. Methods of accelerating orthodontic tooth movement: A review of contemporary literature. Dent. Med. Probl. 2018, 55, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Baek, W.Y.; Byun, I.H.; Yun, I.S.; Kim, J.Y.; Roh, T.S.; Lew, D.H.; Kim, Y.S. The effect of light-emitting diode (590/830 nm)-based low-level laser therapy on posttraumatic edema of facial bone fracture patients. J. Craniomaxillofac. Surg. 2017, 45, 1875–1877. [Google Scholar] [CrossRef] [PubMed]
- Bjordal, J.M.; Johnson, M.I.; Iversen, V.; Aimbire, F.; Lopes-Martins, R.A. Low-level laser therapy in acute pain: A systematic review of possible mechanisms of action and clinical effects in randomized placebo-controlled trials. Photomed. Laser Surg. 2006, 24, 158–168. [Google Scholar] [CrossRef]
- Christie, A.; Jamtvedt, G.; Dahm, K.T.; Moe, R.H.; Haavardsholm, E.A.; Hagen, K.B. Effectiveness of nonpharmacological and nonsurgical interventions for patients with rheumatoid arthritis: An overview of systematic reviews. Phys. Ther. 2007, 87, 1697–1715. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Li, L.; Lin, Z.; Wang, L.; Lin, L.; Li, M.; Zhang, Y.; Yin, Q.; Li, Q.; Xia, H. A New Treatment Modality for Rheumatoid Arthritis: Combined Photothermal and Photodynamic Therapy Using Cu7.2 S4 Nanoparticles. Adv. Heal. Mater. 2018, 7, e1800013. [Google Scholar] [CrossRef]
- Ordahan, B.; Karahan, A.Y. Role of low-level laser therapy added to facial expression exercises in patients with idiopathic facial (Bell’s) palsy. Lasers Med. Sci. 2017, 32, 931–936. [Google Scholar] [CrossRef]
- Genc, G.; Kocadereli, I.; Tasar, F.; Kilinc, K.; El, S.; Sarkarati, B. Effect of low-level laser therapy (LLLT) on orthodontic tooth movement. Lasers Med. Sci. 2013, 28, 41–47. [Google Scholar] [CrossRef]
- Gkantidis, N.; Mistakidis, I.; Kouskoura, T.; Pandis, N. Effectiveness of non-conventional methods for accelerated orthodontic tooth movement: A systematic review and meta-analysis. J. Dent. 2014, 42, 1300–1319. [Google Scholar] [CrossRef]
- Hamblin, M.; Demidova, T. Mechanisms of Low Level Light Therapy; SPIE: San Jose, CA, USA, 2006; Volume 6140. [Google Scholar]
- Nimeri, G.; Kau, C.H.; Abou-Kheir, N.S.; Corona, R. Acceleration of tooth movement during orthodontic treatment--a frontier in orthodontics. Prog. Orthod. 2013, 14, 42. [Google Scholar] [CrossRef]
- Sousa, M.V.; Pinzan, A.; Consolaro, A.; Henriques, J.F.; de Freitas, M.R. Systematic literature review: Influence of low-level laser on orthodontic movement and pain control in humans. Photomed. Laser Surg. 2014, 32, 592–599. [Google Scholar] [CrossRef]
- Vescovi, P.; Meleti, M.; Merigo, E.; Manfredi, M.; Fornaini, C.; Guidotti, R.; Nammour, S. Case series of 589 tooth extractions in patients under bisphosphonates therapy. Proposal of a clinical protocol supported by Nd:YAG low-level laser therapy. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e680–e685. [Google Scholar] [CrossRef]
- Na, S.; TruongVo, T.; Jiang, F.; Joll, J.E.; Guo, Y.; Utreja, A.; Chen, J. Dose analysis of photobiomodulation therapy on osteoblast, osteoclast, and osteocyte. J. Biomed. Opt. 2018, 23, 1–8. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Hayashi, M.; Fujita, S.; Yoshida, T.; Utsunomiya, T.; Yamamoto, H.; Kasai, K. Low-energy laser irradiation facilitates the velocity of tooth movement and the expressions of matrix metalloproteinase-9, cathepsin K, and alpha(v) beta(3) integrin in rats. Eur. J. Orthod. 2010, 32, 131–139. [Google Scholar] [CrossRef]
- Cruz, D.R.; Kohara, E.K.; Ribeiro, M.S.; Wetter, N.U. Effects of low-intensity laser therapy on the orthodontic movement velocity of human teeth: A preliminary study. Lasers Surg. Med. 2004, 35, 117–120. [Google Scholar] [CrossRef]
- Ge, M.K.; He, W.L.; Chen, J.; Wen, C.; Yin, X.; Hu, Z.A.; Liu, Z.P.; Zou, S.J. Efficacy of low-level laser therapy for accelerating tooth movement during orthodontic treatment: A systematic review and meta-analysis. Lasers Med. Sci. 2015, 30, 1609–1618. [Google Scholar] [CrossRef]
- Goulart, C.S.; Nouer, P.R.; Mouramartins, L.; Garbin, I.U.; de Fatima Zanirato Lizarelli, R. Photoradiation and orthodontic movement: Experimental study with canines. Photomed. Laser Surg. 2006, 24, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Kau, C.H.; Kantarci, A.; Shaughnessy, T.; Vachiramon, A.; Santiwong, P.; de la Fuente, A.; Skrenes, D.; Ma, D.; Brawn, P. Photobiomodulation accelerates orthodontic alignment in the early phase of treatment. Prog. Orthod. 2013, 14, 30. [Google Scholar] [CrossRef]
- Nimeri, G.; Kau, C.H.; Corona, R.; Shelly, J. The effect of photobiomodulation on root resorption during orthodontic treatment. Clin. Cosmet. Investig. Dent. 2014, 6, 1–8. [Google Scholar] [CrossRef][Green Version]
- Guray, Y.; Yuksel, A.S. Effect of light-emitting photobiomodulation therapy on the rate of orthodontic tooth movement: A randomized controlled clinical trial. J. Orofac. Orthop. 2022. [Google Scholar] [CrossRef]
- Al-Dboush, R.; Esfahani, A.N.; El-Bialy, T. Impact of photobiomodulation and low-intensity pulsed ultrasound adjunctive interventions on orthodontic treatment duration during clear aligner therapy. Angle Orthod. 2021, 91, 619–625. [Google Scholar] [CrossRef]
- Saccomanno, S.; Saran, S.; Lagana, D.; Mastrapasqua, R.F.; Grippaudo, C. Motivation, Perception, and Behavior of the Adult Orthodontic Patient: A Survey Analysis. Biomed. Res. Int. 2022, 2022, 2754051. [Google Scholar] [CrossRef]
- White, D.W.; Julien, K.C.; Jacob, H.; Campbell, P.M.; Buschang, P.H. Discomfort associated with Invisalign and traditional brackets: A randomized, prospective trial. Angle Orthod. 2017, 87, 801–808. [Google Scholar] [CrossRef]
- Levrini, L.; Tieghi, G.; Bini, V. Invisalign ClinCheck and the Aesthetic Digital Smile Design Protocol. J. Clin. Orthod. 2015, 49, 518–524. [Google Scholar]
- Haouili, N.; Kravitz, N.D.; Vaid, N.R.; Ferguson, D.J.; Makki, L. Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 420–425. [Google Scholar] [CrossRef]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Treatment outcome and efficacy of an aligner technique--regarding incisor torque, premolar derotation and molar distalization. BMC Oral. Health 2014, 14, 68. [Google Scholar] [CrossRef]
- Scribante, A.; Gallo, S.; Bertino, K.; Meles, S.; Gandini, P.; Sfondrini, M.F. The Effect of Chairside Verbal Instructions Matched with Instagram Social Media on Oral Hygiene of Young Orthodontic Patients: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 706. [Google Scholar] [CrossRef]
- Imani, M.M.; Golshah, A.; Safari-Faramani, R.; Sadeghi, M. Effect of Low-level Laser Therapy on Orthodontic Movement of Human Canine: A Systematic Review and Meta-analysis of Randomized Clinical Trials. Acta Inf. Med. 2018, 26, 139–143. [Google Scholar] [CrossRef]
- Torri, S.; Weber, J.B. Influence of low-level laser therapy on the rate of orthodontic movement: A literature review. Photomed. Laser Surg. 2013, 31, 411–421. [Google Scholar] [CrossRef]
- Carroll, J.D.; Milward, M.R.; Cooper, P.R.; Hadis, M.; Palin, W.M. Developments in low level light therapy (LLLT) for dentistry. Dent. Mater. 2014, 30, 465–475. [Google Scholar] [CrossRef]
- Seifi, M.; Shafeei, H.A.; Daneshdoost, S.; Mir, M. Effects of two types of low-level laser wave lengths (850 and 630 nm) on the orthodontic tooth movements in rabbits. Lasers Med. Sci. 2007, 22, 261–264. [Google Scholar] [CrossRef]
- Yang, H.; Liu, J.; Yang, K. Comparative Study of 660 and 830 nm Photobiomodulation in Promoting Orthodontic Tooth Movement. Photobiomodul. Photomed. Laser Surg. 2019, 37, 349–355. [Google Scholar] [CrossRef]
- Al-Shafi, S.; Pandis, N.; Darendeliler, M.A.; Papadopoulou, A.K. Effect of light-emitting diode-mediated photobiomodulation on extraction space closure in adolescents and young adults: A split-mouth, randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 19–28. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
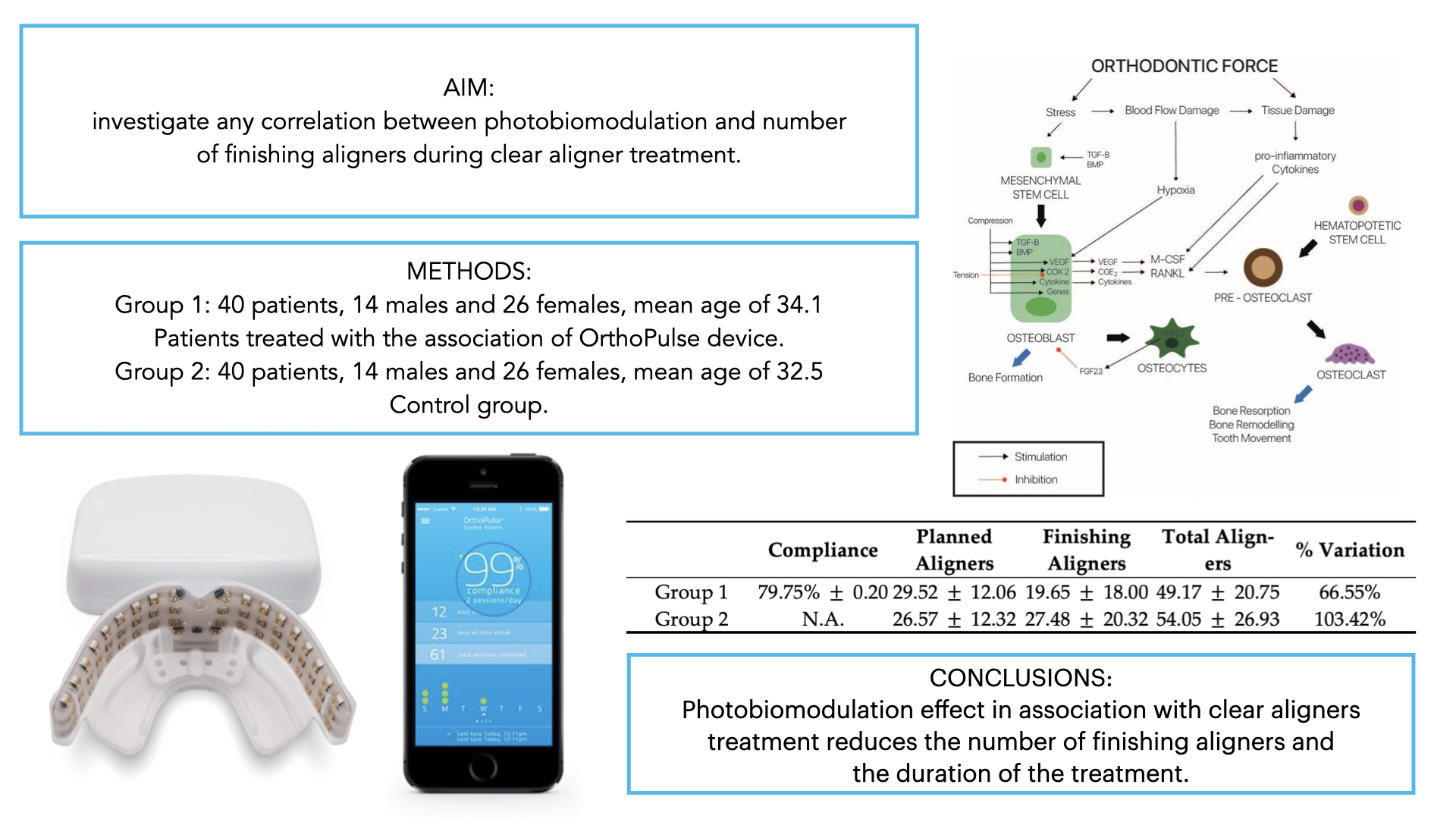
| Compliance | Planned Aligners | Finishing Aligners | Total Aligners | % Variation | |
|---|---|---|---|---|---|
| Group 1 | 79.75% ± 0.20 | 29.52 ± 12.06 | 19.65 ± 18.00 | 49.17 ± 20.75 | 66.55% |
| Group 2 | N.A. | 26.57 ± 12.32 | 27.48 ± 20.32 | 54.05 ± 26.93 | 103.42% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levrini, L.; Carganico, A.; Deppieri, A.; Saran, S.; Bocchieri, S.; Zecca, P.A.; Bertini, S.; D’Apote, A.; Segù, M. Predictability of Invisalign® Clear Aligners Using OrthoPulse®: A Retrospective Study. Dent. J. 2022, 10, 229. https://doi.org/10.3390/dj10120229
Levrini L, Carganico A, Deppieri A, Saran S, Bocchieri S, Zecca PA, Bertini S, D’Apote A, Segù M. Predictability of Invisalign® Clear Aligners Using OrthoPulse®: A Retrospective Study. Dentistry Journal. 2022; 10(12):229. https://doi.org/10.3390/dj10120229
Chicago/Turabian StyleLevrini, Luca, Andrea Carganico, Alessandro Deppieri, Stefano Saran, Salvatore Bocchieri, Piero Antonio Zecca, Sara Bertini, Anna D’Apote, and Marzia Segù. 2022. "Predictability of Invisalign® Clear Aligners Using OrthoPulse®: A Retrospective Study" Dentistry Journal 10, no. 12: 229. https://doi.org/10.3390/dj10120229
APA StyleLevrini, L., Carganico, A., Deppieri, A., Saran, S., Bocchieri, S., Zecca, P. A., Bertini, S., D’Apote, A., & Segù, M. (2022). Predictability of Invisalign® Clear Aligners Using OrthoPulse®: A Retrospective Study. Dentistry Journal, 10(12), 229. https://doi.org/10.3390/dj10120229