
Pityriasis Lichenoides et Varioliformis Acuta as a Complication of COVID-19 Infection

 , , and
, , and 
Abstract
:1. Introduction
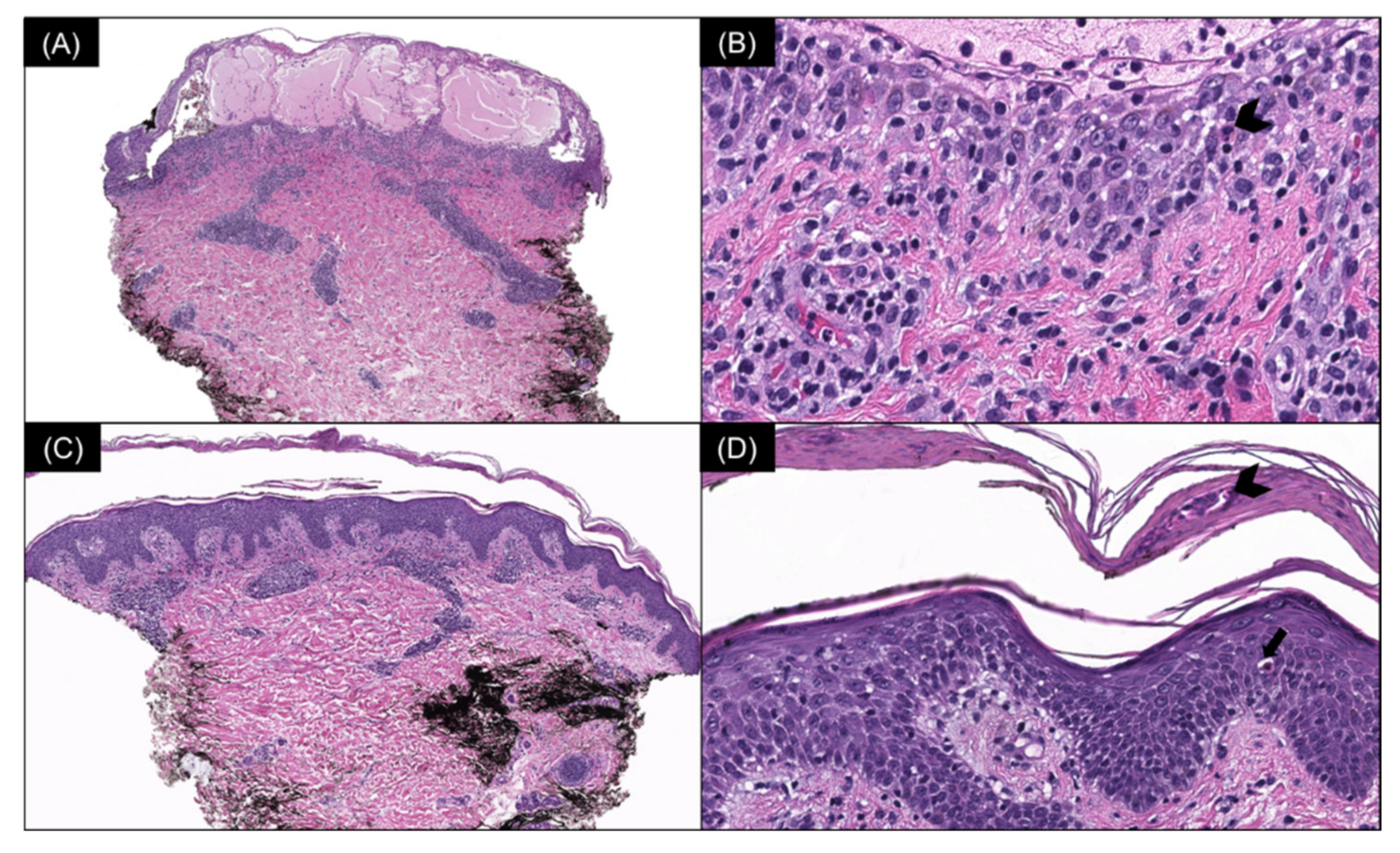
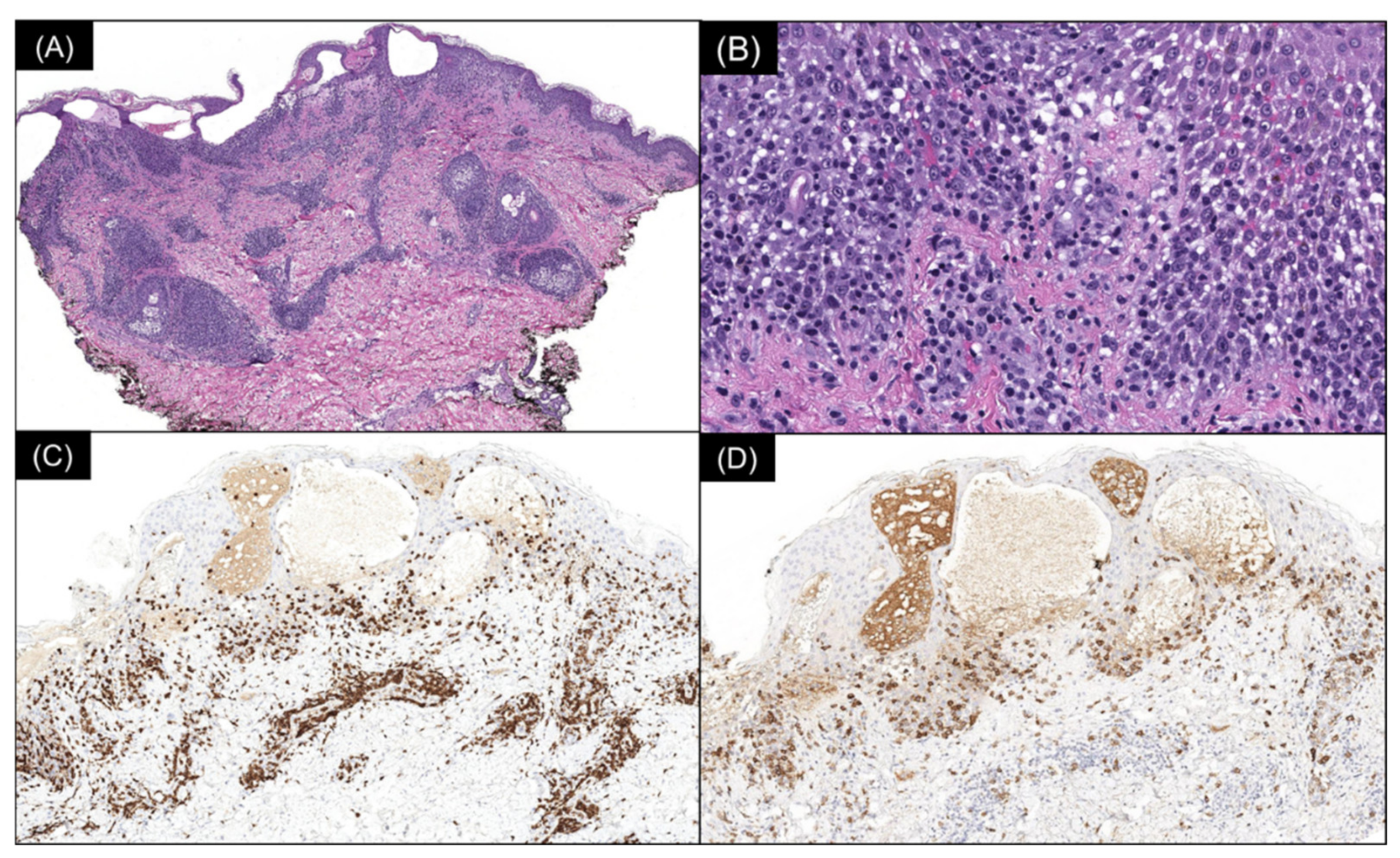
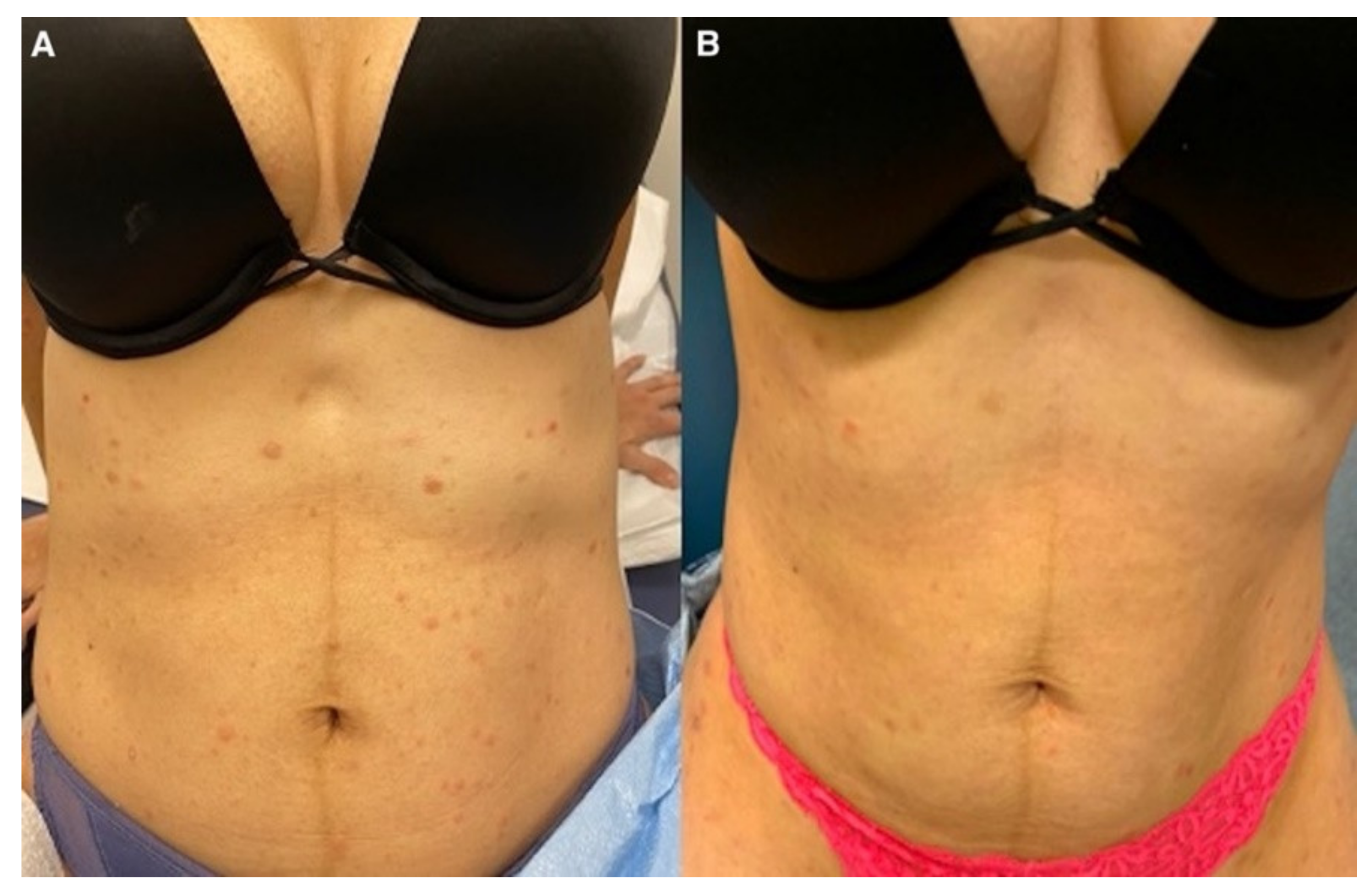
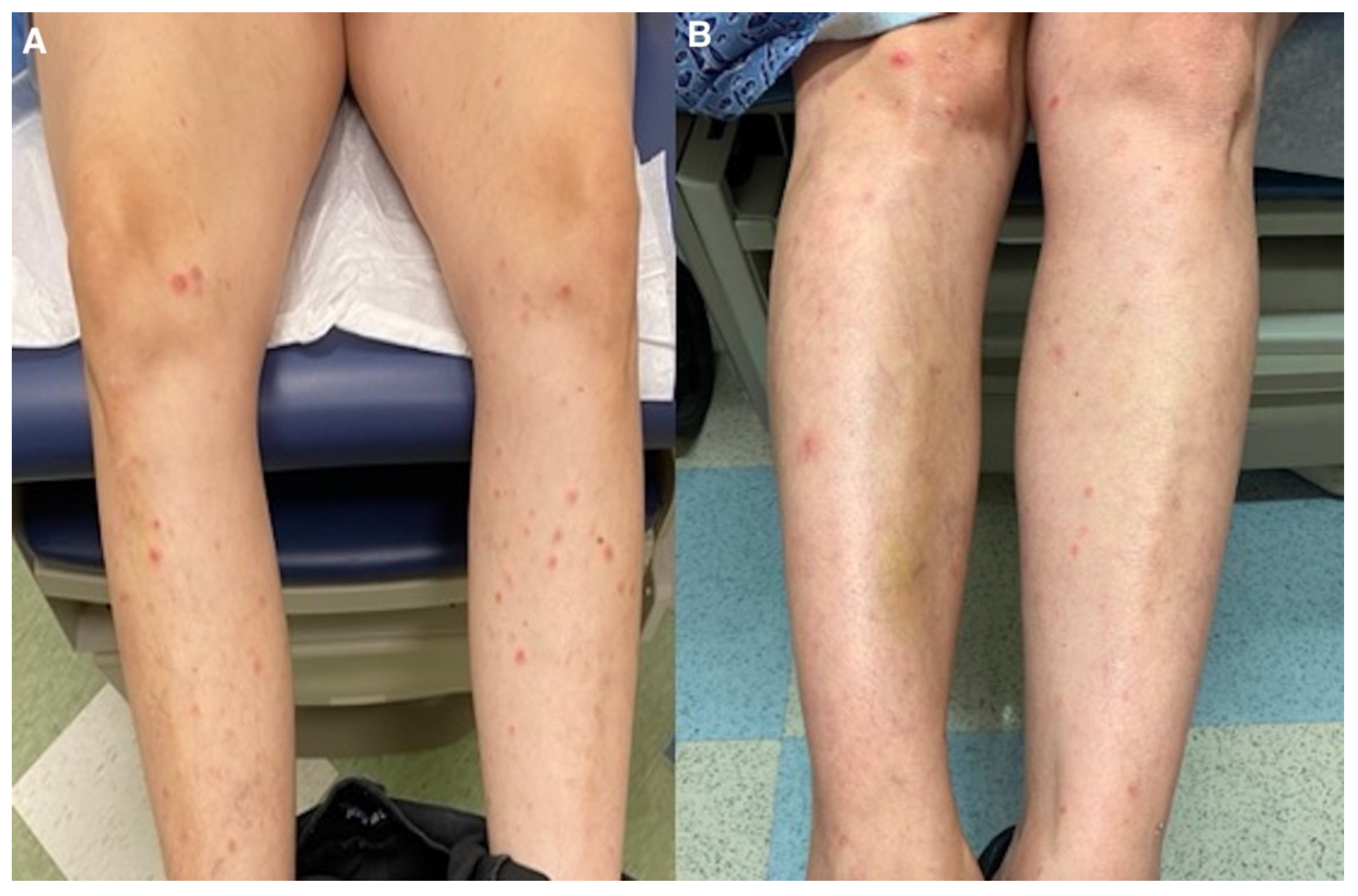
2. Case
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bowers, S.; Warshaw, E.M. Pityriasis lichenoides and its subtypes. J. Am. Acad. Dermatol. 2006, 55, 557–572. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, N.F.; Rozdeba, P.; Schwartz, R.A.; Kihiczak, G.; Lambert, W.C. Pityriasis lichenoides et varioliformis acuta: A disease spectrum. Int. J. Dermatol. 2010, 49, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Khachemoune, A.; Blyumin, M.L. Pityriasis Lichenoides. Am. J. Clin. Dermatol. 2007, 8, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Herron, M.D.; Bohnsack, J.F.; Vanderhooft, S.L. Septic, CD-30 Positive Febrile Ulceronecrotic Pityriasis Lichenoides et Varioliformis Acuta. Pediatr. Dermatol. 2005, 22, 360–365. [Google Scholar] [CrossRef]
- Kempf, W.; Kazakov, D.V.; Palmedo, G.; Fraitag, S.; Schaerer, L.; Kutzner, H. Pityriasis Lichenoides et Varioliformis Acuta With Numerous CD30+ Cells. Am. J. Surg. Pathol. 2012, 36, 1021–1029. [Google Scholar] [CrossRef] [Green Version]
- Borra, T.; Custrin, A.; Saggini, A.; Fink-Puches, R.; Cota, C.; Vermi, W.; Facchetti, F.; Cerroni, L. Pityriasis Lichenoides, Atypical Pityriasis Lichenoides, and Related Conditions. Am. J. Surg. Pathol. 2018, 42, 1101–1112. [Google Scholar] [CrossRef]
- Kim, J.E.; Yun, W.J.; Mun, S.K.; Yoon, G.S.; Huh, J.; Choi, J.H.; Chang, S. Pityriasis lichenoides et varioliformis acuta and pityriasis lichenoides chronica: Comparison of lesional T-cell subsets and investigation of viral associations. J. Cutan. Pathol. 2011, 38, 649–656. [Google Scholar] [CrossRef]
- Dereure, O.; Levi, E.; Kadin, M.E. T-Cell Clonality in Pityriasis Lichenoides et Varioliformis Acuta. Arch. Dermatol. 2000, 136, 1483–1486. [Google Scholar] [CrossRef] [Green Version]
- Gianotti, R.; Restano, L.; Cutrone, M.; Colonna, C.; Fellegara, G.; Debernardi, I.; Boggio, F.; Del Gobbo, A.; Monzani, N.A.; Tripodo, C.; et al. Papulo-purpuric dermatitis of childhood: A distinct PLEVA-like eruption associated to SARS-CoV-2 infection. Clinical, histopathological and immunohistochemical study of 10 cases. Pediatr. Dermatol. 2021, 38, 1185–1190. [Google Scholar] [CrossRef]
- Durusu, I.N.; Gurel, G.; Tokyol, C. Un caso de pitiriasis liquenoide crónica en una paciente infectada por COVID-19. Actas Dermosifiliogr 2021. [Google Scholar] [CrossRef]
- Palmén, J.; Lepistö, M.; Talve, L.; Hieta, N. Pityriasis lichenoides et varioliformis acuta following COVID-19 mRNA vaccination. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e327–e328. [Google Scholar] [CrossRef] [PubMed]
- Sernicola, A.; Dybala, A.; Gomes, V.; Maddalena, P.; Adotti, F.; Soda, G.; Muharremi, R.; Fino, P.; Del Duca, E.; Grieco, T. Lymphomatoid drug reaction developed after BNT162b2 (Comirnaty) COVID-19 vaccine manifesting as pityriasis lichenoides et varioliformis acuta-like eruption. J. Eur. Acad. Dermatol. Venereol. 2021, 36, e172–e174. [Google Scholar] [CrossRef] [PubMed]
- Dawoud, N.M.; Aslam, H.; Ali, I.M.; Dawoud, M.M. The first case report of Pityriasis lichenoides chronica following COVID -19 mRNA vaccination. Dermatol. Ther. 2022, 35, e15445. [Google Scholar] [CrossRef] [PubMed]
- Sechi, A.; Pierobon, E.; Pezzolo, E.; Germi, L.; Trevisan, G.; Zardo, D.; Riva, G.; Mondino, S.; Naldi, L. Abrupt onset of Sweet syndrome, pityriasis rubra pilaris, pityriasis lichenoides et varioliformis acuta and erythema multiforme: Unravelling a possible common trigger, the COVID-19 vaccine. Clin. Exp. Dermatol. 2021, 47, 437–440. [Google Scholar] [CrossRef]
- LeWitt, T.; Chung, C.; Manton, J.; Sergeyenko, A.; Tan, T.; Sigal, A.; Zhou, X. (.; Guitart, J. Rare lymphomatoid reactions following SARS-CoV-2 vaccination. JAAD Case Rep. 2021, 20, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Mäkilä, T.; Jeskanen, L.; Butina, M.; Harjama, L.; Ranki, A.; Mälkönen, T.; Kluger, N. Pityriasis lichenoides et varioliformis acuta after SARS-CoV-2 infection and relapse after vaccination. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e431–e433. [Google Scholar] [CrossRef]
- Filippi, F.; Baraldi, C.; Zinzani, P.; Casadei, B.; Pileri, A. A case of pityriasis lichenoides et varioliformis acuta developed after first dose of Oxford–AstraZeneca COVID -19 vaccine. J. Eur. Acad. Dermatol. Venereol. 2022. [Google Scholar] [CrossRef]
- Vonderheid, E.C.; Kadin, M.E.; Telang, G.H. Commentary about papular mycosis fungoides, lymphomatoid papulosis and lymphomatoid pityriasis lichenoides: More similarities than differences. J. Cutan. Pathol. 2015, 43, 303–312. [Google Scholar] [CrossRef]
- Moy, A.; Sun, J.; Ma, S.; Seminario-Vidal, L. Lymphomatoid Papulosis and Other Lymphoma-Like Diseases. Dermatol. Clin. 2019, 37, 471–482. [Google Scholar] [CrossRef]
- Nieto-Benito, L.M.; de la Torre-Ruiz, E.H.; Balaguer-Franch, I.; Rosell-Díaz, M.; Mateos-Mayo, A.; Herrero-Sanchez, A.; Lacasta-Plasín, C.; García-Piqueras, P.; Barchino-Ortiz, L.; Bergón-Sendín, M.; et al. Histopathological findings in COVID-19-induced cutaneous lesions. Clinicopathological correlation of SARS-CoV-19 dermatologic patterns: Review of the literature. Australas. J. Dermatol. 2020, 62, e98–e101. [Google Scholar] [CrossRef]
- Bellinato, F.; Maurelli, M.; Gisondi, P.; Girolomoni, G. A systematic review of treatments for pityriasis lichenoides. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2039–2049. [Google Scholar] [CrossRef] [PubMed]
- Di Costanzo, L.; Balato, N.; La Bella, S.; Balato, A. Successful association in the treatment of pityriasis lichenoides et varioliformis acuta. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 971–972. [Google Scholar] [CrossRef] [PubMed]
- Skinner, R.B.; Levy, A.L. Rapid resolution of pityriasis lichenoides et varioliformis acuta with azithromycin. J. Am. Acad. Dermatol. 2008, 58, 524–525. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.; Boudny, C.; Nievergelt, H.; Simon, H.-U.; Braathen, L. Successful treatment of pityriasis lichenoides with topical tacrolimus. Br. J. Dermatol. 2004, 150, 1033–1035. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Infection/Vaccine | Histopathology | Cutaneous Lesions |
|---|---|---|---|
| Durusu et al. [10] | COVID-19 infection | Hyperkeratosis; irregular acanthosis; focal spongiosis; lymphocytic exocytosis in the epidermis; and band-like lymphomonocytic infiltrate and melanophages in the superficial dermis. | Erythematous to purple lichenoid papules and plaques and hemorrhagic crusts. |
| Gianotti et al. [9] | COVID-19 infection | Dermal lymphocytic infiltrate; interstitial eosinophils; diffuse interface dermatitis; and scattered necrosis of keratinocytes. | Erythematous and purpuric hemorrhagic papules with crusts. |
| Sechi et al. [14] | 2nd dose Pfizer vaccine | Focal epidermal ulceration; spongiosis; parakeratosis; and interface inflammation within a wedge-shaped dermal inflammatory cell infiltrate. | Scattered, nonfolliculocentric papules with erythematous, raised borders and an eroded center, covered by a hemorrhagic crust. |
| Sernicola et al. [12] | 1st dose Pfizer vaccine | Hyperkeratosis; epidermal hyperplasia; diffuse spongiosis with a foci of mixed, lympho-monocytic infiltrates; Langerhans cells; granulocytes; and a dense, polymorphic inflammatory infiltrate in the dermis. | Erythematous-pinkish papular lesions partially covered by sero-hematic crusts. |
| Palmén et al. [11] | 1st dose Pfizer vaccine | N/A | Erythematous, ulcerative, and crusting lesions. |
| Dawoud et al. [13] | 1st dose Pfizer vaccine | Parakeratosis; moderate spongiosis and focal vacuolar alteration of the basal cell layer; mild edema; extravasated red cells; and superficial and deep dermal perivascular, lymphocytic infiltrate. | Erythematous and purpuric hemorrhagic papules with crusts. |
| Filippi et al. [17] | 1st dose AstraZeneca vaccine | Parakeratosis; mild spongiosis; wedge-shaped perivascular lymphocytic infiltrate; and apoptotic keratinocytes and extravasated erythrocytes in the papillary dermis. | Erythematous and erythematous-crusted papules. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De La Garza, H.; Saliba, E.; Rosales Santillan, M.; Brem, C.; Vashi, N.A. Pityriasis Lichenoides et Varioliformis Acuta as a Complication of COVID-19 Infection. Dermatopathology 2022, 9, 244-250. https://doi.org/10.3390/dermatopathology9030028
De La Garza H, Saliba E, Rosales Santillan M, Brem C, Vashi NA. Pityriasis Lichenoides et Varioliformis Acuta as a Complication of COVID-19 Infection. Dermatopathology. 2022; 9(3):244-250. https://doi.org/10.3390/dermatopathology9030028
Chicago/Turabian StyleDe La Garza, Henriette, Elie Saliba, Monica Rosales Santillan, Candice Brem, and Neelam A. Vashi. 2022. "Pityriasis Lichenoides et Varioliformis Acuta as a Complication of COVID-19 Infection" Dermatopathology 9, no. 3: 244-250. https://doi.org/10.3390/dermatopathology9030028
APA StyleDe La Garza, H., Saliba, E., Rosales Santillan, M., Brem, C., & Vashi, N. A. (2022). Pityriasis Lichenoides et Varioliformis Acuta as a Complication of COVID-19 Infection. Dermatopathology, 9(3), 244-250. https://doi.org/10.3390/dermatopathology9030028