
Effects of Multibracket Orthodontic Treatment versus Clear Aligners on Periodontal Health: An Integrative Review

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Population
2.3. Search Strategy
2.4. Study Selection and Eligibility Process
2.5. Data Items
3. Results
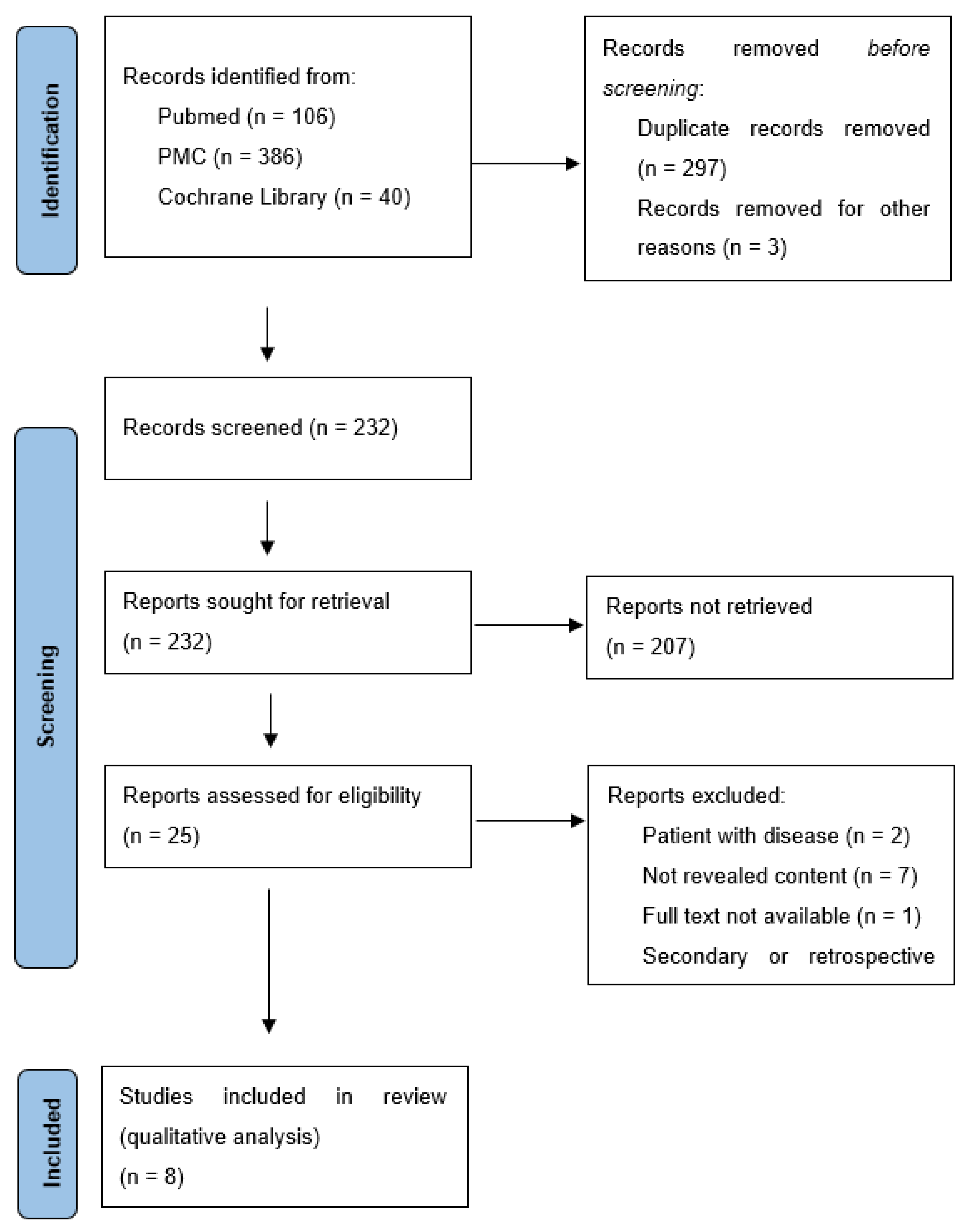
3.1. Search Results
3.2. Introduction of the Selected Studies
3.3. Indexes Comparison
3.4. Studies’ Details
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| AG | Aligners group |
| API | Approximative plaque index |
| BoP | Bleeding of probing |
| CCM | Conventional ceramic brackets |
| ELB | Elastomeric-ligated brackets |
| FG | Fixed group |
| FMBS | Full mouth bleeding score |
| FMPS | Full mouth plaque score |
| GI | Gingival index |
| MPI | Modified plaque index |
| PBE | Periodontal basic examination |
| PBI | Papillary bleeding index |
| PD | Probing depth |
| PI | Plaque index |
| REC | Gingival recession |
| SBI | Sulcus bleeding index |
| SLB | Self-ligated brackets |
| Tn | Time measure in months |
References
- Alfuriji, S.; Alhazmi, N.; Alhamlan, N.; Al-Ehaideb, A.; Alruwaithi, M.; Alkatheeri, N.; Geevarghese, A. The effect of orthodontic therapy on periodontal health: A review of the literature. Int. J. Dent. 2014, 2014, 585048. [Google Scholar] [CrossRef]
- Bollen, A.M.; Cunha-Cruz, J.; Bakko, D.W.; Huang, G.J.; Hujoel, P.P. The effects of orthodontic therapy on periodontal health: A systematic review of controlled evidence. J. Am. Dent. Assoc. 2008, 139, 413–422. [Google Scholar] [CrossRef]
- Ren, Y.; Jongsma, M.A.; Mei, L.; van der Mei, H.C.; Busscher, H.J. Orthodontic treatment with fixed appliances and biofilm formation—A potential public health threat? Clin. Oral Investig. 2014, 18, 1711–1718. [Google Scholar] [CrossRef] [PubMed]
- Sandić, M.Z.; Popović, B.; Carkić, J.; Nikolić, N.; Glisić, B. Changes in subgingival microflora after placement and removal of fixed orthodontic appliances. Srp. Arh. Za Celok. Lek. 2014, 142, 301–305. [Google Scholar] [CrossRef]
- Rosvall, M.D.; Fields, H.W.; Ziuchkovski, J.; Rosenstiel, S.F.; Johnston, W.M. Attractiveness, acceptability, and value of orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2009, 135, e1–e12. [Google Scholar] [CrossRef]
- Paolone, M.G.; Kaitsas, R.; Paolone, G.; Kaitsas, V. Lingual orthodontics and forced eruption: A means for osseous and tissue regeneration. Prog. Orthod. 2008, 9, 46–57. [Google Scholar] [PubMed]
- Martina, S.; Rongo, R.; Bucci, R.; Razionale, A.V.; Valletta, R.; D’Antò, V. In vitro cytotoxicity of different thermoplastic materials for clear aligners. Angle Orthod. 2019, 89, 942–945. [Google Scholar] [CrossRef]
- Dannan, A. An update on periodontic-orthodontic interrelationships. J. Indian Soc. Periodontol. 2010, 14, 66–71. [Google Scholar] [CrossRef]
- Ke, Y.; Zhu, Y.; Zhu, M. A comparison of treatment effectiveness between clear aligner and fixed appliance therapies. BMC Oral Health 2019, 19, 24. [Google Scholar] [CrossRef]
- Miethke, R.R.; Brauner, K. A comparison of the periodontal health of patients during treatment with the Invisalign® system and with fixed lingual appliances. J. Orofac. Orthop. 2007, 68, 223–231. [Google Scholar] [CrossRef]
- Chhibber, A.; Agarwal, S.; Yadav, S.; Kuo, C.-L.; Upadhyay, M. Which orthodontic appliance is best for oral hygiene? A randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Issa, F.H.K.M.; Issa, Z.H.K.M.; Rabah, A.F.; Hu, L. Periodontal parameters in adult patients with clear aligners orthodontics treatment versus three other types of brackets: A cross-sectional study. J. Orthod. Sci. 2020, 9, 4. [Google Scholar]
- Abbate, G.M.; Caria, M.P.; Montanari, P.; Mannu, C.; Orrù, G.; Caprioglio, A.; Levrini, L. Periodontal health in teenagers treated with removable aligners and fixed orthodontic appliances. J. Orofac. Orthop. 2015, 76, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Miethke, R.R.; Vogt, S. A comparison of the periodontal health of patients during treatment with the Invisalign® system and with fixed orthodontic appliances. J. Orofac. Orthop. 2005, 66, 219–229. [Google Scholar] [CrossRef]
- Madariaga, A.C.P.; Bucci, R.; Rongo, R.; Simeon, V.; D’Antò, V.; Valletta, R. Impact of fixed orthodontic appliance and clear aligners on the periodontal health: A prospective clinical study. Dent. J. 2020, 8, 4. [Google Scholar] [CrossRef]
- Levrini, L.; Mangano, A.; Montanari, P.; Margherini, S.; Caprioglio, A.; Abbate, G.M. Periodontal health status in patients treated with the Invisalign® system and fixed orthodontic appliances: A 3 months clinical and microbiological evaluation. Eur. J. Dent. 2015, 9, 404–410. [Google Scholar] [CrossRef]
- Azaripour, A.; Weusmann, J.; Mahmoodi, B.; Peppas, D.; Gerhold-Ay, A.; Van Noorden, C.J.F.; Willershausen, B. Braces versus Invisalign®: Gingival parameters and patients’ satisfaction during treatment: A cross-sectional study. BMC Oral Health 2015, 15, 69. [Google Scholar] [CrossRef]
- Preoteasa, C.T.; Ionescu, E.; Preoteasa, E. Risks and complications associated with orthodontic treatment. In Orthodontics—Basic Aspects and Clinical Considerations, 1st ed.; Bourzgui, F., Ed.; IntechOpen: Rijeka, Crotia, 2012; pp. 403–428. [Google Scholar]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol 2000 2013, 62, 59–94. [Google Scholar] [CrossRef]
- Alexander, S.A. Effects of orthodontic attachments on the gingival health of permanent second molars. Am. J. Orthod. Dentofac. Orthop. 1991, 100, 337–340. [Google Scholar] [CrossRef]
- Garcez, A.S.; Suzuki, S.S.; Ribeiro, M.S.; Mada, E.Y.; Freitas, A.Z.; Suzuki, H. Biofilm retention by 3 methods of ligation on orthodontic brackets: A microbiologic and optical coherence tomography analysis. Am. J. Orthod. Dentofac. Orthop. 2011, 140, e193–e198. [Google Scholar] [CrossRef]
- van Gastel, J.; Quirynen, M.; Teughels, W.; Carels, C. The relationships between malocclusion, fixed orthodontic appliances and periodontal disease. A review of the literature. Aust. Orthod. J. 2007, 23, 121–129. [Google Scholar] [PubMed]
- Davis, S.M.; Plonka, A.B.; Fulks, B.A.; Taylor, K.L.; Bashutski, J. Consequences of orthodontic treatment on periodontal health: Clinical and microbial effects. Semin. Orthod. 2014, 20, 139–149. [Google Scholar] [CrossRef]
- Sifakakis, I.; Papaioannou, W.; Papadimitriou, A.; Kloukos, D.; Papageorgiou, S.N.; Eliades, T. Salivary levels of cariogenic bacterial species during orthodontic treatment with thermoplastic aligners or fixed appliances: A prospective cohort study. Prog. Orthod. 2018, 19, 25. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Vissink, A. Cytokines in crevicular fluid and orthodontic tooth movement. Eur. J. Oral Sci. 2008, 116, 89–97. [Google Scholar] [CrossRef]
- Ristic, M.; Svabic, M.V.; Sasic, M.; Zelic, O. Clinical and microbiological effects of fixed orthodontic appliances on periodontal tissues in adolescents. Orthod. Craniofac. Res. 2007, 10, 187–195. [Google Scholar] [CrossRef]
- Mummolo, S.; Marchetti, E.; Giuca, M.R.; Gallusi, G.; Tecco, S.; Gatto, R.; Marzo, G. In-office bacteria test for a microbial monitoring during the conventional and self-ligating orthodontic treatment. Head Face Med. 2013, 9, 7. [Google Scholar] [CrossRef]
- Lundström, F.; Krasse, B.O. Caries incidence in orthodontic patients with high levels of Streptococcus mutans. Eur. J. Orthod. 1987, 9, 117–121. [Google Scholar] [CrossRef]
- Bräscher, A.K.; Zuran, D.; Feldmann Jr, R.E.; Benrath, J. Patient survey on Invisalign® treatment comparing the SmartTrack® material to the previous aligner material. J. Orofac. Orthop. 2016, 77, 432–438. [Google Scholar] [CrossRef]
- Hohoff, A.; Fillion, D.; Stamm, T.; Goder, G.; Sauerland, C.; Ehmer, U. Oral comfort, function and hygiene in patients with lingual brackets. J. Orofac. Orthop. 2003, 64, 359–371. [Google Scholar] [CrossRef]
- Taylor, M.G.; Mcgorray, S.P.; Durrett, S.; Pavlow, S.; Downey, N.; Lenk, M.; Oxford, D.; Dolce, C.; Wheeler, T.T. Effect of Invisalign aligners on periodontal tissues. J. Dent. Res. 2003, 82, 1483. [Google Scholar]
- Bagga, D.K. Adult orthodontics versus adolescent orthodontics: An overview. J. Oral Health Commun. Dent. 2010, 4, 42–47. [Google Scholar] [CrossRef]
- Addy, M.; Perriam, E.; Sterry, A. Effects of sugared and sugar-free chewing gum on the accumulation of plaque and debris on the teeth. J. Clin. Periodontol. 1982, 9, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Lara-Carrillo, E.; Montiel-Bastida, N.-M.; Sánchez-Pérez, L.; Alanís-Tavira, J. Effect of orthodontic treatment on saliva, plaque and the levels of Streptococcus mutans and Lactobacillus. Med. Oral Patol. Oral Cirugía Bucal 2010, 15, e924–e929. [Google Scholar] [CrossRef] [PubMed]
- Türköz, C.; Bavbek, N.C.; Varlik, S.K.; Akça, G. Influence of thermoplastic retainers on Streptococcus mutans and Lactobacillus adhesion. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 598–603. [Google Scholar] [CrossRef]
- Acharya, S.; Goyal, A.; Utreja, A.K.; Mohanty, U. Effect of three different motivational techniques on oral hygiene and gingival health of patients undergoing multibracketed orthodontics. Angle Orthod. 2011, 81, 884–888. [Google Scholar] [CrossRef]
- Lalic, M.; Aleksic, E.; Gajic, M.; Milic, J.; Malesevic, D. Does oral health counseling effectively improve oral hygiene of orthodontic patients? Eur. J. Paediatr. Dent. 2012, 13, 181–186. [Google Scholar]


{kind=link}
| Population (P) | Patients under Orthodontic Treatment with Multibracket Orthodontic Appliances or Clear Aligners |
|---|---|
| Intervention (I) | Patients treated with clear aligners |
| Comparison (C) | Patients using multibracket orthodontic appliances |
| Outcome (O) | Periodontal health |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Clinical study on human fitting with the subject | Narrative review |
| RCT, prospective or cohort study comparing periodontal indexes of patients treated with multibracket appliance and aligners with follow-up | Retrospective study |
| RCT, prospective or cohort study comparing periodontal indexes of patients treated with multibracket appliance and aligners without follow-up | Secondary study |
| Articles without clinical studies | |
| Articles in English | No full-text available |
| Studies fitting with the subject using Invisalign technology | No relevant title or abstract |
| Patient with antibiotic therapy or periodontitis |
| Authors (Refs.) | Female/Male | Sample Number | Average Age | Recruitment Time | Study Design | City/Country | Outcome Measures | Time Measures | Number of Multibracket Appliances | Number of Clear Aligners | Potential Biases |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pango Madaraiga et al., 2020 | 20/20 | Total: 40 | Mean age FG: 20.6 Mean age CA: 34.7 | Unknown | Prospective clinical study | Naples, Italy | PD PI BoP REC | T0 T3 | 20 | 20 | Without long-term assessment |
| Chhibber et al., 2017 | 30/41 | Total: 71 | Mean age 15.6 ± 4.3 | 2011–2014 | Randomized control trial | Connecticut, Australia | PI GI PerioBl | T0 T9 T18 | 44 22 ELB 22 SLB | 27 | Different periods of assessment (without short-term) |
| Levrini et al., 2015 | 52/25 | Total 77 (33: Control) | 16 to 30 years old Mean age: 24.3 | Unknown | Prospective study | Varese, Italy | PI PD BoP Microbiological analysis | T0 T1 T3 | 35 | 32 | Without long-term of assessment |
| Abbate et al., 2015 | Unknown | Total: 50 | 10 to 18 years old | 2012–2013 | Prospective study | Varese, Italy | PD PI BoP Microbiological analysis | T0 T3 T6 T12 | 25 | 25 | Does not specify female/male ratio; different periods of assessment |
| Azaripour et al., 2015 | 73/27 | Total: 100 | 11 to 62 years old Mean age FG: 16.3 Mean age CA: 31.9 | Unknown | Cross-sectional study | Gutenberg, Germany | GI SBI API MPI | T0 T12 | 50 | 50 | Different periods of assessment and indexes; without short-term assessment; included children |
| Miethke & Vogt, 2005 | 43/17 | Total: 60 | 18 to 51 years old Mean age: 30.1 | 2002–2003 | Clinical trial (Prospective cohort study) | Berlin, Germany | GI PBI PI SPD | T1 T2 T3 3/4 weeks intervals | 30 | 30 | Without long-term assessment |
| Miethke & Brauner, 2007 | Unknown | Total: 60 | 16 to 48 years old Mean age: 39.6 | Feb and May of 2005 | Prospective study | Berlin, Germany | GI PBI PI SPD | T1 T2 T3 3/4 weeks intervals | 30 (lingual group) | 30 (control group from the previous study) | Does not specify female/male ratio; without long-term assessment |
| Issa et al., 2020 | 40/40 | Total:80 | Mean age CA: 26,85 Mean age FG: 27,05 | 2015–2016 | Cross-sectional study | China | PI GI GBI SBI PBI BPE BoP | regular assessments unknown | 60 20 ELB 20 CCB 20 SLB | 20 | No deep information about time of assessment |
| Authors (Refs.) | Gingival Index (GI) | Probing Depth (PD) | Plaque Index (PI) | Bleeding of Probing (BoP) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pango Madaraiga et al., 2020 | not mentioned | not mentioned | not mentioned | AG T0 = 0.1 T3 = 0 | FG T0 = 0.3 T3 = 0.14 | Mean ∑AG = 0.05 ∑FG = 0.22 | AG T0 = 0.42 T3 = 0.11 | FG T0 = 0.31 T3 = 0.15 | Mean ∑AG = 0.27 ∑FG = 0.23 | AG T0 = 0.55 T3 = 0.13 | FG T0 = 0.77 T3 = 0.13 | Mean ∑AG = 0.34 ∑FG = 0.9 |
| Chhibber et al., 2017 | AG T0 = 0.42 ± 0.5 T9 = 0.50 ± 0.59 T18 = 0.75 ± 0.53 | FG T0 = 0.05 ± 0.22 T9 = 1.21 ± 0.79 T18 = 1.32 ± 0.67 | Mean ∑AG = 0.55 ± 0.54 ∑FG = 1.01 ± 0.56 | not mentioned | not mentioned | not mentioned | AG T0 = 0.50 ± 0.51 T9 = 0.83 ± 0.48 T18 = 0.92 ± 0.58 | FG T0 = 0.70 ± 0.73 T9 = 1.32 ± 0.67 T18 = 1.32 ± 0.67 | Mean ∑AG = 0.75 ± 0.52 ∑FG = 1.1 ± 0.69 | not mentioned | not mentioned | not mentioned |
| Levrini et al., 2015 | not mentioned | not mentioned | not mentioned | AG T0 = 2.18 T1 = 2.75 T3 = 1.6 | FG T0 = 2.18 T1 = 2.2 T3 = 1.3 | Mean ∑AG = 2.17 ∑FG = 1.89 | not mentioned | not mentioned | not mentioned | not mentioned | not mentioned | not mentioned |
| Abbate et al., 2015 | not mentioned | not mentioned | not mentioned | AG T0 = 2.28 T3 = 2.23 T6 = 2.37 T12 = 2.5 | FG T0 = 2.26 T3 = 2.86 T6 = 3.22 T12 = 3.42 | Mean ∑AG = 2.35 ∑FG = 2.94 | AG T0 = 0.91 T3 = 0.64 T6 = 0.32 T12 = 0.36 | FG T0 = 0.82 T3 = 1.92 T6 = 2.32 T12 = 2.42 | Mean ∑AG = 0.56 ∑FG = 1.87 | AG T0 = 0.14 T3 = 0 T6 = 0.04 T12 = 0.04 | FG T0 = 0 T3 = 0.36 T6 = 0.58 T12 = 0.74 | Mean ∑AG = 0.05 ∑FG = 0.42 |
| Azaripour et al., 2015 | AG T0 = 0.27 ± 0.25 T12 = 0.35 ± 0.34 | FG T0 = 0.29 ± 0.24 T12 = 0.54 ± 0.50 | Mean ∑AG = 0.31 ± 0.29 ∑FG = 0.42 ± 0.37 | not mentioned | not mentioned | not mentioned | AG T0 = 0.16 ± 0.1 T12 = 0.30 ± 0.25 | FG T0 = 0.20 ± 0.1 T12 = 0.38 ± 0.22 | Mean ∑AG = 0.23 ± 0.18 ∑FG = 0.58 ± 0.16 | not mentioned | not mentioned | not mentioned |
| Miethke & Vogt, 2005 | AG T1 = 0.71 ± 0.39 T2 = 0.61 ± 0.35 T3 = 0.46 ± 0.34 | FG T1 = 1.02 ± 0.69 T2 = 0.73 ± 0.58 T3 = 0.68 ± 0.66 | Mean ∑AG = 0.59 ± 0.30 ∑FG = 0.81 ± 0.59 | AG T1 = 2.39 ± 0.45 T2 = 2.29 ± 0.41 T3 = 2.26 ± 0.48 | FG T1 = 2.60 ± 0.73 T2 = 2.52 ± 0.65 T3 = 2.50 ± 0.67 | Mean ∑AG = 2.31 ± 0.39 ∑FG = 2.45 ± 0.65 | AG T1 = 0.48 ± 0.41 T2 = 0.41 ± 0.37 T3 = 0.28 ± 0.32 | FG T1 = 0.80 ± 0.58 T2 = 0.56 ± 0.44 T3 = 0.50 ± 0.53 | Mean ∑AG = 0.39 ± 0.31 ∑FG = 0.62 ± 0.48 | not mentioned | not mentioned | not mentioned |
| Miethke & Brauner, 2007 | AG T1 = 0.71 ± 0.39 T2 = 0.61 ± 0.35 T3 = 0.46 ± 0.34 | FG T1 = 1.02 ± 0.53 T2 = 1.02 ± 0.43 T3 = 0.96 ± 0.43 | Mean ∑AG = 0.59 ± 0.30 ∑FG = 1.00 ± 0.43 | AG T1 = 2.39 ± 0.45 T2 = 2.29 ± 0.41 T3 = 2.26 ± 0.48 | FG T1 = 2.55 ± 0.38 T2 = 2.43 ± 0.33 T3 = 2.50 ± 0.35 | Mean ∑AG = 2.31 ± 0.39 ∑FG = 2.50 ± 0.33 | AG T1 = 0.48 ± 0.41 T2 = 0.41 ± 0.37 T3 = 0.28 ± 0.32 | FG T1 = 0.84 ± 0.46 T2 = 0.95 ± 0.44 T3 = 0.89 ± 0.45 | Mean ∑AG = 0.39 ± 0.31 ∑FG = 0.89 ± 0.41 | not mentioned | not mentioned | not mentioned |
| Issa et al., 2020 | AG Tx = 0.008 | FG Tx = 1.06 | — | not mentioned | not mentioned | not mentioned | AG Tx = 0.2 | FG Tx = 1.7 | — | AG Tx = 0.01 | FG Tx = 0.37 | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Partouche, A.J.D.; Castro, F.; Baptista, A.S.; Costa, L.G.; Fernandes, J.C.H.; Fernandes, G.V.d.O. Effects of Multibracket Orthodontic Treatment versus Clear Aligners on Periodontal Health: An Integrative Review. Dent. J. 2022, 10, 177. https://doi.org/10.3390/dj10100177
Partouche AJD, Castro F, Baptista AS, Costa LG, Fernandes JCH, Fernandes GVdO. Effects of Multibracket Orthodontic Treatment versus Clear Aligners on Periodontal Health: An Integrative Review. Dentistry Journal. 2022; 10(10):177. https://doi.org/10.3390/dj10100177
Chicago/Turabian StylePartouche, Aaron Jacob David, Filipe Castro, Ana Sofia Baptista, Liliana Gavinha Costa, Juliana Campos Hasse Fernandes, and Gustavo Vicentis de Oliveira Fernandes. 2022. "Effects of Multibracket Orthodontic Treatment versus Clear Aligners on Periodontal Health: An Integrative Review" Dentistry Journal 10, no. 10: 177. https://doi.org/10.3390/dj10100177
APA StylePartouche, A. J. D., Castro, F., Baptista, A. S., Costa, L. G., Fernandes, J. C. H., & Fernandes, G. V. d. O. (2022). Effects of Multibracket Orthodontic Treatment versus Clear Aligners on Periodontal Health: An Integrative Review. Dentistry Journal, 10(10), 177. https://doi.org/10.3390/dj10100177