Abstract
A sensitive, simple, and fast liquid chromatography–tandem mass spectrometry (LC–MS/MS) bioanalytical method was developed to determine remifentanil in human plasma and prevent its instability by esterases during quantification. A 20 μL sample of human plasma, acidified with formic acid, was precipitated using 100 μL of acetonitrile. Chromatography was carried out on an Agilent Poroshell 120 EC-C18 column (4.6 × 50 mm, 2.7 μm) with an isocratic elution by acetonitrile and distilled water containing 0.1% formic acid (65:35, v/v) at a flow rate of 0.5 mL/min. Transition ions were detected as m/z 377.10→113.20 and m/z 277.00→111.00 for remifentanil and chlorpropamide (internal standard), respectively, with positive electrospray ionization in mass spectrometry. The run time was only 3 min per sample. We evaluated the selectivity, linearity, carry-over, accuracy, precision, extraction recovery, absolute matrix effect, stability, and incurred sample reanalysis and found that all these parameters were within acceptable limits. The calibration curve range for remifentanil was 0.05–50 ng/mL with regression coefficient (r) values higher than 0.9939. Given the simple and fast sample preparation and the lower LLOQ concentration compared to those in other methods, this method was successfully used to quantify plasma levels after intravenous infusion of remifentanil to intensive-care-unit patients during extracorporeal membrane oxygenation.
1. Introduction
Remifentanil, which belongs to the fentanyl family comprising fentanyl, sufentanil, and alfentanil, is a highly potent agonist that acts on the μ–opioid receptors. Remifentanil as a general anesthesia drug has been employed alone or in combination with a hypnotic agent for sedation, analgesia, and anesthesia [1]. While remifentanil shares similar pharmacodynamic properties with other members of the fentanyl family, its pharmacokinetic properties are unique [2]. Remifentanil has a lower pKa (pKa 7.26) value than the physiological pH value, which causes it to exist in a non-ionized circulation. Consequently, it rapidly penetrates the blood–brain barrier, leading to a rapid equilibrium between the plasma and the effect site and achieving a rapid onset time (1–1.5 min) [1,2]. Along with the rapid onset time, remifentanil is also characterized by rapid elimination, indicated by a short context-sensitive half-time. Context-sensitive half-time refers to the time needed for the drug’s plasma concentration to decrease by 50% after stopping an intravenous infusion. Unlike other fentanyl family members such as alfentanil (47.3 min) and fentanyl (180 min), remifentanil has been observed to have a very short (3.2 min) context-sensitive half-time, even with a prolonged infusion duration [2,3,4]. The ester structure of remifentanil is responsible for its distinctive properties, allowing for rapid hydrolysis into remifentanil acid, which is significantly less potent than the parent compound (approximately 1/800 to 1/2000 times less) [5]. The hydrolysis process of remifentanil is mediated via nonspecific blood, plasma, and tissue esterases [1,2,3,4,5]. Consequently, pharmacokinetic properties of remifentanil have been observed to be independent of hepatic [6,7] or renal impairment [7,8,9]. This organ-independent metabolism of remifentanil allows it to be used in intensive-care-unit (ICU) patients with varying degrees of organ dysfunction, such as renal or hepatic impairment [6,10].
Opioid analgesics commonly cause respiratory depression, and the onset of opioid-induced respiratory depression occurs at plasma concentration levels required to detect changes in an electroencephalogram [2]. Furthermore, the therapeutic window for analgesic effects is 1–40 ng/mL following an infusion rate of 0.04–2 μg/kg body weight per minute [10]. Therefore, the development of a robust and sensitive bioanalytical assay is crucial for clinical effective usage of remifentanil. Additionally, a rapid-throughput analytical method is necessary to minimize hydrolysis by esterases during sample collection [11]. Various methods have been published for remifentanil quantification; the instrument and sample information are briefly compared in Table 1 [12,13,14,15,16,17,18,19,20,21,22,23,24]. In sample preparation, most previous methods required a large volume of plasma, long run time, and complex methods for remifentanil extraction from plasma, such as liquid–liquid extraction (LLE), solid-phase extraction (SPE), or microextraction by packed sorbent (MEPS).

Table 1.
Comparison of bioanalytical methods for remifentanil quantification.
This study aimed to develop a sensitive and robust LC–MS/MS bioanalytical method with a simple sample preparation for remifentanil quantification. Compared with previously published methods, this present assay demonstrates exceptional performance with the following advantages: minimal sample volume requirement (20 μL of plasma), simple sample preparation, high sensitivity with a low lower limit of quantification (LLOQ; 0.05 ng/mL), and a wide calibration range (0.05–50 ng/mL), which enables comprehensive analysis across different time–concentration profiles. Furthermore, we employed a straightforward method to stabilize remifentanil in plasma. We effectively utilized this assay to quantify plasma levels of remifentanil in ICU patients who underwent extracorporeal membrane oxygenation (ECMO).
2. Materials and Methods
2.1. Chemicals and Reagents
Remifentanil was supplied by Toronto Research Chemicals (North York, ON, Canada). Chlorpropamide for the internal standard (IS) and formic acid were purchased from Sigma-Aldrich (St. Louis, MO, USA). HPLC-grade methanol and acetonitrile were products of Burdick & Jackson (Morristown, NJ, USA). The other reagents employed in this study were of the highest purity. Ultrapure water was produced from distilled water using the Milli-Q Plus System (Millipore, Bedford, MA, USA). K2-EDTA human plasma including hemolytic and lipemic human plasma were obtained from individual donors at Yonsei Severance Hospital (Seoul, Republic of Korea).
2.2. LC–MS/MS System
Plasma samples were quantified using an LCMS–8050 triple-quadrupole mass spectrometer coupled with a Nexera X2 UHPLC system; a system controller, CBM–20A; a degasser, DGU–20A5R; an autosampler, SIL–30AC; and an oven, CTO–20A (Shimadzu Co., Ltd., Kyoto, Japan). An electrospray ionization source was equipped in the positive mode [M + H]+. For chromatographic separation, an Agilent Poroshell 120 EC-C18 column (4.6 × 50 mm, 2.7 μm) with an isocratic elution composed of acetonitrile and 0.1% formic acid in distilled water (65:35, v/v) was used at a flow rate of 0.5 mL/min.
The autosampler tray and column oven temperatures were set at 4 °C and 40 °C during the LC–MS/MS analysis. The injection volume was 5 μL and the analysis time was 3 min per sample.
The selected reaction monitoring (SRM) conditions were set as follows: drying and nebulizing gas flow rates, 10.0 and 3.0 L/min, respectively; interface voltage, 4.0 kV; heat block temperature, 400 °C; desolvation line temperature, 200 °C; collision-induced dissociation argon gas pressure, 270 kPa; and detector voltage, 1.8 kV. The collision energies and dwell times were set at –29 V and 100 ms for remifentanil and –20 V and 150 ms for IS, respectively. The SRM transitions of m/z 377.10 > 113.20 for remifentanil and m/z 277.00 > 111.00 for IS were used as quantitative analysis. Data acquisition and processing were carried out using LabSolutions software (version 5.6, Shimadzu, Japan).
2.3. Calibration Standard and Quality Control (QC) Samples
Remifentanil and chlorpropamide (IS) stock solutions were dissolved in methanol to concentrations of 1 mg/mL each. Then, IS stock solution for routine use was diluted in acetonitrile containing 0.1% formic acid at 1 μg/mL. The working solutions of remifentanil to make calibration standards and QC samples were diluted in methanol serially from the stock solution. Calibration curves and QC samples were prepared by spiking 1 μL of appropriate working solutions into 19 μL blank human plasma. The ranges of seven calibration curves were 0.05, 0.1, 0.2, 1, 5, 10, and 50 ng/mL for remifentanil. The QC samples of remifentanil were separately made at four levels: 0.05 (lower limit of quantification; LLOQ), 0.15 (low QC), 3 (medium QC), and 40 ng/mL (high QC). For each analysis batch, we utilized freshly made calibration standards and QCs. All stock and working solutions were kept in the freezer for storage (at –80 °C).
2.4. Sample Preparation
To prevent the hydrolysis of remifentanil, EDTA plasma was pre-treated with the addition of formic acid (1.5 μL of formic acid/1 mL of plasma), as described previously [12,25]. A 20 µL aliquot of human plasma acidified with formic acid and a 100 µL IS solution (0.1% formic acid in acetonitrile containing 1 µg/mL of chlorpropamide) were added into a 1.5 mL Eppendorf tube, vortexed for 10 min, and then centrifuged at 13,000× g for 10 min at 4 °C. The clean supernatant was put into an LC–MS/MS vial, and 5 µL was injected into the apparatus for analysis.
2.5. Validation of the Method
Validation of the current method was conducted, ensuring compliance with the acceptance criteria outlined in the US FDA industrial guidance for the bioanalytical method validation [26].
2.5.1. Selectivity
The selectivity was evaluated by analyzing eight different batches of blank (remifentanil-free) human plasma samples including one each of lipemic and hemolytic plasma. There were no interfering peaks in retention times of remifentanil (0.93 min) and IS (1.4 min) at the LLOQ level.
2.5.2. Linearity and Sensitivity
Calibration curves were established with the range of 0.05–50 ng/mL encompassing double-blank samples (without remifentanil and IS) and zero-blank (without remifentanil). The linearity of the calibration curve was determined using linear regression analysis, employing various weighting factors (1/x, 1/x2, and none). This analysis was performed by plotting the peak area ratio (y) of remifentanil to that of the IS versus the nominal concentration (x). The established calibration curve exhibited a high regression coefficient (r) of 0.99 or higher. The back-calculated concentrations of the calibration curves and QC samples should meet the accuracy acceptance criteria (85–115%). The LLOQ of remifentanil was determined as the lowest concentration on the calibration curve, giving a signal-to-noise ratio above 10, with acceptable accuracy (80–120%) and precision (≤20%), which were proved by analyzing ten replicates.
2.5.3. Carry-Over
Carry-over was assessed by injecting two double-blank plasma samples directly after injection of the upper-limit-of-quantitation (ULOQ) sample. The acceptable carry-over in the blank sample was no interfering peaks appearing with areas <20% of the LLOQ and <5% for the IS peak area at respective retention times.
2.5.4. Accuracy and Precision
The inter-day accuracy and precision were investigated by measuring ten replicates of four different QCs (0.05, 0.15, 3, and 40 ng/mL) during five different days (two replicates per day), while intra-day accuracy and precision were analyzed by six replicates of four different QCs on the same day. The precision was determined by the relative standard deviation (RSD, %), and the accuracy was calculated as the relative error (RE, %) = [(calculated concentration − spiked concentration)/spiked concentration] × 100. The concentrations of QC samples with LLOQ samples were determined from the standard calibration curve and analyzed on the same day. The acceptance criterion was a ±15% deviation from the normal value except at the LLOQ, which should not be less than ±20%.
2.5.5. Extraction Recovery and Absolute Matrix Effects
Extraction recoveries of remifentanil were evaluated by the percentage ratio of the peak areas of extracted QC samples (A) and post-extraction plasma blanks spiked (B) at the mentioned concentrations at three QC levels. The extraction recovery (%) was defined as B/A × 100% [27].
The absolute matrix effect was tested by measuring eight batches of human plasma, including lipemic and hemolytic plasma, at three QC levels. To determine absolute matrix effects on the ionization, the peak areas of post-extraction-spiked plasma (B) at a concentration of three QCs were compared with the standard solution (C) by direct injection. The extraction recovery and matrix effect of IS at 1 μg/mL were tested in a similar way. The absolute matrix effect was defined as B/C × 100% [27].
2.5.6. Stability
The stock solution of remifentanil was stored at –80 °C and was also assessed after one month. It was considered stable if the RSD and RE values of the peak response were ≤10% compared with those of the freshly prepared stock solution.
In human plasma, the stabilities of remifentanil were assessed at three QCs (n = 6, at each level) under the four following conditions: (1) bench-top stability (3 h at room temperature), (2) long-term storage (4 months at −80 °C), (3) three freeze–thaw cycles, and (4) processed sample stability (autosampler stability; 24 h at 4 °C). The stability was assessed by comparing the QC samples with freshly prepared calibration standards and QC samples. If the deviation fell within ±15.0%, it was considered stable.
2.5.7. Incurred Sample Analysis (ISR)
Incurred samples were reanalyzed to demonstrate the reliability of the present assay and support the accuracy and precision. The initial and repeat analyses were processed separately using the validated bioanalytical method. The re-measured concentration of incurred plasma samples should be within 20% of their original concentration to verify the method’s reliability and the absence of back-conversion of metabolites or variability in the plasma samples during processing and storage.
2.6. Clinical Samples
Plasma was obtained from patients who consented to participate in this clinical study. The study was conducted according to the Declaration of Helsinki and approved by the Severance Hospital Institutional Review Board (IRB no. 4-2014-0919), registered as a clinical trial registration number (NCT02581280).
Adult ICU patients were administered remifentanil (Ultiva®, GlaxoSmithKline, Brentford, UK) by intravenous infusion, and the infusion rate was maintained at 0.35 mg/h. Blood samples were collected 8, 24, and 48 h after the onset of intravenous infusion, while the patient was on ECMO. Blood samples, immediately put on an ice bath after collection, were obtained using an EDTA-coated vacutainer. Subsequently, blood samples were centrifuged at 4 °C as previously mentioned in Section 2.4 [12,25]. The obtained plasma samples were kept at –80 °C before further use.
3. Results and Discussion
3.1. LC–MS/MS Condition
To optimize mass conditions, 50 ng/mL of remifentanil in methanol was directly infused into the mass spectrometer’s ESI conditions. Remifentanil and the IS yielded a better spectrometric response in positive-ionization electrospray ionization. Figure 1 shows MS/MS spectra of remifentanil and the IS. Final mass parameters were optimized for high sensitivity of SRM quantification using the automatic tuning tool.
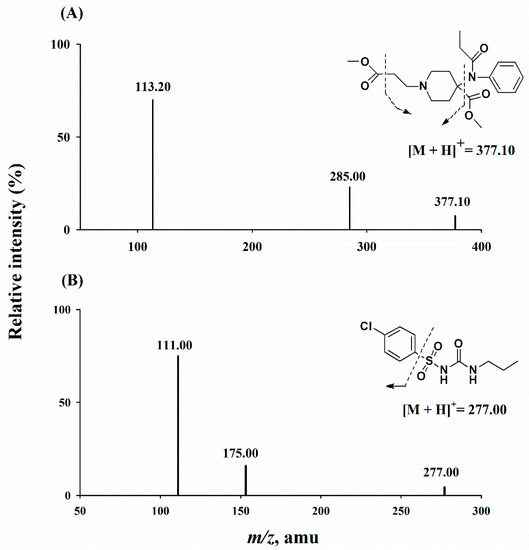
Figure 1.
Precursor ion scans of 377.10 m/z for remifentanil (A) and 277.00 m/z for chlorpropamide (B).
To achieve better optimization of the symmetric peak shapes and appropriate retentions, several columns, including C18 and C8, and various mobile phase compositions were tested. The use of an Agilent Poroshell 120 C18 column (4.6 × 50 mm; 2.7 μm) with an isocratic elution composed of acetonitrile and distilled water including 0.1% formic acid (65:35, v/v) at a flow rate of 0.5 mL/min resulted in a short run time (3 min) and a good peak shape. At the end of each analytical batch, to remove contaminants from a column, the column was flushed with acetonitrile at 1.0 mL/min for at least 30 min, and then re-equilibrated with the current mobile phase for 30 min.
In the early stage, protein precipitation was attempted using methanol and acetonitrile for sample preparation and selected using acetonitrile because of its higher sensitivity and time-saving advantage without evaporation and reconstitution.
The Atmospheric Pressure Chemical Ionization (APCI) condition was attempted to analyze remifentanil because of the possibility of ion suppression in the ESI condition. However, the sensitivity in the APCI condition was too low to analyze remifentanil in human plasma samples. Thus, instead of selecting the APCI condition, chromatographic conditions and sample preparation procedures, such as a decreased plasma volume and modified mobile phase ratio or flow rate, were adjusted to reduce ion suppression.
For bioanalysis with LC–MS/MS, the selection of an ideal IS possessing a suitable retention time, extraction recovery, and minimal matrix effect is crucial for reproducible results. Following these criteria, a stable isotope or a chemical analog of the analyte would be considered the best IS. However, due to instability of remifentanil via endogenous esterases and chemical hydrolysis, many research papers have used stabilizing agents during bioanalysis (Table 1). Therefore, considering the high cost and a long storage period of internal standard stock/or working solution, we did not utilize isotope-labeled remifentanil in this study. In addition, the chemically analog opioid analgesics such as alfentanil or sufentanil, members of the fentanyl family, can be used in combination with remifentanil among critically ill patients in clinics [28,29,30]. In our clinical study, we also have plasma samples from ECMO patients receiving intravenous infusion of remifentanil co-administered with a low dose of sufentanil (patient B). For this reason, several compounds of an optimal IS were investigated with a proper retention time and a similar extent of recovery and matrix effect as remifentanil, and finally chlorpropamide was found to be appropriate in this assay.
3.2. Validation of the Method
3.2.1. Selectivity
Retention times of remifentanil and the IS eluted were 0.93 and 1.38 min, respectively. There were no interfering peaks at elution times of remifentanil and the IS as depicted in Figure 2B. Figure 2 shows typical chromatograms for drug-free human plasma, a plasma sample at LLOQ (0.05 ng/mL), and IS (1 μg/mL).
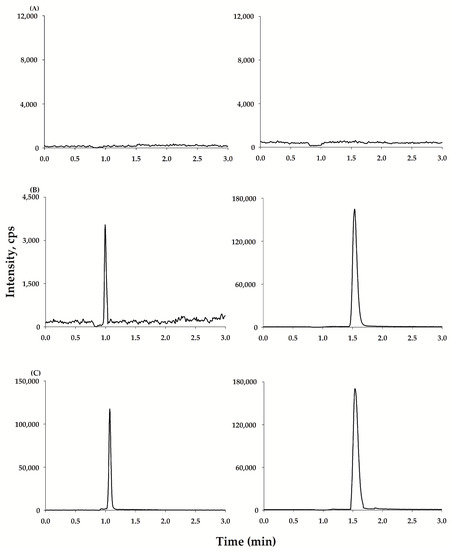
Figure 2.
Typical chromatograms of remifentanil (left) and chlorpropamide (IS, right): (A) blank human plasma; (B) spiked plasma sample at LLOQ (0.05 ng/mL) and the IS (1 μg/mL); and (C) a patient’s plasma at 24 h following intravenous infusion of remifentanil and IS (1 μg/mL).
3.2.2. Linearity and Sensitivity
The calibration curve of remifentanil in human plasma was determined as described in Section 2.5.2. After evaluating the weighting factors (none, 1/x, and 1/x2), it was determined that the regression equation using a weighting factor of 1/x2 provided the best fit with correlation coefficients (r) in the range of 0.9939–0.9981. The representative regression equations for remifentanil calibration curves during the validation were y = 0.022x − 0.000131. The back-calculated results for all calibration standards in human plasma were <5.2% RSD and –2.91 to 7.30% RE. The plasma LLOQ (0.05 ng/mL) was sufficient to measure the plasma concentration of remifentanil in patients with a signal-to-noise ratio above 10.
3.2.3. Carry-Over
No significant peaks (≥20% of the LLOQ and 5% of the IS) related to remifentanil and IS were observed in the chromatogram of double-blank plasma injected after the ULOQ samples.
3.2.4. Precision and Accuracy
The intra- and inter-day precision and accuracy of remifentanil are summarized in Table 2. Seven standard samples of 0.05, 0.1, 0.2, 1, 5, 10, and 50 ng/mL, including four different QC samples (0.05, 0.15, 3, and 40 ng/mL), were evaluated for intra-day and inter-day accuracy and precision. During five different days, the intra-day accuracy (RE, %) and precision (RSD, %) were −1.33 to 4.89% and ≤8.66% for remifentanil, respectively. The inter-day accuracy and precisions were 0.333 to 6.89% and ≤8.47% for remifentanil, respectively. All precision and accuracy results were within the adequate range of 15% without LLOQ (the acceptable range of 20%), indicating that the present method was accurate and precise and met the standard outlined in the U.S. FDA guidance for bioanalytical methods [26].
Table 2.
Intra- and inter-day precision and accuracy for remifentanil.
3.2.5. Extraction Recovery and Absolute Matrix Effects
Table 3 describes the results of extraction recoveries and absolute matrix effects. The extraction recoveries were 101–103% (RSD ≤4.91%) for plasma at three QC levels. The mean extraction recoveries of the IS were 104 ± 4.13%, with an RSD value of 4.13% for plasma. The extraction recoveries of remifentanil and the IS in plasma were consistent and reproducible.
Table 3.
Extraction recoveries and absolute matrix effects for remifentanil (n = 6).
There were no significant matrix effects in all types of matrices including lipemic and hemolyzed plasma (Table 3). The results of absolute matrix effects of remifentanil were 103, 101, and 107% for the three QC levels, and the matrix effect for IS was 100%. This assay did not show the matrix effect and ion suppression or enhancement. Therefore, we safely applied this analysis with consistent, routine recovery and little matrix effect.
3.2.6. Stability
A stock solution of remifentanil was found to be stable after 1 month of storage at −80 °C, exhibiting RSD and RE ≤10% compared with a freshly prepared stock solution; more than 96.1 ± 3.10% of remifentanil was recovered.
The stability tests in human plasma were performed under the four following conditions: bench-top for 3 h, long-term storage for 4 months at –80 °C, three freeze–thaw cycles, and processed sample stability (autosampler stability) for 24 h at 4 °C. Table 4 summarizes the detailed stability results from human plasma. All results were within ±15% compared with freshly prepared plasma samples. As a result, all QC samples for the stability tests met the acceptance criteria (≤15%), indicating adequate stability for storage and analysis.
Table 4.
Stability of remifentanil (n = 6).
3.3. Application to Clinical Samples
The LC–MS/MS method that was developed and validated in this study proved to be effective to measure remifentanil concentration in the plasma of two patients receiving ECMO during intravenous infusion. This analysis was performed from six different samples collected at three time points for each of the two patients. All the concentrations obtained from the patient sample analysis were above the LLOQ and within the calibration range. As shown in Table 5, the plasma concentrations at each time point were 1.39 and 1.16 ng/mL at 8 h, 0.772 and 1.98 ng/mL at 24 h, and 0.0920 and 1.61 ng/mL at 48 h. Although the infusion rate of the two patients was the same, the plasma concentrations were variable because they depended on the patient’s weight, condition, or co-administered drugs. When comparing the difference in the concentration between the initial concentration and the ISR for all tested samples, it was observed that they fell within the acceptance criteria, with a difference of less than 20%. This indicated that the method developed in this study demonstrated good reproducibility.
Table 5.
Remifentanil concentration after intravenous infusion to ECMO patients with re-analysis results.
4. Conclusions
This study aimed to develop a sensitive and robust LC–MS/MS method with a simple sample preparation for remifentanil quantification. Our present method demonstrated exceptional performance, such as using a required small volume of plasma (20 μL), the short run time of each sample (3 min), the highly sensitive LLOQ (0.05 ng/mL), and the simple protein precipitation protocol with protection against hydrolysis. Consequently, this assay was effectively utilized to measure the plasma concentration of remifentanil in ICU patients. This assay is expected to be useful for deciding a suitable dose according to the patient’s condition by adapting this method for routine patient sample analysis.
Author Contributions
Conceptualization, S.U.C., M.J.C. and S.K.B.; methodology, S.U.C., J.S.K., K.L.M. and C.B.L.; software, S.U.C., J.S.K., S.J.J. and C.B.L.; investigation, S.U.C., J.S.K., K.L.M. and C.B.L.; data curation, S.U.C., J.S.K., S.J.J. and C.B.L.; writing—original draft preparation, S.U.C., S.J.J., C.B.L. and S.K.B.; writing—review and editing, M.J.C. and S.K.B.; visualization, S.U.C., S.J.J. and C.B.L.; supervision, S.K.B.; project administration, M.J.C. and S.K.B.; funding acquisition, S.K.B. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by a grant of the Basic Science Research Program through the National Research Foundation of Korea, funded by the Ministry of Education (2018R1A6A1A03025108), and the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health & Welfare (HF20C0002).
Institutional Review Board Statement
The study was conducted according to the Declaration of Helsinki and approved by the Severance Hospital Institutional Review Board (IRB no. 4-2014-0919), registered as a clinical trial registration number (NCT02581280).
Informed Consent Statement
Informed consent was obtained from all patients involved in this study.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank all medical and nursing staffs in the Department of Intensive Care at Yonsei Severance Hospital for supporting this study. We are also grateful to all patients for providing plasma samples during ECMO. The graphical abstract was created with BioRender.com (accessed on 13 June 2023).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Stroumpos, C.; Manolaraki, M.; Paspatis, G.A. Remifentanil, a different opioid: Potential clinical applications and safety aspects. Expert Opin. Drug Saf. 2010, 9, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Beers, R.; Camporesi, E. Remifentanil Update: Clinical science and utility. CNS Drugs 2004, 18, 1085–1104. [Google Scholar] [CrossRef] [PubMed]
- Kapila, A.; Glass, P.S.A.; Jacobs, J.R.; Muir, K.T.; Hermann, D.J.; Shiraishi, M.; Howell, S.; Smith, R.L. Measured Context-sensitive Half-times of Remifentanil and Alfentanil. Anesthesiology 1995, 83, 968–975. [Google Scholar] [CrossRef]
- Michelsen, L.G.; Hug, C.C., Jr. The pharmacokinetics of remifentanil. J. Clin. Anesth. 1996, 8, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Westmoreland, C.L.; Hoke, J.F.; Sebel, P.S.; Hug, C.C.; Muir, K.T. Pharmacokinetics of Remifentanil (GI87084B) and Its Major Metabolite (GI90291) in Patients Undergoing Elective Inpatient Surgery. Anesthesiology 1993, 79, 893–903. [Google Scholar] [CrossRef]
- Dershwitz, M.; Hoke, J.F.; Rosow, C.E.; Michalowski, P.; Connors, P.M.; Muir, K.T.; Dienstag, J. Pharmacokinetics and Pharmacodynamics of Remifentanil in Volunteer Subjects with Severe Liver Disease. Anesthesiology 1996, 84, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Dershwitz, M.; Rosow, C.E. The pharmacokinetics and pharmacodynamics of remifentanil in volunteers with severe hepatic or renal dysfunction. J. Clin. Anesth. 1996, 8, S88–S90. [Google Scholar] [CrossRef]
- Hoke, J.F.; Cunningham, F.; James, M.K.; Muir, K.T.; Hoffman, W.E. Comparative pharmacokinetics and pharmacodynamics of remifentanil, its principle metabolite (GR90291) and alfentanil in dogs. J. Pharmacol. Exp. Ther. 1997, 281, 226–232. [Google Scholar]
- Breen, D.; Wilmer, A.; Bodenham, A.; Bach, V.; Bonde, J.; Kessler, P.; Albrecht, S.; Shaikh, S. Offset of pharmacodynamic effects and safety of remifentanil in intensive care unit patients with various degrees of renal impairment. Crit. Care 2004, 8, R21–R30. [Google Scholar] [CrossRef]
- Pitsiu, M.; Wilmer, A.; Bodenham, A.; Breen, D.; Bach, V.; Bonde, J.; Kessler, P.; Albrecht, S.; Fisher, G.; Kirkham, A. Pharmacokinetics of remifentanil and its major metabolite, remifentanil acid, in ICU patients with renal impairment. Br. J. Anaesth. 2004, 92, 493–503. [Google Scholar] [CrossRef]
- Egan, T.D. Remifentanil Pharmacokinetics and Pharmacodynamics. Clin. Pharmacokinet. 1995, 29, 80–94. [Google Scholar] [CrossRef] [PubMed]
- Koster, R.A.; Vereecke, H.E.M.; Greijdanus, B.; Touw, D.J.; Struys, M.M.R.F.; Alffenaar, J.W.C. Analysis of Remifentanil with Liquid Chromatography-Tandem Mass Spectrometry and an Extensive Stability Investigation in EDTA Whole Blood and Acidified EDTA Plasma. Anesth. Analg. 2015, 120, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- O’hara, K.; Schneider, J.J.; Jones, A.L.; Wright, I.M.R.; Martin, J.; Galettis, P. Development of an UHPLC-MS/MS method for remifentanil quantification in a small plasma volume. J. Liq. Chromatogr. Relat. Technol. 2019, 42, 521–527. [Google Scholar] [CrossRef]
- Bender, J.; Elshout, J.V.D.; Selinger, K.; Broeders, G.; Dankers, J.; van der Heiden, C. Determination of remifentanil in human heparinised whole blood by tandem mass spectrometry with short-column separation. J. Pharm. Biomed. Anal. 1999, 21, 559–567. [Google Scholar] [CrossRef]
- Gergov, M.; Nokua, P.; Vuori, E.; Ojanperä, I. Simultaneous screening and quantification of 25 opioid drugs in post-mortem blood and urine by liquid chromatography–tandem mass spectrometry. Forensic Sci. Int. 2009, 186, 36–43. [Google Scholar] [CrossRef]
- Cooreman, S.; Deprez, C.; Martens, F.; Van Bocxlaer, J.; Croes, K. A comprehensive LC-MS-based quantitative analysis of fentanyl-like drugs in plasma and urine. J. Sep. Sci. 2010, 33, 2654–2662. [Google Scholar] [CrossRef]
- El Hamd, M.A.; Wada, M.; Ikeda, R.; Kawakami, S.; Kuroda, N.; Nakashima, K. Simultaneous determination of propofol and remifentanil in rat plasma by liquid chromatography-tandem mass spectrometry: Application to preclinical pharmacokinetic drug-drug interaction analysis. Biomed. Chromatogr. 2015, 29, 325–327. [Google Scholar] [CrossRef]
- Alvarez, J.C.; Abe, E.; Etting, I.; Le Guen, M.; Devillier, P.; Grassin-Delyle, S. Quantification of remifentanil and propofol in human plasma: A LC–MS/MS assay validated according to the EMA guideline. Bioanalysis 2015, 7, 1675–1684. [Google Scholar] [CrossRef]
- Said, R.; Pohanka, A.; Andersson, M.; Beck, O.; Abdel-Rehim, M. Determination of remifentanil in human plasma by liquid chromatography–tandem mass spectrometry utilizing micro extraction in packed syringe (MEPS) as sample preparation. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2011, 879, 815–818. [Google Scholar] [CrossRef]
- Eckart, K.; Röhrich, J.; Breitmeier, D.; Ferner, M.; Laufenberg-Feldmann, R.; Urban, R. Development of a new multi-analyte assay for the simultaneous detection of opioids in serum and other body fluids using liquid chromatography–tandem mass spectrometry. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2015, 1001, 1–8. [Google Scholar] [CrossRef]
- Selinger, K.; Lanzo, C.; Sekut, A. Determination of remifentanil in human and dog blood by HPLC with UV detection. J. Pharm. Biomed. Anal. 1994, 12, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Haidar, S.H.; Liang, Z.; Selinger, K.; Hamlett, L.; Eddington, N.D. Determination of remifentanil, an ultra-short-acting opioid anesthetic, in rat blood by high performance liquid chromatography with ultraviolet detection. J. Pharm. Biomed. Anal. 1996, 14, 1727–1732. [Google Scholar] [CrossRef] [PubMed]
- Bjorksten, A.R.; Chan, C.; Crankshaw, D.P. Determination of remifentanil in human blood by capillary gas chromatography with nitrogen-selective detection. J. Chromatogr. B 2002, 775, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Grosse, C.; Davis, I.; Arrendale, R.; Jersey, J.; Amin, J. Determination of remifentanil in human blood by liquid-liquid extraction and capillary GC-HRMS-SIM using a deuterated internal standard. J. Pharm. Biomed. Anal. 1994, 12, 195–203. [Google Scholar] [CrossRef]
- Yang, S.; Noh, H.; Hahn, J.; Jin, B.H.; Min, K.L.; Bae, S.K.; Kim, J.; Park, M.S.; Hong, T.; Wi, J.; et al. Population pharmacokinetics of remifentanil in critically ill patients receiving extracorporeal membrane oxygenation. Sci. Rep. 2017, 7, 16276. [Google Scholar] [CrossRef]
- Center of Drug Evaluation and Research; US Food and Drug Administration. Guidance for Industry-Bioanalytical Method Validation. Available online: https://www.fda.gov/media/70858/download (accessed on 9 May 2023).
- Matuszewski, B.K.; Constanzer, M.L.; Chavez-Eng, C.M. Strategies for the Assessment of Matrix Effect in Quantitative Bioanalytical Methods Based on HPLC−MS/MS. Anal. Chem. 2003, 75, 3019–3030. [Google Scholar] [CrossRef]
- Lin, W.; Sun, J.; Fu, S. A small dose of remifentanil pretreatment suppresses sufentanil-induced cough during general anesthesia induction: A randomized, double-blind, placebo-controlled trial. BMC Anesthesiol. 2019, 19, 164. [Google Scholar] [CrossRef]
- Lin, Y.-J.; Wang, Y.-C.; Huang, H.-H.; Huang, C.-H.; Lin, P.-L. Efficacy and safety of remifentanil for endoscopic ultrasound-guided tissue acquisition: A single center retrospective study. Surg. Endosc. 2022, 36, 6516–6521. [Google Scholar] [CrossRef]
- Sneyd, J.; Whaley, A.; Dimpel, H.L.; Andrews, C.J. An open, randomized comparison of alfentanil, remifentanil and alfentanil followed by remifentanil in anaesthesia for craniotomy. Br. J. Anaesth. 1998, 81, 361–364. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).