
Kaposi Sarcoma in Afghanistan: A Case Series from a Tertiary Referral Center

 , ,
, ,
Abstract
1. Introduction
2. Case Reports
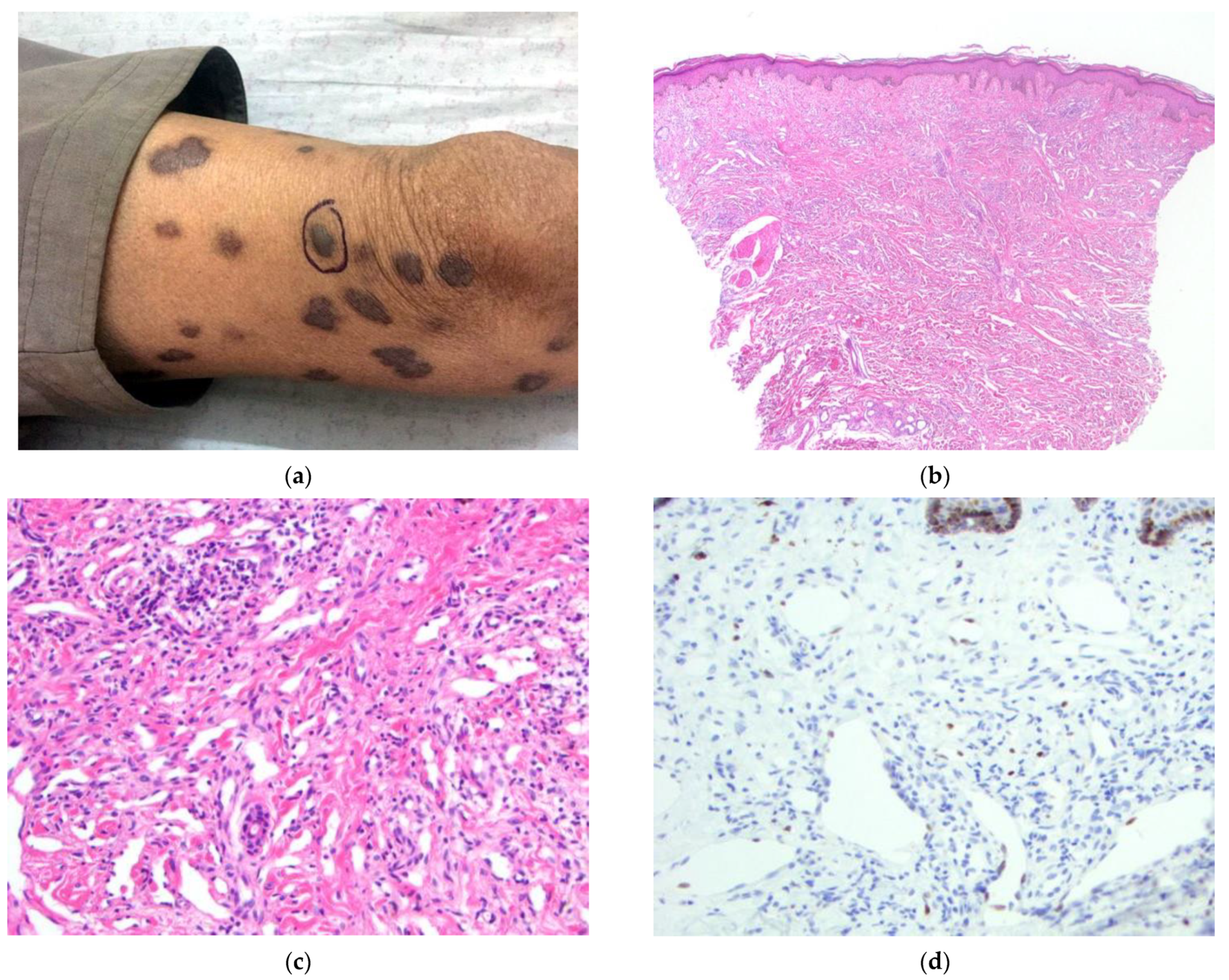
2.1. Case 1
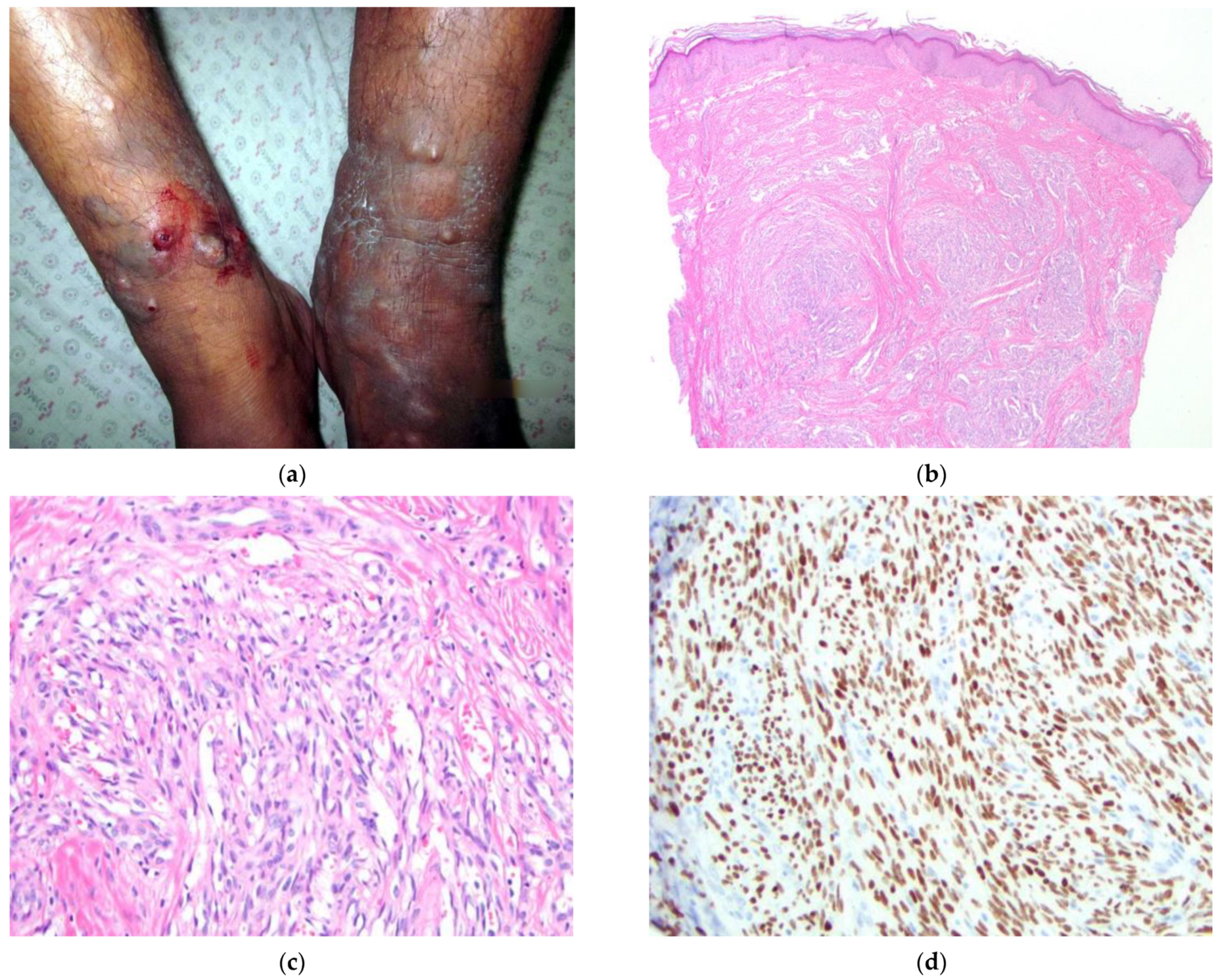
2.2. Case 2
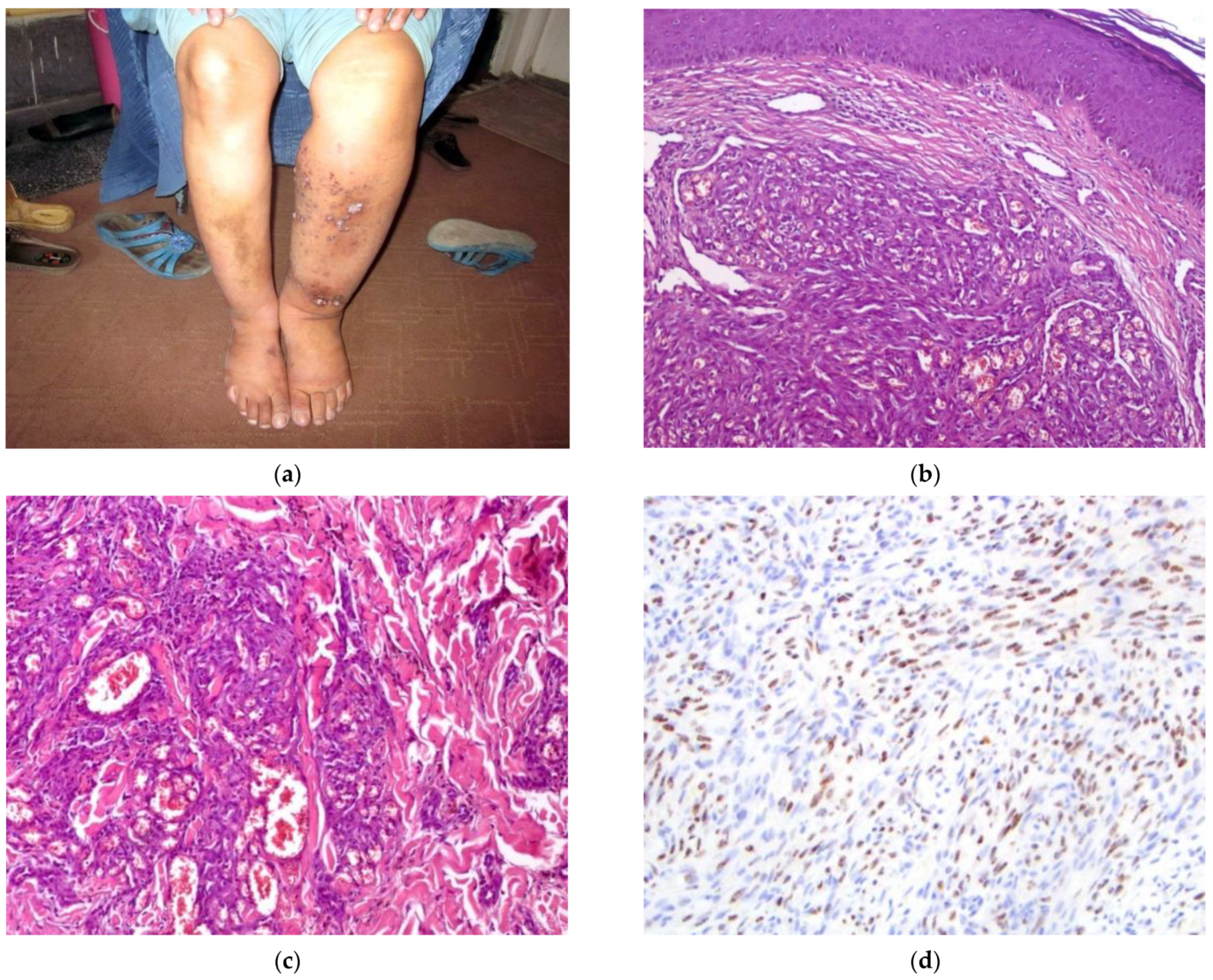
2.3. Case 3
2.4. Case 4
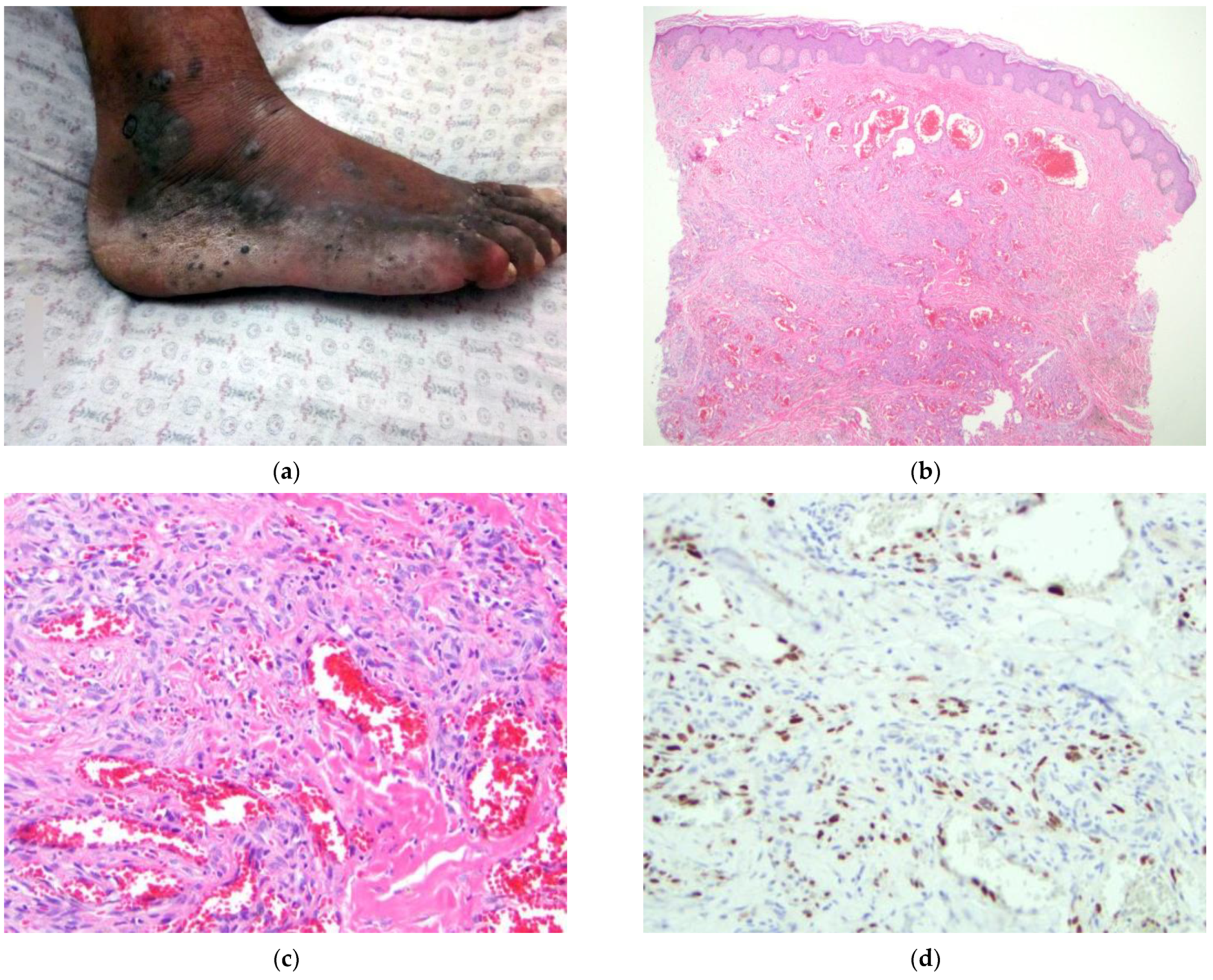
2.5. Case 5
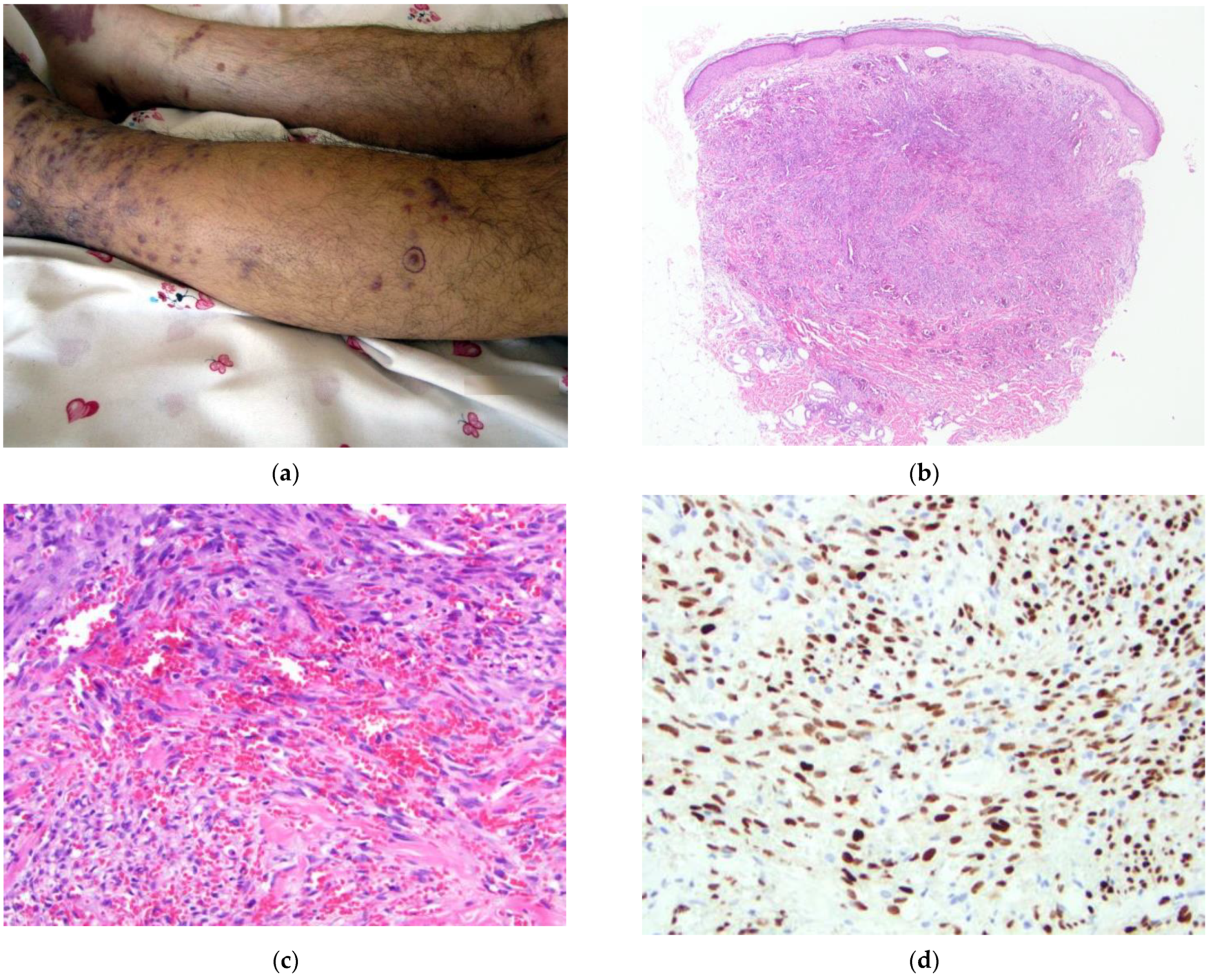
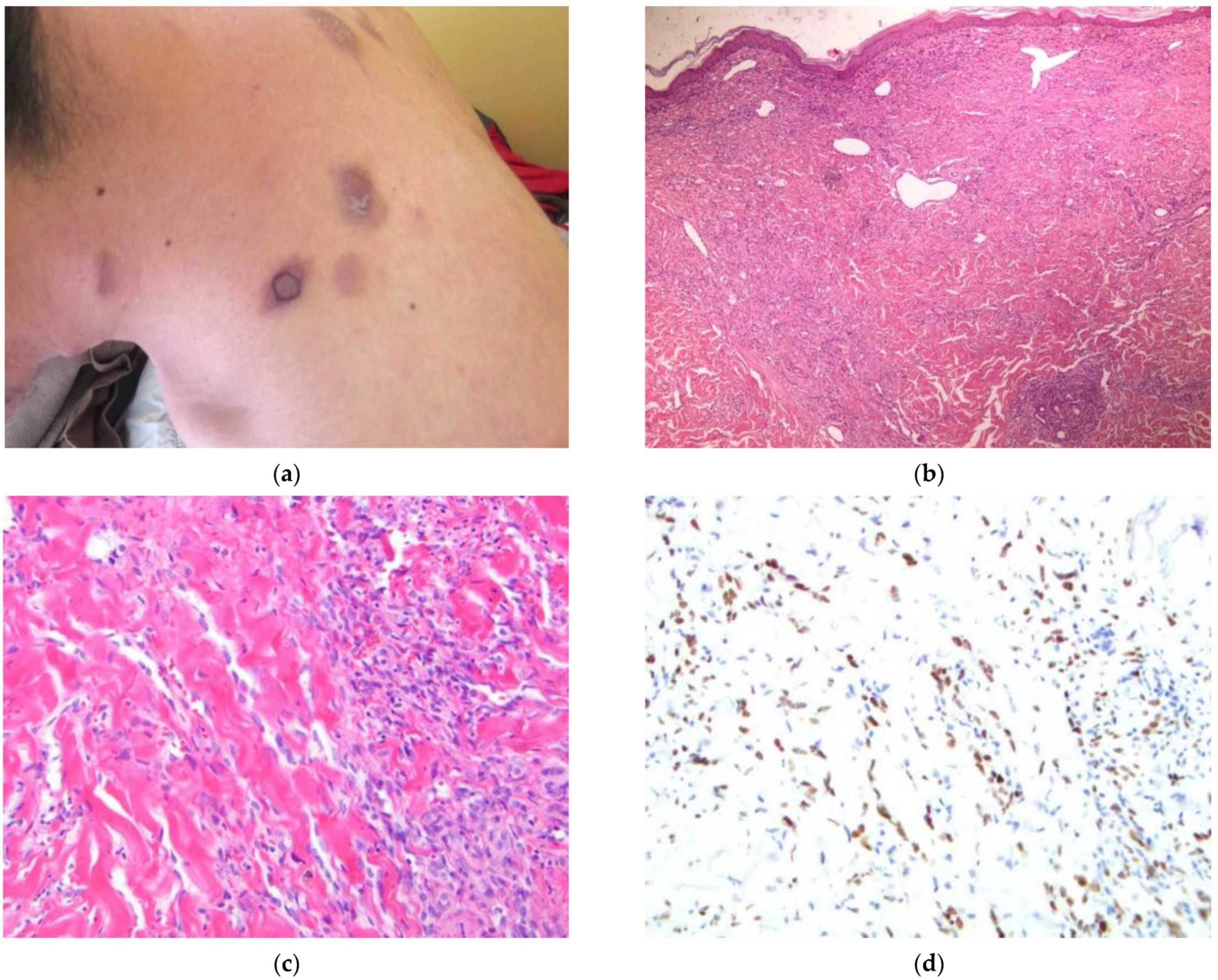
2.6. Case 6
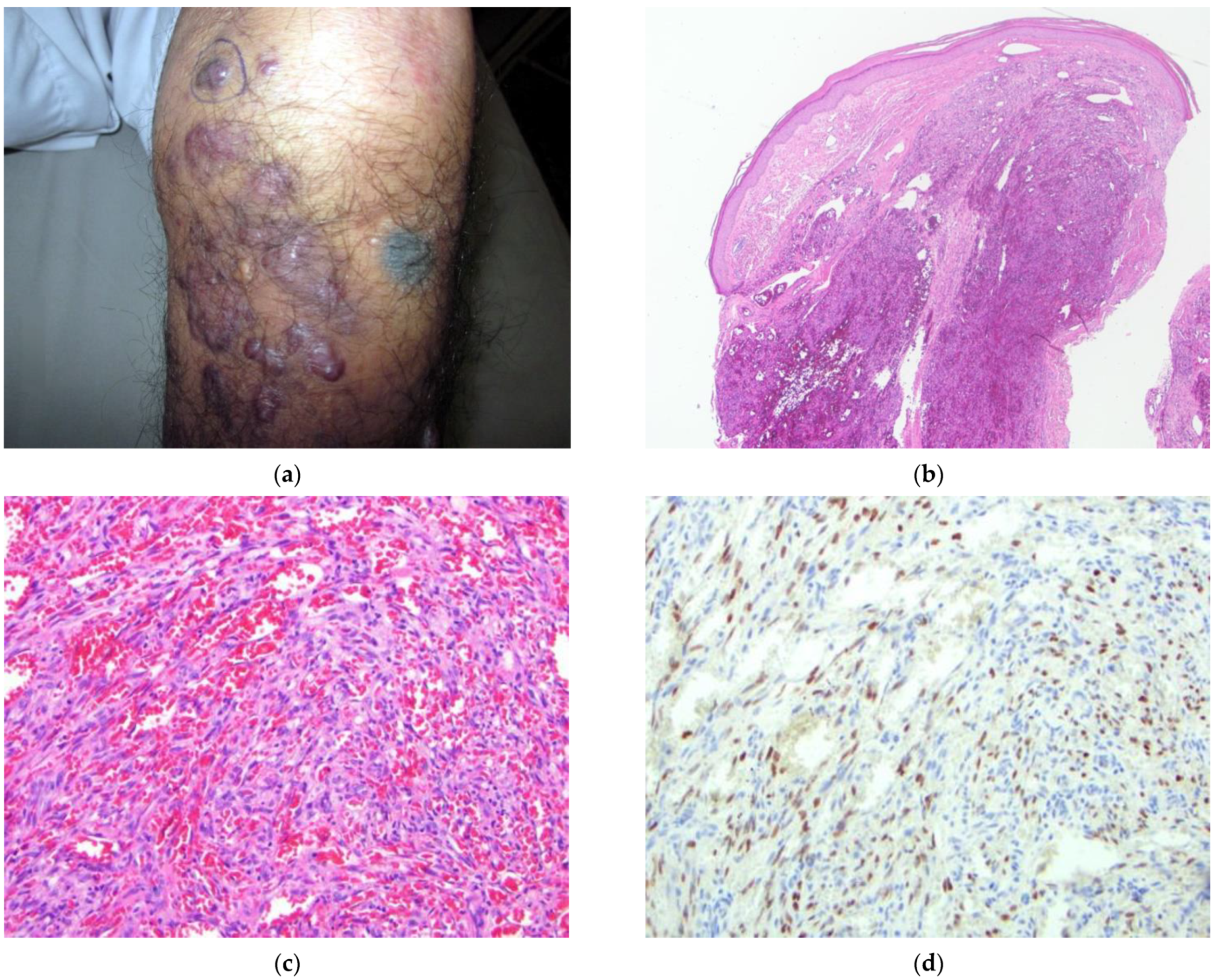
2.7. Case 7
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cesarman, E.; Damania, B.; Krown, S.E.; Martin, J.; Bower, M.; Whitby, D. Kaposi sarcoma. Nat. Rev. Dis. Primers 2019, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, M.R.; Gardner, J.M. Kaposi Sarcoma. In Diagnostic Pathology: Soft Tissue Tumors, 3rd ed.; Reynolds, J., Gelsinger, A., Bluth, R., Bennett, N., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 468–475. [Google Scholar]
- Gilani, J.A.; Khan, A.U.; Shahid, S.; Khan, I.U.; Khan, S.U. Clinical presentation of non-HIV Kaposi Sarcoma. J. Coll. Physicians Surg. Pak. 2009, 19, 586–588. [Google Scholar] [PubMed]
- Cattelan, A.M.; Calabrò, M.L.; De Rossi, A.; Aversa, S.M.L.; Barbierato, M.; Trevenzoli, M.; Gasperini, P.; Zanchetta, M.; Cadrobbi, P.; Monfardini, S.; et al. Long-term clinical outcome of AIDS-related Kaposi’s sarcoma during highly active antiretroviral therapy. Int. J. Oncol. 2005, 27, 779–785. [Google Scholar] [PubMed]
- Hiatt, K.M.; Nelson, A.M.; Lichy, J.H.; Fanburg-Smith, J.C. Classic Kaposi Sarcoma in the United States over the last two decades: A clinicopathologic and molecular study of 438 non-HIV-related Kaposi Sarcoma patients with comparison to HIV-related Kaposi Sarcoma. Mod. Pathol. 2008, 21, 572–582. [Google Scholar] [CrossRef] [PubMed]
- Mohanlal, R.D.; Pather, S. Variability of HHV8 LNA-1 immunohistochemical staining across the 3 histologic stages of HIV-associated mucocutaneous Kaposi sarcoma. Am. J. Dermatopathol. 2015, 37, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Hong, A.; Davies, S.; Soon Lee, C. Immunohistochemical detection of the human herpes virus 8 (HHV8) latent nuclear antigen-1 in Kaposi’s sarcoma. Pathology 2003, 35, 448–450. [Google Scholar] [CrossRef]
- Robin, Y.-M.; Guillou, L.; Michels, J.-J.; Coindre, J.-M. Human herpesvirus 8 immunostaining. Am. J. Clin. Pathol. 2004, 121, 330–334. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chatlynne, L.G.; Ablashi, D.V. Seroepidemiology of Kaposi’s sarcoma-associated herpesvirus (KSHV). Semin. Cancer Biol. 1999, 9, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Jalilvand, S.; Shoja, Z.; Mokhtari-Azad, T.; Nategh, R.; Gharehbaghian, A. Seroprevalence of Human herpesvirus 8 (HHV-8) and incidence of Kaposi’s sarcoma in Iran. Infect. Agent Cancer 2011, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.; McMichael, J.R.; Stoff, B.K. Utility of international store-and-forward teledermatopathology among a cohort of mostly female patients at a tertiary referral center in Afghanistan. Int. J. Womens Dermatol. 2017, 4, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Dollard, S.C.; Butler, L.M.; Jones, A.M.G.; Mermin, J.H.; Chidzonga, M.; Chipato, T.; Shiboski, C.H.; Brander, C.; Mosam, A.; Kiepiela, P.; et al. Substantial regional differences in human herpesvirus 8 seroprevalence in sub-Saharan Africa: Insights on the origin of the “Kaposi’s sarcoma belt”. Int. J. Cancer 2010, 127, 2395–2401. [Google Scholar] [CrossRef] [PubMed]
- HIV AIDS Asia Pacific Research Statistical Data Information Resources AIDS Data Hub. Key Facts on HIV in Asia and the Pacific [Internet]. Bangkok Thailand: Joint United Nations Program on HIV/AIDS; [Updated September 2020; Cited May 2021]. Available online: https://www.aidsdatahub.org/resource/afghanistan-country-slides (accessed on 26 August 2021).
- Massone, C.; Brunasso, A.M.; Campbell, T.M.; Soyer, H.P. State of the art of teledermatopathology. Am. J. Dermatopathol. 2008, 30, 446–450. [Google Scholar] [CrossRef] [PubMed]
- United Nations: Office on Drugs and Crime. World Drug Report 2012. 2012. Available online: https://www.unodc.org/unodc/en/data-and-analysis/WDR-2012.html (accessed on 28 August 2021).
- Hall, W.D.; Degenhardt, L. Afghanistan has a sizeable problem with opioid use. Lancet Glob. Health 2014, 2, e557–e558. [Google Scholar] [CrossRef]
- Cottler, L.B.; Ajinkya, S.; Goldberger, B.A.; Ghani, M.A.; Martin, D.M.; Hu, H.; Gold, M.S. Prevalence of drug and alcohol use in urban Afghanistan: Epidemiological data from the Afghanistan National URBAN drug use STUDY (ANUDUS). Lancet Glob. Health 2014, 2, e592–e600. [Google Scholar] [CrossRef]
- Todd, C.S.; Abed, A.M.; Strathdee, S.A.; Scott, P.T.; Botros, B.A.; Safi, N.; Earhart, K.C. HIV, hepatitis C, and hepatitis B infections and associated risk behavior in injection drug users, Kabul, Afghanistan. Emerg. Infect. Dis. 2007, 13, 1327–1331. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID # | Age | Sex | Province | HIV Status | Lesion Morphology | Lesion Location | Histologic Features |
|---|---|---|---|---|---|---|---|
| 1 | 63 | Male | Kabul | Negative | Violaceous papules and nodules | Trunk, extremities, soft palate |
|
| 2 | 60 | Male | Faryab | Negative | Painful, pruritic nodules, some with ulceration | Bilateral lower legs, distal upper extremities |
|
| 3 | 45 | Female | Takhar | Negative | Violaceous, pruritic, painless papules and nodules | Left lower leg |
|
| 4 | 61 | Male | Takhar | Negative | Violaceous papules, nodules, and patches | Bilateral lower legs, dorsal hands |
|
| 5 | 68 | Male | Faryab | Negative | Painful nodules and papules | Right dorsal and plantar foot, ankles, and anterior lower leg, left plantar foot |
|
| 6 | 27 | Male | Kabul | Positive | Indurated, violaceous nodules | Face, trunk, extremities, oral mucosa |
|
| 7 | 85 | Male | Kabul | Negative | Confluent, nodular, violaceous plaques | Bilateral lower legs and feet, bilateral forearms, soft palate |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Higgins, A.D.; Dunn, R.J.; Malikzai, O.; Ahmadzai, M.; Gardner, J.M.; Stoff, B.K.; McMichael, J.R. Kaposi Sarcoma in Afghanistan: A Case Series from a Tertiary Referral Center. Dermatopathology 2022, 9, 258-270. https://doi.org/10.3390/dermatopathology9030030
Higgins AD, Dunn RJ, Malikzai O, Ahmadzai M, Gardner JM, Stoff BK, McMichael JR. Kaposi Sarcoma in Afghanistan: A Case Series from a Tertiary Referral Center. Dermatopathology. 2022; 9(3):258-270. https://doi.org/10.3390/dermatopathology9030030
Chicago/Turabian StyleHiggins, Alyssa D., Richard J. Dunn, Omer Malikzai, Mirwais Ahmadzai, Jerad M. Gardner, Benjamin K. Stoff, and Josette R. McMichael. 2022. "Kaposi Sarcoma in Afghanistan: A Case Series from a Tertiary Referral Center" Dermatopathology 9, no. 3: 258-270. https://doi.org/10.3390/dermatopathology9030030
APA StyleHiggins, A. D., Dunn, R. J., Malikzai, O., Ahmadzai, M., Gardner, J. M., Stoff, B. K., & McMichael, J. R. (2022). Kaposi Sarcoma in Afghanistan: A Case Series from a Tertiary Referral Center. Dermatopathology, 9(3), 258-270. https://doi.org/10.3390/dermatopathology9030030