
SATB2 and MDM2 Immunoexpression and Diagnostic Role in Primary Osteosarcomas of the Jaw


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Clinicopathologic Findings
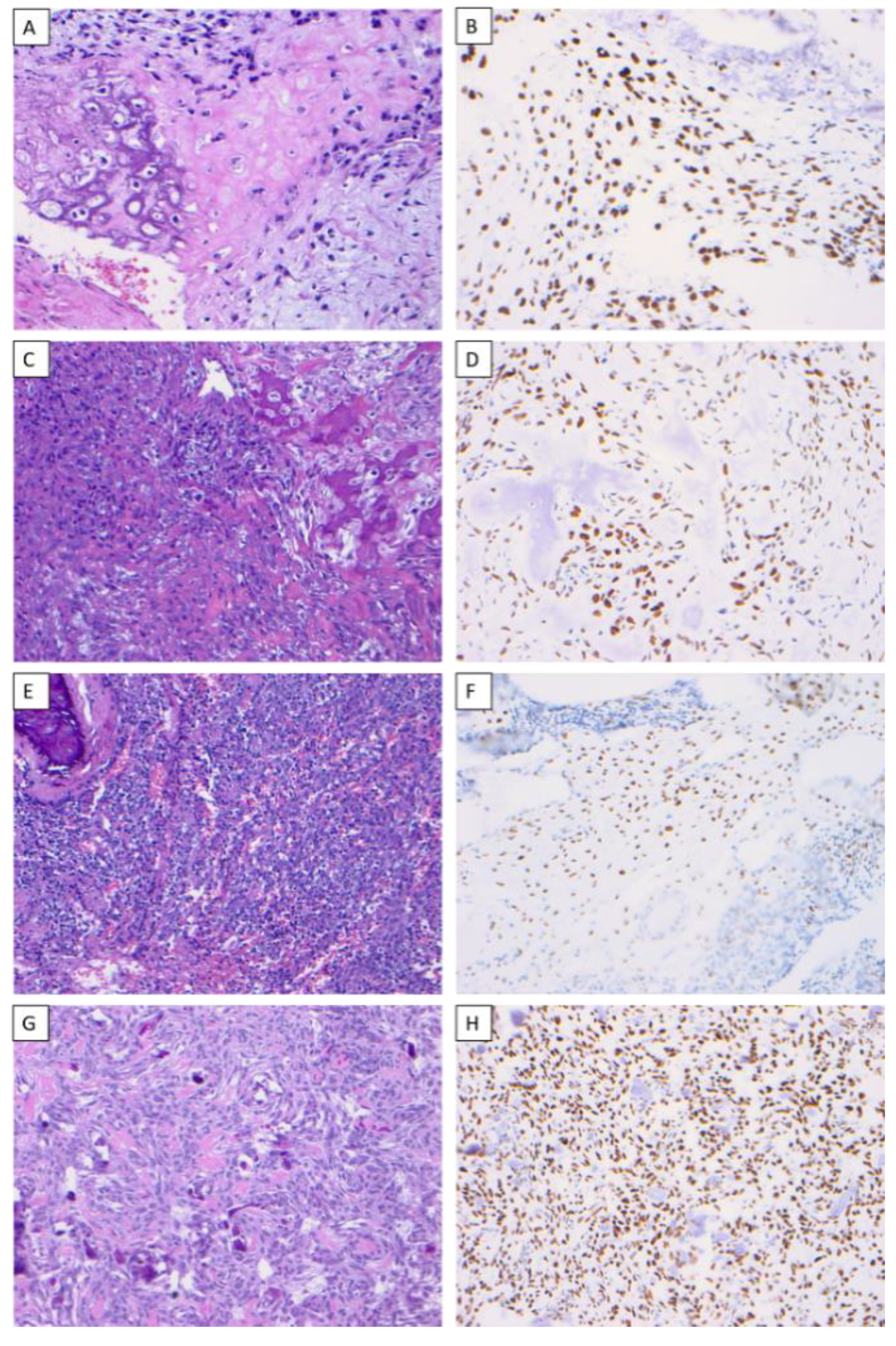
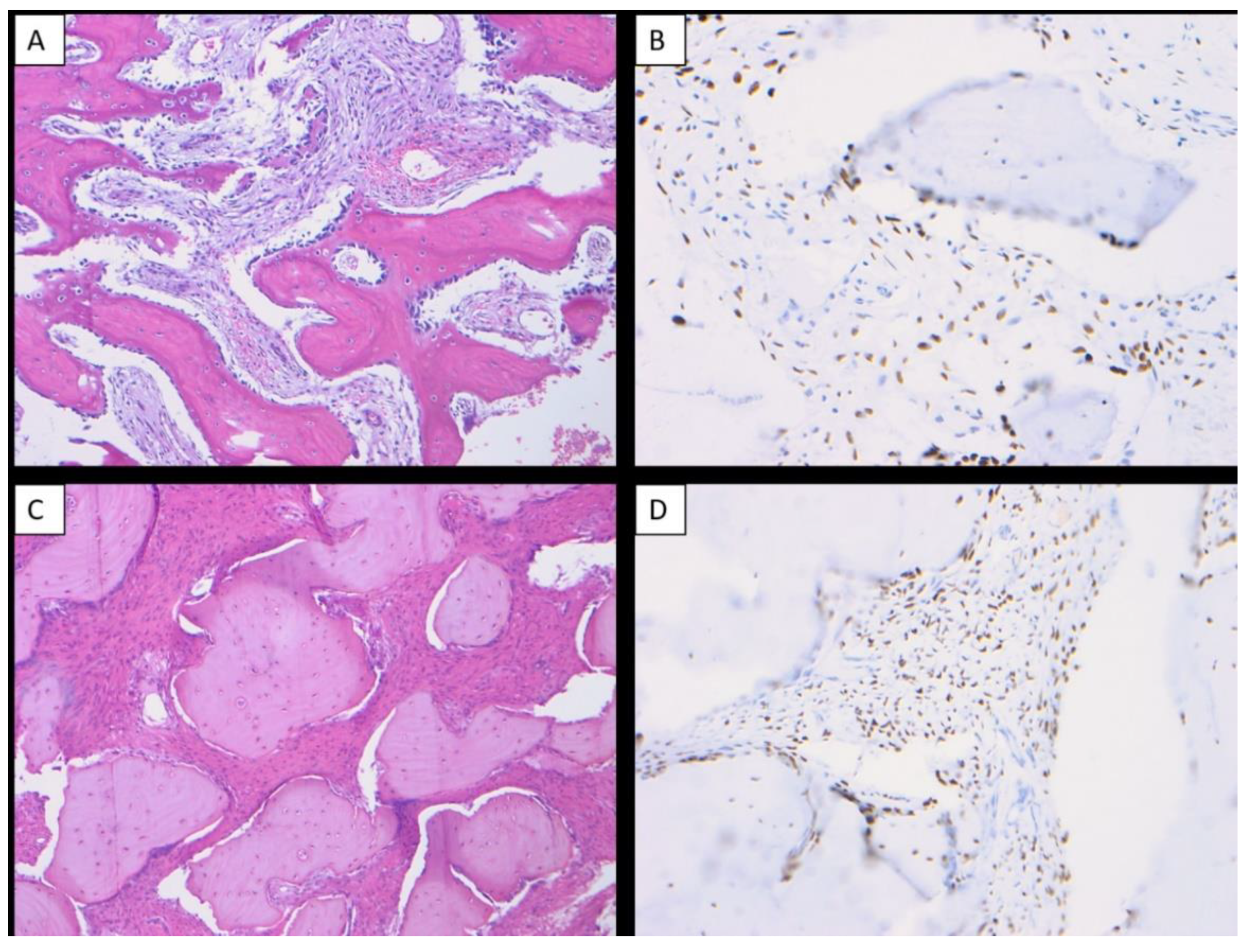
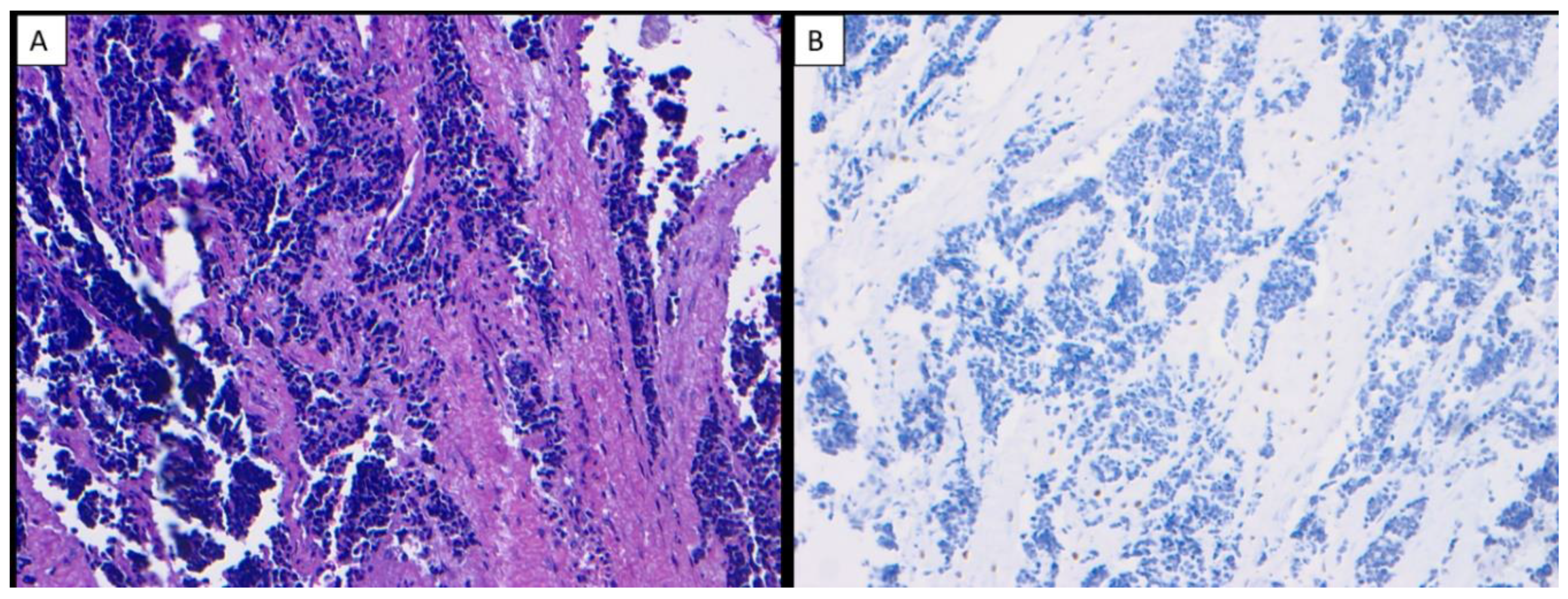
3.2. SATB2 Status
3.3. MDM2 Status
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Baumhoer, D.; Brunner, P.; Eppenberger-Castori, S.; Smida, J.; Nathrath, M.; Jundt, G. Osteosarcomas of the Jaws Differ from Their Peripheral Counterparts and Require a Distinct Treatment Approach. Experiences from the Doesak Registry. Oral Oncol. 2014, 50, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Paparella, M.L.; Olvi, L.G.; Brandizzi, D.; Keszler, A.; Santini-Araujo, E.; Cabrini, R.L. Osteosarcoma of the Jaw: An Analysis of a Series of 74 Cases. Histopathology 2013, 63, 551–557. [Google Scholar] [CrossRef]
- Cheng, Y.S.; Wright, J.M.; Walstad, W.R.; Finn, M.D. Osteosarcoma Arising in Paget’s Disease of the Mandible. Oral Oncol. 2002, 38, 785–792. [Google Scholar] [CrossRef]
- Ginat, D.; Schulte, J.; Gooi, Z.; Cipriani, N. High-Grade Conventional Osteosarcoma of the Mandible Associated with P53 Germline Mutation. J. Craniofac. Surg. 2018, 29, 738–740. [Google Scholar] [CrossRef]
- Bennett, J.H.; Thomas, G.; Evans, A.W.; Speight, P.M. Osteosarcoma of the Jaws: A 30-Year Retrospective Review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 90, 323–332. [Google Scholar] [CrossRef]
- Garrington, G.E.; Scofield, H.H.; Cornyn, J.; Hooker, S.P. Osteosarcoma of the Jaws. Analysis of 56 Cases. Cancer 1967, 20, 377–391. [Google Scholar] [CrossRef]
- Granowski-LeCornu, M.; Chuang, S.K.; Kaban, L.B.; August, M. Osteosarcoma of the Jaws: Factors Influencing Prognosis. J. Oral Maxillofac. Surg. 2011, 69, 2368–2375. [Google Scholar] [CrossRef] [PubMed]
- Broadhead, M.L.; Clark, J.C.; Myers, D.E.; Dass, C.R.; Choong, P.F. The Molecular Pathogenesis of Osteosarcoma: A Review. Sarcoma 2011, 2011, 959248. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, H.; Schreuder, W.H.; de Lange, J. Osteosarcoma: A Comparison of Jaw Versus Nonjaw Localizations and Review of the Literature. Sarcoma 2013, 2013, 316123. [Google Scholar] [CrossRef] [PubMed]
- Kassir, R.R.; Rassekh, C.H.; Kinsella, J.B.; Segas, J.; Carrau, R.L.; Hokanson, J.A. Osteosarcoma of the Head and Neck: Meta-Analysis of Nonrandomized Studies. Laryngoscope 1997, 107, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Russ, J.E.; Jesse, R.H. Management of Osteosarcoma of the Maxilla and Mandible. Am. J. Surg. 1980, 140, 572–576. [Google Scholar] [CrossRef]
- Uhlen, M.; Fagerberg, L.; Hallstrom, B.M.; Lindskog, C.; Oksvold, P.; Mardinoglu, A.; Sivertsson, A.; Kampf, C.; Sjostedt, E.; Asplund, A.; et al. Tissue-Based Map of the Human Proteome. Science 2015, 347, 1260419. [Google Scholar] [CrossRef] [PubMed]
- FitzPatrick, D.R.; Carr, I.M.; McLaren, L.; Leek, J.P.; Wightman, P.; Williamson, K.; Gautier, P.; McGill, N.; Hayward, C.; Firth, H.; et al. Identification of Satb2 as the Cleft Palate Gene on 2q32-Q33. Hum. Mol. Genet. 2003, 12, 2491–2501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeld, J.A.; Ballif, B.C.; Lucas, A.; Spence, E.J.; Powell, C.; Aylsworth, A.S.; Torchia, B.A.; Shaffer, L.G. Small Deletions of Satb2 Cause Some of the Clinical Features of the 2q33.1 Microdeletion Syndrome. PLoS ONE 2009, 4, e6568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dixon, M.J.; Marazita, M.L.; Beaty, T.H.; Murray, J.C. Cleft Lip and Palate: Understanding Genetic and Environmental Influences. Nat. Rev. Genet. 2011, 12, 167–178. [Google Scholar] [CrossRef] [Green Version]
- Britanova, O.; Depew, M.J.; Schwark, M.; Thomas, B.L.; Miletich, I.; Sharpe, P.; Tarabykin, V. Satb2 Haploinsufficiency Phenocopies 2q32-Q33 Deletions, Whereas Loss Suggests a Fundamental Role in the Coordination of Jaw Development. Am. J. Hum. Genet. 2006, 79, 668–678. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Tu, Q.; Grosschedl, R.; Kim, M.S.; Griffin, T.; Drissi, H.; Yang, P.; Chen, J. Roles of Satb2 in Osteogenic Differentiation and Bone Regeneration. Tissue Eng. Part A 2011, 17, 1767–1776. [Google Scholar] [CrossRef]
- Dobreva, G.; Chahrour, M.; Dautzenberg, M.; Chirivella, L.; Kanzler, B.; Farinas, I.; Karsenty, G.; Grosschedl, R. Satb2 Is a Multifunctional Determinant of Craniofacial Patterning and Osteoblast Differentiation. Cell 2006, 125, 971–986. [Google Scholar] [CrossRef] [Green Version]
- Magnusson, K.; de Wit, M.; Brennan, D.J.; Johnson, L.B.; McGee, S.F.; Lundberg, E.; Naicker, K.; Klinger, R.; Kampf, C.; Asplund, A.; et al. Satb2 in Combination with Cytokeratin 20 Identifies over 95% of All Colorectal Carcinomas. Am. J. Surg. Pathol. 2011, 35, 937–948. [Google Scholar] [CrossRef]
- Machado, I.; Navarro, S.; Picci, P.; Llombart-Bosch, A. The Utility of Satb2 Immunohistochemical Expression in Distinguishing between Osteosarcomas and Their Malignant Bone Tumor Mimickers, Such as Ewing Sarcomas and Chondrosarcomas. Pathol. Res. Pract. 2016, 212, 811–816. [Google Scholar] [CrossRef]
- Guerin, M.; Thariat, J.; Ouali, M.; Bouvier, C.; Decouvelaere, A.V.; Cassagnau, E.; Aubert, S.; Lepreux, S.; Coindre, J.M.; Valmary-Degano, S.; et al. A New Subtype of High-Grade Mandibular Osteosarcoma with Rasal1/Mdm2 Amplification. Hum. Pathol. 2016, 50, 70–78. [Google Scholar] [CrossRef] [Green Version]
- Dujardin, F.; Binh, M.B.; Bouvier, C.; Gomez-Brouchet, A.; Larousserie, F.; Muret, A.; Louis-Brennetot, C.; Aurias, A.; Coindre, J.M.; Guillou, L.; et al. Mdm2 and Cdk4 Immunohistochemistry Is a Valuable Tool in the Differential Diagnosis of Low-Grade Osteosarcomas and Other Primary Fibro-Osseous Lesions of the Bone. Mod. Pathol. 2011, 24, 624–637. [Google Scholar] [CrossRef] [Green Version]
- Momand, J.; Wu, H.H.; Dasgupta, G. Mdm2--Master Regulator of the P53 Tumor Suppressor Protein. Gene 2000, 242, 15–29. [Google Scholar] [CrossRef]
- Momand, J.; Zambetti, G.P.; Olson, D.C.; George, D.; Levine, A.J. The Mdm-2 Oncogene Product Forms a Complex with the P53 Protein and Inhibits P53-Mediated Transactivation. Cell 1992, 69, 1237–1245. [Google Scholar] [CrossRef]
- Chen, J.; Lin, J.; Levine, A.J. Regulation of Transcription Functions of the P53 Tumor Suppressor by the Mdm-2 Oncogene. Mol. Med. 1995, 1, 142–152. [Google Scholar] [CrossRef] [Green Version]
- Haupt, Y.; Maya, R.; Kazaz, A.; Oren, M. Mdm2 Promotes the Rapid Degradation of P53. Nature 1997, 387, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Pilotti, S.; della Torre, G.; Lavarino, C.; di Palma, S.; Sozzi, G.; Minoletti, F.; Rao, S.; Pasquini, G.; Azzarelli, A.; Rilke, F.; et al. Distinct Mdm2/P53 Expression Patterns in Liposarcoma Subgroups: Implications for Different Pathogenetic Mechanisms. J. Pathol. 1997, 181, 14–24. [Google Scholar] [CrossRef]
- Bode-Lesniewska, B.; Zhao, J.; Speel, E.J.; Biraima, A.M.; Turina, M.; Komminoth, P.; Heitz, P.U. Gains of 12q13-14 and Overexpression of Mdm2 Are Frequent Findings in Intimal Sarcomas of the Pulmonary Artery. Virchows Arch. 2001, 438, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Quesnel, B.; Preudhomme, C.; Oscier, D.; Lepelley, P.; Collyn-d’Hooghe, M.; Facon, T.; Zandecki, M.; Fenaux, P. Over-Expression of the Mdm2 Gene Is Found in Some Cases of Haematological Malignancies. Br. J. Haematol. 1994, 88, 415–418. [Google Scholar] [CrossRef]
- Grad-Akrish, S.; Rachmiel, A.; Ben-Izhak, O. Satb2 Is Not a Reliable Diagnostic Marker for Distinguishing between Oral Osteosarcoma and Fibro-Osseous Lesions of the Jaws. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Conner, J.R.; Hornick, J.L. Satb2 Is a Novel Marker of Osteoblastic Differentiation in Bone and Soft Tissue Tumours. Histopathology 2013, 63, 36–49. [Google Scholar] [CrossRef]
- Limbach, A.L.; Lingen, M.W.; McElherne, J.; Mashek, H.; Fitzpatrick, C.; Hyjek, E.; Mostofi, R.; Cipriani, N.A. The Utility of Mdm2 and Cdk4 Immunohistochemistry and Mdm2 Fish in Craniofacial Osteosarcoma. Head Neck Pathol. 2020, 14, 889–898. [Google Scholar] [CrossRef]
- Lopes, M.A.; Nikitakis, N.G.; Ord, R.A.; Sauk, J., Jr. Amplification and Protein Expression of Chromosome 12q13-15 Genes in Osteosarcomas of the Jaws. Oral Oncol. 2001, 37, 566–571. [Google Scholar] [CrossRef]
- Junior, A.T.; Alves, F.d.; Pinto, C.A.; Carvalho, A.L.; Kowalski, L.P.; Lopes, M.A. Clinicopathological and Immunohistochemical Analysis of Twenty-Five Head and Neck Osteosarcomas. Oral Oncol. 2003, 39, 521–530. [Google Scholar] [CrossRef]
- Tabareau-Delalande, F.; Collin, C.; Gomez-Brouchet, A.; Bouvier, C.; Decouvelaere, A.V.; de Muret, A.; Pages, J.C.; de Pinieux, G. Chromosome 12 Long Arm Rearrangement Covering Mdm2 and Rasal1 Is Associated with Aggressive Craniofacial Juvenile Ossifying Fibroma and Extracranial Psammomatoid Fibro-Osseous Lesions. Mod. Pathol. 2015, 28, 48–56. [Google Scholar] [CrossRef]
- Wang, B.; Fang, L.; Zhao, H.; Xiang, T.; Wang, D. Mdm2 Inhibitor Nutlin-3a Suppresses Proliferation and Promotes Apoptosis in Osteosarcoma Cells. Acta Biochim. Biophys. Sin. 2012, 44, 685–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, H.; Maki, C.G. Pharmacologic Activation of P53 by Small-Molecule Mdm2 Antagonists. Curr. Pharm. Des. 2011, 17, 560–568. [Google Scholar] [CrossRef] [Green Version]
- Barbieri, E.; Mehta, P.; Chen, Z.; Zhang, L.; Slack, A.; Berg, S.; Shohet, J.M. Mdm2 Inhibition Sensitizes Neuroblastoma to Chemotherapy-Induced Apoptotic Cell Death. Mol. Cancer Ther. 2006, 5, 2358–2365. [Google Scholar] [CrossRef] [Green Version]
- Zauli, G.; Voltan, R.; Bosco, R.; Melloni, E.; Marmiroli, S.; Rigolin, G.M.; Cuneo, A.; Secchiero, P. Dasatinib Plus Nutlin-3 Shows Synergistic Antileukemic Activity in Both P53 Wild-Type and P53 Mutated B Chronic Lymphocytic Leukemias by Inhibiting the Akt Pathway. Clin. Cancer Res. 2011, 17, 762–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilgelm, A.E.; Pawlikowski, J.S.; Liu, Y.; Hawkins, O.E.; Davis, T.A.; Smith, J.; Weller, K.P.; Horton, L.W.; McClain, C.M.; Ayers, G.D.; et al. Mdm2 and Aurora Kinase a Inhibitors Synergize to Block Melanoma Growth by Driving Apoptosis and Immune Clearance of Tumor Cells. Cancer Res. 2015, 75, 181–193. [Google Scholar] [CrossRef] [Green Version]
- Carter, B.Z.; Mak, P.Y.; Mak, D.H.; Ruvolo, V.R.; Schober, W.; McQueen, T.; Cortes, J.; Kantarjian, H.M.; Champlin, R.E.; Konopleva, M.; et al. Synergistic Effects of P53 Activation Via Mdm2 Inhibition in Combination with Inhibition of Bcl-2 or Bcr-Abl in Cd34+ Proliferating and Quiescent Chronic Myeloid Leukemia Blast Crisis Cells. Oncotarget 2015, 6, 30487–30499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, D.G.; Koh, J.S.; Cho, W.H.; Song, W.S.; Kong, C.B.; Cho, S.H.; Lee, S.Y.; Lee, S.Y. Clinical Outcome of Low-Grade Central Osteosarcoma and Role of Cdk4 and Mdm2 Immunohistochemistry as a Diagnostic Adjunct. J. Orthop. Sci. 2015, 20, 529–537. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Age | Sex | Location | Size (cm) | SATB2 IHC | MDM2 IHC | MDM2 FISH |
|---|---|---|---|---|---|---|---|
| 1 | 49 | M | Mandible | 5 | Positive | Positive | Failed |
| 2 | 19 | F | Mandible | 10 | Positive | Positive | Failed |
| 3 | 16 | M | Mandible | NA | Positive | Positive, focal | Failed |
| 4 | 35 | F | Mandible | 9.5 | Positive | Negative | Failed |
| 5 | 35 | M | Maxilla | 10 | Positive | Negative | Failed |
| 6 | 23 | F | Maxilla | 5 | Positive | Negative | Failed |
| 7 | 10 | M | Mandible | 6.5 | Positive | Negative | Failed |
| 8 | 42 | F | Maxilla | 12 | Positive | Negative | Failed |
| 9 | 17 | F | Mandible | 16 | Positive | Negative | Failed |
| 10 | 42 | F | Maxilla | 5 | Positive | Negative | No amplification |
| 11 | 31 | M | Mandible | 12 | Positive | Negative | No amplification |
| Diagnosis | No. of Cases | No. (%) of Cases Positive for SATB2 | No. (%) of Cases Positive for MDM2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Score 0 | Score 1 | Score 2 | Score 3 | Score 0 | Score 1 | Score 2 | Score 3 | ||
| Chondroblastic OSJ | 5 | 0 | 1 (20) | 2 (40) | 2 (40) | 4 (80) | 1 (20) | 0 | 0 |
| Osteoblastic OSJ | 3 | 0 | 0 | 0 | 3 (100) | 2 (67) | 1 (33) | 0 | 0 |
| Fibroblastic OSJ | 2 | 0 | 0 | 1 (50) | 1 (50) | 1 (50) | 1 (50) | 0 | 0 |
| Small-cell OSJ | 1 | 0 | 0 | 1 (100) | 0 | 1 (100) | 0 | 0 | 0 |
| Ewing sarcoma | 1 | 1 (100) | 0 | 0 | 0 | 1 (100) | 0 | 0 | 0 |
| Ossifying fibroma | 7 | 0 | 3 (43) | 2 (28) | 2 (28) | 7 (100) | 0 | 0 | 0 |
| Fibrous dysplasia | 5 | 0 | 4 (80) | 1 (20) | 0 | 5 (100) | 0 | 0 | 0 |
| Articles | SATB2 IHC | MDM2 IHC |
|---|---|---|
| Grad-Akrish et al. [30] | 15/15 (100%) all moderate or strong diffuse | NP |
| Lott Limbach et al. [32] | NP | 7/11 (63%; all weak focal) |
| Guerin et al. [21] | NP | 3/36 (8%) |
| Lopes et al. [33] | NP | 8/9 (89%) |
| Junior et al. [34] | NP | 6/25 (24%) |
| Owosho et al. (current) | 11/11 (100%) all strong diffuse | 3/11 (27%; two moderate diffuse, one weak focal) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owosho, A.A.; Ladeji, A.M.; Adesina, O.M.; Adebiyi, K.E.; Olajide, M.A.; Okunade, T.; Palmer, J.; Kehinde, T.; Vos, J.A.; Cole, G.; et al. SATB2 and MDM2 Immunoexpression and Diagnostic Role in Primary Osteosarcomas of the Jaw. Dent. J. 2022, 10, 4. https://doi.org/10.3390/dj10010004
Owosho AA, Ladeji AM, Adesina OM, Adebiyi KE, Olajide MA, Okunade T, Palmer J, Kehinde T, Vos JA, Cole G, et al. SATB2 and MDM2 Immunoexpression and Diagnostic Role in Primary Osteosarcomas of the Jaw. Dentistry Journal. 2022; 10(1):4. https://doi.org/10.3390/dj10010004
Chicago/Turabian StyleOwosho, Adepitan A., Adeola M. Ladeji, Olufunlola M. Adesina, Kehinde E. Adebiyi, Mofoluwaso A. Olajide, Toluwaniyin Okunade, Jacob Palmer, Temitope Kehinde, Jeffrey A. Vos, Grayson Cole, and et al. 2022. "SATB2 and MDM2 Immunoexpression and Diagnostic Role in Primary Osteosarcomas of the Jaw" Dentistry Journal 10, no. 1: 4. https://doi.org/10.3390/dj10010004
APA StyleOwosho, A. A., Ladeji, A. M., Adesina, O. M., Adebiyi, K. E., Olajide, M. A., Okunade, T., Palmer, J., Kehinde, T., Vos, J. A., Cole, G., & Summersgill, K. F. (2022). SATB2 and MDM2 Immunoexpression and Diagnostic Role in Primary Osteosarcomas of the Jaw. Dentistry Journal, 10(1), 4. https://doi.org/10.3390/dj10010004