Optical Diagnostics in Herpetic Keratitis


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Herpetic Keratitis Pathophysiology
3.2. Characteristics and Diagnostic Challenges
3.3. Anterior Segment Optical Coherence Tomography
3.4. Clinical Application of AS-OCT in HSV Infection
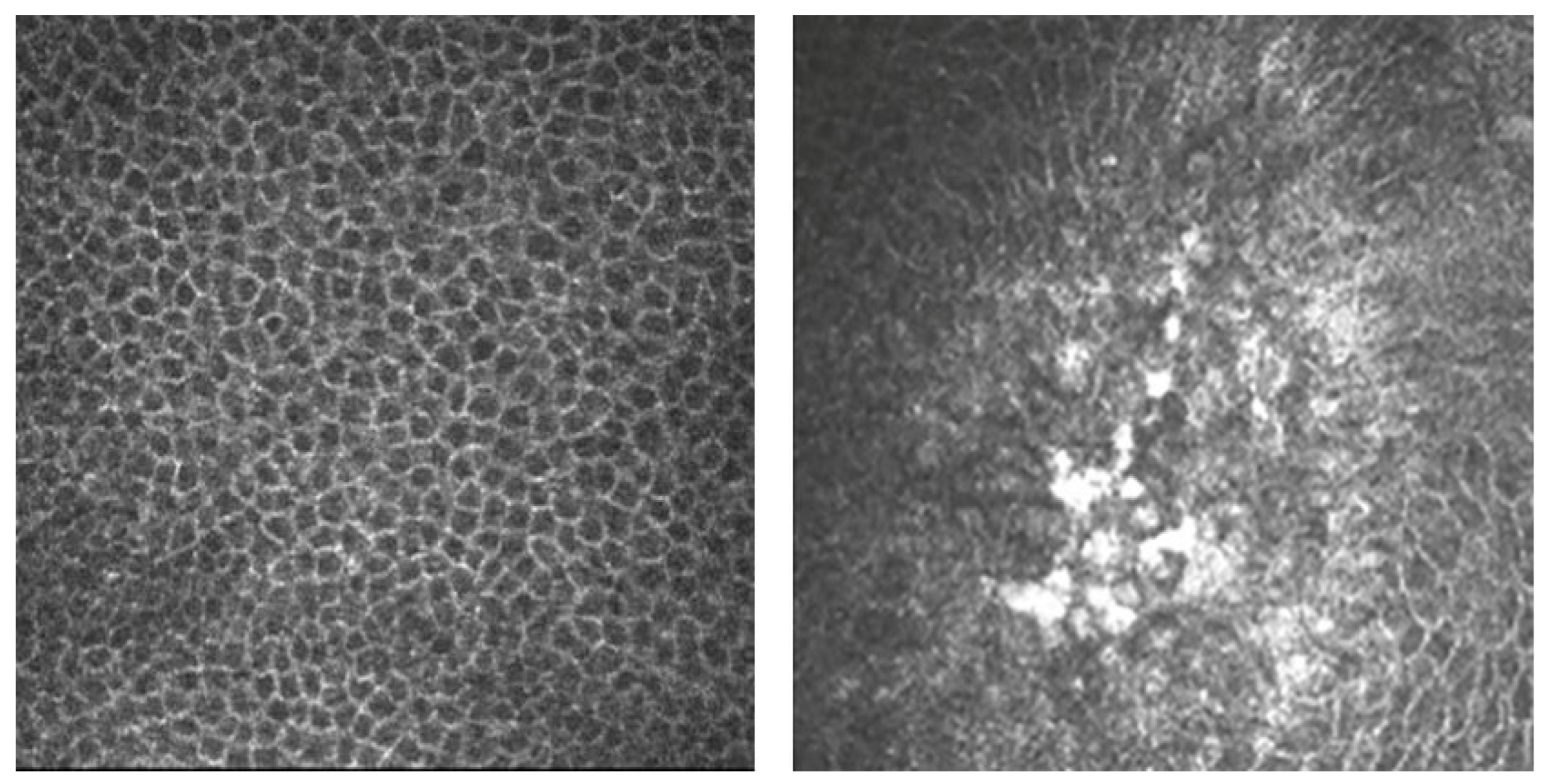
3.5. In Vivo Confocal Microscopy
3.6. In Vivo Confocal Microscopy Clinical Applications
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liesegang, T.J. Herpes Simplex Virus Epidemiology and Ocular Importance. Cornea 2001, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- McQuillan, G.; Kruszon-Moran, D.; Flagg, E.W.; Paulose-Ram, R. Prevalence of Herpes Simplex Virus Type 1 and Type 2 in Persons Aged 14–49: United States, 2015–2016; NCHS Data Brief: Hyattsville, MD, USA, 2018; pp. 1–8. [Google Scholar]
- Farooq, A.V.; Shukla, D. Herpes Simplex Epithelial and Stromal Keratitis: An Epidemiologic Update. Surv. Ophthalmol. 2012, 57, 448–462. [Google Scholar] [CrossRef] [PubMed]
- Borkar, D.S.; Gonzales, J.A.; Tham, V.M.; Esterberg, E.; Vinoya, A.C.; Parker, J.V.; Uchida, A.; Acharya, N.R. Association between Atopy and Herpetic Eye Disease: Results from the Pacific Ocular Inflammation Study. JAMA Ophthalmol. 2014, 132, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Gonzalez, L.A.; Molina-Prat, N.; Doctor, P.; Tauber, J.; Sainz de la Maza, M.T.; Foster, C.S. Clinical Features and Presentation of Infectious Scleritis from Herpes Viruses: A Report of 35 Cases. Ophthalmology 2012, 119, 1460–1464. [Google Scholar] [CrossRef] [PubMed]
- Roozbahani, M.; Hammersmith, K.M. Management of Herpes Simplex Virus Epithelial Keratitis. Curr. Opin. Ophthalmol. 2018, 29, 360–364. [Google Scholar] [CrossRef]
- Arshad, S.; Petsoglou, C.; Lee, T.; Al-Tamimi, A.; Carnt, N.A. 20 Years since the Herpetic Eye Disease Study: Lessons, Developments and Applications to Clinical Practice. Clin. Exp. Optom. 2021, 104, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Rowe, A.M.; St Leger, A.J.; Jeon, S.; Dhaliwal, D.K.; Knickelbein, J.E.; Hendricks, R.L. Herpes Keratitis. Prog. Retin. Eye Res. 2013, 32, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Liesegang, T.J. Classification of Herpes Simplex Virus Keratitis and Anterior Uveitis. Cornea 1999, 18, 127–143. [Google Scholar] [CrossRef] [PubMed]
- Giménez, F.; Suryawanshi, A.; Rouse, B.T. Pathogenesis of Herpes Stromal Keratitis—A Focus on Corneal Neovascularization. Prog. Retin. Eye Res. 2013, 33, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Ohashi, Y. Corneal Endotheliitis. Semin. Ophthalmol. 2008, 23, 235–240. [Google Scholar] [CrossRef]
- Azher, T.N.; Yin, X.-T.; Tajfirouz, D.; Huang, A.J.; Stuart, P.M. Herpes Simplex Keratitis: Challenges in Diagnosis and Clinical Management. Clin. Ophthalmol. 2017, 11, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Carnt, N.; Robaei, D.; Minassian, D.C.; Dart, J.K.G. Acanthamoeba Keratitis in 194 Patients: Risk Factors for Bad Outcomes and Severe Inflammatory Complications. Br. J. Ophthalmol. 2018, 102, 1431–1435. [Google Scholar] [CrossRef] [PubMed]
- Subhan, S.; Jose, R.J.; Duggirala, A.; Hari, R.; Krishna, P.; Reddy, S.; Sharma, S. Diagnosis of Herpes Simplex Virus-1 Keratitis: Comparison of Giemsa Stain, Immunofluorescence Assay and Polymerase Chain Reaction. Curr. Eye Res. 2004, 29, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical Coherence Tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [PubMed]
- Stachs, O.; Guthoff, R.F.; Aumann, S. In Vivo Confocal Scanning Laser Microscopy. In High Resolution Imaging in Microscopy and Ophthalmology: New Frontiers in Biomedical Optics; Bille, J.F., Ed.; Springer: Cham, Switzerland, 2019; ISBN 978-3-030-16637-3. [Google Scholar]
- Petroll, W.M.; Robertson, D.M. In Vivo Confocal Microscopy of the Cornea: New Developments in Image Acquisition, Reconstruction, and Analysis Using the HRT-Rostock Corneal Module. Ocul. Surf. 2015, 13, 187–203. [Google Scholar] [CrossRef]
- Patel, D.V.; McGhee, C.N.J. Contemporary in Vivo Confocal Microscopy of the Living Human Cornea Using White Light and Laser Scanning Techniques: A Major Review. Clin. Exp. Ophthalmol. 2007, 35, 71–88. [Google Scholar] [CrossRef]
- Darougar, S.; Wishart, M.S.; Viswalingam, N.D. Epidemiological and Clinical Features of Primary Herpes Simplex Virus Ocular Infection. Br. J. Ophthalmol. 1985, 69, 2–6. [Google Scholar] [CrossRef]
- Shoji, J.; Sakimoto, T.; Inada, N.; Kamei, Y.; Matsubara, M.; Takamura, E.; Sawa, M. A Diagnostic Method for Herpes Simplex Keratitis by Simultaneous Measurement of Viral DNA and Virus-Specific Secretory IgA in Tears: An Evaluation. Jpn. J. Ophthalmol. 2016, 60, 294–301. [Google Scholar] [CrossRef]
- Austin, A.; Lietman, T.; Rose-Nussbaumer, J. Update on the Management of Infectious Keratitis. Ophthalmology 2017, 124, 1678–1689. [Google Scholar] [CrossRef]
- Chang, E.J.; Dreyer, E.B. Herpesvirus Infections of the Anterior Segment. Int. Ophthalmol. Clin. 1996, 36, 17–28. [Google Scholar] [CrossRef]
- Tabery, H.M. Epithelial Changes in Early Primary Herpes Simplex Virus Keratitis. Photomicrographic Observations in a Case of Human Infection. Acta Ophthalmol. Scand. 2000, 78, 706–709. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, N.; Nishida, K.; Adachi, W.; Tei, M.; Honma, Y.; Dota, A.; Sotozono, C.; Yokoi, N.; Yamamoto, S.; Kinoshita, S. Detection of Herpes Simplex Virus DNA in Atypical Epithelial Keratitis Using Polymerase Chain Reaction. Br. J. Ophthalmol. 1999, 83, 957–960. [Google Scholar] [CrossRef] [PubMed]
- El-Aal, A.M.A.; Sayed, M.E.; Mohammed, E.; Ahmed, M.; Fathy, M. Evaluation of Herpes Simplex Detection in Corneal Scrapings by Three Molecular Methods. Curr. Microbiol. 2006, 52, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Satpathy, G.; Mishra, A.K.; Tandon, R.; Sharma, M.K.; Sharma, A.; Nayak, N.; Titiyal, J.S.; Sharma, N. Evaluation of Tear Samples for Herpes Simplex Virus 1 (HSV) Detection in Suspected Cases of Viral Keratitis Using PCR Assay and Conventional Laboratory Diagnostic Tools. Br. J. Ophthalmol. 2011, 95, 415–418. [Google Scholar] [CrossRef]
- Reidy, J.J.; American Academy of Ophthalmology. External Disease and Cornea; American Academy of Ophthalmology: San Francisco, CA, USA, 2011. [Google Scholar]
- Kaye, S.; Choudhary, A. Herpes Simplex Keratitis. Prog. Retin. Eye Res. 2006, 25, 355–380. [Google Scholar] [CrossRef]
- Olsen, T.W.; Hardten, D.R.; Meiusi, R.S.; Holland, E.J. Linear Endotheliitis. Am. J. Ophthalmol. 1994, 117, 468–474. [Google Scholar] [CrossRef]
- McGilligan, V.; Moore, J.E.; Tallouzi, M.; Atkinson, S.D.; O’Neill, H.; Feeney, S.; Novitskaya, E.S.; Sharma, A.; Shah, S.; Jackson, J.A.; et al. A Comparison of the Clinical and Molecular Diagnosis of Herpes Simplex Keratitis. Open J. Ophthalmol. 2014, 4, 65–74. [Google Scholar] [CrossRef]
- Wilhelmus, K.R. Antiviral Treatment and Other Therapeutic Interventions for Herpes Simplex Virus Epithelial Keratitis. Cochrane Database Syst. Rev. 2015, 1, CD002898. [Google Scholar] [CrossRef]
- Kowalski, R.P.; Gordon, Y.J.; Romanowski, E.G.; Araullo-Cruz, T.; Kinchington, P.R. A Comparison of Enzyme Immunoassay and Polymerase Chain Reaction with the Clinical Examination for Diagnosing Ocular Herpetic Disease. Ophthalmology 1993, 100, 530–533. [Google Scholar] [CrossRef]
- Ramos, J.L.B.; Li, Y.; Huang, D. Clinical and Research Applications of Anterior Segment Optical Coherence Tomography—A Review. Clin. Exp. Ophthalmol. 2009, 37, 81–89. [Google Scholar] [CrossRef]
- Han, S.B.; Liu, Y.-C.; Noriega, K.M.; Mehta, J.S. Applications of Anterior Segment Optical Coherence Tomography in Cornea and Ocular Surface Diseases. J. Ophthalmol. 2016, 2016, 4971572. [Google Scholar] [CrossRef] [PubMed]
- van Velthoven, M.E.J.; Faber, D.J.; Verbraak, F.D.; van Leeuwen, T.G.; de Smet, M.D. Recent Developments in Optical Coherence Tomography for Imaging the Retina. Prog. Retin. Eye Res. 2007, 26, 57–77. [Google Scholar] [CrossRef] [PubMed]
- Jancevski, M.; Foster, C.S. Anterior Segment Optical Coherence Tomography. Semin. Ophthalmol. 2010, 25, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Xia, X.; Tian, B.; Zhou, S. Comparison of Fourier-Domain and Time-Domain Optical Coherence Tomography in the Measurement of Thinnest Corneal Thickness in Keratoconus. J. Ophthalmol. 2015, 2015, 402925. [Google Scholar] [CrossRef]
- Choma, M.; Sarunic, M.; Yang, C.; Izatt, J. Sensitivity Advantage of Swept Source and Fourier Domain Optical Coherence Tomography. Opt. Express 2003, 11, 2183. [Google Scholar] [CrossRef]
- Wang, S.B.; Cornish, E.E.; Grigg, J.R.; McCluskey, P.J. Anterior Segment Optical Coherence Tomography and Its Clinical Applications. Clin. Exp. Optom. 2019, 102, 195–207. [Google Scholar] [CrossRef]
- Gupta, N.; Varshney, A.; Ramappa, M.; Basu, S.; Romano, V.; Acharya, M.; Gaur, A.; Kapur, N.; Singh, A.; Shah, G.; et al. Role of AS-OCT in Managing Corneal Disorders. Diagnostics 2022, 12, 918. [Google Scholar] [CrossRef]
- Soliman, W.; Nassr, M.A.; Abdelazeem, K.; Al-Hussaini, A.K. Appearance of Herpes Simplex Keratitis on Anterior Segment Optical Coherence Tomography. Int. Ophthalmol. 2019, 39, 2923–2928. [Google Scholar] [CrossRef]
- Park, Y.M.; Lee, J.S.; Yoo, J.-M.; Park, J.M.; Seo, S.-W.; Chung, I.-Y.; Kim, S.J. Comparison of Anterior Segment Optical Coherence Tomography Findings in Acanthamoeba Keratitis and Herpetic Epithelial Keratitis. Int. J. Ophthalmol. 2018, 11, 1416–1420. [Google Scholar] [CrossRef]
- Hixson, A.; Blanc, S.; Sowka, J. Monitoring Keratitis Resolution with Optical Coherence Tomography. Optom. Vis. Sci. 2014, 91, S40–S45. [Google Scholar] [CrossRef]
- Lu, L.; Palioura, S. Management of Stromal Herpes Simplex Virus Keratitis With Epithelial Ulceration Using Optical Coherence Tomography-Generated Corneal Thickness Maps. Cornea 2020, 39, 1566–1570. [Google Scholar] [CrossRef] [PubMed]
- Minsky, M. Memoir on Inventing the Confocal Scanning Microscope. Scanning 1988, 10, 128–138. [Google Scholar] [CrossRef]
- Petráň, M.; Hadravský, M.; Egger, M.D.; Galambos, R. Tandem-Scanning Reflected-Light Microscope*. J. Opt. Soc. Am. 1968, 58, 661. [Google Scholar] [CrossRef]
- Lemp, M.A.; Dilly, P.N.; Boyde, A. Tandem-Scanning (Confocal) Microscopy of the Full-Thickness Cornea. Cornea 1985, 4, 205–209. [Google Scholar] [CrossRef]
- McLaren, J.W.; Nau, C.B.; Kitzmann, A.S.; Bourne, W.M. Keratocyte Density: Comparison of Two Confocal Microscopes. Eye Contact Lens. 2005, 31, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Svishchev, G. Microscope for the Study of Transparent Light-Scattering Objects in Incident Light. Opt. Spectrosc. 1969, 30, 188–191. [Google Scholar]
- Masters, B.R.; Thaer, A.A. In-Vivo Real-Time Confocal Microscopy of the Human Cornea. In Proceedings of the Ophthalmic Technologies III, Los Angeles, CA, USA, 24 June 1993; Volume 1877, pp. 100–121. [Google Scholar]
- Mustonen, R.K.; McDonald, M.B.; Srivannaboon, S.; Tan, A.L.; Doubrava, M.W.; Kim, C.K. Normal Human Corneal Cell Populations Evaluated by in Vivo Scanning Slit Confocal Microscopy. Cornea 1998, 17, 485–492. [Google Scholar] [CrossRef]
- Harrison, D.A.; Joos, C.; Ambrósio, R. Morphology of Corneal Basal Epithelial Cells by in Vivo Slit-Scanning Confocal Microscopy. Cornea 2003, 22, 246–248. [Google Scholar] [CrossRef]
- Matsuda, H. Electron Microscopic Study on the Corneal Nerve with Special Reference to Its Endings. Jpn. J. Ophthalmol. 1968, 12, 163–173. [Google Scholar]
- Popper, M.; Morgado, A.M.; Quadrado, M.J.; Best, J.A. van Corneal Cell Density Measurement in Vivo by Scanning Slit Confocal Microscopy: Method and Validation. ORE 2004, 36, 270–276. [Google Scholar] [CrossRef]
- Hollingsworth, J.; Perez-Gomez, I.; Mutalib, H.A.; Efron, N. A Population Study of the Normal Cornea Using an in Vivo, Slit-Scanning Confocal Microscope. Optom. Vis. Sci. 2001, 78, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Poon, S.H.L.; Wong, W.H.L.; Lo, A.C.Y.; Yuan, H.; Chen, C.-F.; Jhanji, V.; Chan, Y.K.; Shih, K.C. A Systematic Review on Advances in Diagnostics for Herpes Simplex Keratitis. Surv. Ophthalmol. 2021, 66, 514–530. [Google Scholar] [CrossRef] [PubMed]
- Yokogawa, H.; Kobayashi, A.; Mori, N.; Sugiyama, K. Mapping of Dendritic Lesions in Patients with Herpes Simplex Keratitis Using in Vivo Confocal Microscopy. Clin. Ophthalmol. 2015, 9, 1771–1777. [Google Scholar] [CrossRef]
- Nagasato, D.; Araki-Sasaki, K.; Kojima, T.; Ideta, R.; Dogru, M. Morphological Changes of Corneal Subepithelial Nerve Plexus in Different Types of Herpetic Keratitis. Jpn. J. Ophthalmol. 2011, 55, 444–450. [Google Scholar] [CrossRef]
- Rosenberg, M.E.; Tervo, T.M.T.; Müller, L.J.; Moilanen, J.A.O.; Vesaluoma, M.H. In Vivo Confocal Microscopy after Herpes Keratitis. Cornea 2002, 21, 265–269. [Google Scholar] [CrossRef]
- Mocan, M.C.; Irkec, M.; Mikropoulos, D.G.; Bozkurt, B.; Orhan, M.; Konstas, A.G.P. In Vivo Confocal Microscopic Evaluation of the Inflammatory Response in Non-Epithelial Herpes Simplex Keratitis. Curr. Eye Res. 2012, 37, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Zhivov, A.; Stave, J.; Vollmar, B.; Guthoff, R. In Vivo Confocal Microscopic Evaluation of Langerhans Cell Density and Distribution in the Corneal Epithelium of Healthy Volunteers and Contact Lens Wearers. Cornea 2007, 26, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Hamrah, P.; Cruzat, A.; Dastjerdi, M.H.; Zheng, L.; Shahatit, B.M.; Bayhan, H.A.; Dana, R.; Pavan-Langston, D. Corneal Sensation and Subbasal Nerve Alterations in Patients with Herpes Simplex Keratitis: An in Vivo Confocal Microscopy Study. Ophthalmology 2010, 117, 1930–1936. [Google Scholar] [CrossRef]
- Wang, Y.E.; Tepelus, T.C.; Vickers, L.A.; Baghdasaryan, E.; Gui, W.; Huang, P.; Irvine, J.A.; Sadda, S.; Hsu, H.Y.; Lee, O.L. Role of in Vivo Confocal Microscopy in the Diagnosis of Infectious Keratitis. Int. Ophthalmol. 2019, 39, 2865–2874. [Google Scholar] [CrossRef]
- Fox, P.D.; Khaw, P.T.; McBride, B.W.; McGill, J.I.; Ward, K.A. Tear and Serum Antibody Levels in Ocular Herpetic Infection: Diagnostic Precision of Secretory IgA. Br. J. Ophthalmol. 1986, 70, 584–588. [Google Scholar] [CrossRef]
- Ma, J.-X.; Wang, L.-N.; Zhou, R.-X.; Yu, Y.; Du, T.-X. Real-Time Polymerase Chain Reaction for the Diagnosis of Necrotizing Herpes Stromal Keratitis. Int. J. Ophthalmol. 2016, 9, 682–686. [Google Scholar] [CrossRef]
- Graiver, D.A.; Saunders, S.E.; Topliff, C.L.; Kelling, C.L.; Bartelt-Hunt, S.L. Ethidium Monoazide Does Not Inhibit RT-PCR Amplification of Nonviable Avian Influenza RNA. J. Virol. Methods 2010, 164, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.; Chan, P.K.S.; Hui, D.S.C.; Rainer, T.H.; Wong, E.; Choi, K.-W.; Lui, G.C.Y.; Wong, B.C.K.; Wong, R.Y.K.; Lam, W.-Y.; et al. Viral Loads and Duration of Viral Shedding in Adult Patients Hospitalized with Influenza. J. Infect. Dis. 2009, 200, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Mahlum, C.E.; Haugerud, S.; Shivers, J.L.; Rossow, K.D.; Goyal, S.M.; Collins, J.E.; Faaberg, K.S. Detection of Bovine Viral Diarrhea Virus by TaqMan Reverse Transcription Polymerase Chain Reaction. J. Vet. Diagn. Investig. 2002, 14, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Shimomura, Y.; Fukuda, M.; Miyazaki, D.; Ohashi, Y.; Sasaki, H.; Tagawa, Y.; Shiota, H.; Inada, N.; Okamoto, S.; et al. Multicentre Clinical Study of the Herpes Simplex Virus Immunochromatographic Assay Kit for the Diagnosis of Herpetic Epithelial Keratitis. Br. J. Ophthalmol. 2013, 97, 1108–1112. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Jiang, D.; Tang, K.; Chen, W. Current Clinical Applications of Anterior Segment Optical Coherence Tomography Angiography: A Review. Graefes Arch. Clin. Exp. Ophthalmol. 2023. [Google Scholar] [CrossRef]
- Patel, D.V.; Zhang, J.; McGhee, C.N.J. In Vivo Confocal Microscopy of the Inflamed Anterior Segment: A Review of Clinical and Research Applications. Clin. Exp. Ophthalmol. 2019, 47, 334–345. [Google Scholar] [CrossRef]
- Kumar, R.L.; Cruzat, A.; Hamrah, P. Current State of in Vivo Confocal Microscopy in Management of Microbial Keratitis. Semin. Ophthalmol. 2010, 25, 166–170. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | N Eyes | AS OCT Finding |
|---|---|---|
| Soliman et al. [41] | 11 | Stromal haze without epithelial defect |
| 14 | Sub-epithelial haze, diffuse stromal infiltrates, corneal epithelium cystic spaces | |
| 10 | Hyper-reflective stroma associated with epithelial defects | |
| 3 | Stromal condensation with intact epithelium | |
| 3 | Stromal condensation and thinning with overlying epithelial defect | |
| 1 | Localized stromal and endothelial thickening.Epithelial heaping at the edge of epithelial defect | |
| Young Ming Park et al. [42] | 3 | Subepithelial highly reflective lesions, corneal epithelial irregularity |
| Hixson et al. [43] | 2 | To locate and assess corneal thickness to manage the follow up and treatment of corneal edema |
| Louise et al. [44] | 2 | Pachymetric and corneal epithelial maps to assess stromal inflammation for diagnostic purposes and treatment follow up |
| Authors | N Eyes | ICVM |
|---|---|---|
| Yokugawa et al. [57] | 4 | Hyperreflective irregular epithelial cells surrounded by elongated epithelial cells. Langerhans cells within the epithelium and nerve plexus |
| Rosenberg et al. [59] | 10 | Highly reflective dendritic structures in the basal epithelium |
| Mocan et al. [60] | 11 | Infiltration of basal epithelial layers with inflammatory cells |
| 20 | Stromal inflammation evidence: round-shaped, with hyperreflective nuclei, smaller than keratocytes, surrounded by microdeposits | |
| 18 | Keratic precipitates (KPs): in 11 eyes, small round KPs; in 9, globular KPs; in 8, dendritiform KPs | |
| 17 | Endothelial blebs as hyporeflective dark spaces between endothelial cells | |
| 19 | Alteration in the sub-basal plexus: attenuated in 9 eyes, not visible in 10 eyes | |
| Hamrah et al. [62] | 32 | Lower mean nerve density, total nerve number, main nerve trunks, and number of branches |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Staso, F.; Rullo, D.; Di Pippo, M.; Di Staso, S.; Abdolrahimzadeh, S. Optical Diagnostics in Herpetic Keratitis. Photonics 2023, 10, 349. https://doi.org/10.3390/photonics10040349
Di Staso F, Rullo D, Di Pippo M, Di Staso S, Abdolrahimzadeh S. Optical Diagnostics in Herpetic Keratitis. Photonics. 2023; 10(4):349. https://doi.org/10.3390/photonics10040349
Chicago/Turabian StyleDi Staso, Federico, Daria Rullo, Mariachiara Di Pippo, Silvio Di Staso, and Solmaz Abdolrahimzadeh. 2023. "Optical Diagnostics in Herpetic Keratitis" Photonics 10, no. 4: 349. https://doi.org/10.3390/photonics10040349
APA StyleDi Staso, F., Rullo, D., Di Pippo, M., Di Staso, S., & Abdolrahimzadeh, S. (2023). Optical Diagnostics in Herpetic Keratitis. Photonics, 10(4), 349. https://doi.org/10.3390/photonics10040349