
Comparing Distal-Jet with Dental Anchorage to Distal-Jet with Skeletal Anchorage: A Prospective Parallel Cohort Study





Abstract
:1. Introduction
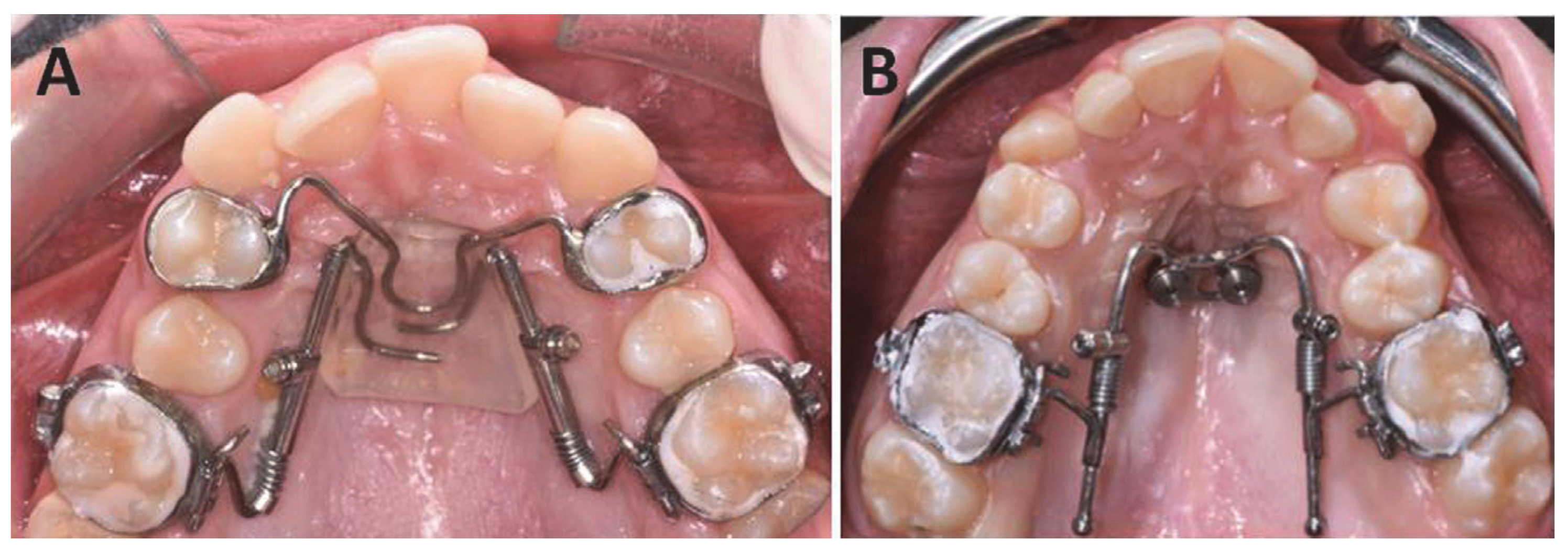
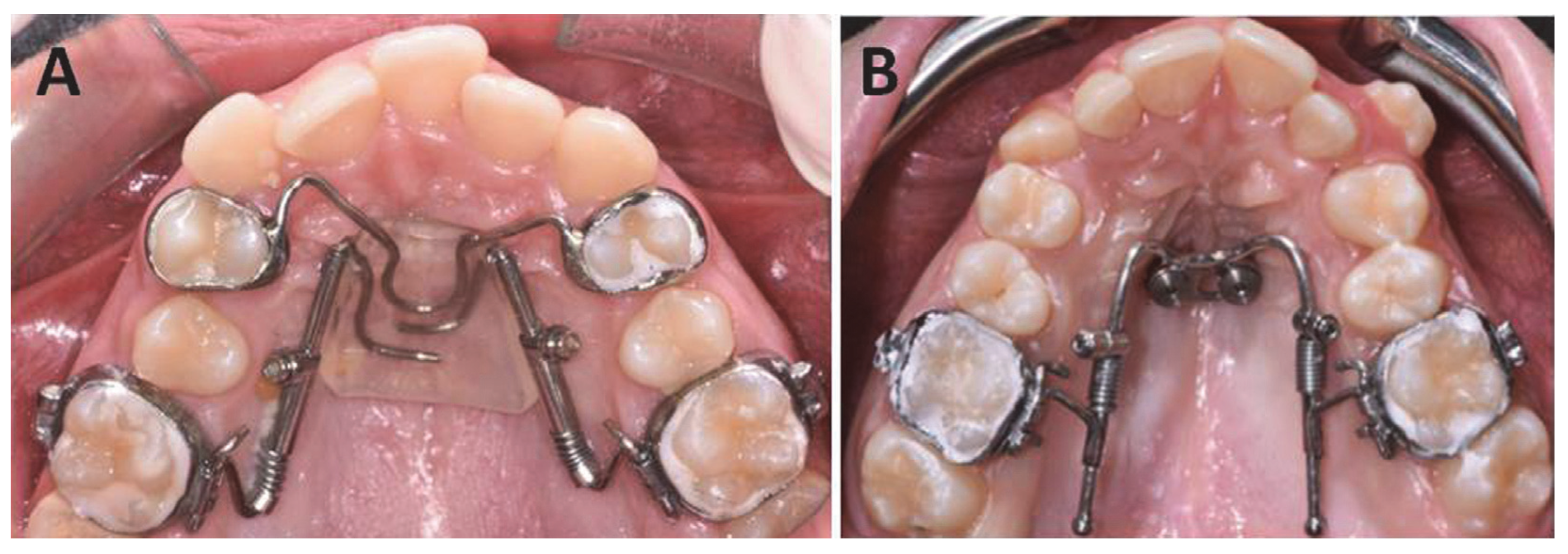
- − a traditional distal-jet appliance;
- − a miniscrew-supported distal-jet appliance.
2. Materials and Methods
- Adolescents with late mixed dentition or permanent dentition;
- Good oral hygiene with the absence of plaque or calculus;
- Bilateral dental Class II malocclusion with mesial migration of the maxillary posterior teeth;
- No adequate space for the correct eruption of one or both maxillary canines;
- Absence of previous orthodontic treatment;
- No systemic syndrome involved.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Moghrabi, D.; Salazar, F.C.; Pandis, N.; Fleming, P.S. Compliance with removable orthodontic appliances and adjuncts: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Bussick, T.J.; McNamara, J.A. Dentoalveolar and skeletal changes associated with the pendulum appliance. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 333–343. [Google Scholar] [CrossRef]
- Baccetti, T.; Franchi, L.; Mc Namara, J.A.; Tollaro, I. Early dentofacial features in Class II malocclusion: A longitudinal study from the deciduous through the mixed dentition. Am. J. Orthod. Dentofac. Orthop. 1997, 111, 502–509. [Google Scholar] [CrossRef]
- Carano, A.; Testa, M. The distal jet for upper molar distalization. J. Clin. Orthod. 1996, 30, 374–380. [Google Scholar]
- Fudalej, P.; Antoszewska, J. Are orthodontic distalizers reinforced with the temporary skeletal anchorage devices effective? Am. J. Orthod. Dentofac. Orthop. 2011, 139, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Brandetti, G.; Altieri, F. Miniscrew-supported distal jet versus conventional distal jet appliance: A pilot study. J. Clin. Exp. Dent. 2019, 11, e650–e658. [Google Scholar] [CrossRef]
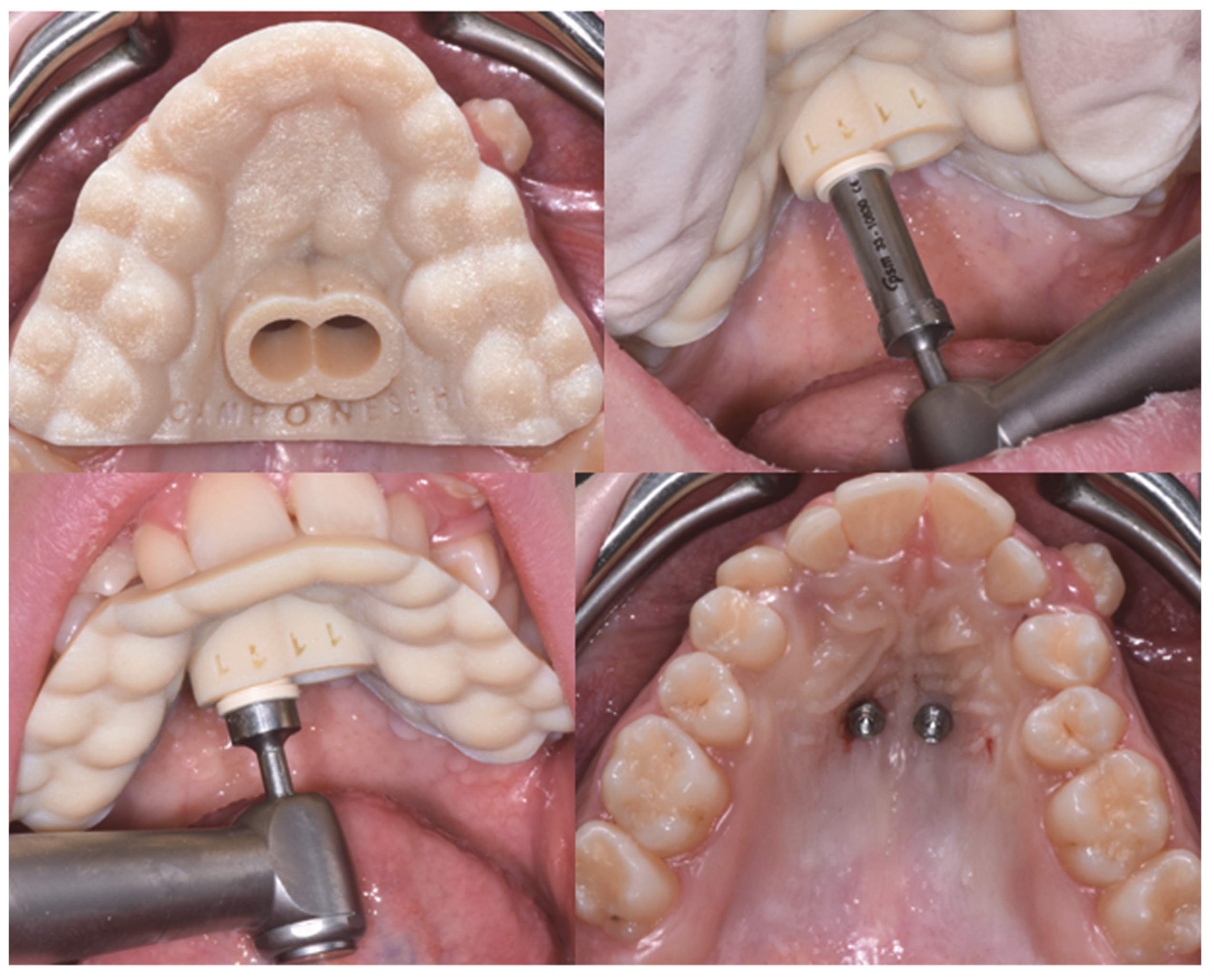
- Altieri, F.; Padalino, G.; Guarnieri, R.; Barbato, E.; Cassetta, M. Computer-guided palatal canine disimpaction: A technical note. Int. J. Comput. Dent. 2020, 23, 219–224. [Google Scholar]
- Thurzo, A.; Kočiš, F.; Novák, B.; Czako, L.; Varga, I. Three-Dimensional Modeling and 3D Printing of Biocompatible Orthodontic Power-Arm Design with Clinical Application. Appl. Sci. 2021, 11, 9693. [Google Scholar] [CrossRef]
- Haas, S.E.; Cisneros, G.J. The Goshgarian transpalatal bar: A clinical and an experimental investigation. Semin. Orthod. 2000, 6, 98–105. [Google Scholar] [CrossRef]
- Hoggan, B.R.; Sadowsky, C. The use of palatal rugae for the assessment of anteroposterior tooth movements. Am. J. Orthod. Dentofac. Orthop. 2001, 119, 482–488. [Google Scholar] [CrossRef]
- Kinzinger, G.S.; Gülden, N.; Yildizhan, F.; Diedrich, P.R. Efficiency of a skeletonized distal jet appliance supported by miniscrew anchorage for noncompliance maxillary molar distalization. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Kinzinger, G.S.M.; Fritz, U.B.; Sander, F.G.; Diedrich, P.R. Efficiency of a pendulum appliance for molar distalization related to second and third molar eruption stage. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 8–23. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, D.; Riboli, F.; Gibelli, D.; Cappella, A.; Cattaneo, C. Palatal rugae as an individualising marker: Reliability for forensic odontology and personal identification. Sci. Justice 2012, 52, 181–184. [Google Scholar] [CrossRef]
- Bolla, E.; Muratore, F.; Carano, A.; Bowman, S.J. Evaluation of maxillary molar distalization with the distal jet: A comparison with other contemporary methods. Angle Orthod. 2002, 72, 481–494. [Google Scholar] [PubMed]
- Ngantung, V.; Nanda, R.S.; Bowman, S.J. Posttreatment evaluation of the distal jet appliance. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Cozzani, M.; Pasini, M.; Zallio, F.; Ritucci, R.; Mutinelli, S.; Mazzotta, L.; Giuca, M.R.; Piras, V. Comparison of maxillary molar distalization with an implant-supported distal jet and a traditional tooth-supported distal jet appliance. Int. J. Dent. 2014, 2014, 937059. [Google Scholar] [CrossRef]
- Escobar, S.A.; Tellez, P.A.; Moncada, C.A.; Villegas, C.A.; Latorre, C.M.; Oberti, G. Distalization of maxillary molars with the bone-supported pendulum: A clinical study. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 545–549. [Google Scholar] [CrossRef]
- Gelgor, E.; Karaman, A.I.; Buyukyilmaz, T. Comparison of 2 distalization systems supported by intraosseous screws. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 161.e1–161.e8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
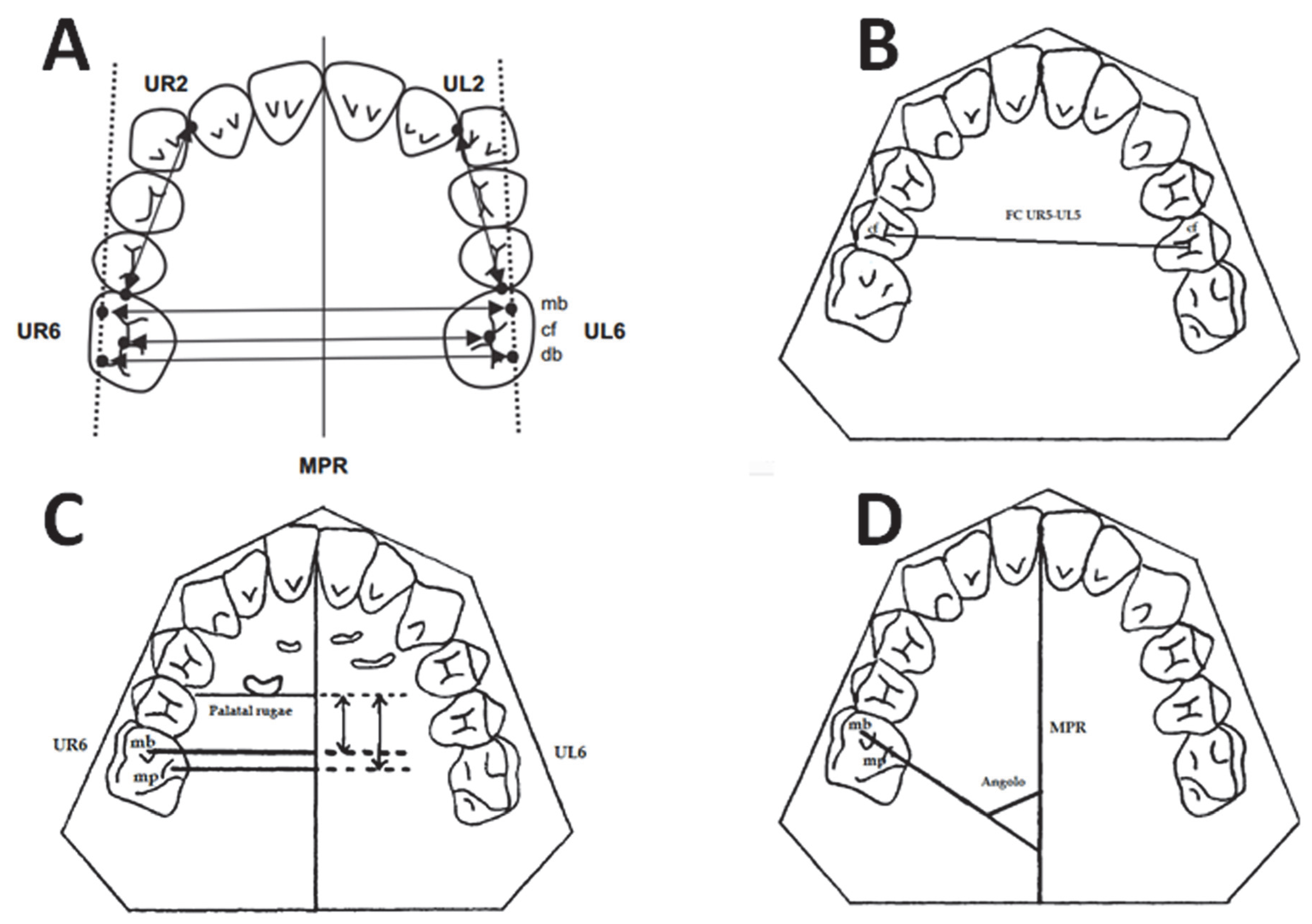
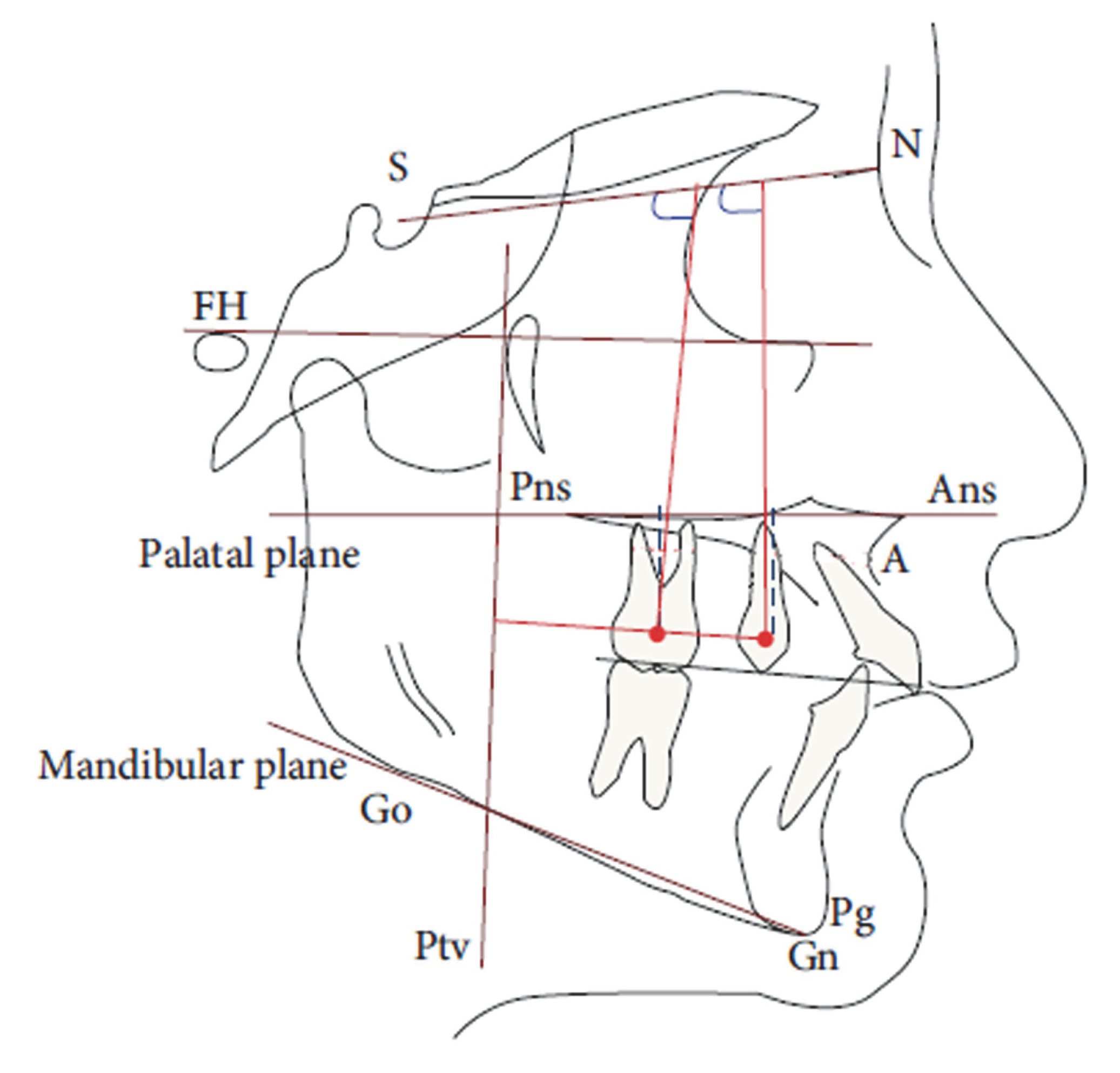
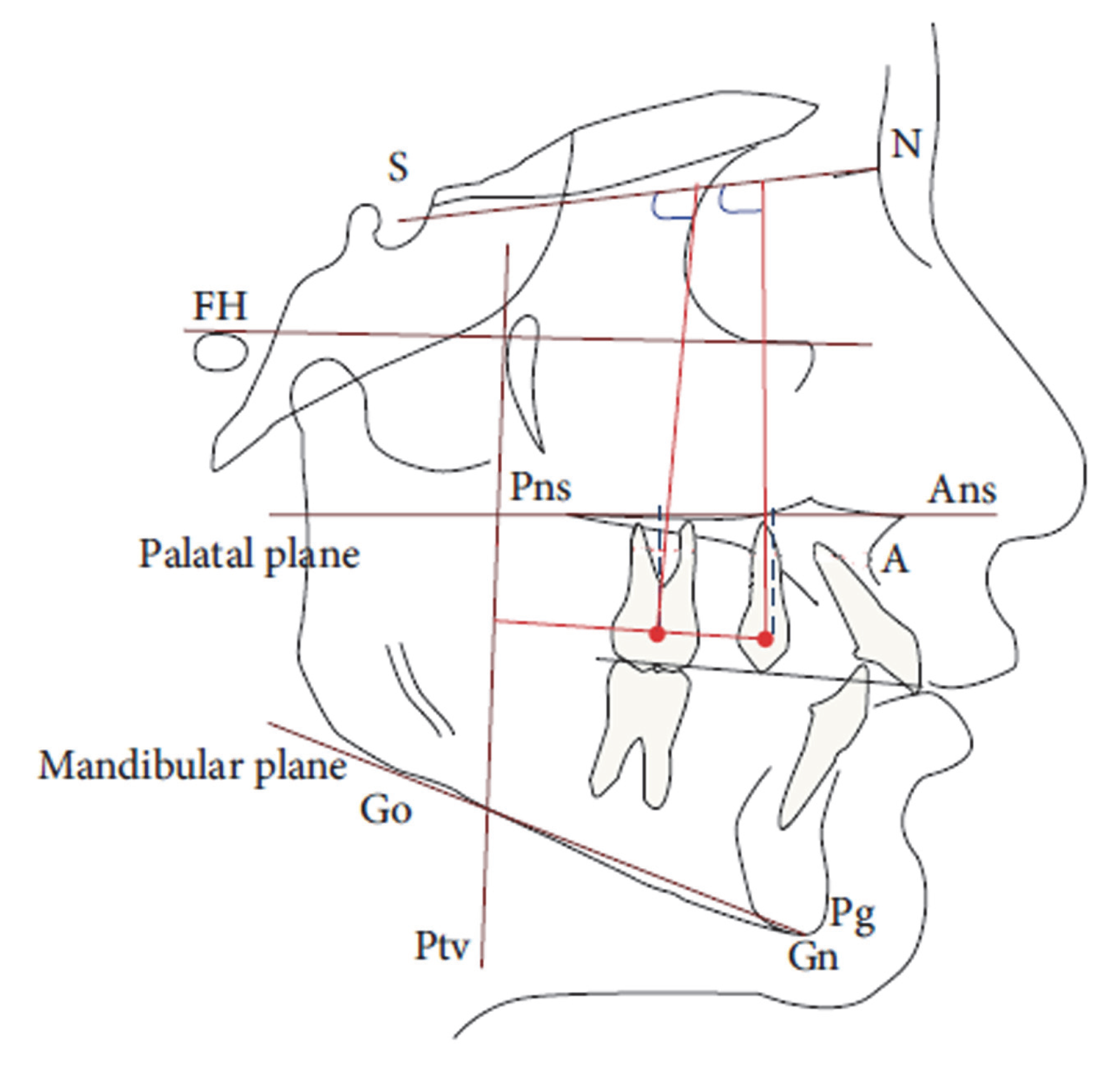
| Cephalometric Variables | Description |
|---|---|
| PTV-U6 (mm) | Horizontal measurement from the PTV line to the maxillary first molar. |
| PTV-U4 (mm) | Horizontal measurement from the palatal plane to the maxillary first premolar. |
| PP-U6 (mm) | Vertical measurement from the palatal plane to the maxillary first molar. |
| PP-U4 (mm) | Vertical measurement from the palatal plane to the maxillary first premolar. |
| SN ^ U6 (degrees °) | Angle formed by the intersection of the axis of the first upper molar and the Sella-Nasion plane. |
| SN ^ U4 (degrees °) | Angle formed by the intersection of the axis of the first upper premolar and the Sella-Nasion plane |
| PP ^ U1 (degrees °) | Angle between the upper central incisor and the palatal plane |
| SN ^ U1 (degrees °) | Angle between the upper central incisor and the anterior cranial base |
| 1 ^ 1 (degrees °) | Interincisive angle |
| ANB (degrees °) | Angle used for the evaluation of the skeletal class in the sagittal plane |
| FMA (degrees °) | Angle between the Frankfurt plane and the Gonion-Menton plane |
| PP ^ Go-Me (degrees °) | Angle between the palatal plane and the mandibular plane |
| SN ^ Go-Me (degrees °) | Angle between the anterior cranial base and the mandibular plane |
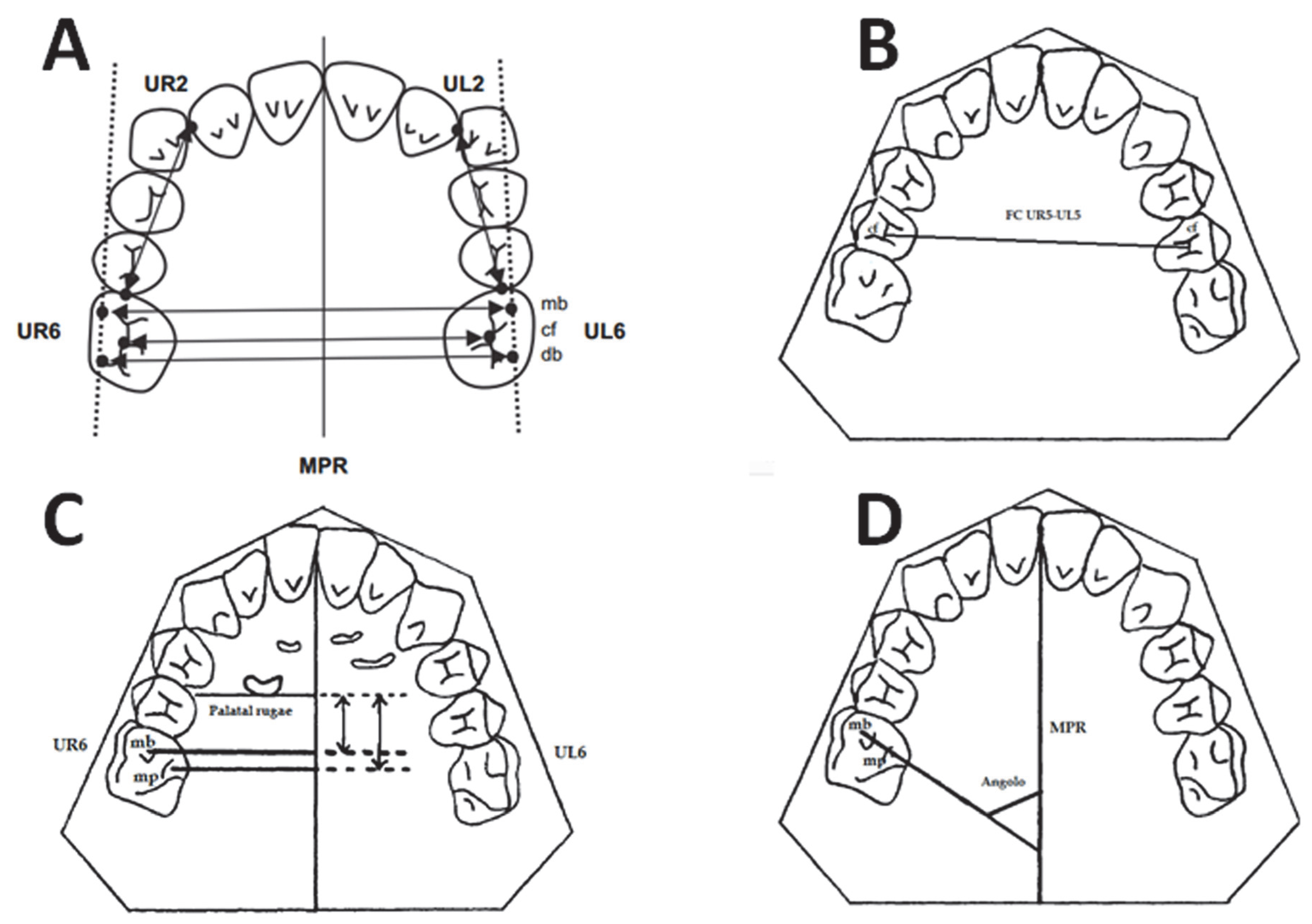
| Variable | T1−T0 Group A | T1−T0 Group A SD | T1−T0 Group B | T1−T0 Group B SD | Significance | Mean Difference (95% CI) |
|---|---|---|---|---|---|---|
| UR2-UR6 | 4.2 | 1.7 | 3.7 | 2.7 | NS | 0.50 (−1.44 to 2.44) |
| UL2-UL6 | 2.9 | 2.2 | 4 | 2.3 | NS | −1.08 (−3.17 to 1.01) |
| MB UR6-UL6 | 1.9 | 2.4 | 3.2 | 1.3 | NS | −1.25 (−3.16 to 0.66) |
| CF UR6-UL6 | 1.9 | 1.9 | 3.7 | 2.0 | * | −1.77 (−3.53 to −0.02) |
| DB UR6-UL6 | 3 | 3.4 | 3.8 | 1.4 | NS | −0.76 (−3.42 to 1.90) |
| UR6 ROTATION | 1.5 | 6.7 | −2.7 | 5.1 | NS | 4.25 (−1.50 to 10.00) |
| UL6 ROTATION | −0.3 | 7.4 | −1.6 | 6.0 | NS | 1.23 (−5.18 to 7.65) |
| CF UR5-UL5 | 1.4 | 1.9 | 2.7 | 2.9 | NS | −1.17 (−3.01 to 0.67) |
| LINE AR | 4.3 | 2.8 | 1.5 | 3.1 | * | 2.85 (0.17 to 5.52) |
| LINE AL | 4.1 | 2.8 | 3.1 | 3.3 | NS | 0.95 (−1.81 to 3.71) |
| LINE BR | 3.8 | 2.8 | 1.0 | 2.4 | * | 2.87 (0.41 to 5.3) |
| LINE BL | 3.6 | 2.5 | 2.5 | 2.7 | NS | 1.03 (−1.37 to 3.42) |
| Variable | T1−T0 Group A | T1−T0 Group A SD | T1−T0 Group B | T1−T0 Group B SD | Significance | Mean Difference (95% CI) |
|---|---|---|---|---|---|---|
| PTV-U6 mm | −3.9 | 1.2 | −2.2 | 1.5 | * | −1.72 (−2.91 to −0.53) |
| PTV-U4 mm | −2.2 | 1.5 | 2.2 | 1.9 | * | −4.45 (−5.98 to −2.92) |
| SN ^ U6 | −0.1 | 3.0 | −2.5 | 6.8 | NS | 2.38 (−1.96 to 6.73) |
| SN ^ U4 | −2.4 | 2.4 | 3.6 | 4.7 | * | −5.98 (−9.10 to −2.87) |
| PP-U6 mm | 0.6 | 3.6 | 0.3 | 1.0 | NS | 0.22 (−2.52 to 2.96) |
| PP-U4 mm | −0.1 | 0.6 | 1.1 | 0.8 | * | −1.19 (−1.82 to −0.56) |
| PP ^ U1 | −3.4 | 2.8 | 5.5 | 4.0 | * | −8.82 (−11.82 to −5.82) |
| SN ^ U1 | −4.9 | 3.9 | 5.3 | 4.6 | * | −10.25 (−14.10 to −6.40) |
| 1 ^ 1 | 3.9 | 4.5 | −5.1 | 6.9 | * | 8.95 (3.90 to 14.00) |
| OVJ | −0.6 | 0.5 | 1.0 | 0.6 | * | −1.55 (−2.02 to −1.07) |
| OVB | −0.2 | 0.9 | −0.9 | 1 | NS | 0.75 (−0.10 to 1.61) |
| ANB | −0.3 | 0.8 | 0.1 | 0.7 | NS | −0.16 (−0.85 to 0.52) |
| FMA | −0.6 | 2.5 | 0.0 | 3.2 | NS | −0.65 (−3.21 to 1.91) |
| PP ^ Go-Me | −0.9 | 2.2 | 0.3 | 2.6 | NS | −1.26 (−3.42 to 0.89) |
| SN ^ Go-Me | −0.4 | 2.1 | 0.1 | 1.8 | NS | −0.50 (−2.37 to 1.38) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altieri, F.; Mezio, M.; Guarnieri, R.; Cassetta, M. Comparing Distal-Jet with Dental Anchorage to Distal-Jet with Skeletal Anchorage: A Prospective Parallel Cohort Study. Dent. J. 2022, 10, 179. https://doi.org/10.3390/dj10100179
Altieri F, Mezio M, Guarnieri R, Cassetta M. Comparing Distal-Jet with Dental Anchorage to Distal-Jet with Skeletal Anchorage: A Prospective Parallel Cohort Study. Dentistry Journal. 2022; 10(10):179. https://doi.org/10.3390/dj10100179
Chicago/Turabian StyleAltieri, Federica, Martina Mezio, Rosanna Guarnieri, and Michele Cassetta. 2022. "Comparing Distal-Jet with Dental Anchorage to Distal-Jet with Skeletal Anchorage: A Prospective Parallel Cohort Study" Dentistry Journal 10, no. 10: 179. https://doi.org/10.3390/dj10100179
APA StyleAltieri, F., Mezio, M., Guarnieri, R., & Cassetta, M. (2022). Comparing Distal-Jet with Dental Anchorage to Distal-Jet with Skeletal Anchorage: A Prospective Parallel Cohort Study. Dentistry Journal, 10(10), 179. https://doi.org/10.3390/dj10100179