
Qualitative/Quantitative Analysis of Alcohol and Licit/Illicit Drugs on Post-Mortem Biological Samples from Road Traffic Deaths

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
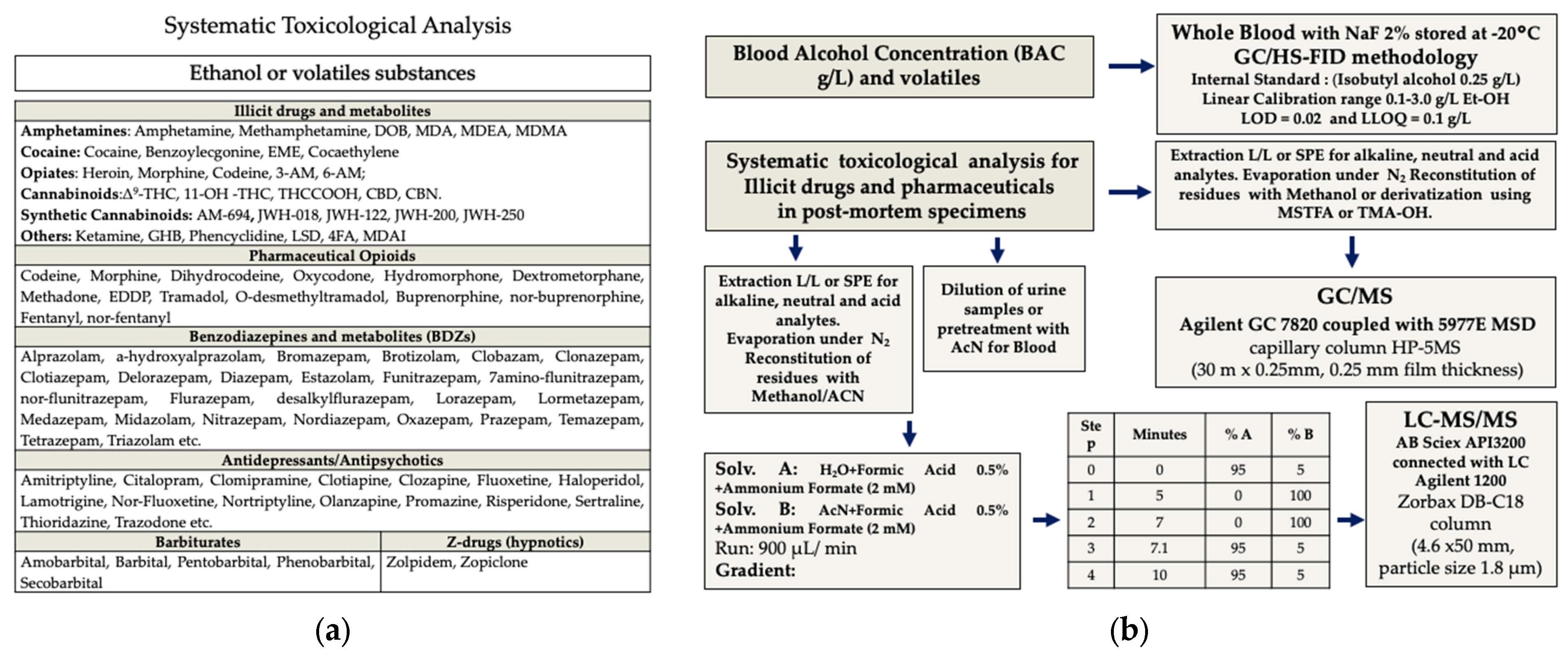
2.2. Sample Collection and Analytical Procedures
2.3. Statistical Analysis
3. Results
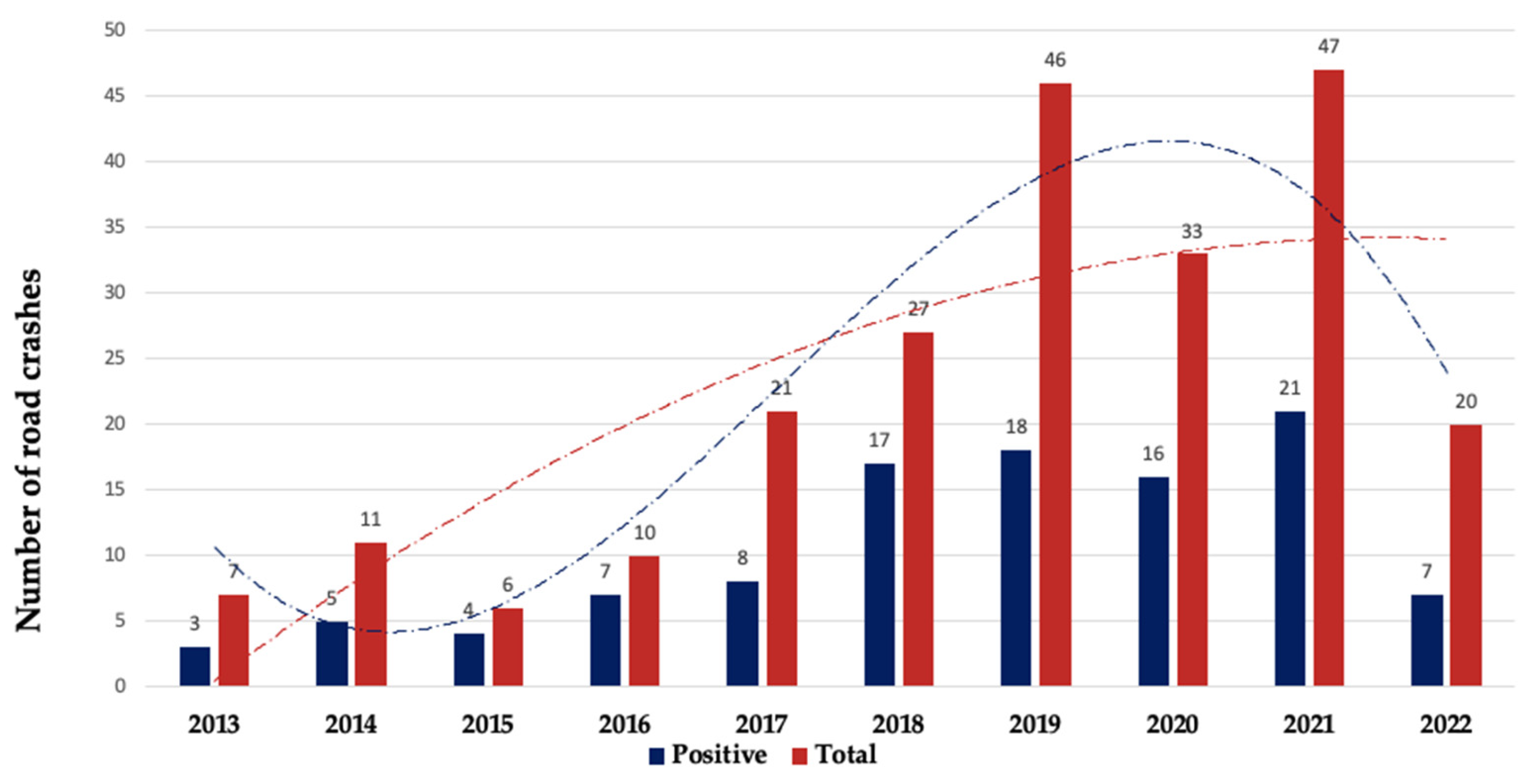
3.1. Characteristics of Fatal Road Accidents
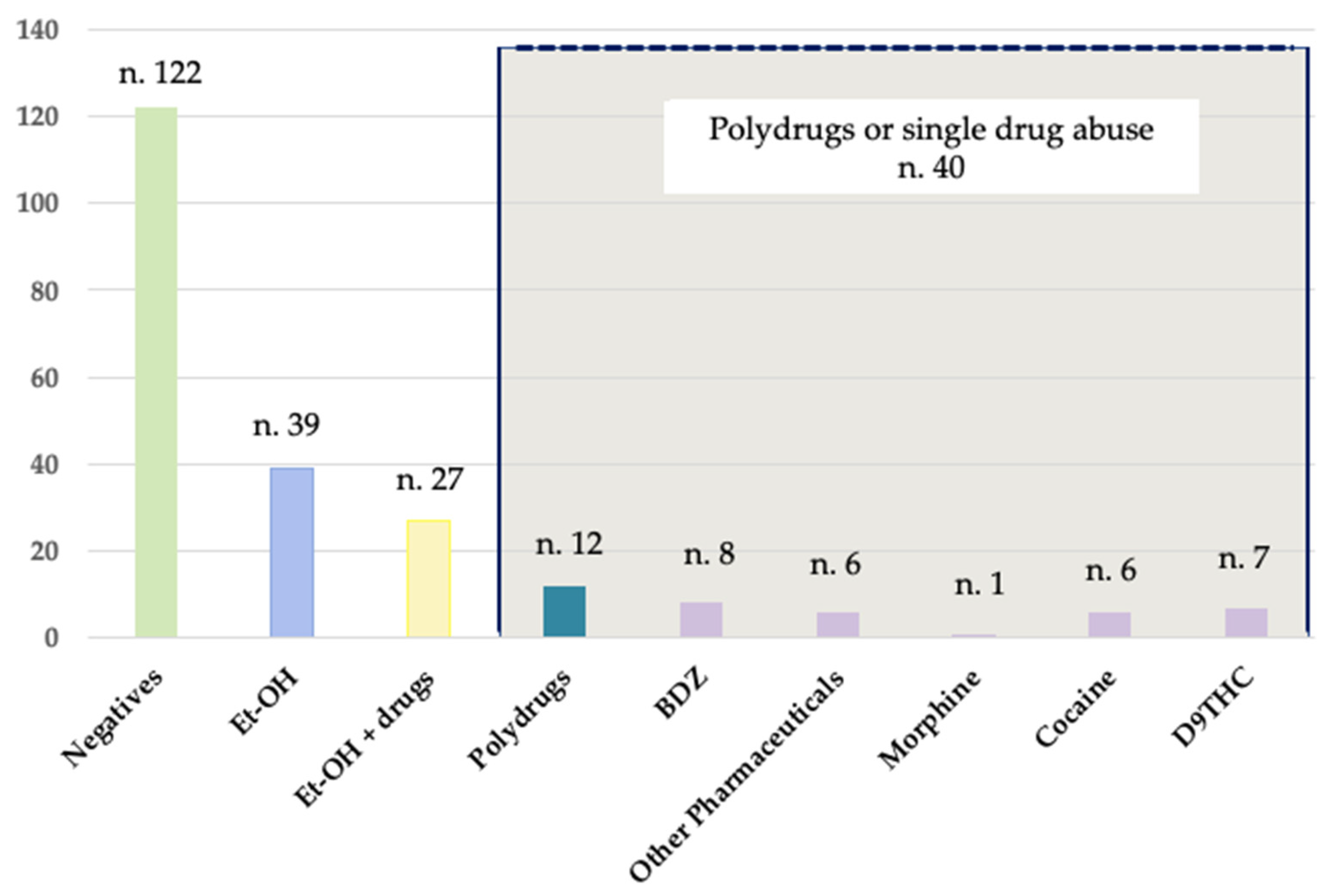
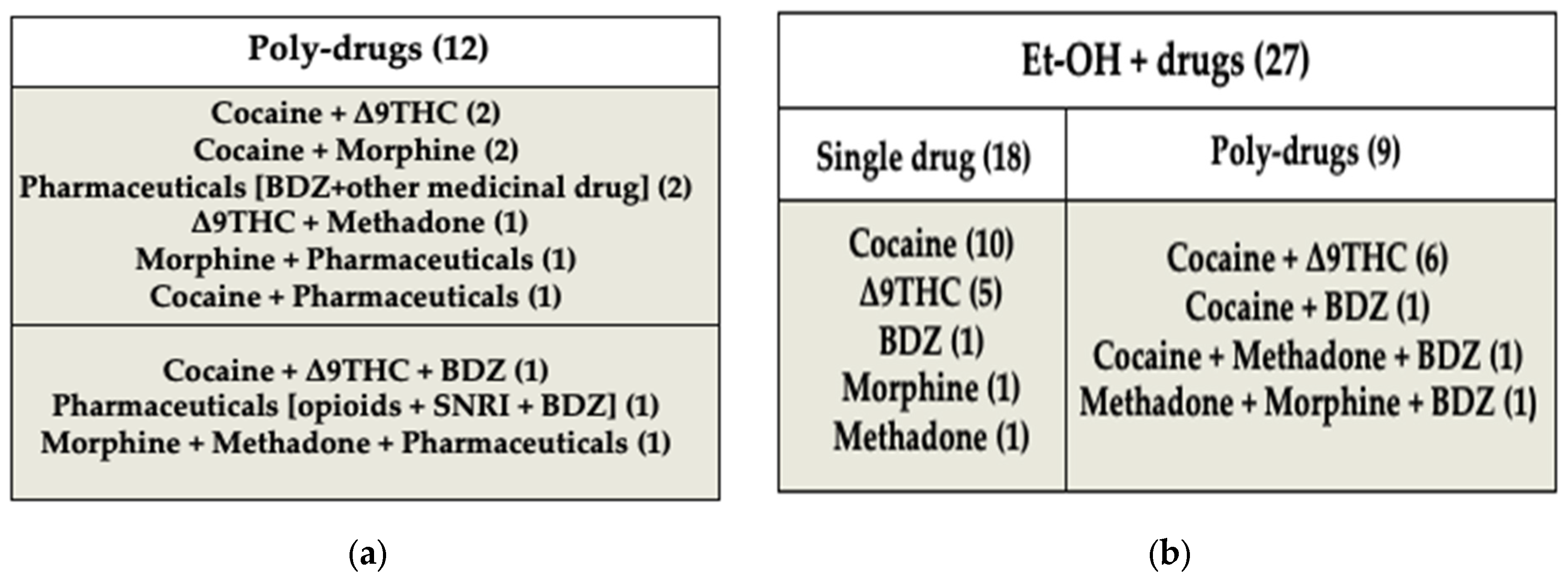
3.2. Toxicological Results: Summary and Further Details
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, W.S.; Wong, G.F.; Hung, C.W.; Wong, Y.N.; Fung, K.M.; Lee, W.K.; Dao, K.L.; Leung, C.W.; Lo, K.M.; Lee, W.M.; et al. Interpol review of toxicology 2016–2019. Forensic Sci. Int. Synerg. 2020, 2, 563–607. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Peregrina, S.; Casares-López, M.; Ortiz, C.; Castro-Torres, J.J.; Martino, F.; Jiménez, J.R. Comparison of the effects of alcohol and cannabis on visual function and driving performance. Does the visual impairment affect driving? Drug Alcohol Depend. 2022, 237, 109538. [Google Scholar] [CrossRef] [PubMed]
- Fares, A.; Wickens, C.M.; Mann, R.E.; Di Ciano, P.; Wright, M.; Matheson, J.; Hasan, O.S.M.; Rehm, J.; George, T.P.; Samokhvalov, A.V.; et al. Combined effect of alcohol and cannabis on simulated driving. Psychopharmacology 2022, 239, 1263–1277. [Google Scholar] [CrossRef] [PubMed]
- Schnakenberg Martin, A.M.; Flynn, L.T.; Sefik, E.; Luddy, C.; Cortes-Briones, J.; Skosnik, P.D.; Pittman, B.; Ranganathan, M.; D’Souza, D.C. Preliminary study of the interactive effects of THC and ethanol on self-reported ability and simulated driving, subjective effects, and cardiovascular responses. Psychopharmacology 2023, 240, 1235–1246. [Google Scholar] [CrossRef] [PubMed]
- Goullé, J.P.; Verstraete, A.; Boulu, R.; Costentin, J.; Foucher, J.P.; Raes, E.; Tillement, J.P. Drogues, médicaments et accidentologie [Illicit drugs, medications and traffic accidents]. In Annales Pharmaceutiques Françaises; Elsevier Masson: Gainesville, FL, USA, 2008; Volume 66, pp. 196–205. [Google Scholar]
- Van der Sluiszen, N.N.; Vermeeren, A.; Verster, J.C.; van de Loo, A.J.A.E.; van Dijken, J.H.; Veldstra, J.L.; Brookhuis, K.A.; de Waard, D.; Ramaekers, J.G. Driving performance and neurocognitive skills of long-term users of benzodiazepine anxiolytics and hypnotics. Hum. Psychopharmacol. 2019, 34, e2715. [Google Scholar] [CrossRef] [PubMed]
- Irwin, C.; Iudakhina, E.; Desbrow, B.; McCartney, D. Effects of acute alcohol consumption on measures of simulated driving: A systematic review and meta-analysis. Accid. Anal. Prev. 2017, 102, 248–266. [Google Scholar] [CrossRef] [PubMed]
- Fares, A.; Wright, M.; Matheson, J.; Mann, R.E.; Stoduto, G.; Le Foll, B.; Wickens, C.M.; Brands, B.; Di Ciano, P. Effects of combining alcohol and cannabis on driving, breath alcohol level, blood THC, cognition, and subjective effects: A narrative review. Exp. Clin. Psychopharmacol. 2022, 30, 1036–1049. [Google Scholar] [CrossRef]
- Wickens, C.M.; Wright, M.; Mann, R.E.; Brands, B.; Di Ciano, P.; Stoduto, G.; Fares, A.; Matheson, J.; George, T.P.; Rehm, J.; et al. Separate and combined effects of alcohol and cannabis on mood, subjective experience, cognition and psychomotor performance: A randomized trial. Prog. Neuropsychopharmacol. Biol. Psychiatry 2022, 118, 110570. [Google Scholar] [CrossRef]
- Van Der Sluiszen, N.N.; Vermeeren, A.; van Dijken, J.H.; J A E van de Loo, A.; Veldstra, J.L.; de Waard, D.; C Verster, J.; A Brookhuis, K.; Ramaekers, J.G. Driving performance and neurocognitive skills of long-term users of sedating antidepressants. Hum. Psychopharmacol. 2021, 36, 1–12. [Google Scholar] [CrossRef]
- Brunnauer, A.; Herpich, F.; Zwanzger, P.; Laux, G. Driving Performance Under Treatment of Most Frequently Prescribed Drugs for Mental Disorders: A Systematic Review of Patient Studies. Int. J. Neuropsychopharmacol. 2021, 24, 679–693. [Google Scholar] [CrossRef]
- Ramaekers, J.G. Antidepressants and driver impairment: Empirical evidence from a standard on-the-road test. J. Clin. Psychiatry 2003, 64, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Judd, L.L. The effect of antipsychotic drugs on driving and driving related psychomotor functions. Accid. Anal. Prev. 1985, 17, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.M.; Wu, E.C.; Chen, C.Y.; Wu, K.Y.; Liang, H.Y.; Chau, Y.L.; Wu, C.S.; Lin, K.M.; Tsai, H.J. Psychotropic drugs and risk of motor vehicle accidents: A population-based case-control study. Br. J. Clin. Pharmacol. 2013, 75, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.E. Benzodiazepine use and motor vehicle accidents. Systematic review of reported association. Can. Fam. Physician 1998, 44, 799–808. [Google Scholar] [PubMed]
- Dassanayake, T.; Michie, P.; Carter, G.; Jones, A. Effects of benzodiazepines, antidepressants and opioids on driving: A systematic review and meta-analysis of epidemiological and experimental evidence. Drug Saf. 2011, 34, 125–156. [Google Scholar] [CrossRef] [PubMed]
- Johnell, K.; Laflamme, L.; Möller, J.; Monárrez-Espino, J. The role of marital status in the association between benzodiazepines, psychotropics and injurious road traffic crashes: A register-based nationwide study of senior drivers in Sweden. PLoS ONE 2014, 9, e86742. [Google Scholar] [CrossRef] [PubMed]
- Skyving, M.; Forsman, Å.; Dukic Willstrand, T.; Laflamme, L.; Möller, J. Medical impairment and road traffic crashes among older drivers in Sweden—A national, population-based, case-control study. Accid. Anal. Prev. 2021, 163, 106434. [Google Scholar] [CrossRef]
- Anzillotti, L.; Dagoli, S.; Calò, L.; Maglietta, G.; Cecchi, R. Road traffic deaths: A retrospective analysis (2009–2019) in the north of the Italian region Emilia Romagna. Traffic Inj. Prev. 2022, 23, 29–33. [Google Scholar] [CrossRef]
- Global Status Report on Road Safety 2018; World Health Organization: Geneva, Switzerland. 2018. Available online: https://www.who.int/publications/i/item/9789241565684 (accessed on 1 October 2023).
- Drinking Driving: A Road Safety Manual for Decision-Makers and Practitioners; Road Safety Partnership, International Federation of Red Cross and Red Crescent Societies: Geneva, Switzerland. 2022. Available online: https://cdn.who.int/media/docs/default-source/documents/health-topics/road-traffic-injuries/ifrc-drink-driving-2022-final.pdf?sfvrsn=f3e09010_6&download=true (accessed on 1 October 2023).
- Rosen, H.E.; Bari, I.; Paichadze, N.; Peden, M.; Khayesi, M.; Monclús, J.; Hyder, A.A. Global road safety 2010–18: An analysis of Global Status Reports. Injury 2022, in press. [Google Scholar] [CrossRef]
- Drunk Driving; National Highway Traffic Safety Administration: Washington, DC, USA. 2021. Available online: https://www.nhtsa.gov/risky-driving/drunk-driving (accessed on 1 October 2023).
- Progress in Reducing Drink-Driving and Other Alcohol-Related Road Deaths in Europe; European Transport Safety Council: Brussels, Belgium. 2022. Available online: https://etsc.eu/progress-in-reducing-drink-driving-and-other-alcohol-related-road-deaths-in-europe/ (accessed on 1 October 2023).
- Cittadini, F.; De Giovanni, N.; Caradonna, L.; Vetrugno, G.; Oliva, A.; Fucci, N.; Zuppi, C.; Pascali, V.L.; Covino, M. Prevalence of alcohol and other drugs in injured drivers and their association with clinical outcomes. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2008–2014. [Google Scholar]
- Incidenti Stradali. Anno 2021. ISTAT (Istituto Nazionale di Statistica). Available online: https://www.istat.it/it/archivio/273324#:~:text=Nel%202021%20sono%202.875%20i,11%2C8%25%20incidenti (accessed on 1 October 2023).
- Carfora, A.; Campobasso, C.P.; Cassandro, P.; Petrella, R.; Borriello, R. Alcohol and drugs use among drivers injured in road accidents in Campania (Italy): A 8-years retrospective analysis. Forensic Sci. Int. 2018, 288, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Linee Guida per Strutture dotate di Laboratori per gli Accertamenti di Sostanze d’Abuso con Finalità Tossicologo-Forensi e Medico-Legali Rev. n. 4, Ital. J. Addict. 2012, 2, 34–47. Available online: https://iris.unipa.it/retrieve/handle/10447/75815/76143/IJA_vol_2_num_5-6.pdf (accessed on 15 November 2023).
- Linee Guida per Strutture dotate di Laboratori per gli Accertamenti di Sostanze d’Abuso con Finalità Tossicologo-Forensi e Medico-Legali Rev. n. 5 of 29 May 2017. Available online: http://www.gtfi.it/wp-content/uploads/2017/06/LG_biologico_revi-sione_2017_29_05.pdf (accessed on 15 November 2023).
- Peters, F.T.; Drummer, O.H.; Musshoff, F. Validation of new methods. Forensic Sci. Int. 2007, 165, 216–224. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER) Center for Veterinary Medicine (CVM) Guidance for Industry for Bioanalytical Method Validation. 2018. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/bioanalytical-method-validation-guidance-industry (accessed on 15 November 2023).
- Domingo-Salvany, A.; Herrero, M.J.; Fernandez, B.; Perez, J.; Del Real, P.; González-Luque, J.C.; de la Torre, R. Prevalence of psychoactive substances, alcohol and illicit drugs, in Spanish drivers: A roadside study in 2015. Forensic Sci. Int. 2017, 278, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Jewett, A.; Peterson, A.B.; Sauber-Schatz, E.K. Exploring substance use and impaired driving among adults aged 21 years and older in the United States, 2015. Traffic Inj. Prev. 2018, 19, 693–700. [Google Scholar] [CrossRef]
- Wiese Simonsen, K.; Steentoft, A.; Bernhoft, I.M.; Hels, T.; Rasmussen, B.S.; Linnet, K. Psychoactive substances in seriously injured drivers in Denmark. Forensic Sci. Int. 2013, 224, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Sewell, R.A.; Poling, J.; Sofuoglu, M. The effect of cannabis compared with alcohol on driving. Am. J. Addict. 2009, 18, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Drummer, O.H. The role of drugs in road safety. Aust. Prescr. 2008, 31, 33–35. [Google Scholar] [CrossRef]
- Drummer, O.H.; Yap, S. The involvement of prescribed drugs in road trauma. Forensic Sci. Int. 2016, 265, 17–21. [Google Scholar] [CrossRef]
- Naglaa, F.M.; Maha, K.A.M.; Mostafa, M.A. The Prevalence of Illicit Drugs and Alcohol in Road Traffic Accident Fatalities in the Eastern Region of Saudi Arabia. Indian J. Med. Forensic Med. Toxicol. 2021, 4, 3219–3225. [Google Scholar]
- Alcohol. European Road Safety Observatory. 2007. Available online: https://road-safety.transport.ec.europa.eu/system/files/2021-07/02-alcohol_en.pdf (accessed on 1 October 2023).
- Hels, T.; Lyckegaard, A.; Simonsen, K.W.; Steentoft, A.; Bernhoft, I.M. Risk of severe driver injury by driving with psychoactive substances. Accid. Anal. Prev. 2013, 59, 346–356. [Google Scholar] [CrossRef]
- Carfora, A.; Petrella, R.; Ambrosio, G.; Fracassi, I.; Festinese, S.; Feola, A.; Campobasso, C.P. Toxicological Analysis of Illicit Drugs Seized in Naples (Italy) and First Detection of Synthetic Cannabinoids during COVID-19 Pandemic. Healthcare 2022, 10, 1488. [Google Scholar] [CrossRef]
- Moè, A.; Cadinu, M.; Maas, A. Women drive better if not stereotyped. Accid. Anal. Prev. 2015, 85, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Roudsari, B.; Ramisetty-Mikler, S.; Rodriguez, L.A. Ethnicity, age, and trends in alcohol-related driver fatalities in the United States. Traffic Inj. Prev. 2009, 10, 410–414. [Google Scholar] [CrossRef]
- Papalimperi, A.H.; Athanaselis, S.A.; Mina, A.D.; Papoutsis, I.I.; Spiliopoulou, C.A.; Papadodima, S.A. Incidence of fatalities of road traffic accidents associated with alcohol consumption and the use of psychoactive drugs: A 7-year survey (2011–2017). Exp. Ther. Med. 2019, 18, 2299–2306. [Google Scholar] [CrossRef] [PubMed]
- Gjerde, H.; Christophersen, A.S.; Normann, P.T.; Mørland, J. Toxicological investigations of drivers killed in road traffic accidents in Norway during 2006–2008. Forensic Sci. Int. 2011, 212, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Santoyo-Castillo, D.; Pérez-Núñez, R.; Borges, G.; Híjar, M. Estimating the drink driving attributable fraction of road traffic deaths in Mexico. Addiction 2018, 113, 828–835. [Google Scholar] [CrossRef]
- Road Safety Report 2021. Italy. The Impact of COVID-19. Available online: https://www.itf-oecd.org/sites/default/files/italy-road-safety.pdf (accessed on 1 October 2023).
- Lacey, J.H.; Kelley-Baker, T.; Berning, A.; Romano, E.; Ramirez, A.; Yao, J.; Compton, R. Drug and Alcohol Crash Risk: A Case-Control Study; National Highway Traffic Safety Administration: Washington, DC, USA, 2016. Available online: https://www.nhtsa.gov/sites/nhtsa.gov/files/documents/812355_drugalcoholcrashrisk.pdf (accessed on 1 October 2023).
- Bernhoft, I.M.; Hels, T.; Lyckegaard, A.; Houwing, S.; Verstraete, A.G. Prevalence and risk of injury in Europe by driving with alcohol, illicit drugs and medicines. Procedia Soc. Behav. Sci. 2012, 48, 2907–2916. [Google Scholar] [CrossRef]
- Brady, J.E.; Li, G. Trends in alcohol and other drugs detected in fatally injured drivers in the United States, 1999–2010. Am. J. Epidemiol. 2014, 179, 692–699. [Google Scholar] [CrossRef]
- Costa, N.; Silva, R.; Mendonça, M.C.; Real, F.C.; Vieira, D.N.; Teixeira, H.M. Prevalence of ethanol and illicit drugs in road traffic accidents in the centre of Portugal: An eighteen-year update. Forensic Sci. Int. 2012, 216, 37–43. [Google Scholar] [CrossRef]
- Wundersitz, L.; Raftery, S. Understanding the context of alcohol impaired driving for fatal crash-involved drivers: A descriptive case analysis. Traffic Inj. Prev. 2017, 18, 781–787. [Google Scholar] [CrossRef]
- Arkell, T.R.; Vinckenbosch, F.; Kevin, R.C.; Theunissen, E.L.; McGregor, I.S.; Ramaekers, J.G. Effect of Cannabidiol and Δ9-Tetrahydrocannabinol on Driving Performance: A Randomized Clinical Trial. JAMA 2020, 324, 2177–2186. [Google Scholar] [CrossRef]
- Baldock, M.R.; Lindsay, V.L. Examination of the role of the combination of alcohol and cannabis in South Australian road crashes. Traffic Inj. Prev. 2015, 16, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Arkell, T.R.; Abelev, S.V.; Mills, L.; Suraev, A.; Arnold, J.C.; Lintzeris, N.; McGregor, I.S. Driving-related behaviors, attitudes, and perceptions among Australian medical cannabis users: Results from the CAMS 20 survey. J. Cannabis Res. 2023, 5, 35. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, D.; Manca, M.; Premaschi, S.; Banfi, G.; Locatelli, M. Toxicological investigation in blood samples from suspected impaired driving cases in the Milan area: Possible loss of evidence due to late blood sampling. Forensic Sci. Int. 2018, 288, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Di Ciano, P.; Brands, B.; Fares, A.; Wright, M.; Stoduto, G.; Byrne, P.; McGrath, M.; Hasan, O.S.M.; Le Foll, B.; Wickens, C.M. The utility of THC cutoff levels in blood and saliva for detection of impaired driving. Cannabis Cannabinoid Res. 2023, 8, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Hartman, R.L.; Huestis, M.A. Cannabis effects on driving skills. Clin. Chem. 2013, 59, 478–492. [Google Scholar] [CrossRef] [PubMed]
- Pelletti, G.; Verstraete, A.G.; Reyns, T.; Barone, R.; Rossi, F.; Garagnani, M.; Pelotti, S. Prevalence of therapeutic drugs in blood of drivers involved in traffic crashes in the area of Bologna, Italy. Forensic Sci. Int. 2019, 302, 109914. [Google Scholar] [CrossRef] [PubMed]
- Brubacher, J.R.; Chan, H.; Erdelyi, S.; Macdonald, S.; Asbridge, M.; Mann, R.E.; Eppler, J.; Lund, A.; MacPherson, A.; Martz, W.; et al. Cannabis use as a risk factor for causing motor vehicle crashes: A prospective study. Addiction 2019, 114, 1616–1626. [Google Scholar] [CrossRef]
- Hartman, R.L.; Brown, T.L.; Milavetz, G.; Spurgin, A.; Pierce, R.S.; Gorelick, D.A.; Gaffney, G.; Huestis, M.A. Cannabis effects on driving lateral control with and without alcohol. Drug Alcohol Depend. 2015, 154, 25–37. [Google Scholar] [CrossRef]
- Arkell, T.R.; Lintzeris, N.; Kevin, R.C.; Ramaekers, J.G.; Vandrey, R.; Irwin, C.; Haber, P.S.; McGregor, I.S. Cannabidiol (CBD) content in vaporized cannabis does not prevent tetrahydrocannabinol (THC)-induced impairment of driving and cognition. Psychopharmacology 2019, 236, 2713–2724. [Google Scholar] [CrossRef]
- Downey, L.A.; King, R.; Papafotiou, K.; Swann, P.; Ogden, E.; Boorman, M.; Stough, C. The effects of cannabis and alcohol on simulated driving: Influences of dose and experience. Accid. Anal. Prev. 2013, 50, 879–886. [Google Scholar] [CrossRef]
- Brunnauer, A.; Laux, G.; Geiger, E.; Soyka, M.; Möller, H.J. Antidepressants and driving ability: Results from a clinical study. J. Clin. Psychiatry. 2006, 67, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Wingen, M.; Ramaekers, J.G.; Schmitt, J.A. Driving impairment in depressed patients receiving long-term antidepressant treatment. Psychopharmacology 2006, 188, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Martin, T.L.; Solbeck, P.A.; Mayers, D.J.; Langille, R.M.; Buczek, Y.; Pelletier, M.R. A review of alcohol-impaired driving: The role of blood alcohol concentration and complexity of the driving task. J. Forensic Sci. 2013, 58, 1238–1250. [Google Scholar] [CrossRef]
- Campobasso, C.P.; De Micco, F.; Corbi, G.; Keller, T.; Hartung, B.; Daldrup, T.; Monticelli, F. Pupillary effects in habitual cannabis consumers quantified with pupillography. Forensic Sci. Int. 2020, 317, 110559. [Google Scholar] [CrossRef]
- Monticelli, F.C.; Tutsch-Bauer, E.; Hitzl, W.; Keller, T. Pupil function as a parameter for assessing impairment of the central nervous system from a traffic-medicine perspective. Leg. Med. 2009, 11 (Suppl. S1), S331–S332. [Google Scholar] [CrossRef]
- Manning, B.; Hayley, A.C.; Catchlove, S.; Shiferaw, B.; Stough, C.; Downey, L.A. Effect of CannEpil® on simulated driving performance and co-monitoring of ocular activity: A randomised controlled trial. J. Psychopharmacol. 2023, 37, 472–483. [Google Scholar] [CrossRef] [PubMed]
- Casares-López, M.; Ortiz-Peregrina, S.; Castro-Torres, J.J.; Ortiz, C.; Martino, F.; Jiménez, J.R. Assessing the influence of cannabis and alcohol use on different visual functions: A comparative study. Exp. Eye Res. 2022, 224, 109231. [Google Scholar] [CrossRef]
- McCartney, D.; Suraev, A.S.; Doohan, P.T.; Irwin, C.; Kevin, R.C.; Grunstein, R.R.; Hoyos, C.M.; McGregor, I.S. Effects of cannabidiol on simulated driving and cognitive performance: A dose-ranging randomised controlled trial. J. Psychopharmacol. 2022, 36, 1338–1349. [Google Scholar] [CrossRef]
- Grabe, H.J.; Wolf, T.; Grätz, S.; Laux, G. The influence of polypharmacological antidepressive treatment on central nervous information processing of depressed patients: Implications for fitness to drive. Neuropsychobiology 1998, 37, 200–204. [Google Scholar] [CrossRef]
- Casares-López, M.; Ortiz-Peregrina, S.; Ortiz, C.; Castro-Torres, J.J.; Anera, R.G. Comparison of the influence of alcohol and cannabis on the dynamics of the accommodative response. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 2281–2289. [Google Scholar] [CrossRef]
- Casares-López, M.; Castro-Torres, J.J.; Martino, F.; Ortiz-Peregrina, S.; Ortiz, C.; Anera, R.G. Contrast sensitivity and retinal straylight after alcohol consumption: Effects on driving performance. Sci. Rep. 2020, 10, 13599. [Google Scholar] [CrossRef] [PubMed]
- Martino, F.; Castro-Torres, J.J.; Casares-López, M.; Ortiz-Peregrina, S.; Ortiz, C.; Anera, R.G. Deterioration of binocular vision after alcohol intake influences driving performance. Sci. Rep. 2021, 11, 8904. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Peregrina, S.; Ortiz, C.; Casares-López, M.; Jiménez, J.R.; Anera, R.G. Effects of cannabis on visual function and self-perceived visual quality. Sci. Rep. 2021, 11, 1655. [Google Scholar] [CrossRef] [PubMed]
- Schumann, J.; Perkins, M.; Dietze, P.; Nambiar, D.; Mitra, B.; Gerostamoulos, D.; Drummer, O.H.; Cameron, P.; Smith, K.; Beck, B. The prevalence of alcohol and other drugs in fatal road crashes in Victoria, Australia. Accid. Anal. Prev. 2021, 153, 105905. [Google Scholar] [CrossRef]
- Jones, A.W.; Holmgren, A.; Kugelberg, F.C. Driving under the influence of central stimulant amines: Age and gender differences in concentrations of amphetamine, methamphetamine, and ecstasy in blood. J. Stud. Alcohol Drugs 2008, 69, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Borriello, R.; Carfora, A.; Cassandro, P.; Petrella, R. A five years study on drug-related deaths in Campania (Italy). Ann. Ist. Super. Sanita 2014, 50, 328–333. [Google Scholar]
- Maatz, K.R. Driving inability after drug use. Blutalkohol 2006, 43, 451–465. [Google Scholar]
- Legal Approaches to Drugs and Driving Topic Overview. European Monitoring Center for Drug and Drug Addiction. Available online: https://www.emcdda.europa.eu/publications/topic-overviews/legal-approaches-to-drugs-and-driving/html_en (accessed on 1 October 2023).
- Favretto, D.; Visentin, S.; Stocchero, G.; Vogliardi, S.; Snenghi, R.; Montisci, M. Driving under the influence of drugs: Prevalence in road traffic accidents in Italy and considerations on per se limits legislation. Traffic Inj. Prev. 2018, 19, 786–793. [Google Scholar] [CrossRef]
- Wolff, K.; Brimblecombe, R.; Forfar, J.; Forrest, A.; Gilvarry, E.; Johnston, A.; Morgan, J.; Osselton, M.; Read, L.; Taylor, D. Driving under the Influence of Drugs: Report from the Expert Panel on Drug Driving; Department for Transport: London, UK, 2013.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Total Victims | Total Positive Victims | ||||
|---|---|---|---|---|---|---|
| Years | No. (%) | No. (%) | ||||
| Total | Female | Male | Total | Female | Male | |
| <18 | 10 (4.4) | 0 (0) | 10 (4.4) | 2 (1.9) | 0 (0) | 2 (1.9) |
| 19–29 | 55 (24.1) | 3 (1.3) | 52 (22.8) | 25 (23.6) | 1 (0.9) | 24 (22.6) |
| 30–39 | 46 (20.2) | 2 (0.9) | 44 (19.3) | 26 (24.5) | 1 (0.9) | 25 (23.6) |
| 40–49 | 49 (21.5) | 2 (0.9) | 47 (20.6) | 30 (28.3) | 1 (0.9) | 29 (27.4) |
| 50–59 | 28 (12.3) | 2 (0.9) | 26 (11.4) | 14 (13.2) | 0 (0) | 14 (13.2) |
| >60 | 37 (16.2) | 3 (1.3) | 34 (14.9) | 8 (7.5) | 0 (0) | 8 (7.5) |
| Undetermined | 3 (1.3) | 2 (0.9) | 1 (0.4) | 1 (0.9) | 0 (0) | 1 (0.9) |
| Total | 228 | 14 | 214 | 106 | 3 | 103 |
| Occupants. | No. of Victims | Vehicle (No) | No. of Positive Victims | Vehicle |
|---|---|---|---|---|
| Drivers | 154 | Car (54) Motorcycle (79) Bus (1) Bicycle (18) Truck (2) | 74 | Car (28) Motorcycle (39) Bus (1) Bicycle (5) Truck (1) |
| Passengers | 15 | Car (11) Motorcycle (4) | 8 | Car (6) Motorcycle (2) |
| Pedestrians | 55 | Hit by car (52) Hit by train (3) | 21 | Hit by car (20) Hit by train (1) |
| Unknown | 4 | 3 | ||
| Total | 228 | 106 |
| BAC Range | Positive Only for Et-OH | Positive for Et-OH and Drugs |
|---|---|---|
| g/L | No (%) | No (%) |
| <0.5 | 1 (2.6) | 1 (3.7) |
| 0.51–0.8 | 1 (2.6) | 1 (3.7) |
| 0.81–1.5 | 9 (23.0) | 12 (44.4) |
| >1.5 | 28 (71.8) | 13 (48.2) |
| Total 66 | 39 | 27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carfora, A.; Feola, A.; Petrella, R.; Ambrosio, G.; Festinese, S.; Fracassi, I.; Palermo, P.; Zampone, M.; Campobasso, C.P. Qualitative/Quantitative Analysis of Alcohol and Licit/Illicit Drugs on Post-Mortem Biological Samples from Road Traffic Deaths. Separations 2023, 10, 589. https://doi.org/10.3390/separations10120589
Carfora A, Feola A, Petrella R, Ambrosio G, Festinese S, Fracassi I, Palermo P, Zampone M, Campobasso CP. Qualitative/Quantitative Analysis of Alcohol and Licit/Illicit Drugs on Post-Mortem Biological Samples from Road Traffic Deaths. Separations. 2023; 10(12):589. https://doi.org/10.3390/separations10120589
Chicago/Turabian StyleCarfora, Anna, Alessandro Feola, Raffaella Petrella, Giusy Ambrosio, Stefano Festinese, Ilaria Fracassi, Paolo Palermo, Martina Zampone, and Carlo Pietro Campobasso. 2023. "Qualitative/Quantitative Analysis of Alcohol and Licit/Illicit Drugs on Post-Mortem Biological Samples from Road Traffic Deaths" Separations 10, no. 12: 589. https://doi.org/10.3390/separations10120589
APA StyleCarfora, A., Feola, A., Petrella, R., Ambrosio, G., Festinese, S., Fracassi, I., Palermo, P., Zampone, M., & Campobasso, C. P. (2023). Qualitative/Quantitative Analysis of Alcohol and Licit/Illicit Drugs on Post-Mortem Biological Samples from Road Traffic Deaths. Separations, 10(12), 589. https://doi.org/10.3390/separations10120589