

Cumulative Violence and Post-Traumatic Stress: An Integrative Model of Coping and Resilience Among Women Exposed to Sexual and Conflict-Related Violence




Abstract
1. Introduction
1.1. Ongoing Exposure to Conflict-Related Violence
1.2. Exposure to Sexual Violence
1.3. Intersection of Conflict-Related and Sexual Violence
1.4. Theoretical Framework and Key Resilience Constructs
1.5. Post-Traumatic Symptoms
1.6. Research Questions and Hypotheses
- 1.
- Do levels of coping strategies, SOC, CR, and post-traumatic symptoms differ in accordance with the level of exposure to conflict-related and/or sexual violence?We hypothesized that significant group differences would be observed across the research variables. Women with high exposure to both sexual violence and conflict-related violence would be expected to report the highest use of non-adaptive coping strategies, the lowest levels of SOC and CR, and the most severe post-traumatic symptoms. In contrast, women with low exposure to both types of violence would be expected to report the lowest levels of non-adaptive coping strategies and post-traumatic symptoms, as well as the highest levels of adaptive coping, SOC, and CR.
- 2.
- What are the relationships between exposure to ongoing conflict-related violence, exposure to sexual violence, coping strategies, SOC, CR, and post-traumatic symptoms?We expected to find no correlation between the level of exposure to conflict-related violence and the level of exposure to sexual violence. We did expect to find positive correlations between the levels of exposure to conflict-related and sexual violence, the use of non-adaptive coping strategies, and the severity of post-traumatic symptoms. We also expected to find positive correlations between adaptive coping strategies, SOC, and CR. We expected to find negative correlations between levels of exposure and post-traumatic symptoms, on the one hand, and indicators of resilience (adaptive coping strategies, SOC, and CR) on the other.
- 3.
- To what extent do combined exposure to ongoing conflict-related and sexual violence, sociodemographic characteristics (i.e., age and socioeconomic status), coping strategies, and resilience factors (i.e., SOC and CR) explain the severity of post-traumatic symptoms?
2. Materials and Methods
2.1. Study Population and Sample
- 104 women (18.3% of the sample) had been exposed to high levels of both sexual assault and conflict-related violence.
- 137 women (24.1% of the sample) had been exposed to high levels of conflict-related violence.
- 156 women (27.5% of the sample) had been exposed to high levels of sexual violence.
- 171 women (30.1% of the sample) had been exposed to low levels of both forms of violence.
2.2. Research Instruments
2.2.1. Demographic Data
2.2.2. Exposure to Ongoing Conflict-Related Violence
2.2.3. Exposure to Sexual Violence
2.2.4. Coping Strategies
2.2.5. Personal Resilience
2.2.6. Community Resilience (CR)
2.2.7. Post-Traumatic Stress Disorder (PTSD)
2.3. Research Procedure
2.4. Data Analysis
3. Results
3.1. Differences Between Research Groups in Terms of the Study Variables
3.2. Relationships Between Study Variables
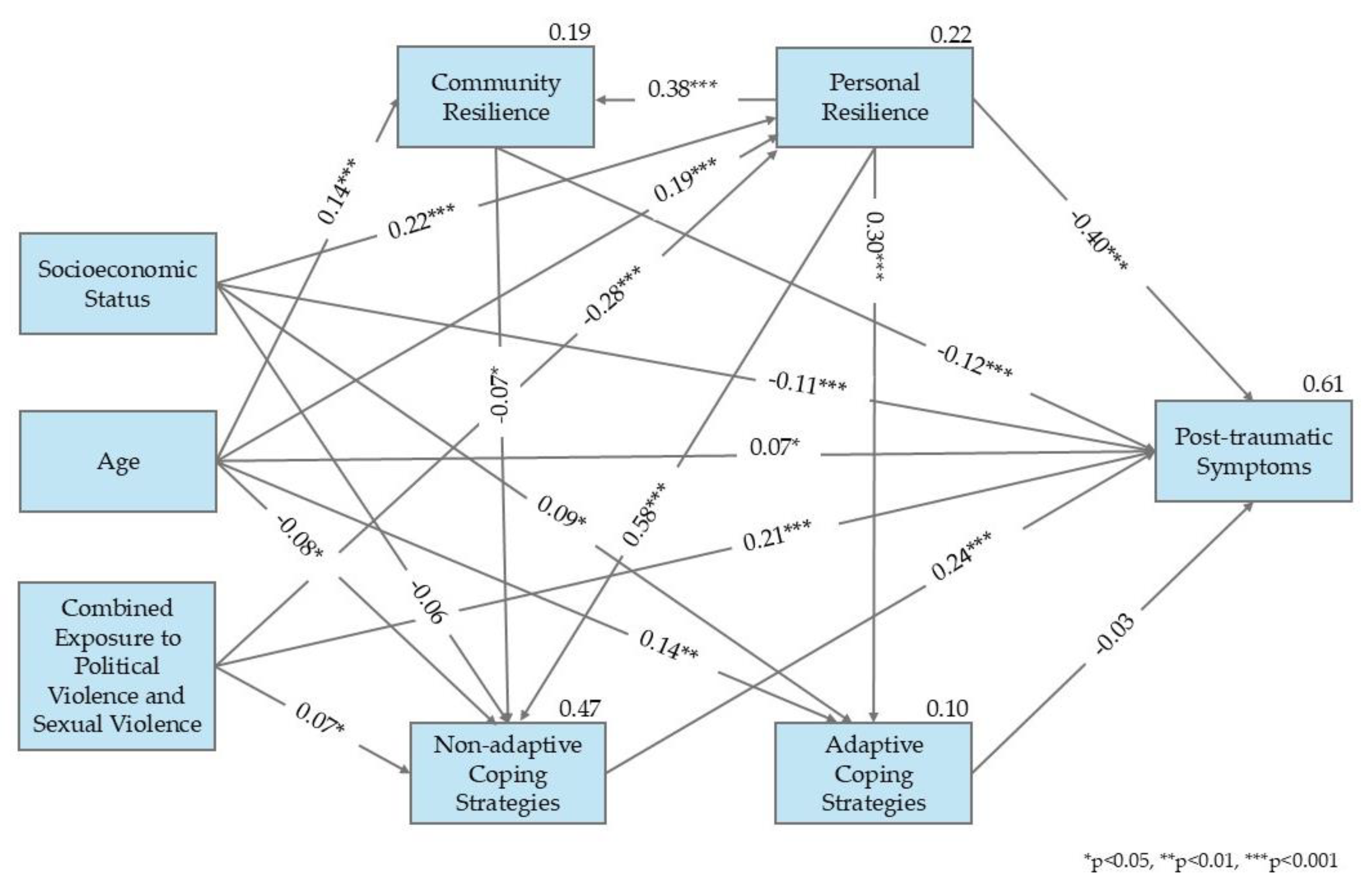
3.3. Model Analysis
4. Discussion
4.1. Theoretical Contribution and Practical Implications
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CR | Community resilience |
| PTSD | Post-traumatic stress disorder |
| SOC | Sense of coherence |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Low Exposure (d) n ≈ 165 | High Sexual Violence (c) n ≈ 156 | High Conflict-Related Violence (b) n ≈ 135 | Dual Exposure (a) n ≈ 104 | Cohen’s d | F # | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| SD | M | SD | M | SD | M | SD | M | |||
| Active coping | 0.75 | 2.16 | 0.75 | 2.17 | 0.75 | 2.2 | 0.84 | 1.88 | 0.4 ab 0.36 ac 0.35 ad | 4.3 ab,ac,ad * |
| Emotional support | 0.82 | 2.12 | 0.83 | 2.14 | 0.86 | 2.09 | 0.86 | 1.81 | 0.39 ac 0.36 ad | 3.89 ac,ad * |
| Instrumental support | 0.82 | 1.71 | 0.88 | 1.54 | 0.81 | 1.53 | 0.83 | 1.62 | 1.65 | |
| Positive reframing | 0.78 | 1.91 | 0.82 | 1.94 | 0.79 | 1.98 | 0.88 | 1.85 | 0.55 | |
| Planning | 0.62 | 2.4 | 0.7 | 2.41 | 0.68 | 2.35 | 0.76 | 2.18 | 2.95 * | |
| Acceptance | 0.66 | 1.71 | 0.74 | 1.86 | 0.78 | 1.83 | 0.79 | 1.88 | 1.55 | |
| Variable | Low Exposure (d) n ≈ 165 | High Sexual Violence (c) n ≈ 156 | High Conflict-Related Violence (b) n ≈ 135 | Dual Exposure (a) n ≈ 104 | Cohen’s d | F # | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| SD | M | SD | M | SD | M | SD | M | |||
| Distraction | 0.73 | 1.52 | 0.75 | 1.51 | 0.69 | 1.47 | 0.78 | 1.63 | 0.99 | |
| Denial | 0.63 | 0.63 | 0.79 | 0.76 | 0.61 | 0.44 | 0.88 | 1.93 | 1.96 ab 1.39 ac 1.69 ad 0.45 bc | 10.3 ab,ac,ad,bc ** |
| Substance use | 0.8 | 0.43 | 0.95 | 0.65 | 0.67 | 1.31 | 1.07 | 0.79 | 0.58 ab 0.38 ad 0.80 bc | 7.59 ab,ad,bc ** |
| Avoidance | 0.78 | 1 | 0.77 | 1.04 | 0.68 | 0.88 | 0.71 | 1.13 | 0.35 ab | 2.81 ab * |
| Venting | 0.8 | 1.64 | 0.84 | 1.88 | 0.89 | 1.35 | 0.88 | 1.75 | 0.45 ab 0.61 bc 0.34 bd | 9.91 ab,bc,bd ** |
| Self-blame | 0.9 | 1.54 | 0.99 | 1.74 | 0.9 | 1.34 | 0.97 | 1.8 | 0.49 ab 0.42 bc | 6.25 ab,bc ** |
References
- Abu-Raiya, H., Sasson, T., Pargament, K. I., & Rosmarin, D. H. (2020). Religious coping and health and well-being among Jews and Muslims in Israel. The International Journal for the Psychology of Religion, 30(3), 202–215. [Google Scholar] [CrossRef]
- Ainamani, H. E., Elbert, T., Olema, D. K., & Hecker, T. (2020). Gender differences in response to war-related trauma and posttraumatic stress disorder—A study among the Congolese refugees in Uganda. BMC Psychiatry, 20, 17. [Google Scholar] [CrossRef] [PubMed]
- Albala, D., & Shapira, S. (2024). Parent-adolescent coping with prolonged geopolitical conflict: A qualitative analysis focusing on distress and resilience. Family Process, 63(3), 1502–1520. [Google Scholar] [CrossRef]
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders: DSM-5-TR (5th ed., text Revision). American Psychiatric Association Publishing. [Google Scholar]
- Antonovsky, A. (1979). Health, stress and coping: New perspectives on mental and physical wellbeing. Jossey-Bass. [Google Scholar]
- Antonovsky, A. (1987). Unraveling the mystery of health: How people manage stress and stay well (1st ed.). Jossey-Bass. [Google Scholar]
- Antonovsky, A. (1993). The structure and properties of the sense of coherence scale. Social Science & Medicine, 36(6), 725–733. [Google Scholar] [CrossRef]
- Association of Rape Crisis Centers in Israel. (2022). Sexual violence in Israel: A national plan to eliminate sexual violence in Israel and promote the rights of victims. Association of Rape Crisis Centers in Israel. Available online: https://fs.knesset.gov.il/25/Committees/25_cs_bg_2551494.pdf (accessed on 11 April 2025).
- Baron-Epel, O., Barerdi, V., Bellettiere, J., & Shalata, W. (2017). The relation between discrimination, sense of coherence and health varies according to ethnicity: A study among three distinct populations in Israel. Journal of Immigrant and Minority Health, 19, 1386–1396. [Google Scholar] [CrossRef]
- Ben Eliyahu, H., Hasson, Y., & Dagan-Buzaglo, N. (2024). The October 2023 war: Imapcts on women in Israel. Friedrich Ebert Foundation. [Google Scholar]
- Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107(2), 238–246. [Google Scholar] [CrossRef]
- Betke, K., Basińska, M. A., & Andruszkiewicz, A. (2021). Sense of coherence and strategies for coping with stress among nurses. BMC Nursing, 20(1), 107. [Google Scholar] [CrossRef]
- Boehm-Tabib, E., & Gelkopf, M. (2021). Posttraumatic growth: A deceptive illusion or a coping pattern that facilitates functioning? Psychological Trauma, 13(2), 193–201. [Google Scholar] [CrossRef] [PubMed]
- Bollen, K. A. (1989). Structural equations with latent variables. John Wiley & Sons. [Google Scholar]
- Braun-Lewensohn, O., Kalagy, T., & Abu-Kaf, S. (2025). Have coping resources and trust in state institutions helped Jews and Arabs to overcome stress during the Iron Swords War? European Journal of Investigation in Health, Psychology and Education (EJIHPE), 15(4), 59. [Google Scholar] [CrossRef]
- Braun-Lewensohn, O., & Mayer, C.-H. (2020). Salutogenesis and coping: Ways to overcome stress and conflict. International Journal of Environmental Research and Public Health, 17(18), 6667. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. (1979). The ecology of human development. Harvard University Press. [Google Scholar]
- Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. In K. A. Bollen, & J. S. Long (Eds.), Testing structural equation models (pp. 136–162). Sage. [Google Scholar]
- Carver, C. S. (1997). You want to measure coping but your protocol’s too long: Consider the brief COPE. International Journal of Behavioral Medicine, 4(1), 92–100. [Google Scholar] [CrossRef] [PubMed]
- Chudzicka-Czupała, A., Hapon, N., Chiang, S. K., Żywiołek-Szeja, M., Karamushka, L., Lee, C. T., Grabowski, D., Paliga, M., Rosenblat, J. D., McIntyre, R. S., & Chen, Y. L. (2023). Depression, anxiety and post-traumatic stress during the 2022 Russo-Ukrainian war, a comparison between populations in Poland, Ukraine, and Taiwan. Scientific Reports, 13(1), 3602. [Google Scholar] [CrossRef]
- Chung, M. C., & Freh, F. M. (2019). The trajectory of bombing-related posttraumatic stress disorder among Iraqi civilians: Shattered world assumptions and altered self-capacities as mediators; attachment and crisis support as moderators. Psychiatry Research, 273, 1–8. [Google Scholar] [CrossRef]
- Cohen-Louck, K., & Zvi, L. (2022). A model for predicting post-traumatic stress disorder due to exposure to chronic political violence: Big five personality traits, ego-resiliency, and coping. Journal of Interpersonal Violence, 37(23–24), NP23241–NP23261. [Google Scholar] [CrossRef] [PubMed]
- Cooper, B. (2015). Intersectionality (L. Disch, & M. Hawkesworth, Eds.; Vol. 1). Oxford University Press. [Google Scholar] [CrossRef]
- Daneshvar, S., Shafiei, M., & Basharpoor, S. (2022). Group-based compassion-focused therapy on experiential avoidance, meaning-in-life, and sense of coherence in female survivors of intimate partner violence with PTSD: A randomized controlled trial. Journal of Interpersonal Violence, 37(7–8), NP4187–NP4211. [Google Scholar] [CrossRef]
- DeCandia, C., & Guarino, K. (2015). Trauma-informed care: An ecological response. Journal of Child and Youth Care Work, 25, 7–32. [Google Scholar] [CrossRef]
- Domhardt, M., Münzer, A., Fegert, J. M., & Goldbeck, L. (2015). Resilience in survivors of child sexual abuse. Trauma, Violence, & Abuse, 16(4), 476–493. [Google Scholar] [CrossRef]
- Dube, S. R., & Rishi, S. (2017). Utilizing the salutogenic paradigm to investigate well-being among adult survivors of childhood sexual abuse and other adversities. Child Abuse & Neglect, 66, 130–141. [Google Scholar] [CrossRef]
- Fernández-Fillol, C., Pitsiakou, C., Perez-Garcia, M., Teva, I., & Hidalgo-Ruzzante, N. (2021). Complex PTSD in survivors of intimate partner violence: Risk factors related to symptoms and diagnoses. European Journal of Psychotraumatology, 12(1), 2003616. [Google Scholar] [CrossRef]
- Goral, A., Feder-Bubis, P., Lahad, M., Galea, S., O’Rourke, N., & Aharonson-Daniel, L. (2021). Development and validation of the Continuous Traumatic Stress Response scale (CTSR) among adults exposed to ongoing security threats. PLoS ONE, 16(5), e0251724. [Google Scholar] [CrossRef]
- Greene, T., Itzhaky, L., Bronstein, I., & Solomon, Z. (2018). Psychopathology, risk, and resilience under exposure to continuous traumatic stress: A systematic review of studies among adults living in southern Israel. Traumatology, 24(2), 83–103. [Google Scholar] [CrossRef]
- Hailes, H. P., Yu, R., Danese, A., & Fazel, S. (2019). Long-term outcomes of childhood sexual abuse: An umbrella review. The Lancet Psychiatry, 6(10), 830–839. [Google Scholar] [CrossRef] [PubMed]
- Herman, J. L. (1992). Trauma and recovery: The aftermath of violence—From domestic abuse to political terror. Basic Books. [Google Scholar]
- Hirsch, L. A. (2022). The role of coping self-efficacy, coping strategies, and resiliency following sexual assault. Seattle Pacific University. [Google Scholar]
- Hoyle, R. H. (Ed.). (1995). Structural equation modeling: Concepts, issues, and applications. Sage. [Google Scholar]
- Jaffe, A. E., Blayney, J. A., Schallert, M. R., Edwards, M. E., & Dworkin, E. R. (2022). Social network changes and disclosure responses after sexual assault. Psychology of Women Quarterly, 46(3), 299–315. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, A. E., DiLillo, D., Hoffman, L., Haikalis, M., & Dykstra, R. E. (2015). Does it hurt to ask? A meta-analysis of participant reactions to trauma research. Clinical Psychology Review, 40, 40–56. [Google Scholar] [CrossRef] [PubMed]
- Kamin, R., Reter, A., & Amital, D. (2023). Where is the front? The front is here: Impressions from the Department of Psychiatry, Barzilai Medical Center in Ashkelon, the “Iron Swords” War, October 2023. Harfua, 162(9), 548–551. (In Hebrew). [Google Scholar]
- Kaye-Tzadok, A., & Davidson-Arad, B. (2016). Posttraumatic growth among women survivors of childhood sexual abuse: Its relation to cognitive strategies, posttraumatic symptoms, and resilience. Psychological Trauma: Theory, Research, Practice, and Policy, 8(5), 550–558. [Google Scholar] [CrossRef]
- Kazlauskas, E., Gailiene, D., Vaskeliene, I., & Skeryte-Kazlauskiene, M. (2017). Intergenerational transmission of resilience? Sense of coherence is associated between Lithuanian survivors of political violence and their adult offspring. Frontiers in Psychology, 8, 1677. [Google Scholar] [CrossRef]
- Koren-Karie, N., Oppenheim, D., & Getzler-Yosef, R. (2008). Shaping children’s internal working models through mother–child dialogues: The importance of resolving past maternal trauma. Attachment & Human Development, 10(4), 465–483. [Google Scholar] [CrossRef]
- Korosteleva, E. A., & Petrova, I. (2022). What makes communities resilient in times of complexity and change? Cambridge Review of International Affairs, 35(2), 137–157. [Google Scholar] [CrossRef]
- Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. Springer Pub. Co. [Google Scholar]
- Leykin, D., Lahad, M., Cohen, O., Goldberg, A., & Aharonson-Daniel, L. (2013). Conjoint community resiliency assessment measure-28/10 items (CCRAM28 and CCRAM10): A self-report tool for assessing community resilience. American Journal of Community Psychology, 52(3–4), 313–323. [Google Scholar] [CrossRef]
- Mahoney, C. T., Lynch, S. M., & Benight, C. C. (2021). The indirect effect of coping self-efficacy on the relation between sexual violence and PTSD symptoms. Journal of Interpersonal Violence, 36(21–22), 9996–10012. [Google Scholar] [CrossRef] [PubMed]
- McGee, S. L., Höltge, J., Maercker, A., & Thoma, M. V. (2018). Sense of coherence and stress-related resilience: Investigating the mediating and moderating mechanisms in the development of resilience following stress or adversity. Frontiers in Psychiatry, 9, 378. [Google Scholar] [CrossRef] [PubMed]
- McIver, J. P., & Carmines, E. G. (1981). Unidimensional scaling (No. 24). Sage. [Google Scholar]
- Mugisha, J. (2021). Sociocultural aspects of health promotion in palliative care in Uganda. In G. Haugan, & M. Eriksson (Eds.), Health promotion in health care—Vital theories and research (pp. 303–312). Spring. [Google Scholar]
- Muldoon, O. T., Lowe, R. D., Jetten, J., Cruwys, T., & Haslam, S. A. (2021). Personal and political: Post-traumatic stress through the lens of social identity, power, and politics. Political Psychology, 42(3), 501–533. [Google Scholar] [CrossRef]
- Nurius, P. S., Uehara, E., & Zatzick, D. F. (2013). Intersection of stress, social disadvantage, and life course processes: Reframing trauma and mental health. American Journal of Psychiatric Rehabilitation, 16(2), 91–114. [Google Scholar] [CrossRef] [PubMed]
- Okeke-Ihejirika, P., Yohani, S., & McMenemy, C. (2018). Support programs for women survivors of sexualized gender-based violence from African conflict zones: A contextual review. Sage Open, 8(2), 2158244018784342. [Google Scholar] [CrossRef]
- Pat-Horenczyk, R., & Schiff, M. (2019). Continuous traumatic stress and the life cycle: Exposure to repeated political violence in Israel. Current Psychiatry Reports, 21(8), 71. [Google Scholar] [CrossRef]
- Punamäki, R.-L., Qouta, S. R., & Diab, S. Y. (2019). The role of maternal attachment in mental health and dyadic relationships in war trauma. Heliyon, 5(12), e02867. [Google Scholar] [CrossRef]
- Sa’ar, A., Sachs, D., & Aharoni, S. (2011). Between a gender and a feminist analysis. International Sociology, 26(1), 50–73. [Google Scholar] [CrossRef]
- Sachs, D., Sa’ar, A., & Aharoni, S. (2007). “How can I feel for others when I myself am beaten?” The impact of the armed conflict on women in Israel. Sex Roles, 57(7–8), 593–606. [Google Scholar] [CrossRef]
- Sagy, S., & Braun-Lewensohn, O. (2009). Adolescents under rocket fire: When are coping resources significant in reducing emotional distress? Global Health Promotion, 16(4), 5–15. [Google Scholar] [CrossRef]
- Scarduzio, J. A., Sheff, S. E., & Smith, M. (2018). Coping and sexual harassment: How victims cope across multiple settings. Archives of Sexual Behavior, 47(2), 327–340. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, S. K., Becker, N., King, L., Horsch, A., & Michael, T. (2019). The relationship between sense of coherence and post-traumatic stress: A meta-analysis. European Journal of Psychotraumatology, 10(1), 1562839. [Google Scholar] [CrossRef]
- Shapira, S. (2022). Trajectories of community resilience over a multi-crisis period: A repeated cross-sectional study among small rural communities in Southern Israel. International Journal of Disaster Risk Reduction, 76, 103006. [Google Scholar] [CrossRef]
- Shapira, S., Cohen, O., & Aharonson-Daniel, L. (2020). The contribution of personal and place-related attributes to the resilience of conflict-affected communities. Journal of Environmental Psychology, 72, 101520. [Google Scholar] [CrossRef]
- Shapira, S., Sold, A., & Refaeli, T. (2025). The interplay of personal and collective resilience and mental health during prolonged conflict: Insights from young adults in Israel. Stress and Health, 41(3), e70047. [Google Scholar] [CrossRef] [PubMed]
- Slopen, N., Meyer, C., & Williams, D. R. (2018). Cumulative stress and health. In C. D. Ryff, & R. F. Krueger (Eds.), The Oxford handbook of integrative health science (pp. 75–82). Oxford University Press. [Google Scholar] [CrossRef]
- Solberg, B. (2021). The ethics of health promotion: From public health to health care. In G. Haugan, & M. Eriksson (Eds.), Health promotion in health care—Vital theories and research (pp. 23–33). Springer. [Google Scholar] [CrossRef]
- Stein, J. Y., Levin, Y., Gelkopf, M., Tangir, G., & Solomon, Z. (2018). Traumatization or habituation? A four-wave investigation of exposure to continuous traumatic stress in Israel. International Journal of Stress Management, 25(S1), 137–153. [Google Scholar] [CrossRef]
- Stevanović, A., Frančišković, T., & Vermetten, E. (2016). Relationship of early-life trauma, war-related trauma, personality traits, and PTSD symptom severity: A retrospective study on female civilian victims of war. European Journal of Psychotraumatology, 7(1), 30964. [Google Scholar] [CrossRef] [PubMed]
- Stockman, D., Haney, L., Uzieblo, K., Littleton, H., Keygnaert, I., Lemmens, G., & Verhofstadt, L. (2023). An ecological approach to understanding the impact of sexual violence: A systematic meta-review. Frontiers in Psychology, 14, 1032408. [Google Scholar] [CrossRef]
- Ungar, M. (Ed.). (2011). The social ecology of resilience: A handbook of theory and practice. Springer Science & Business Media. [Google Scholar]
- van der Kolk, B. A. (2021). The body keeps the score: Brain, mind, and body in the healing of trauma (I. Rilov, Trans.). A. Bar, Scientific Ed. Hebrew Translation. Pardes Publishing. (Original work published 2014). [Google Scholar]
- Wachter, K., Murray, S. M., Hall, B. J., Annan, J., Bolton, P., & Bass, J. (2018). Stigma modifies the association between social support and mental health among sexual violence survivors in the Democratic Republic of Congo: Implications for practice. Anxiety, Stress, and Coping, 31(4), 459–474. [Google Scholar] [CrossRef]
- Weathers, F. W., Litz, B. T., Keane, T. M., Palmieri, P. A., Marx, B. P., & Schnurr, P. P. (2013). The PTSD checklist for DSM-5 (PCL-5). Scale Available from the National Center for PTSD. Available online: https://www.ptsd.va.gov/ (accessed on 30 March 2025).
- World Health Organization (WHO) and partners. (2021). Devastatingly pervasive: 1 in 3 women globally experience violence [Joint News Release]. WHO. [Google Scholar]
- Zelis, T., & Shapira, S. (2025). The moderating impact of personal and collective resilience resources on postpartum depression in conflict-affected environments. Midwifery, 147, 104425. [Google Scholar] [CrossRef]
| Variable | The Entire Sample n = 568 | Dual Low Exposure n ≈ 171 | High Exposure to Sexual Violence n ≈ 156 | High Exposure to Conflict-Related Violence n ≈ 137 | Dual High Exposure n ≈ 104 | χ2/F | |
|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | ||||
| Age (M ± SD) | 18–81 | 41.44 ± 12.99 | 40.29 ± 12.3 | 41.3 ± 12.48 | 43.28 ± 13.82 | 43.28 ± 13.68 | 1.27 |
| Marital status | In a relationship | 406 (71) | 127 (73.8) | 99 (63.5) | 109 (79) | 71 (67) | 9.66 * |
| Not in a relationship | 166 (29) | 45 (26.2) | 57 (36.5) | 29 (21) | 35 (33) | ||
| Level of religiosity | Secular | 361 (65.75) | 100 (60.24) | 110 (72.36) | 84 (63.63) | 67 (67.67) | 5.61 |
| Traditional/religious/ultra-orthodox | 188 (34.24) | 67 (39.75) | 42 (27.63) | 48 (36.36) | 32 (32.32) | ||
| Education | Academic | 422 (75.3) | 134 (80.2) | 109 (71.2) | 101 (74.8) | 75 (73.5) | 3.72 |
| Not academic | 138 (24.6) | 33 (19.8) | 44 (28.8) | 34 (25.2) | 27 (26.5) | ||
| Income level | Below average | 282 (49.3) | 76 (44.4) | 77 (49.4) | 63 (46) | 66 (63.5) | 13.1 * |
| Average or close to average | 140 (24.5) | 48 (28.1) | 38 (24.4) | 40 (29.2) | 14 (13.5) | ||
| Above average | 146 (25.5) | 47 (27.5) | 41 (26.3) | 34 (24.85) | 24 (23.1) | ||
| Employment | Unemployed | 71 (13.2) | 21 (13) | 20 (12.8) | 11 (8) | 19 (17) | 6.48 |
| Temporary jobs/part-time job | 147 (27.3) | 48 (29.8) | 37 (23.7) | 35 (25.4) | 27 (25.4) | ||
| Full-time job/freelancer | 320 (59.5) | 92 (57.1) | 86 (55.1) | 86 (62.3) | 56 (52.8) |
| Item | Mean | SD |
|---|---|---|
| Incendiary balloons/kites | 1.66 | 1.09 |
| Rocket-fire | 3.00 | 1.09 |
| Tunnel threat or fear of terrorist infiltration | 1.69 | 1.02 |
| Evacuation from home due to conflict-related threat | 1.69 | 1.00 |
| Physical injury | 1.05 | 0.31 |
| Injury of someone who is close to the participant | 1.50 | 0.87 |
| Item | Mean | SD |
|---|---|---|
| Has anyone kissed or touched you in a sexual manner without your consent? | 2.44 | 0.97 |
| Has anyone exposed their genitals, sexual acts, or any form of pornographic material to you? | 1.92 | 1.01 |
| Has anyone published a picture, recording, or video focusing on your sexuality without your consent? | 1.06 | 0.31 |
| Has anyone inserted a body part or object into your genitals, anus, or mouth without your consent? | 1.43 | 0.84 |
| Variable | Scale Range | Low Exposure (d) n ≈ 165 | High Sexual Violence (c) n ≈ 156 | High Conflict-Related Violence (b) n ≈ 135 | Dual Exposure (a) n ≈ 104 | Cohen’s d | F # | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SD | M | SD | M | SD | M | SD | M | ||||
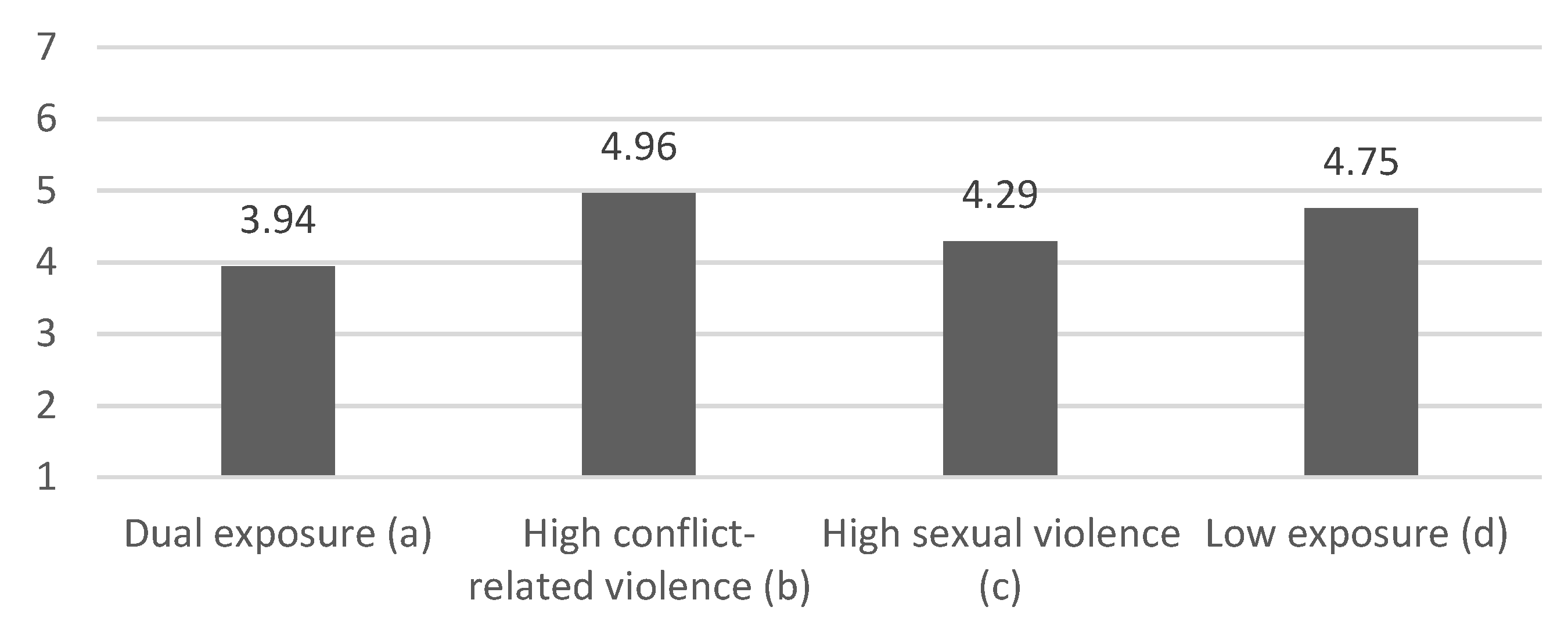
| SOC | 1–7 | 1.01 | 4.75 | 1.24 | 4.29 | 1.03 | 4.96 | 1.33 | 3.94 | 0.79 ab 0.68 ad 0.59 bc 0.40 cd | 19.72 ab,ad,bc,cd ** |
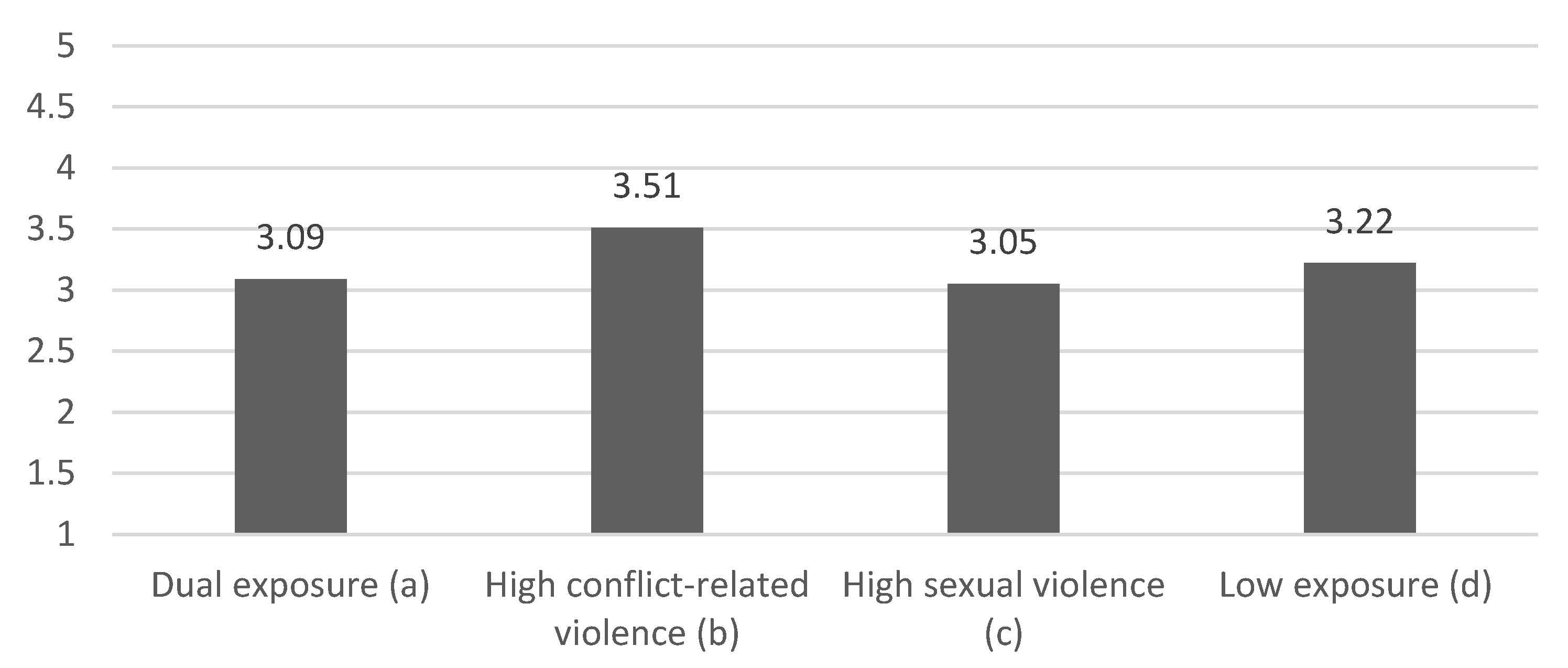
| CR | 1–5 | 0.82 | 3.22 | 0.8 | 3.05 | 0.8 | 3.51 | 0.84 | 3.09 | 0.55 ab 0.62 bc 0.38 bd | 9.3 ab,bc,bd ** |
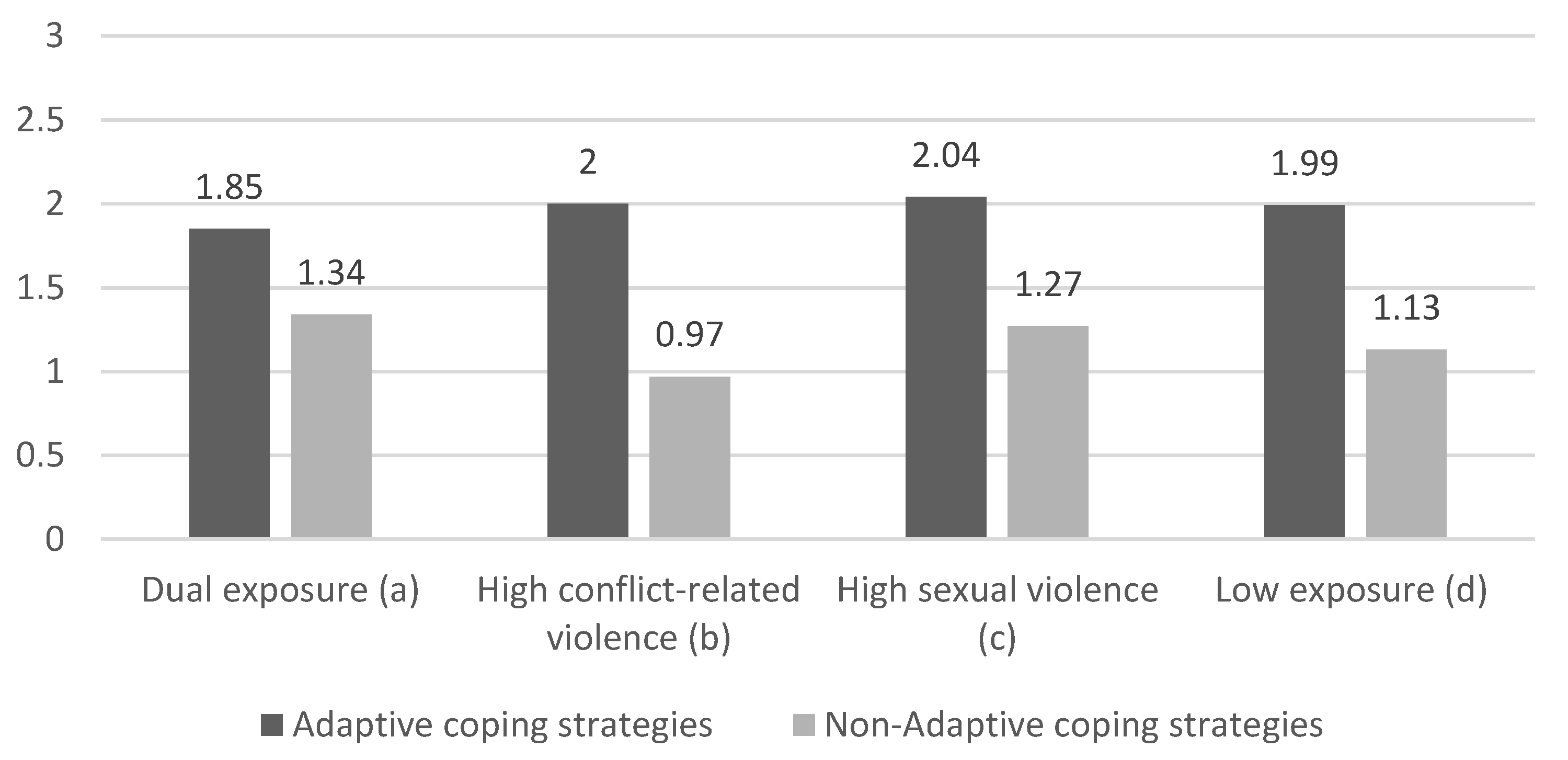
| Adaptive coping strategies | 0–3 | 0.45 | 1.99 | 0.5 | 2.04 | 0.54 | 2 | 0.53 | 1.85 | 0.36 ac | 3.03 ac * |
| Non-adaptive coping strategies | 0–3 | 0.46 | 1.13 | 0.55 | 1.27 | 0.47 | 0.97 | 0.62 | 1.34 | 0.67 ab 0.4 ad 0.58 bc | 12.48 ab,ad,bc ** |
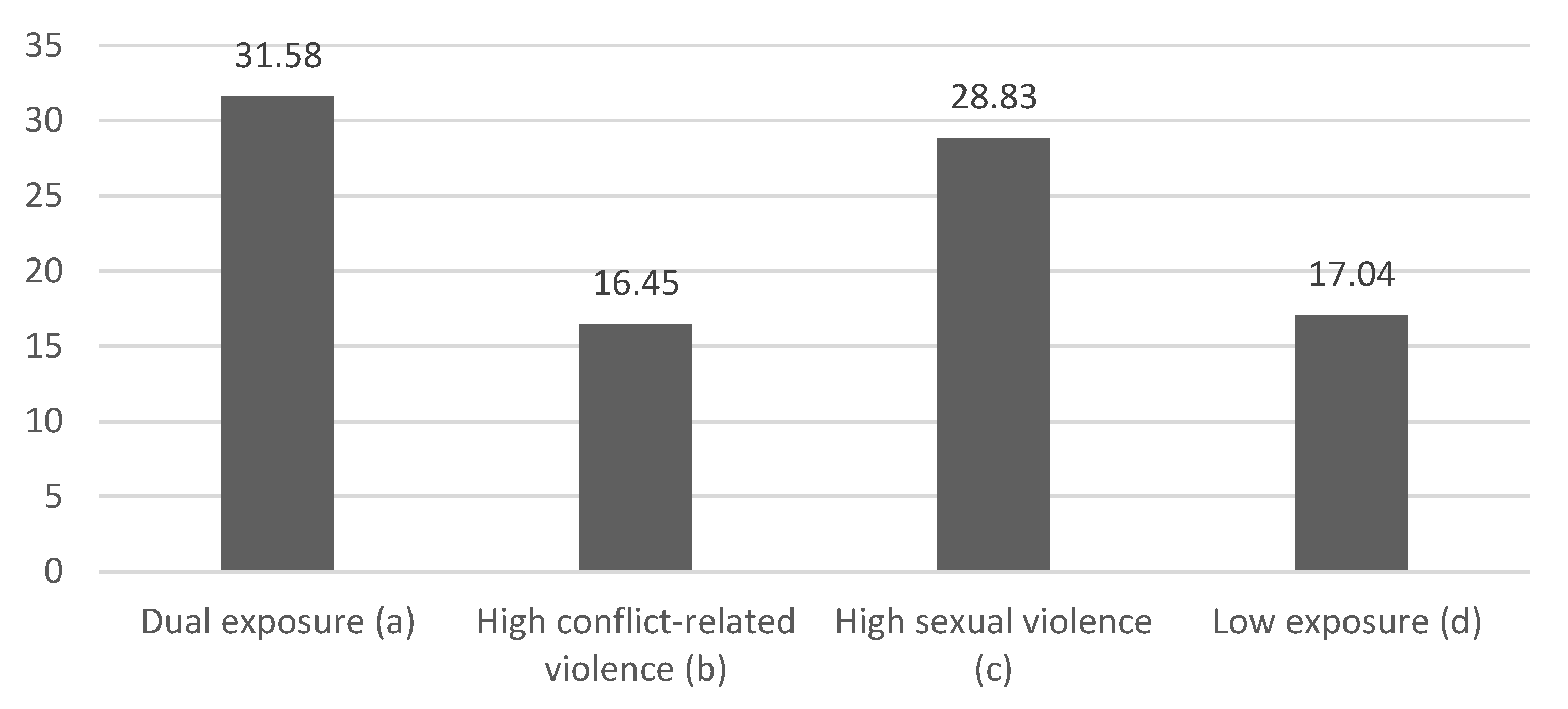
| Post-traumatic symptoms | 0–80 | 14.37 | 17.04 | 18.64 | 28.83 | 13.76 | 16.45 | 18.43 | 31.58 | 0.40 ab 0.88 ad 0.75 bc 0.70 cd | 31.39 ab,ad,bc,cd ** |
| Variable | Sexual Violence Exposure | Conflict-Related Violence Exposure | Combined Exposure to Conflict-Related Violence and Sexual Violence | SOC | CR | Adaptive Coping Strategies | Non-Adaptive Coping Strategies | PTSD Symptoms |
|---|---|---|---|---|---|---|---|---|
| Sexual violence exposure | 1 | |||||||
| Conflict-related violence exposure | 0.16− | 1 | ||||||
| Combined exposure to conflict-related violence and sexual violence | 0.90 ** | 0.40 ** | 1 | |||||
| SOC | −0.38 ** | 0.009 | −0.34 ** | 1 | ||||
| CR | −0.21 ** | 0.16 ** | −0.13 ** | 0.41 ** | 1 | |||
| Adaptive coping strategies | −0.10 * | −0.03 | −0.10 * | 0.29 ** | 0.16 ** | 1 | ||
| Non-adaptive coping strategies | 0.36 ** | −0.07 | 0.29 ** | −0.67 ** | −0.33 ** | −0.09 * | 1 | |
| PTSD symptoms | 0.50 ** | −0.005 | 0.44 ** | −0.71 ** | −0.39 ** | −0.22 ** | 0.62 ** | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the University Association of Education and Psychology. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bar, N.; Shapira, S.; Braun-Lewensohn, O. Cumulative Violence and Post-Traumatic Stress: An Integrative Model of Coping and Resilience Among Women Exposed to Sexual and Conflict-Related Violence. Eur. J. Investig. Health Psychol. Educ. 2025, 15, 110. https://doi.org/10.3390/ejihpe15060110
Bar N, Shapira S, Braun-Lewensohn O. Cumulative Violence and Post-Traumatic Stress: An Integrative Model of Coping and Resilience Among Women Exposed to Sexual and Conflict-Related Violence. European Journal of Investigation in Health, Psychology and Education. 2025; 15(6):110. https://doi.org/10.3390/ejihpe15060110
Chicago/Turabian StyleBar, Naama, Stav Shapira, and Orna Braun-Lewensohn. 2025. "Cumulative Violence and Post-Traumatic Stress: An Integrative Model of Coping and Resilience Among Women Exposed to Sexual and Conflict-Related Violence" European Journal of Investigation in Health, Psychology and Education 15, no. 6: 110. https://doi.org/10.3390/ejihpe15060110
APA StyleBar, N., Shapira, S., & Braun-Lewensohn, O. (2025). Cumulative Violence and Post-Traumatic Stress: An Integrative Model of Coping and Resilience Among Women Exposed to Sexual and Conflict-Related Violence. European Journal of Investigation in Health, Psychology and Education, 15(6), 110. https://doi.org/10.3390/ejihpe15060110