
Analysis of Osteoclasts and Root Resorption in Corticotomy-Facilitated Orthodontics with Ibuprofen Administration—An Animal Study


Abstract
:1. Introduction
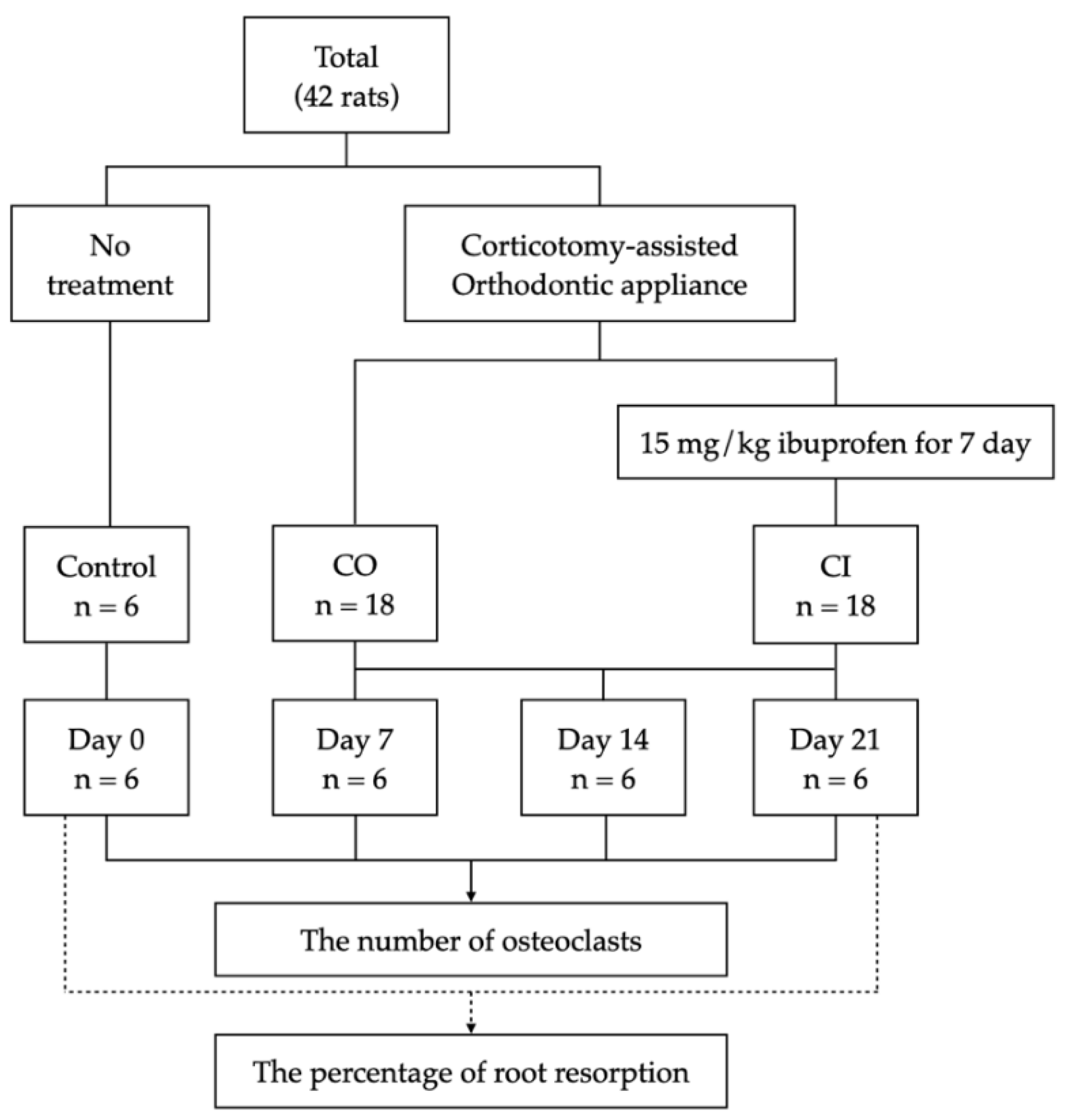
2. Materials and Methods
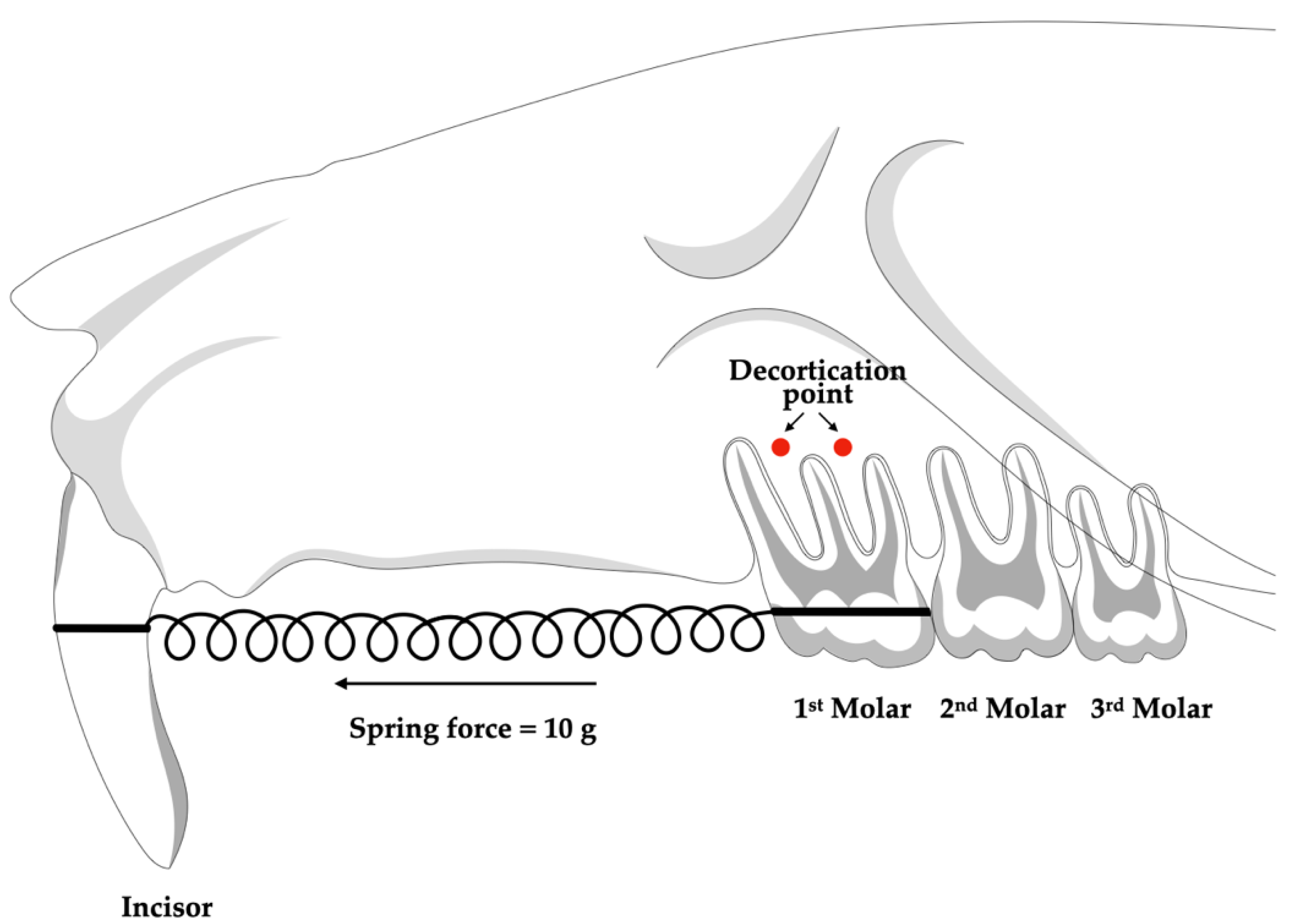
2.1. Alveolar Corticotomy Procedure
2.2. Orthodontic Application Placement
2.3. Administration of Medication
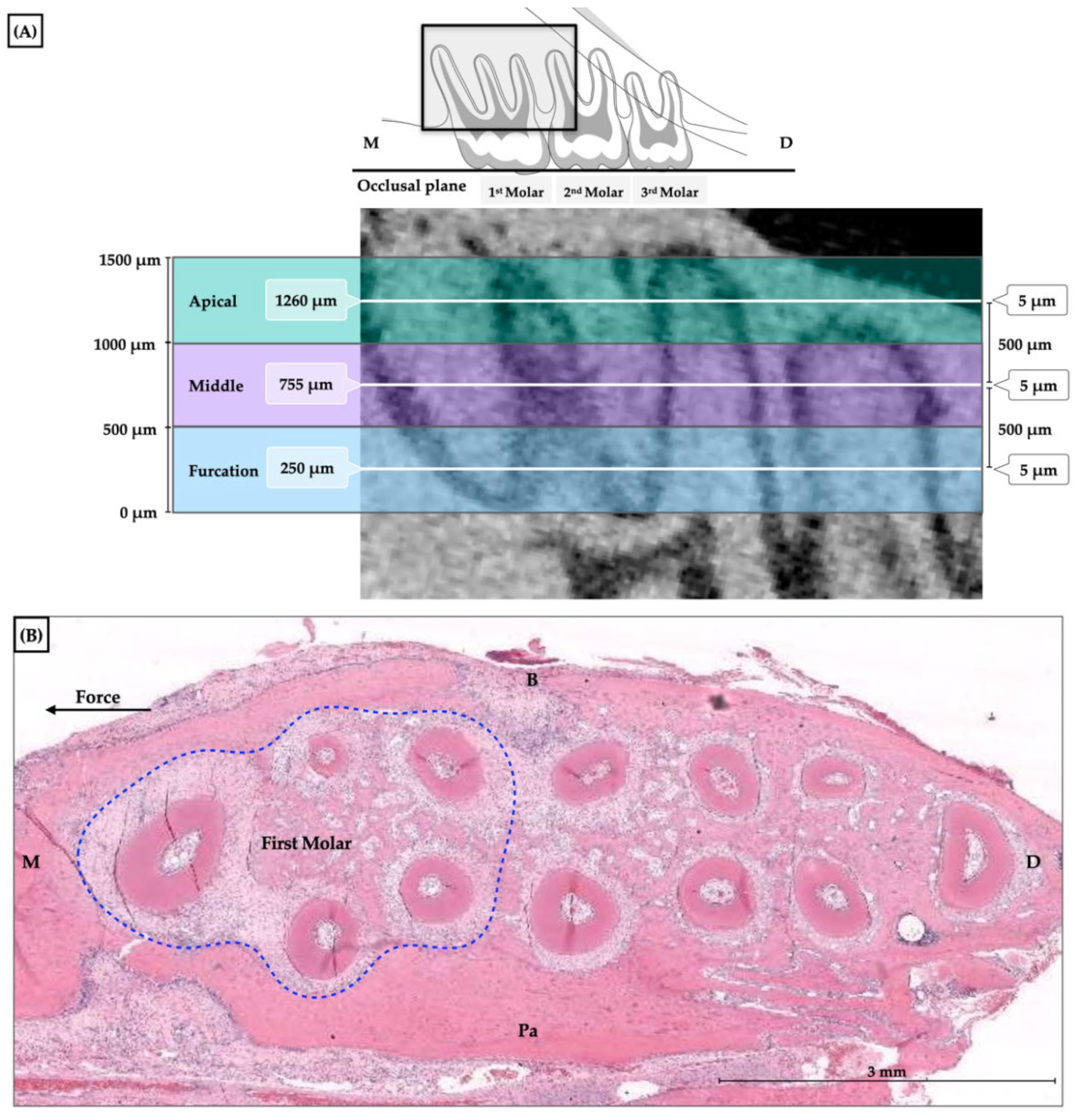
2.4. Histological Approach
2.5. Measurement of Osteoclast Numbers
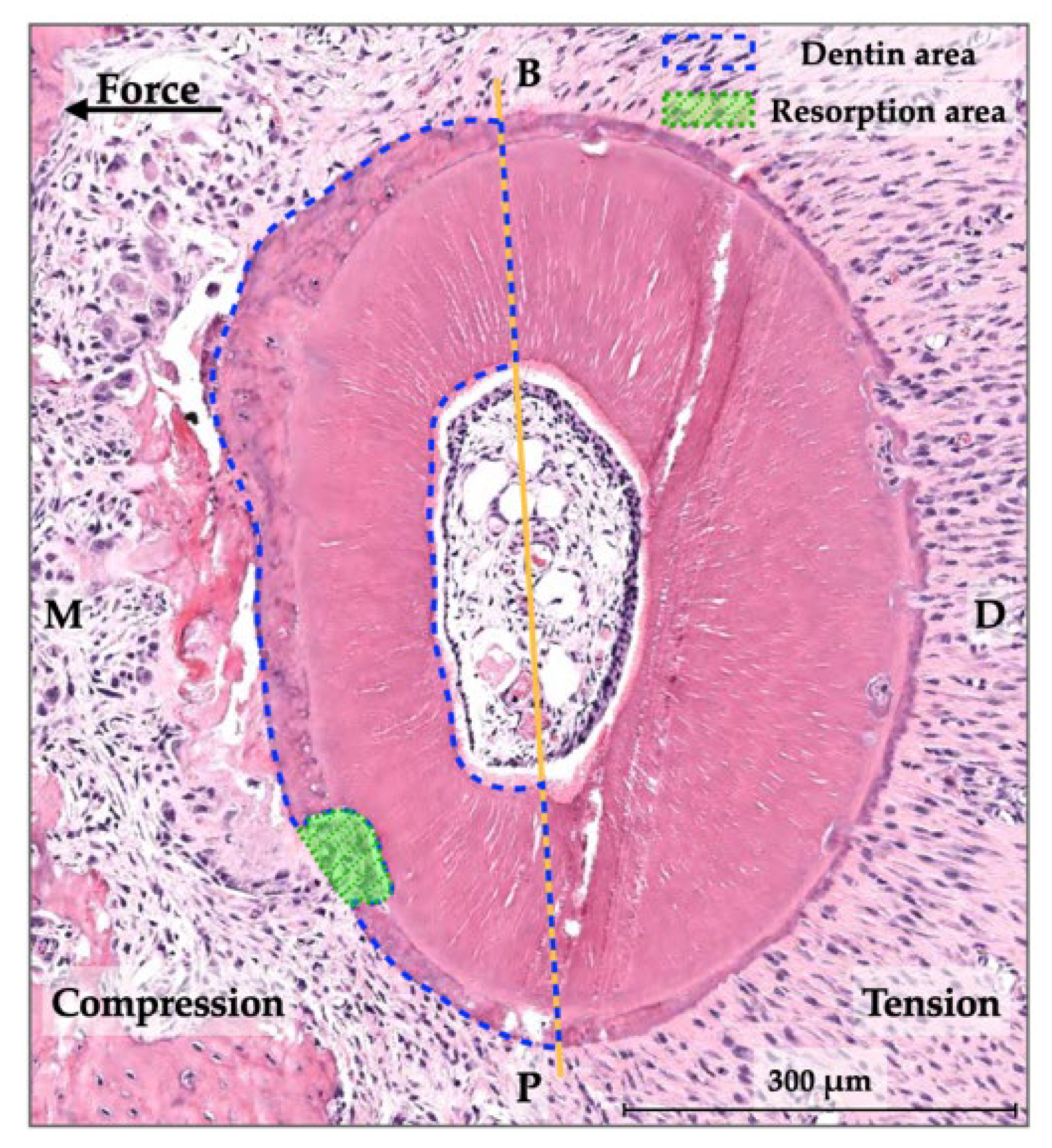
2.6. Measurement of Root Resorption
2.7. Statistical Analysis
3. Results
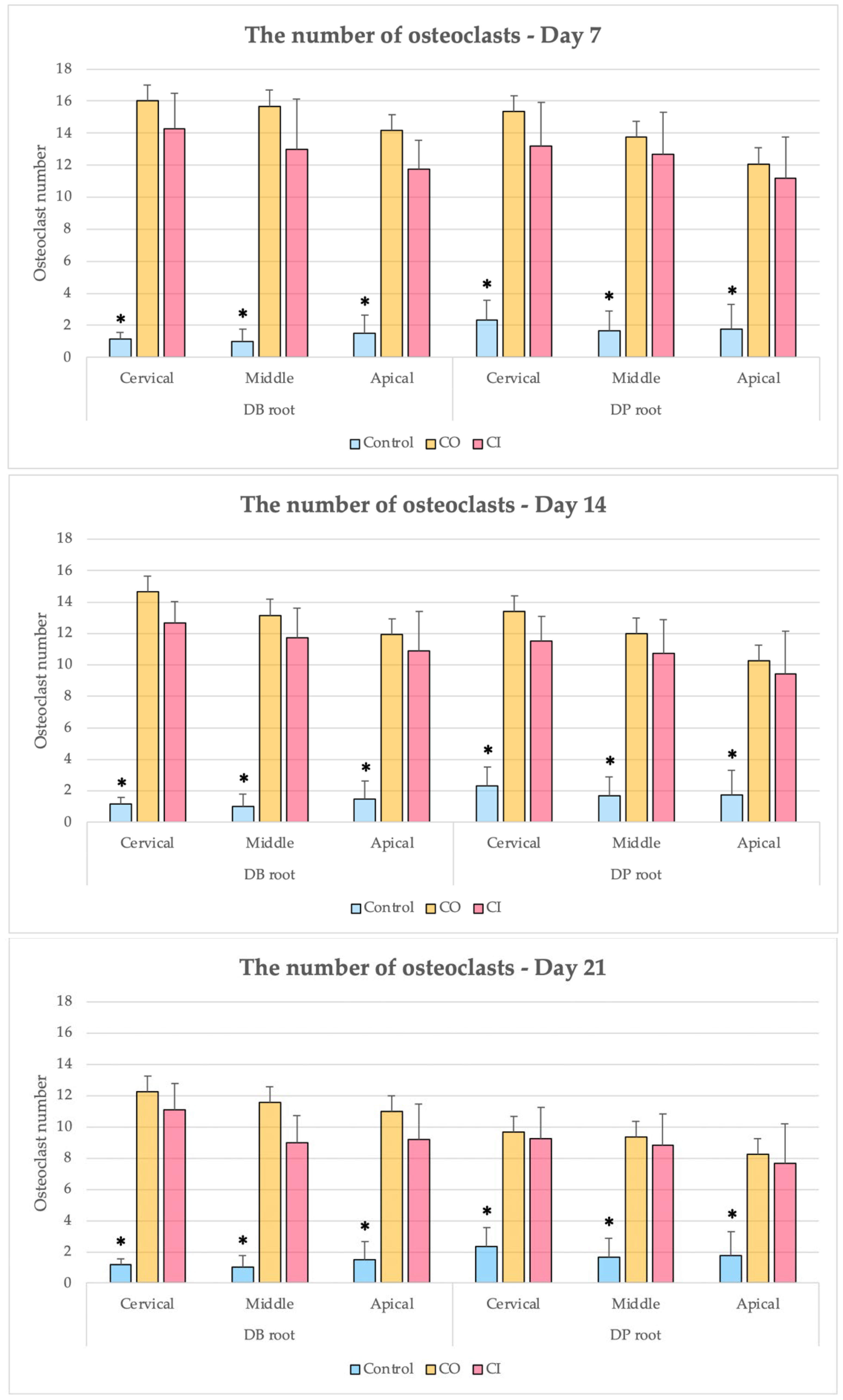
3.1. Numbers of Osteoclasts
3.2. Percentages of Root Resorption
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Talic, N.F. Adverse effects of orthodontic treatment: A clinical perspective. Saudi Dent. J. 2011, 23, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Segal, G.; Schiffman, P.; Tuncay, O. Meta analysis of the treatment-related factors of external apical root resorption. Orthod. Craniofac. Res. 2004, 7, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Pyakurel, U.; Wang, Y.; Liao, L.; Zhou, Y.; Lai, W. Interventions for accelerating orthodontic tooth movement. Angle Orthod. 2013, 83, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Köle, H. Surgical operations on the alveolar ridge to correct occlusal abnormalities. Oral. Surg. Oral. Med. Oral. Pathol. 1959, 12, 515–529. [Google Scholar] [CrossRef]
- Frost, H.M. The regional acceleratory phenomenon: A review. Henry Ford Hosp. Med. J. 1983, 31, 3–9. [Google Scholar]
- Apalimova, A.; Roselló, À.; Jané-Salas, E.; Arranz-Obispo, C.; Marí-Roig, A.; López-López, J. Corticotomy in orthodontic treatment: Systematic review. Heliyon 2020, 6, e04013. [Google Scholar] [CrossRef]
- Al-Naoum, F.; Hajeer, M.Y.; Al-Jundi, A. Does Alveolar Corticotomy Accelerate Orthodontic Tooth Movement When Retracting Upper Canines? A Split-Mouth Design Randomized Controlled Trial. J. Oral Maxillofac. Surg. 2014, 72, 1880–1889. [Google Scholar] [CrossRef]
- Gasparro, R.; Bucci, R.; De Rosa, F.; Sammartino, G.; Bucci, P.; D’Antò, V.; Marenzi, G. Effectiveness of surgical procedures in the acceleration of orthodontic tooth movement: Findings from systematic reviews and meta-analyses. Jpn. Dent. Sci. Rev. 2022, 58, 137–154. [Google Scholar] [CrossRef]
- Cheng, C.; Xie, T.; Wang, J. The efficacy of analgesics in controlling orthodontic pain: A systematic review and meta-analysis. BMC Oral Health 2020, 20, 259. [Google Scholar] [CrossRef]
- Pozzi, A.; Gallelli, L. Pain management for dentists: The role of ibuprofen. Ann. Stomatol. 2011, 2 (Suppl. S3–S4), 3–24. [Google Scholar]
- Kawabata, A. Prostaglandin E2 and Pain-An Update. Biol. Pharm. Bull. 2011, 34, 1170–1173. [Google Scholar] [CrossRef]
- Shetty, N.; Patil, A.K.; Ganeshkar, S.V.; Hegde, S. Comparison of the effects of ibuprofen and acetaminophen on PGE2 levels in the GCF during orthodontic tooth movement: A human study. Prog. Orthod. 2013, 14, 6. [Google Scholar] [CrossRef] [Green Version]
- Kehoe, M.J.; Cohen, S.M.; Zarrinnia, K.; Cowan, A. The effect of acetaminophen, ibuprofen, and misoprostol on prostaglandin E2 synthesis and the degree and rate of orthodontic tooth movement. Angle Orthod. 1996, 66, 339–349. [Google Scholar]
- Arias, O.R.; Marquez-Orozco, M.C. Aspirin, acetaminophen, and ibuprofen: Their effects on orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 364–370. [Google Scholar] [CrossRef]
- Brunson, T.D. Effect of Cyclooxygenase Inhibitors on Rat Root Resorption and Tooth Movement. Master’s Thesis, Faculty of the Graduate School, University of South California, Los Angeles, CA, USA, 2008. [Google Scholar]
- Jindarojanakul, C.; Samruajbenjakun, B. Influence of ibuprofen combined with corticotomy on tooth movement and alveolar bone remodeling in rats. Angle Orthod. 2022; in press. [Google Scholar] [CrossRef]
- Kraiwattanapong, K.; Samruajbenjakun, B. Effects of different force magnitudes on corticotomy-assisted orthodontic tooth movement in rats. Angle Orthod. 2018, 88, 632–637. [Google Scholar] [CrossRef]
- Flecknell, P.A. Analgesia and Post-Operative Care. In Laboratory Animal Anaesthesia, 4th ed.; Flecknell, P.A., Ed.; Elsevier Science: Amsterdam, NY, USA, 2016; pp. 141–192. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Krishnan, V.; Kuijpers-Jagtman, A.M.; Davidovitch, Z. Cellular and molecular biology behind orthodontic tooth movement. In Biological Mechanisms of Tooth Movement, 3rd ed.; Krishnan, V., Davidovitch, Z., Eds.; John Wiley & Sons: West Sussex, UK, 2015; pp. 30–50. [Google Scholar]
- Peron, A.P.L.M.; Johann, A.C.B.R.; Papalexiou, V.; Tanaka, O.M.; Guariza-Filho, O.; Ignácio, S.A.; Camargo, E.S. Tissue responses resulting from tooth movement surgically assisted by corticotomy and corticision in rats. Angle Orthod. 2017, 87, 118–124. [Google Scholar] [CrossRef]
- Schneider, P.P.; Silva, L.P.; Carvalho, F.J.L.C.; Lon, L.F.S.; Gandini Júnior, L.G. Histological evaluation of the effects of corticotomy on induced orthodontic movement in rats. Rev. Odontol. Unesp. 2017, 46, 368–373. [Google Scholar] [CrossRef]
- Iino, S.; Sakoda, S.; Ito, G.; Nishimori, T.; Ikeda, T.; Miyawaki, S. Acceleration of orthodontic tooth movement by alveolar corticotomy in the dog. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 448.e1–448.e8. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, H.; Sun, W.; Wang, S.; Zhang, S.; Zhu, L.; Chen, Y.; Xie, L.; Sun, Z.; Yan, B. Macrophages mediate corticotomy-accelerated orthodontic tooth movement. Sci. Rep. 2018, 8, 16788. [Google Scholar]
- Becker, D.E.; Phero, J.C. Drug Therapy in Dental Practice: Nonopioid and Opioid Analgesics. Anesth. Prog. 2005, 52, 140–149. [Google Scholar] [CrossRef]
- Hargreaves, K.; Abbott, P.V. Drugs for pain management in dentistry. Aust. Dental J. 2005, 50, S14–S22. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Root Resorption (%) | p-Value | ||||
|---|---|---|---|---|---|
| Control | CO | CI | Inter-Group | ||
| DB root | Cervical | 1.78 (1.32) NS | 5.08 (2.94) NS | 2.30 (2.58) NS | 0.065 |
| Middle | 1.78 (2.00) NS | 4.54 (3.27) NS | 3.48 (2.45) NS | 0.219 | |
| Apical | 3.43 (2.94) NS | 2.73 (2.36) NS | 1.32 (1.66) NS | 0.323 | |
| p-value intra-group | 0.350 | 0.361 | 0.286 | ||
| DP root | Cervical | 0.94 (0.56) NS | 2.27 (1.16) NS | 2.13 (1.60) NS | 0.137 |
| Middle | 1.23 (1.02) NS | 3.45 (4.04) NS | 3.31 (2.58) NS | 0.341 | |
| Apical | 3.07 (2.94) NS | 3.10 (2.61) NS | 1.50 (2.04) NS | 0.480 | |
| p-value intra-group | 0.091 | 0.700 | 0.345 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jindarojanakul, C.; Chanmanee, P.; Samruajbenjakun, B. Analysis of Osteoclasts and Root Resorption in Corticotomy-Facilitated Orthodontics with Ibuprofen Administration—An Animal Study. Dent. J. 2022, 10, 170. https://doi.org/10.3390/dj10090170
Jindarojanakul C, Chanmanee P, Samruajbenjakun B. Analysis of Osteoclasts and Root Resorption in Corticotomy-Facilitated Orthodontics with Ibuprofen Administration—An Animal Study. Dentistry Journal. 2022; 10(9):170. https://doi.org/10.3390/dj10090170
Chicago/Turabian StyleJindarojanakul, Chanakant, Pannapat Chanmanee, and Bancha Samruajbenjakun. 2022. "Analysis of Osteoclasts and Root Resorption in Corticotomy-Facilitated Orthodontics with Ibuprofen Administration—An Animal Study" Dentistry Journal 10, no. 9: 170. https://doi.org/10.3390/dj10090170
APA StyleJindarojanakul, C., Chanmanee, P., & Samruajbenjakun, B. (2022). Analysis of Osteoclasts and Root Resorption in Corticotomy-Facilitated Orthodontics with Ibuprofen Administration—An Animal Study. Dentistry Journal, 10(9), 170. https://doi.org/10.3390/dj10090170