
Biomechanical Behavior Evaluation of a Novel Hybrid Occlusal Splint-Mouthguard for Contact Sports: 3D-FEA

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miró, A.; Buscà, B.; Aguilera-Castells, J.; Arboix-Alió, J. Acute effects of wearing bite-aligning mouthguards on muscular strength, power, agility and quickness in a trained population: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 6933. [Google Scholar] [CrossRef] [PubMed]
- Tripodi, D.; Cosi, A.; Fulco, D.; D’Ercole, S. The impact of sport training on oral health in athletes. Dent. J. 2021, 9, 51. [Google Scholar] [CrossRef] [PubMed]
- Tribst, J.P.M.; Dal Piva, A.M.d.O.; Bottino, M.A.; Kleverlaan, C.J.; Koolstra, J.H. Mouthguard use and TMJ injury prevention with different occlusions: A three-dimensional finite element analysis. Dent. Traumatol. 2020, 36, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Tribst, J.P.M.; Dal Piva, A.M.d.O.; Borges, A.L.S.; Bottino, M.A. Simulation of mouthguard use in preventing dental injuries caused by different impacts in sports activities. Sport Sci. Health 2019, 15, 85–90. [Google Scholar] [CrossRef]
- Nam, H.J.; Lee, J.-H.; Hong, D.-S.; Jung, H.C. The effect of wearing a customized mouthguard on body alignment and balance performance in professional basketball players. Int. J. Environ. Res. Public Health 2020, 17, 6431. [Google Scholar] [CrossRef]
- Borges, A.L.S.; Dal Piva, A.M.d.O.; Concílio, L.R.d.S.; Paes-Junior, T.J.d.A.; Tribst, J.P.M. Mouthguard use effect on the biomechanical response of an ankylosed maxillary central incisor during a traumatic impact: A 3-dimensional finite element analysis. Life 2020, 10, 294. [Google Scholar] [CrossRef] [PubMed]
- Tribst, J.P.M.; de Oliveira Dal Piva, A.M.; Borges, A.L.S.; Bottino, M.A. Influence of custom-made and stock mouthguard thickness on biomechanical response to a simulated impact. Dent. Traumatol. 2018, 34, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Sousa, A.M.; Pinho, A.C.; Messias, A.; Piedade, A.P. Present status in polymeric mouthguards. A future area for additive manufacturing? Polymers 2020, 12, 1490. [Google Scholar] [CrossRef]
- de la Parte, A.; Monticelli, F.; Toro-Román, V.; Pradas, F. Differences in oral health status in elite athletes according to sport modalities. Sustainability 2021, 13, 7282. [Google Scholar] [CrossRef]
- Mordini, L.; Lee, P.; Lazaro, R.; Biagi, R.; Giannetti, L. Sport and dental traumatology: Surgical solutions and prevention. Dent. J. 2021, 9, 33. [Google Scholar] [CrossRef]
- Leal, T.R.; de Lima, L.C.M.; Perazzo, M.F.; Neves, É.T.B.; Paiva, S.M.; Serra-Negra, J.M.C.; Ferreira, F.M.; Granville-Garcia, A.F. Influence of the practice of sports, sleep disorders, and habits on probable sleep bruxism in children with mixed dentition. Oral Dis. 2021. [Google Scholar] [CrossRef]
- Wetselaar, P.; Vermaire, E.J.H.; Lobbezoo, F.; Schuller, A.A. The prevalence of awake bruxism and sleep bruxism in the Dutch adult population. J. Oral Rehabil. 2019, 46, 617–623. [Google Scholar] [CrossRef]
- Okeson, J.P. The effects of hard and soft occlusal splints on nocturnal bruxism. J. Am. Dent. Assoc. 1987, 114, 788–791. [Google Scholar] [CrossRef]
- Dalewski, B.; Kamińska, A.; Kiczmer, P.; Węgrzyn, K.; Pałka, Ł.; Janda, K.; Sobolewska, E. Pressure algometry evaluation of two occlusal splint designs in bruxism management-randomized, controlled clinical trial. J. Clin. Med. 2021, 10, 2342. [Google Scholar] [CrossRef] [PubMed]
- Baena Lopes, M.; Romero Felizardo, K.; Danil Guiraldo, R.; Fancio Sella, K.; Ramos Junior, S.; Gonini Junior, A.; Bittencourt Berger, S. Photoelastic stress analysis of different types of anterior teeth splints. Dent. Traumatol. 2021, 37, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Tribst, J.P.M.; Dal Piva, A.M.d.O.; Ausiello, P.; De Benedictis, A.; Bottino, M.A.; Borges, A.L.S. Biomechanical analysis of a custom-made mouthguard reinforced with different Elastic Modulus laminates during a simulated maxillofacial trauma. Craniomaxillofac. Trauma Reconstr. 2021, 14, 254–260. [Google Scholar] [CrossRef]
- Cruz-Reyes, R.A.; Martínez-Aragón, I.; Guerrero-Arias, R.E.; García-Zura, D.A.; González-Sánchez, L.E. Influence of occlusal stabilization splints and soft occlusal splints on the electromyographic pattern, in basal state and at the end of six weeks treatment in patients with bruxism. Acta Odontol. Latinoam. 2011, 24, 66–74. [Google Scholar] [PubMed]
- Kalman, L. Preliminary investigation of a novel mouthguard. Int. J. Prev. Med. 2018, 9, 60. [Google Scholar] [CrossRef] [PubMed]
- Tiernan, S.; Meagher, A.; O’Sullivan, D.; O’Kelly, E. Finite element simulation of head impacts in mixed martial arts. Comput. Methods Biomech. Biomed. Engin. 2021, 24, 278–288. [Google Scholar] [CrossRef]
- Gialain, I.O.; Coto, N.P.; Driemeier, L.; Noritomi, P.Y.; Dias, R.B.E. A three-dimensional finite element analysis of the sports mouthguard. Dent. Traumatol. 2016, 32, 409–415. [Google Scholar] [CrossRef]
- Toma, M.; Chan-Akeley, R.; Lipari, C.; Kuo, S.-H. Mechanism of coup and contrecoup injuries induced by a knock-out punch. Math. Comput. Appl. 2020, 25, 22. [Google Scholar]
- Campaner, L.M.; Silveira, M.P.M.; de Andrade, G.S.; Borges, A.L.S.; Bottino, M.A.; Dal Piva, A.M.d.O.; Lo Giudice, R.; Ausiello, P.; Tribst, J.P.M. Influence of polymeric restorative materials on the stress distribution in posterior fixed partial dentures: 3D finite element analysis. Polymers 2021, 13, 758. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, H.; Inaba, R.; Iwata, H. Biting force and physical fitness in athletes. Nihon Eiseigaku Zasshi 1994, 49, 654–659. [Google Scholar] [CrossRef]
- Ono, Y.; Tanaka, Y.; Sako, K.; Tanaka, M.; Fujimoto, J. Association between sports-related concussion and mouthguard use among college sports players: A case-control study based on propensity score matching. Int. J. Environ. Res. Public Health 2020, 17, 4493. [Google Scholar] [CrossRef] [PubMed]
- Di Giorgio, G.; Salucci, A.; Sfasciotti, G.L.; Iaculli, F.; Bossù, M. External root resorption management of an avulsed and reimplanted central incisor: A case report. Dent. J. 2021, 9, 72. [Google Scholar] [CrossRef]
- Murri Dello Diago, A.; Apponi, R.; Colombini, V.; Mordini, L.; Ideo, F. Complex implant-prosthetic rehabilitation following sports trauma with 14 years of follow-up: Case report. Dent. J. 2021, 9, 6. [Google Scholar] [CrossRef]
- Kim, H.-N.; Kwon, Y.-B.; Jun, E.-J.; Kim, J.-B. Health-risk behavior-, mental health-, and physical exercise-related risk factors for tooth fractures in Korean adolescents. Int. J. Environ. Res. Public Health 2020, 17, 7815. [Google Scholar] [CrossRef]
- Hayashi, K.; Churei, H.; Tanabe, G.; Togawa, K.; Chowdhury, R.U.; Ueno, T. Improving the wearing rate of mouthguards in the youth rugby category affects the total future mouthguard wearing rate. Dent. J. 2020, 8, 77. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Bando, Y. Effect of model height and model position on forming table on mouthguard thickness in thermoforming using circular frame. Mater. Sci. Appl. 2021, 12, 197–206. [Google Scholar] [CrossRef]
- Paterson, N.T.; Gorham, D.A.; Matela, R.; Moffatt, J.E.; Greasley, A. A finite element study of the mechanics of sports mouthguards. Sports Eng. 2004, 7, 182–195. [Google Scholar]
- Sánchez-Avila, M.B.; Gutmann, J.L.; Navas-Barrantes, E.; Leal-Fernández, M.C.; Mejía-Morales, S. Management of external replacement root resorption in a tooth with a history of avulsion. In Endodontic Practice Today; Quintessence Publishing Company Inc.: Batavia, IL, USA, 2020. [Google Scholar]
- Bergman, L.; Milardović Ortolan, S.; Žarković, D.; Viskić, J.; Jokić, D.; Mehulić, K. Prevalence of dental trauma and use of mouthguards in professional handball players. Dent. Traumatol. 2017, 33, 199–204. [Google Scholar] [CrossRef]
- Sarao, S.K.; Rattai, J.; Levin, L. Dental trauma among hockey players: Preventive measures, compliance and injury types. J. Can. Dent. Assoc. 2021, 87, l8. [Google Scholar] [PubMed]
- Gholampour, S.; Gholampour, H.; Khanmohammadi, H. Finite element analysis of occlusal splint therapy in patients with bruxism. BMC Oral Health 2019, 19, 205. [Google Scholar] [CrossRef]
- Gribov, D.; Antonik, M.; Butkov, D.; Stepanov, A.; Antonik, P.; Kharakh, Y.; Pivovarov, A.; Arutyunov, S. Personalized biomechanical analysis of the mandible teeth behavior in the treatment of masticatory muscles parafunction. J. Funct. Biomater. 2021, 12, 23. [Google Scholar] [CrossRef]
- Rovira-Wilde, A.; Longridge, N.; McKernon, S. Management of severe traumatic intrusion in the permanent dentition. BMJ Case Rep. 2021, 14, e235676. [Google Scholar] [CrossRef] [PubMed]
- Biagi, R.; Bardini, G.; Guidazzi, G.; Spinas, E. Conservative Non-Surgical Management of Horizontal Root-Fractured Maxillary Incisors in a Young Male with Angle Class II, Division 2, Malocclusion. Dent. J. 2021, 9, 55. [Google Scholar] [CrossRef] [PubMed]
- Messias, A.; Gomes, I.J.; Reis, P.N.B.; Amaro, A.M.; Neto, M.A. The Effectiveness of Dental Protection and the Material Arrangement in Custom-Made Mouthguards. Appl. Sci. 2021, 11, 9363. [Google Scholar] [CrossRef]
- Zaman, I.; Rozlan, S.A.M.; Manshoor, B.; Ngali, M.Z.; Khalid, A.; Amin, N.A.M. Study of mouthguard design for endurance and air-flow intake. IOP Conf. Ser. Mater. Sci. Eng. 2017, 226, 012007. [Google Scholar] [CrossRef]
- Silva, C.A.G.D.; Grossi, M.L.; Araldi, J.C.; Corso, L.L. Can hard and/or soft occlusal splints reduce the bite force transmitted to the teeth and temporomandibular joint discs? A finite element method analysis. Cranio 2020, 1–8. [Google Scholar] [CrossRef]
- Noh, K.-T.; Kim, I.-H.; Roh, H.-S.; Kim, J.-Y.; Woo, Y.-H.; Kwon, K.-R.; Choi, D.-G. Finite element analysis of the effects of a mouthguard on stress distribution of facial bone and skull under mandibular impacts. J. Korean Acad. Prosthodont. 2012, 50, 217. [Google Scholar] [CrossRef][Green Version]
- Burgos-Flórez, F.J.; Garzón-Alvarado, D.A. Stress and strain propagation on infant skull from impact loads during falls: A finite element analysis. Int. biomech. 2020, 7, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Szarek, A.; Paszta, P. Possibilities of the Manufacturing and Simulation of the Load on a Customised Mouthguard Used in Combat Sports. Fibres Text. East. Eur. 2020, 2, 110–118. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material/Structure | Elastic Modulus (MPa) | Poisson Ratio |
|---|---|---|
| Enamel | 84.100 | 0.30 |
| Dentin | 18.600 | 0.30 |
| Bone tissue | 13.700 | 0.30 |
| Ethylene vinyl acetate | 18 | 0.30 |
| Polycarbonate | 2.200 | 0.30 |
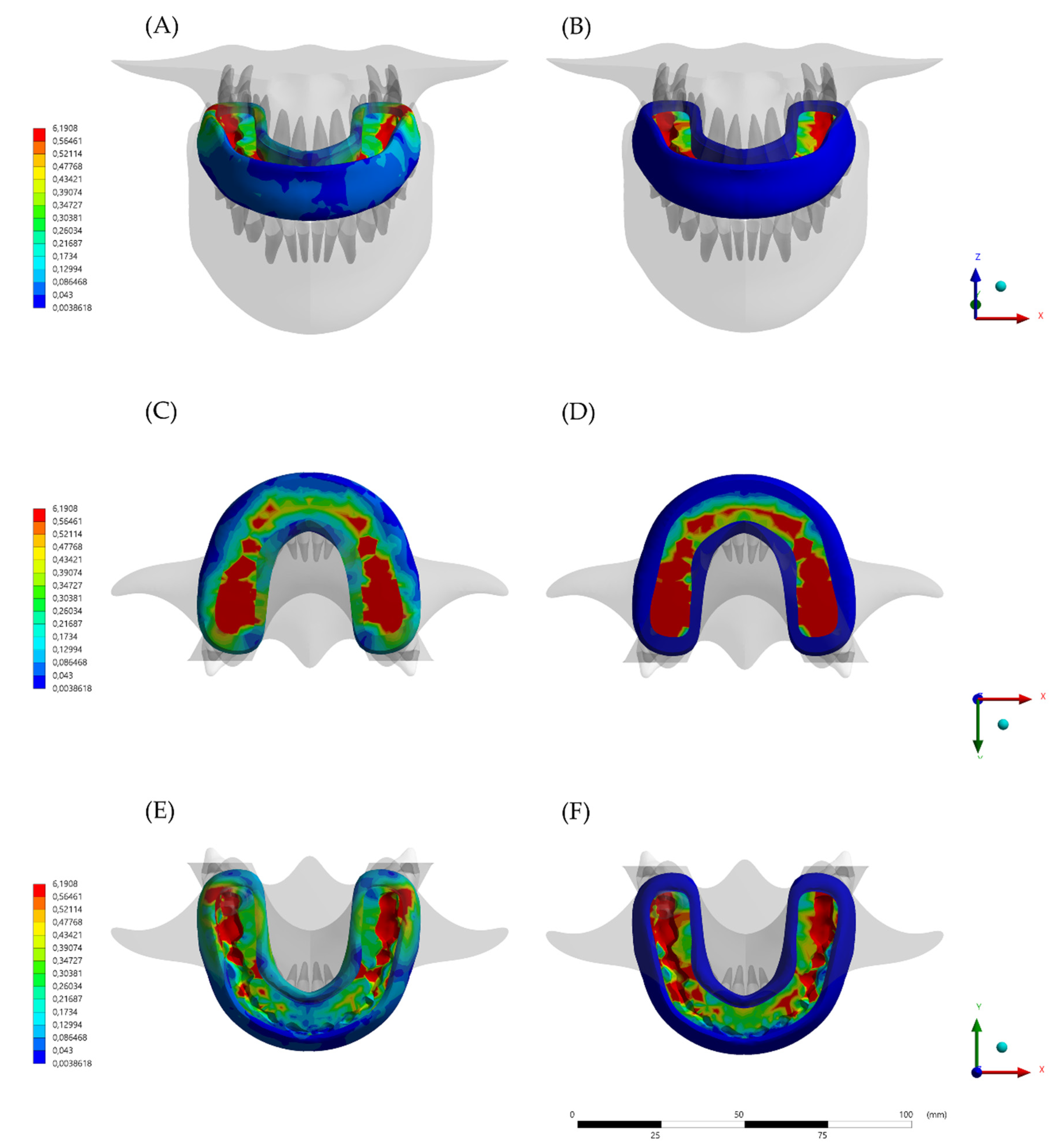
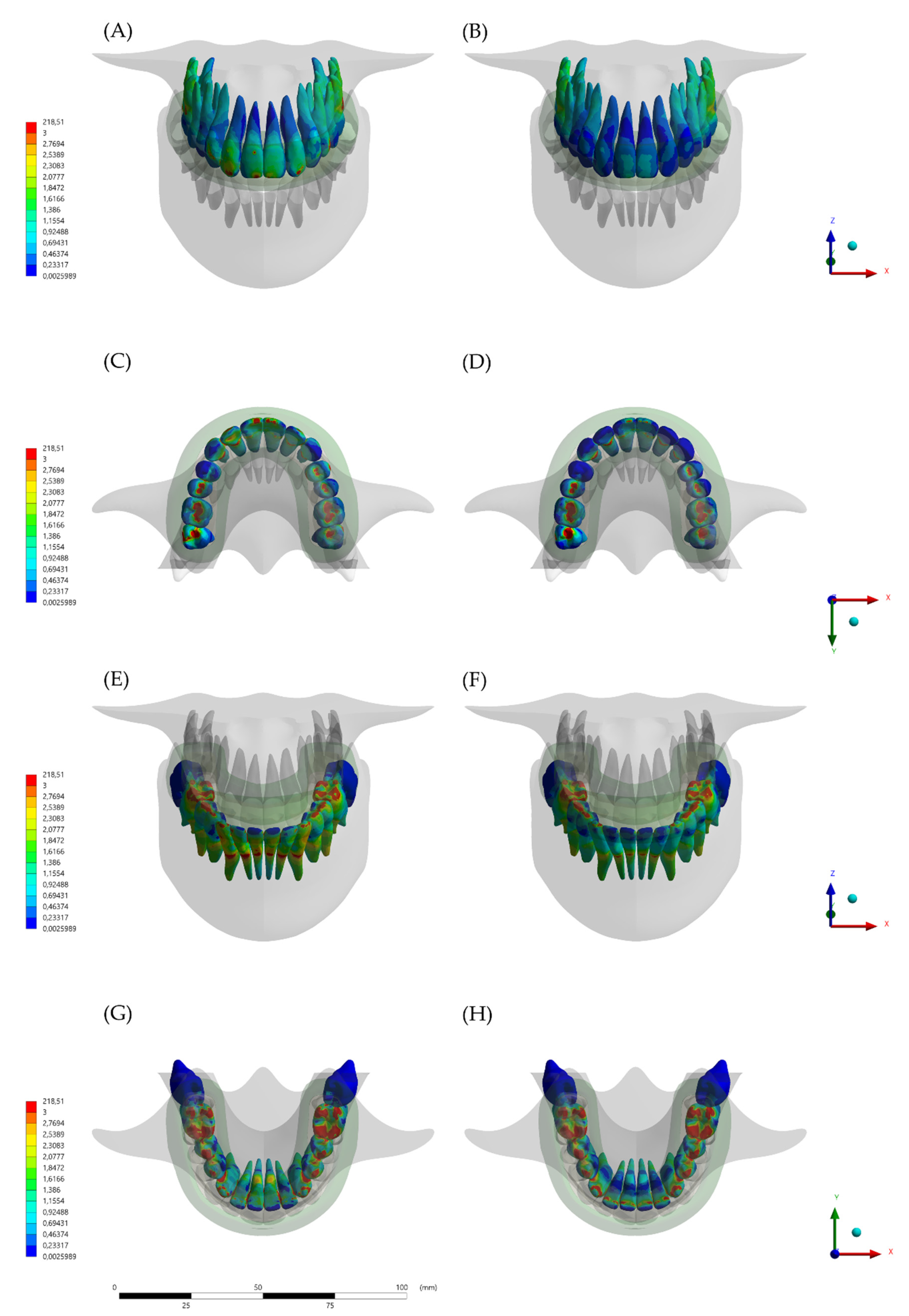
| Model | Jaw Displacement (mm) | Mouthguard Deformation (mm) | Stress at MG Occlusal Surface (MPa) | Stress at MG Axial Flanges (MPa) |
|---|---|---|---|---|
| Conventional mouthguard (MG) | 2.45 | 0.1 | 7.05 | 0.02 |
| Hybrid occlusal splint mouthguard (HMG) | 0.03 | 0.01 | 6.19 | 3.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalman, L.; Dal Piva, A.M.d.O.; de Queiroz, T.S.; Tribst, J.P.M. Biomechanical Behavior Evaluation of a Novel Hybrid Occlusal Splint-Mouthguard for Contact Sports: 3D-FEA. Dent. J. 2022, 10, 3. https://doi.org/10.3390/dj10010003
Kalman L, Dal Piva AMdO, de Queiroz TS, Tribst JPM. Biomechanical Behavior Evaluation of a Novel Hybrid Occlusal Splint-Mouthguard for Contact Sports: 3D-FEA. Dentistry Journal. 2022; 10(1):3. https://doi.org/10.3390/dj10010003
Chicago/Turabian StyleKalman, Les, Amanda Maria de Oliveira Dal Piva, Talita Suelen de Queiroz, and João Paulo Mendes Tribst. 2022. "Biomechanical Behavior Evaluation of a Novel Hybrid Occlusal Splint-Mouthguard for Contact Sports: 3D-FEA" Dentistry Journal 10, no. 1: 3. https://doi.org/10.3390/dj10010003
APA StyleKalman, L., Dal Piva, A. M. d. O., de Queiroz, T. S., & Tribst, J. P. M. (2022). Biomechanical Behavior Evaluation of a Novel Hybrid Occlusal Splint-Mouthguard for Contact Sports: 3D-FEA. Dentistry Journal, 10(1), 3. https://doi.org/10.3390/dj10010003