


Trends in Suicidal Mortality and Motives among Working-Ages Individuals in Japan during 2007–2022

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Statistical Analysis
3. Results
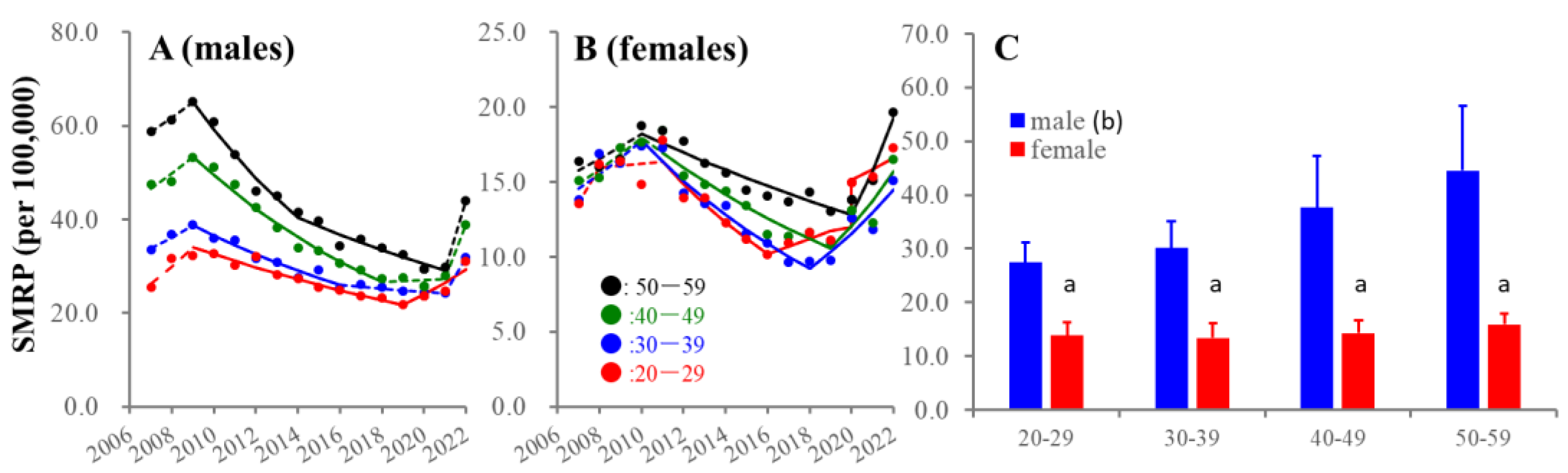
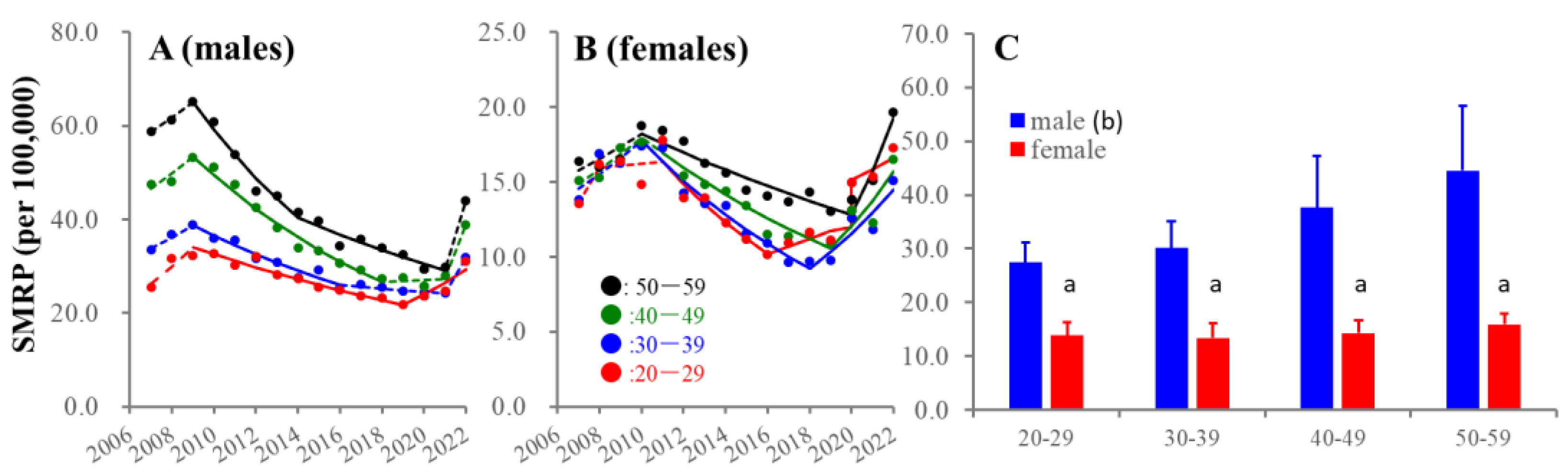
3.1. SMRPs Disaggregated by Se, Age and Suicidal Motives from 2007–2022
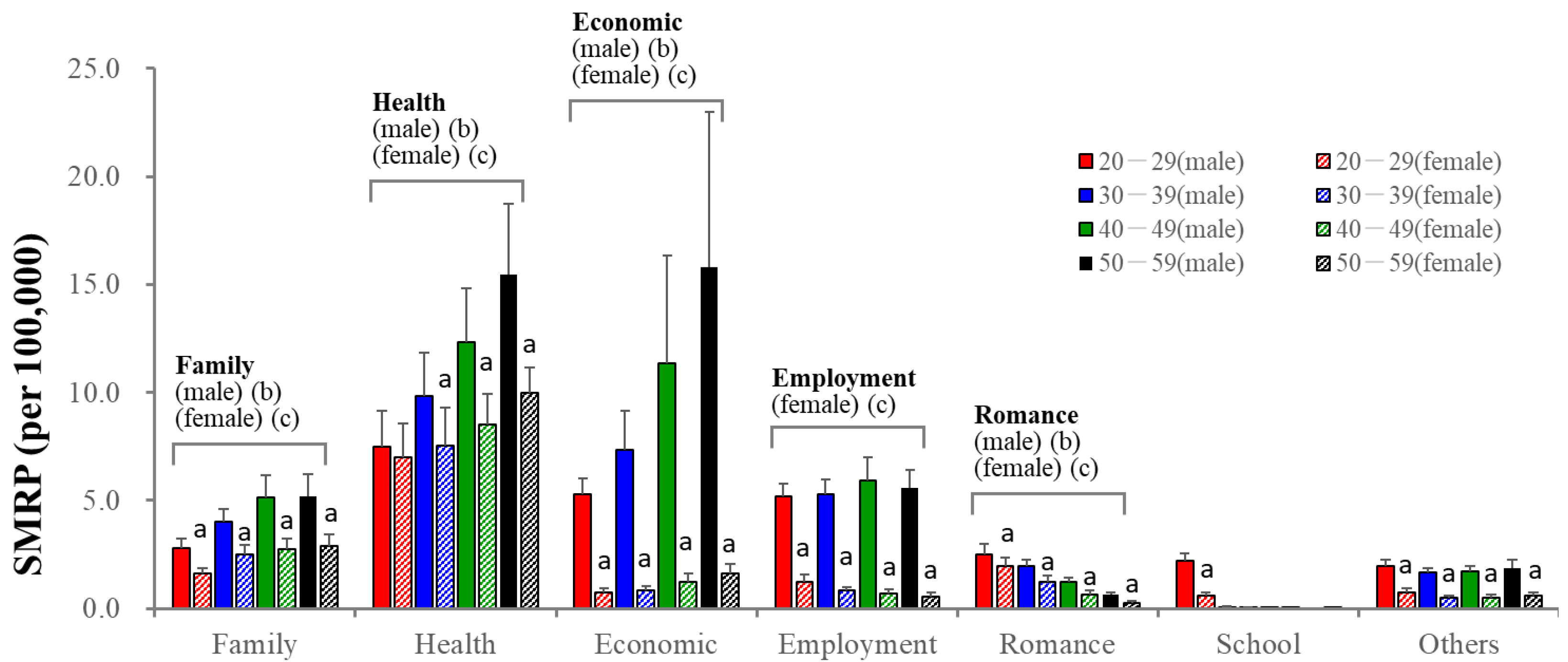
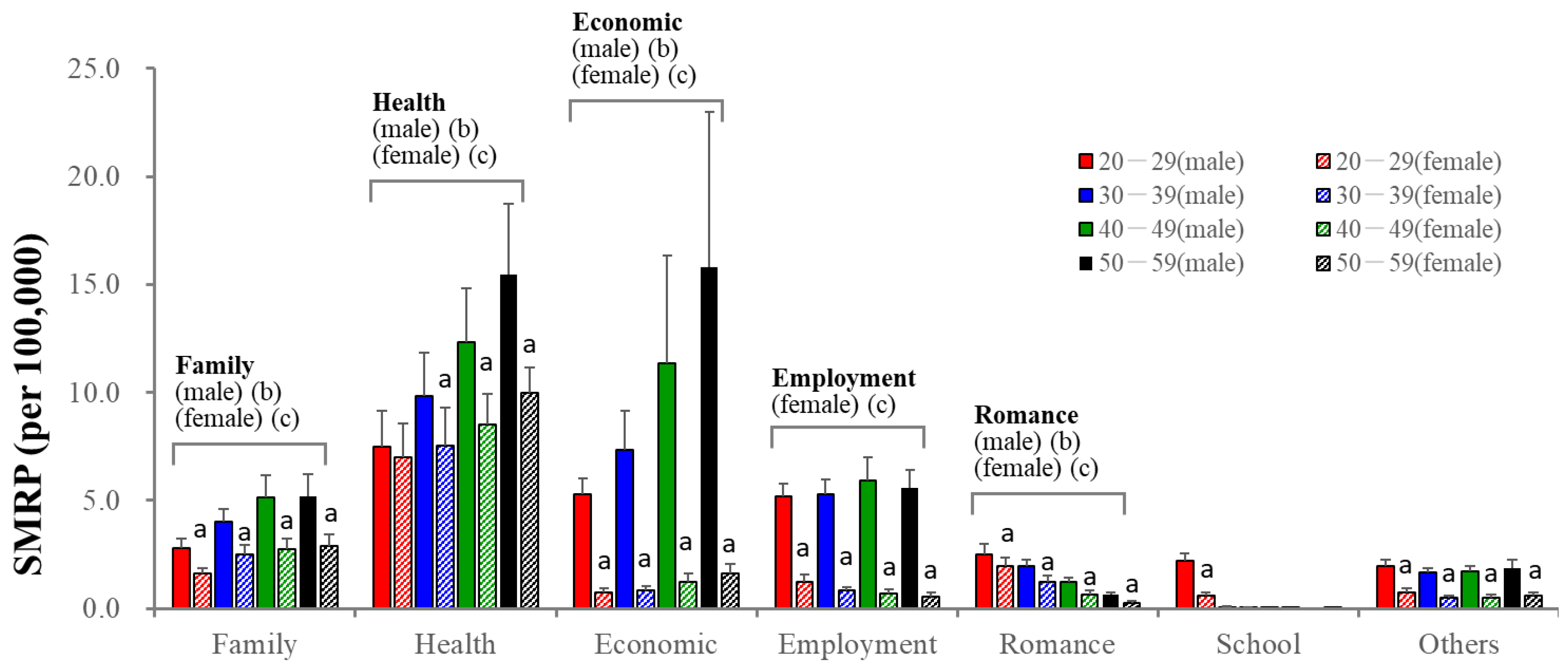
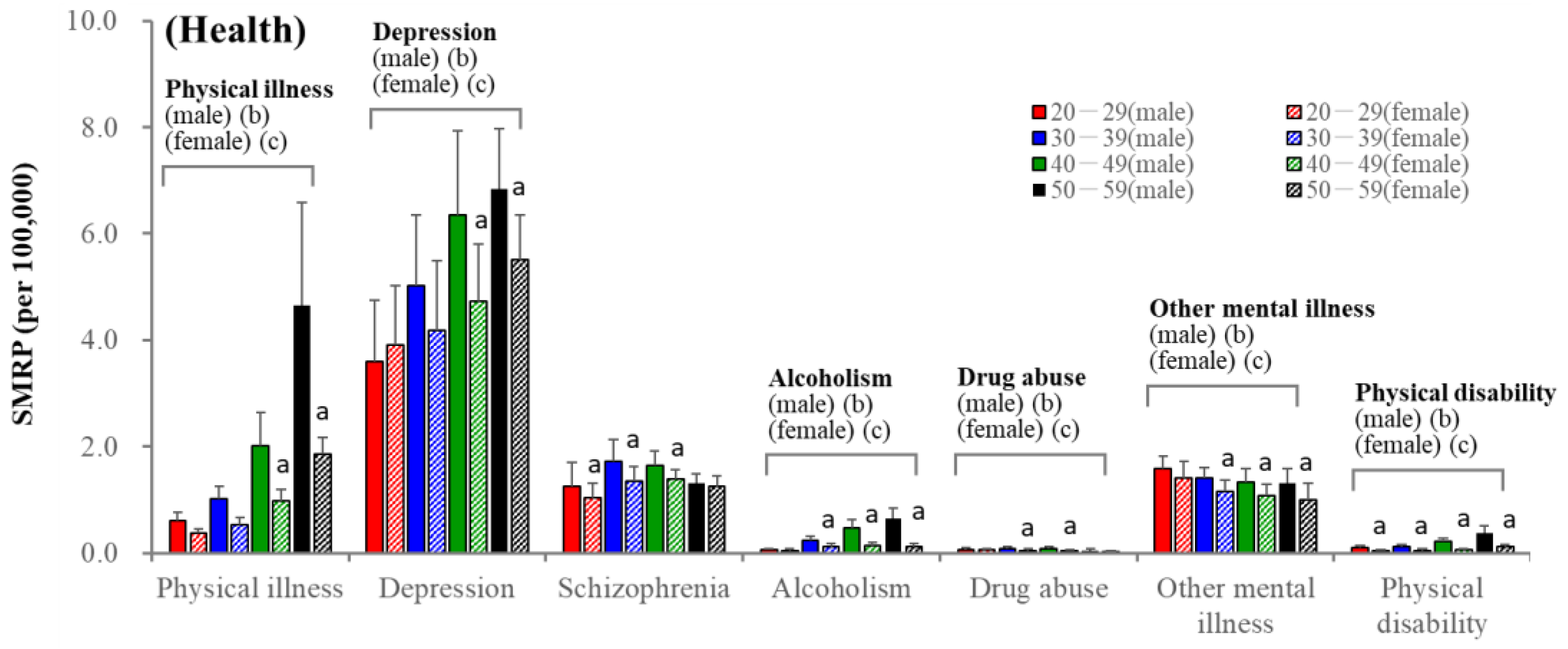
3.2. Age- and Sex-Dependent Impacts of Suicidal Motives
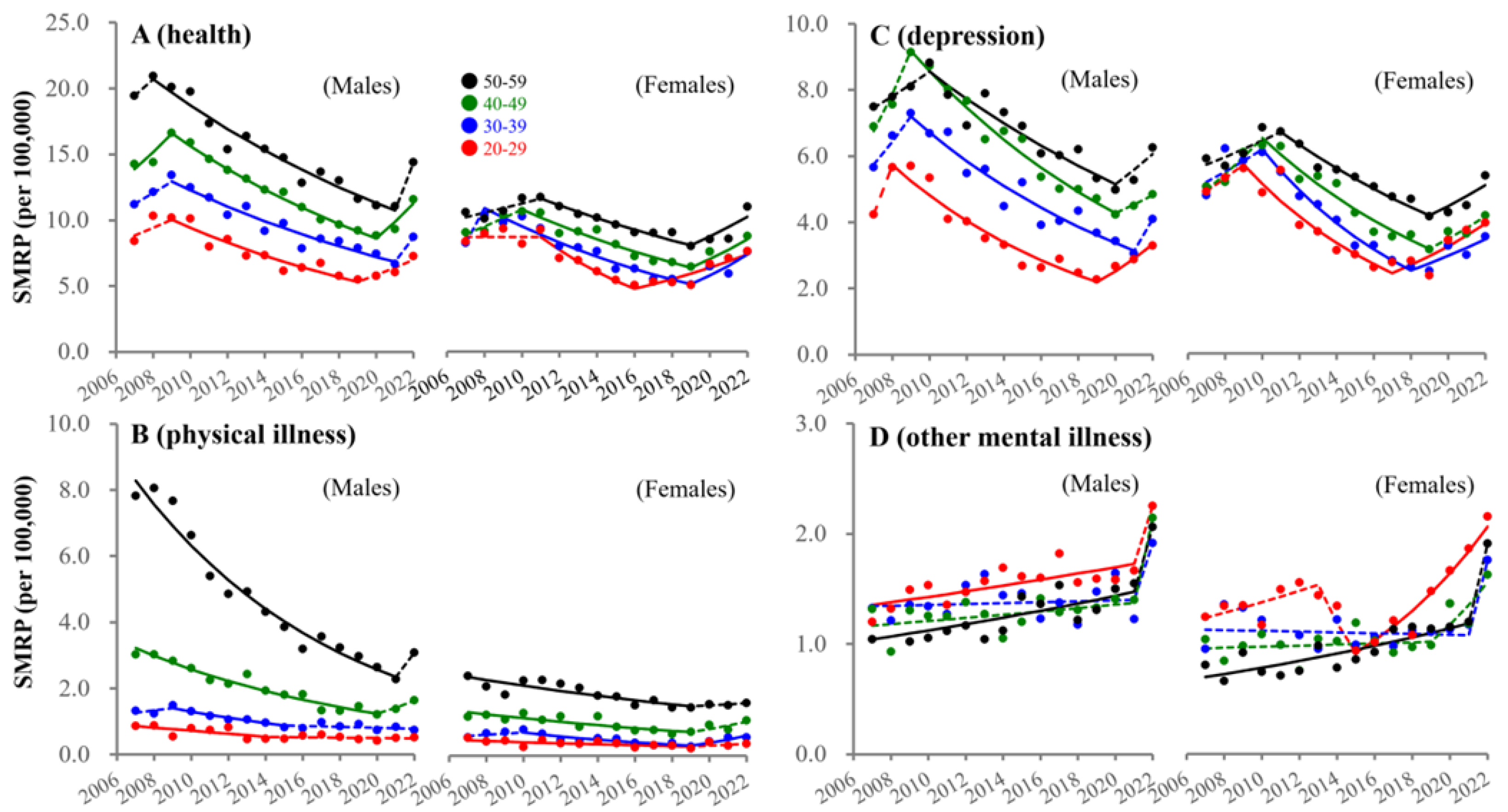
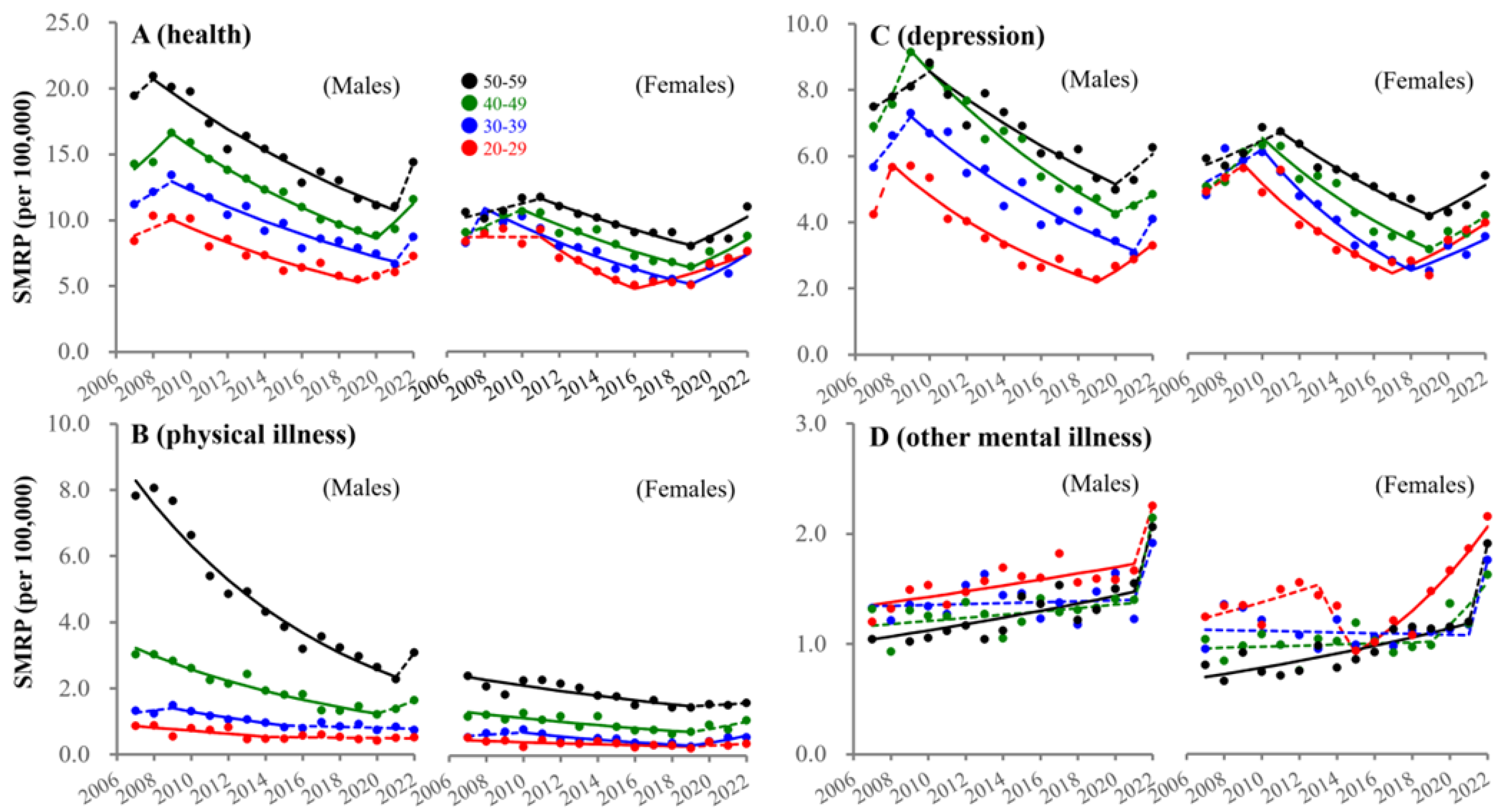
3.3. Fluctuations in SMRPs Caused by Health-Related Motives
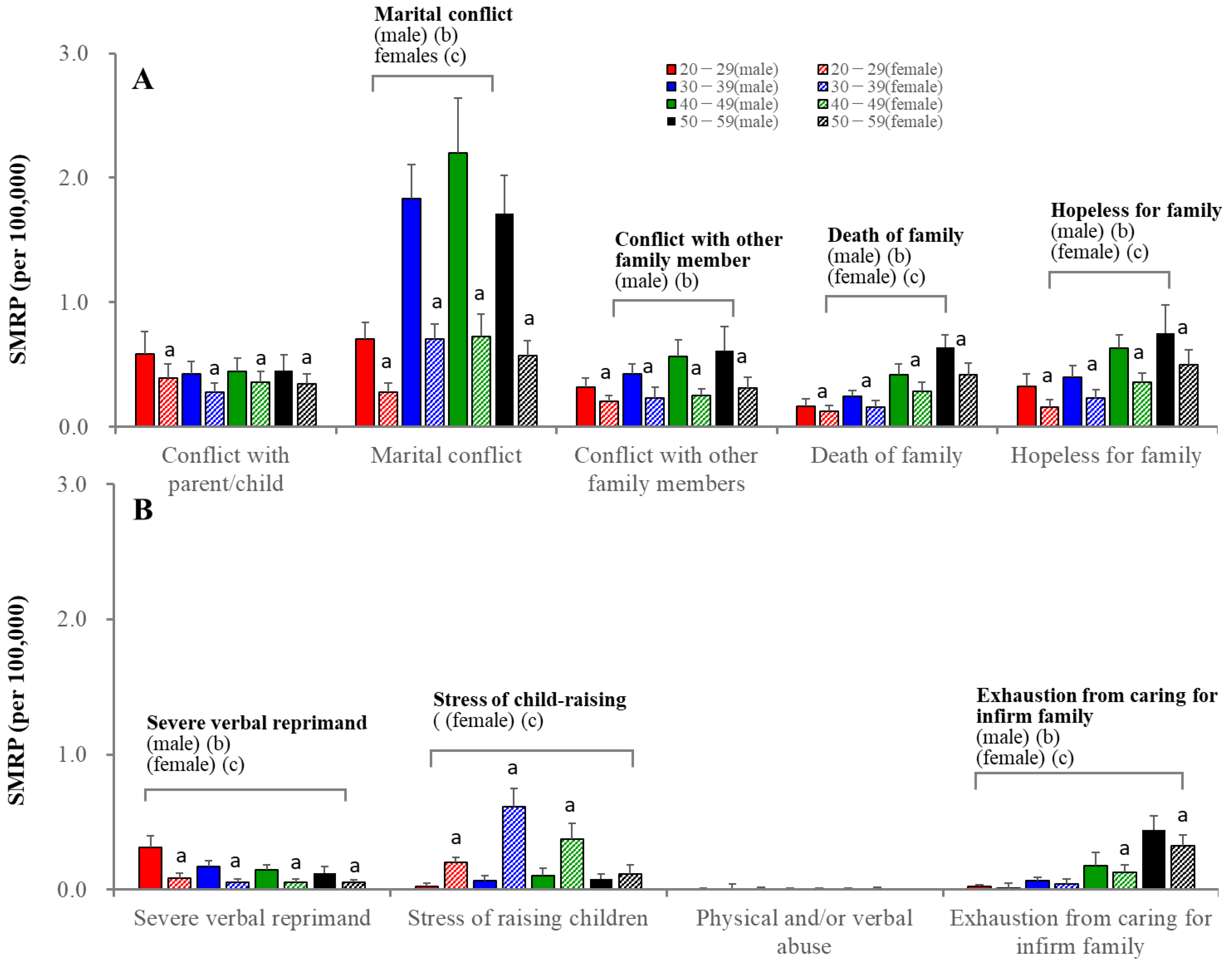
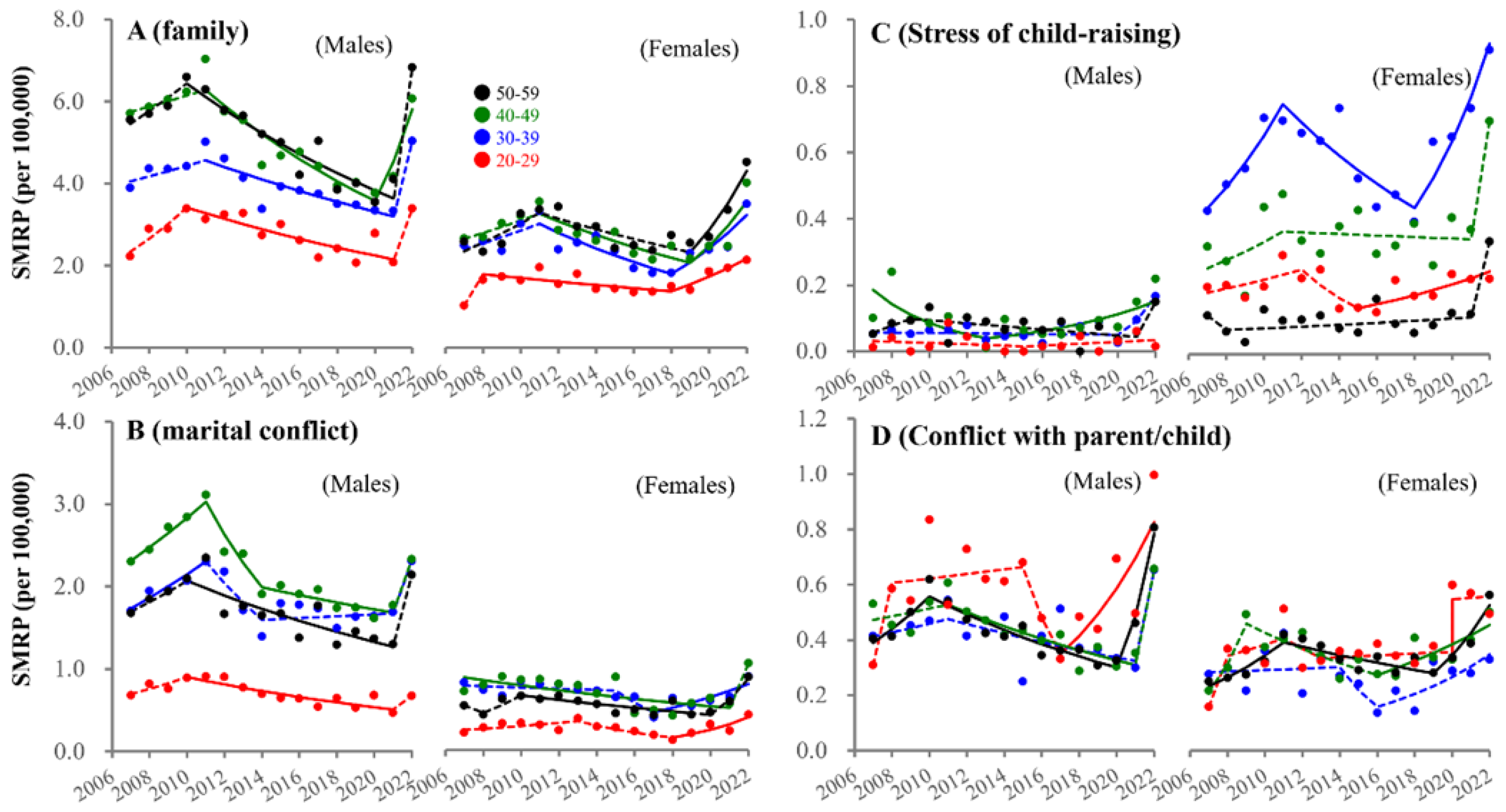
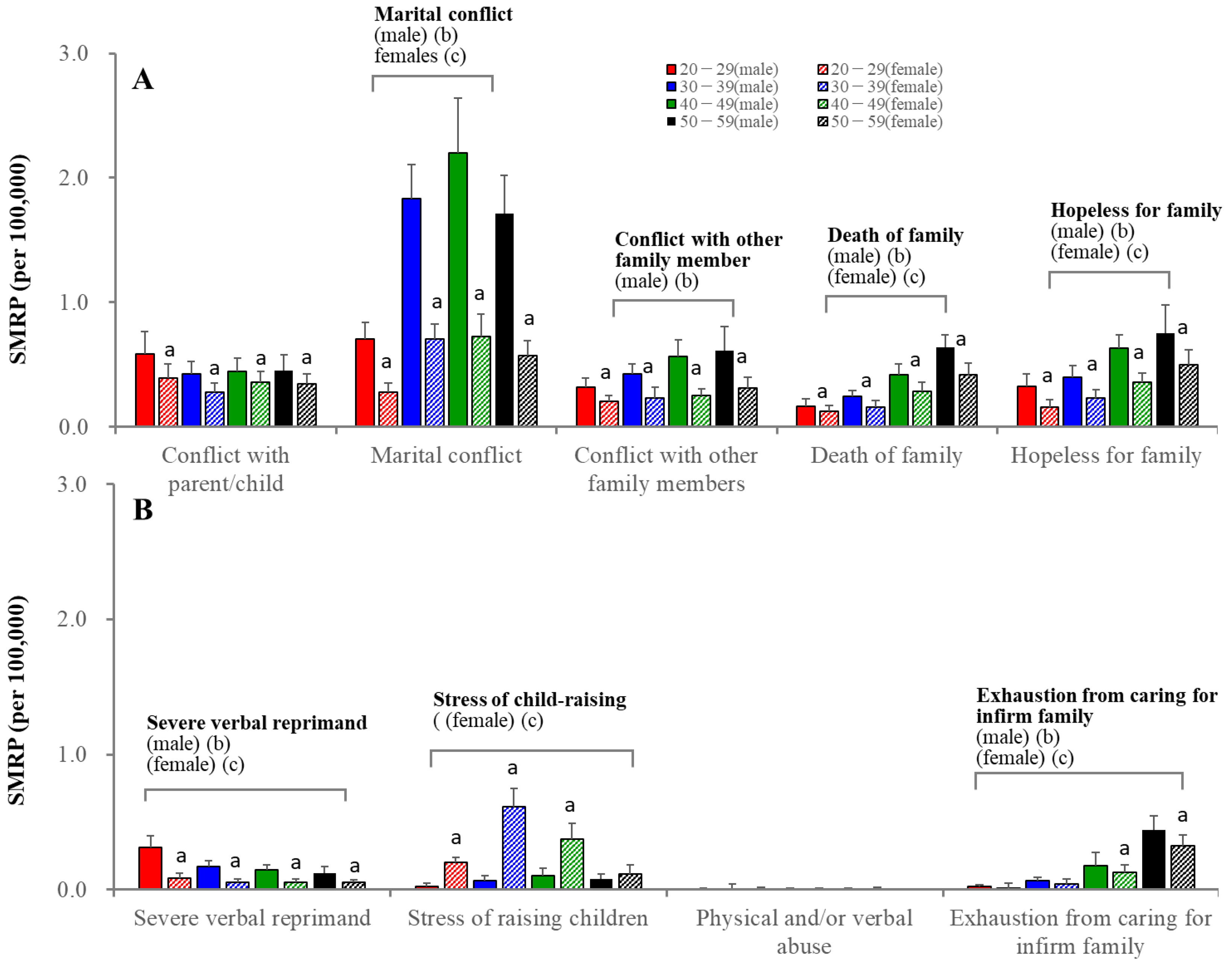
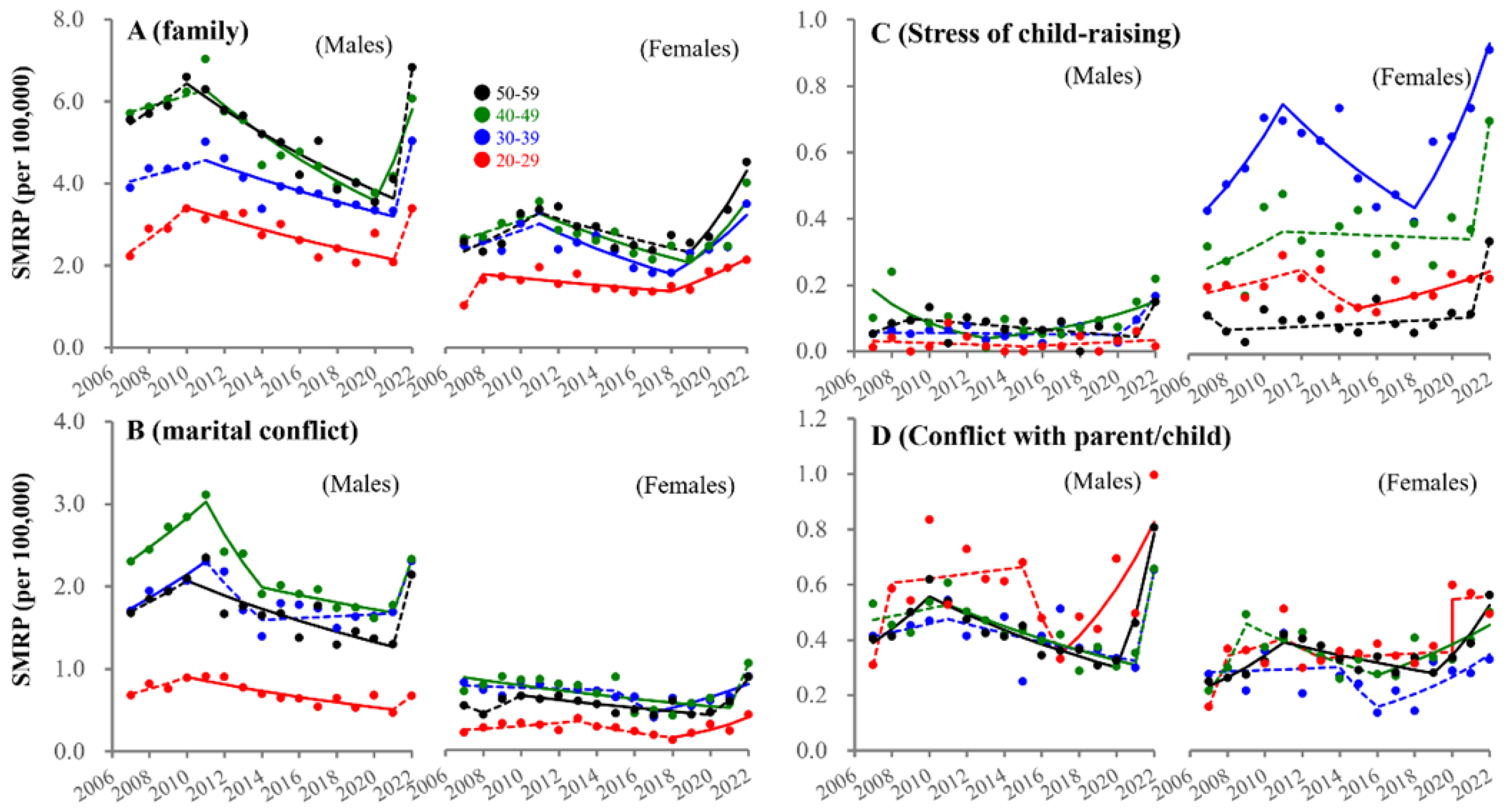
3.4. Fluctuations in SMRPs Caused by Family-Related Motive
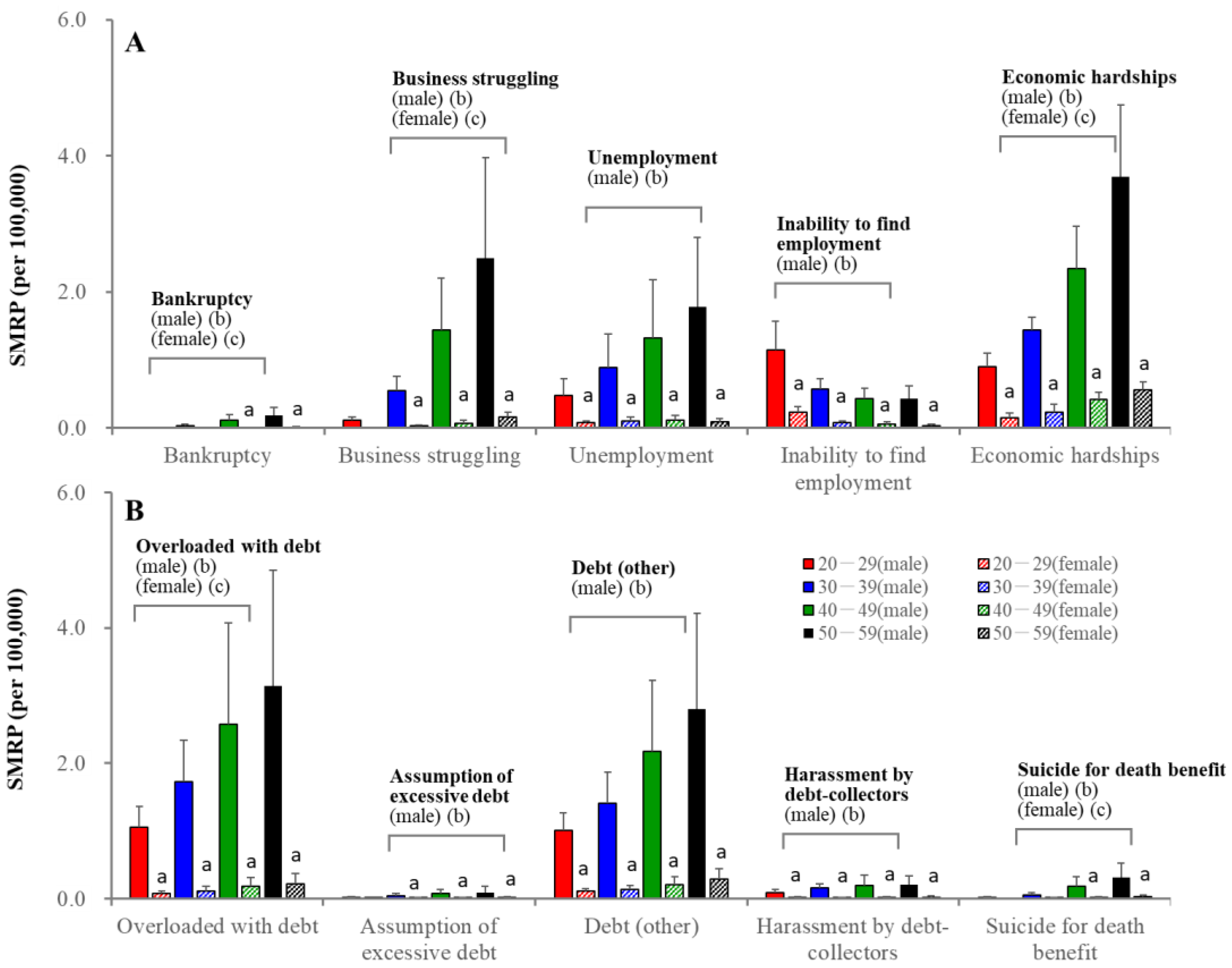
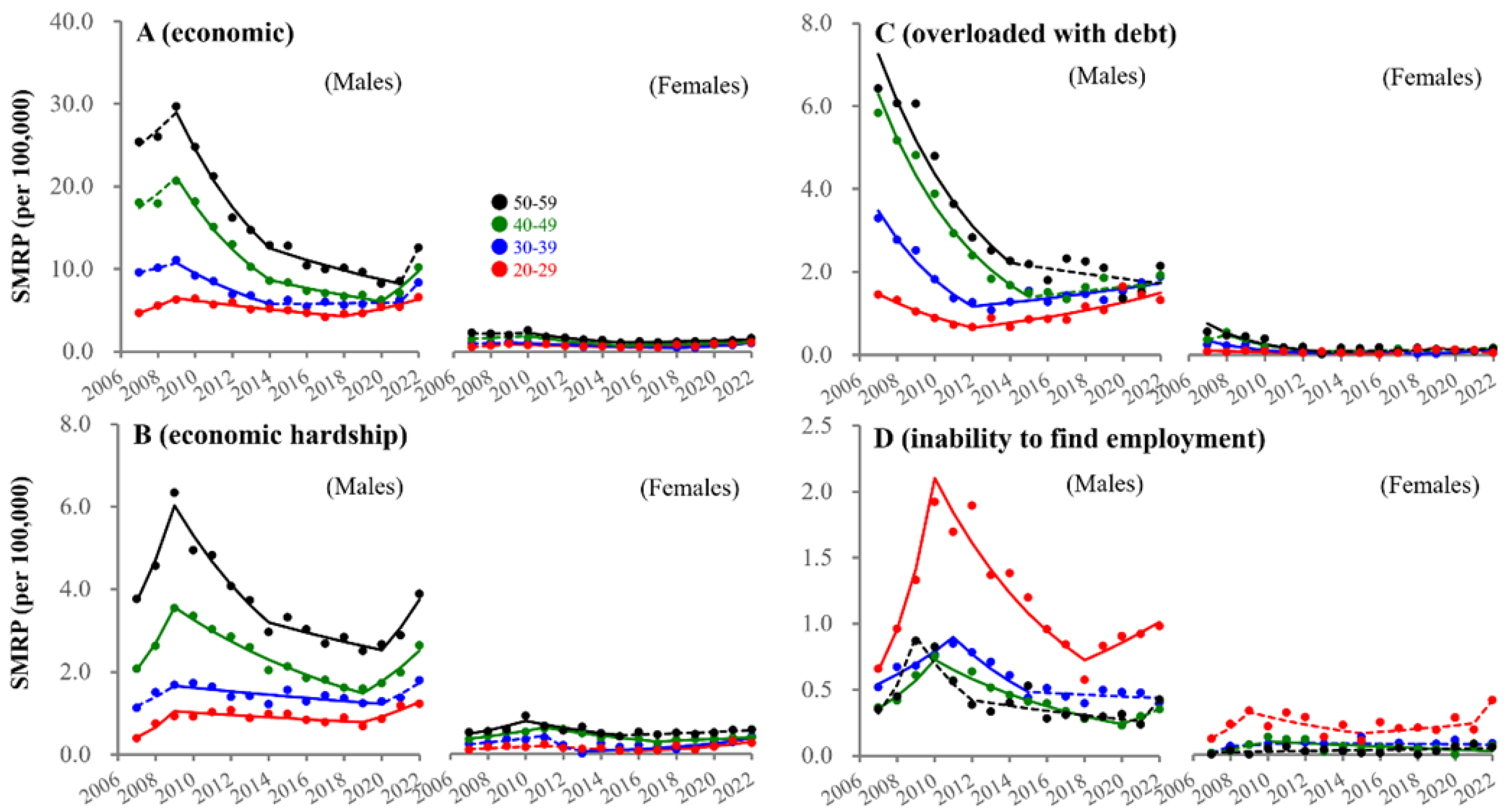
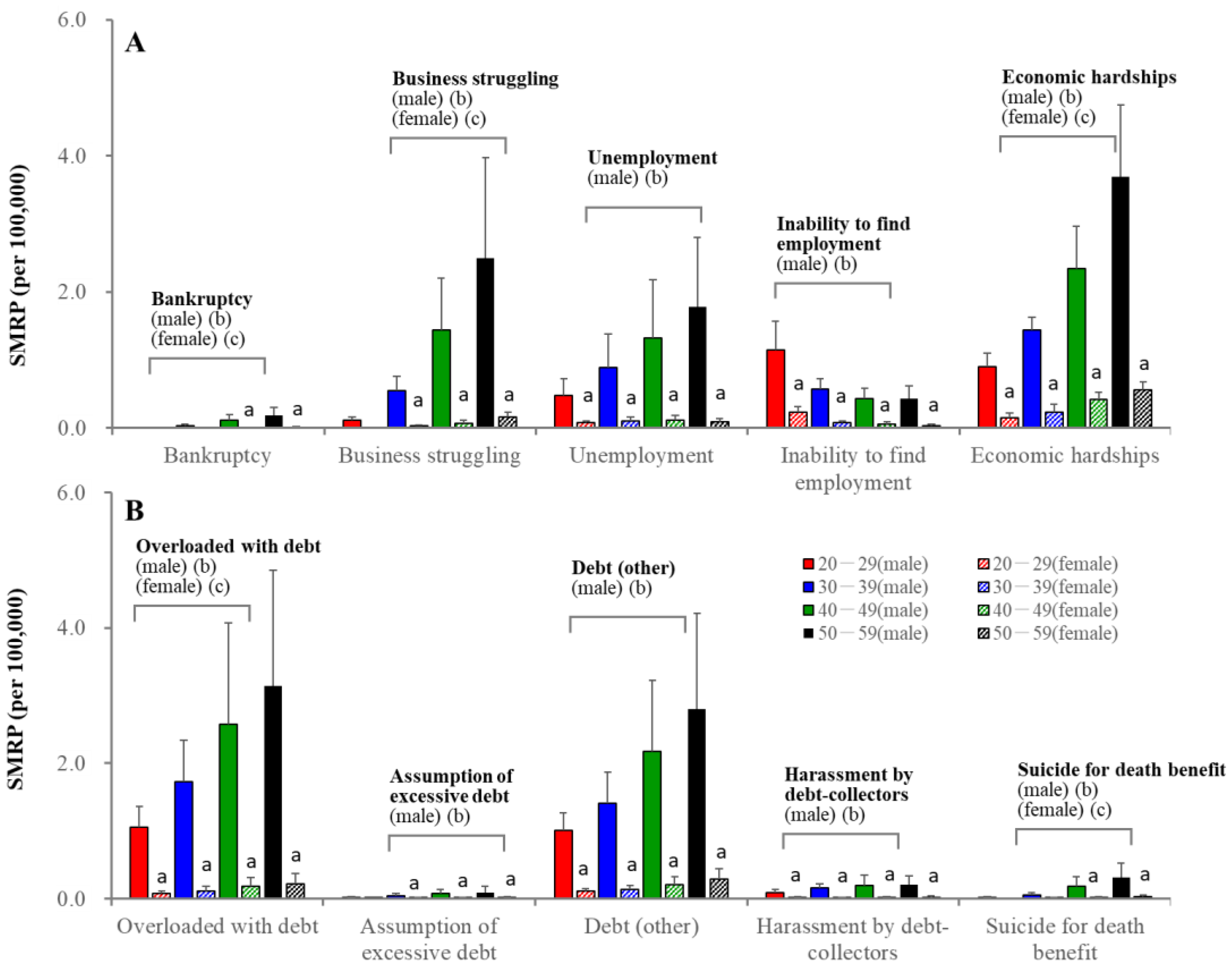
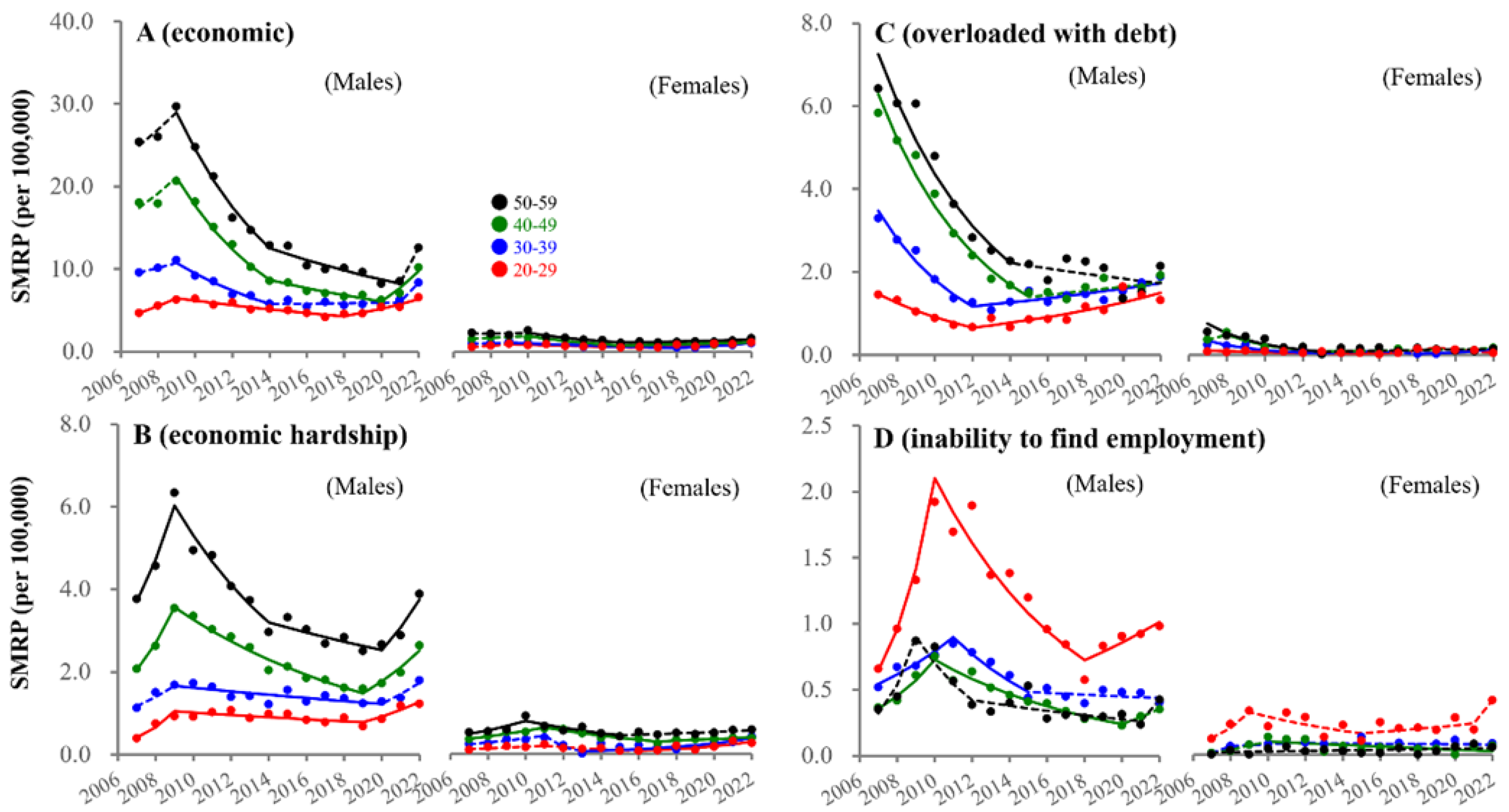
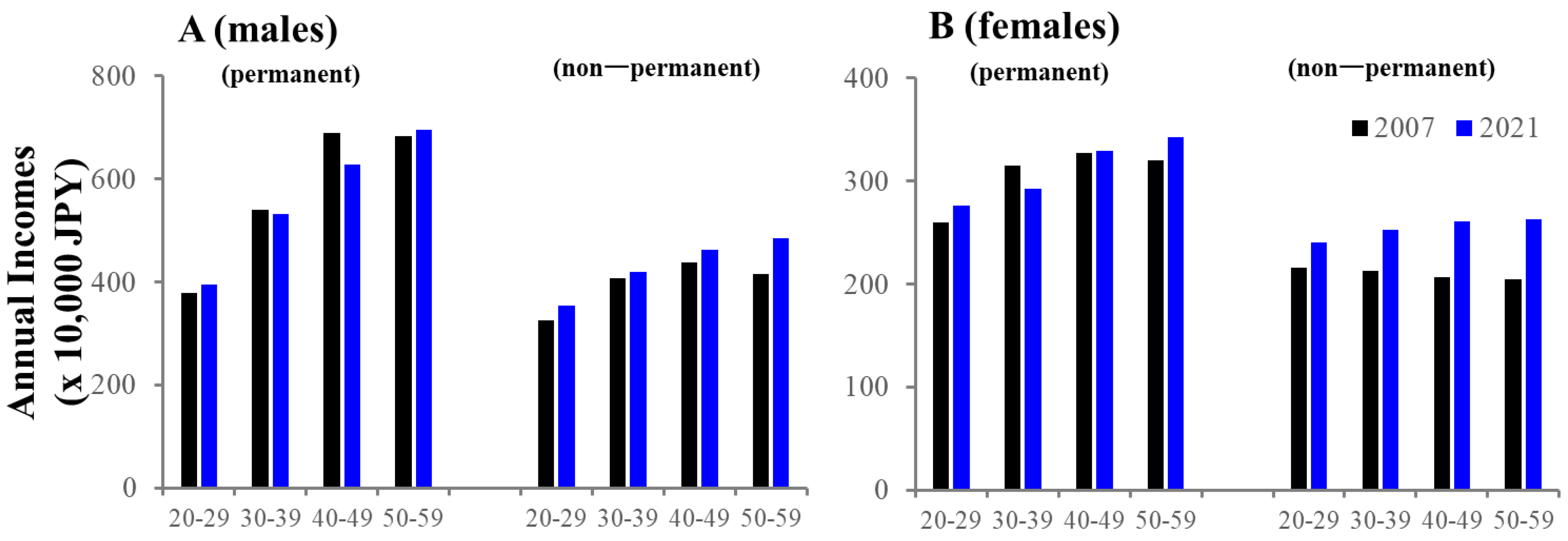
3.5. Fluctuations in SMRPs Caused by Economy-Related Motive
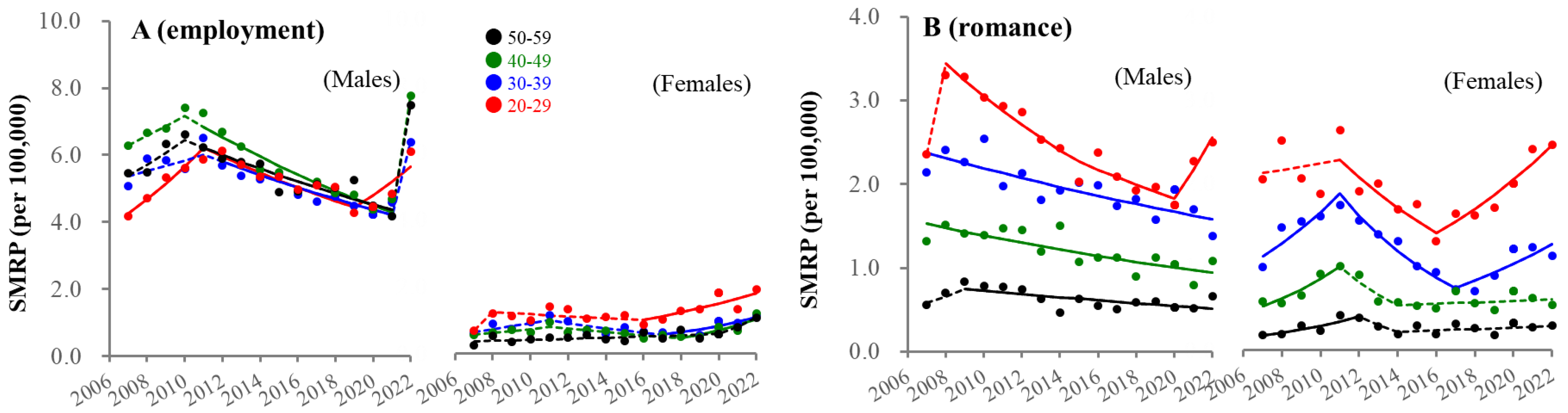
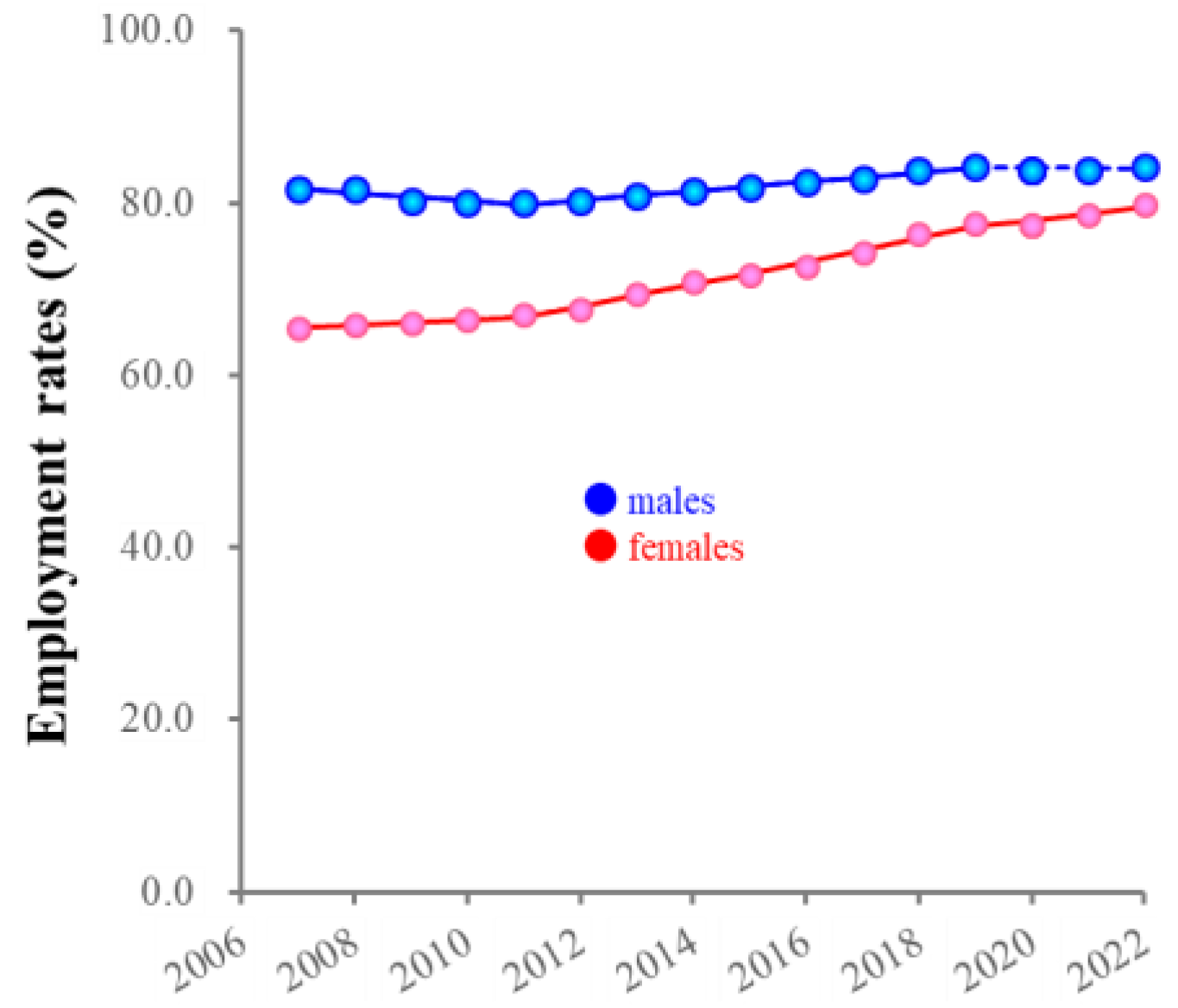
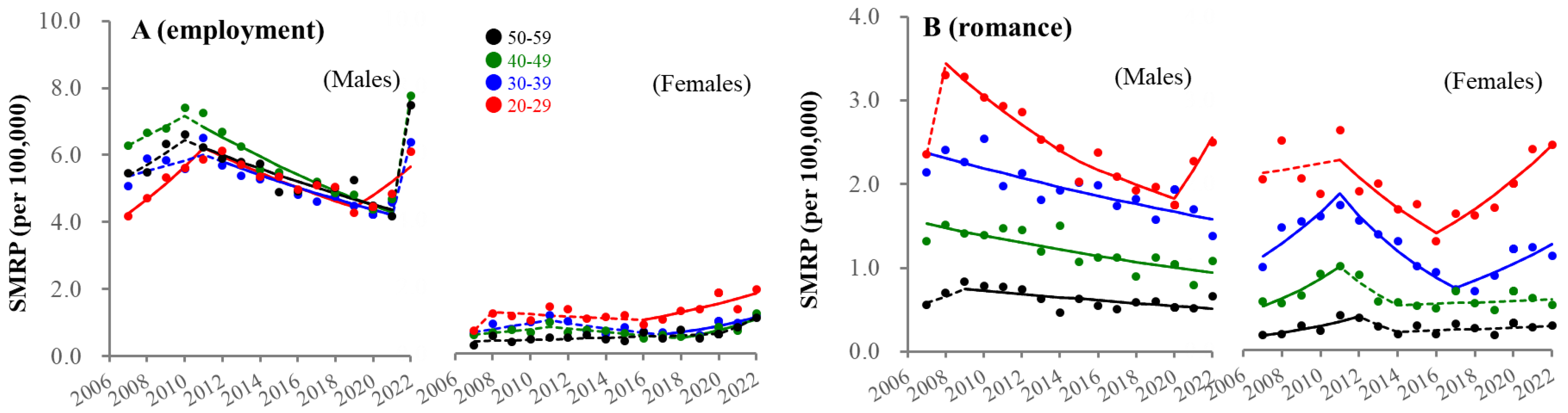
3.6. Fluctuations in SMRPs Caused by Employment-Related and Romance-Related Motives
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- MHLW. 2022 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2022.html (accessed on 1 April 2023).
- Wada, K.; Gilmour, S. Inequality in mortality by occupation related to economic crisis from 1980 to 2010 among working-age Japanese males. Sci. Rep. 2016, 6, 22255. [Google Scholar] [CrossRef]
- Wada, K.; Kondo, N.; Gilmour, S.; Ichida, Y.; Fujino, Y.; Satoh, T.; Shibuya, K. Trends in cause specific mortality across occupations in Japanese men of working age during period of economic stagnation, 1980–2005: Retrospective cohort study. BMJ 2012, 344, e1191. [Google Scholar] [CrossRef]
- Dhungel, B.; Sugai, M.K.; Gilmour, S. Trends in Suicide Mortality by Method from 1979 to 2016 in Japan. Int. J. Environ. Res. Public Health 2019, 16, 1794. [Google Scholar] [CrossRef]
- Yoshioka, E.; Hanley, S.J.; Kawanishi, Y.; Saijo, Y. Time trends in method-specific suicide rates in Japan, 1990–2011. Epidemiol. Psychiatr. Sci. 2016, 25, 58–68. [Google Scholar] [CrossRef]
- Kato, R.; Okada, M. Can Financial Support Reduce Suicide Mortality Rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. [Google Scholar] [CrossRef]
- MHLW. Basic Data on Suicide in the Region. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html (accessed on 31 January 2023).
- Kino, S.; Jang, S.N.; Gero, K.; Kato, S.; Kawachi, I. Age, period, cohort trends of suicide in Japan and Korea (1986–2015): A tale of two countries. Soc. Sci. Med. 2019, 235, 112385. [Google Scholar] [CrossRef]
- Hasegawa, T.; Matsumoto, R.; Yamamoto, Y.; Okada, M. Analysing effects of financial support for regional suicide prevention programmes on methods of suicide completion in Japan between 2009 and 2018 using governmental statistical data. BMJ Open 2021, 11, e049538. [Google Scholar] [CrossRef]
- Okada, M.; Hasegawa, T.; Kato, R.; Shiroyama, T. Analysing regional unemployment rates, GDP per capita and financial support for regional suicide prevention programme on suicide mortality in Japan using governmental statistical data. BMJ Open 2020, 10, e037537. [Google Scholar] [CrossRef]
- Nakano, T.; Hasegawa, T.; Okada, M. Analysing the Impacts of Financial Support for Regional Suicide Prevention Programmes on Suicide Mortality Caused by Major Suicide Motives in Japan Using Statistical Government Data. Int. J. Environ. Res. Public Health 2021, 18, 3414. [Google Scholar] [CrossRef]
- MHLW. 2007 White Paper on Suicide Prevention. Available online: https://warp.da.ndl.go.jp/info:ndljp/pid/9929094/www8.cao.go.jp/jisatsutaisaku//whitepaper/w-2007/html/part1/b1_1_01.html (accessed on 1 April 2023).
- MHLW. 2013 White Paper on Suicide Prevention. Available online: https://warp.da.ndl.go.jp/info:ndljp/pid/9929094/www8.cao.go.jp/jisatsutaisaku//whitepaper/en/w-2013/summary.html (accessed on 1 April 2023).
- MHLW. 2018 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2018.html (accessed on 1 April 2023).
- Shiroyama, T.; Fukuyama, K.; Okada, M. Effects of Financial Expenditure of Prefectures/Municipalities on Regional Suicide Mortality in Japan. Int. J. Environ. Res. Public Health 2021, 18, 8639. [Google Scholar] [CrossRef]
- Kikuchi, K.; Anzai, T.; Takahashi, K. The Unusual Increase in Suicides Among Women in Japan During the COVID-19 Pandemic: A Time-series Analysis Until October 2021. J. Epidemiol. 2023, 33, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, E.; Hanley, S.J.B.; Sato, Y.; Saijo, Y. Impact of the COVID-19 pandemic on suicide rates in Japan through December 2021: An interrupted time series analysis. Lancet Reg. Health West. Pac. 2022, 24, 100480. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, R.; Motomura, E.; Fukuyama, K.; Shiroyama, T.; Okada, M. Determining What Changed Japanese Suicide Mortality in 2020 Using Governmental Database. J. Clin. Med. 2021, 10, 5199. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, R.; Kawano, Y.; Motomura, E.; Shiroyama, T.; Okada, M. Analyzing the Changing Relationship Between Personal Consumption and Suicide Mortality During COVID-19 Pandemic in Japan, using governmental and personal consumption transaction databases. Front. Public Health 2022, 10, 982341. [Google Scholar] [CrossRef] [PubMed]
- Okada, M. Is an increase in Japan’s suicides caused by COVID-19 alone? Asian J. Psychiatry 2022, 78, 103320. [Google Scholar] [CrossRef]
- Okada, M.; Matsumoto, R.; Motomura, E.; Shiroyama, T.; Murata, M. Exploring characteristics of increased suicide during the COVID-19 pandemic in Japan using provisional governmental data. Lancet Reg. Health West. Pac. 2022, 24, 100481. [Google Scholar] [CrossRef]
- Matsumoto, R.; Motomura, E.; Okada, M. Fluctuation of suicide mortality and temporal causality from unemployment duration to suicide mortality in Japan during 2009–2022. Asian J. Psychiatry 2023, 84, 103574. [Google Scholar] [CrossRef]
- Okada, M.; Matsumoto, R.; Shiroyama, T.; Motomura, E. Suicidal Mortality and Motives Among Middle-School, High-School and University Students. JAMA Netw. Open 2023, 6, e2328144. [Google Scholar] [CrossRef]
- Tanaka, T.; Okamoto, S. Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nat. Hum. Behav. 2021, 5, 229–238. [Google Scholar] [CrossRef]
- Anzai, T.; Fukui, K.; Ito, T.; Ito, Y.; Takahashi, K. Excess Mortality From Suicide During the Early COVID-19 Pandemic Period in Japan: A Time-Series Modeling Before the Pandemic. J. Epidemiol. 2021, 31, 152–156. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ghaznavi, C.; Ueda, P. Assessment of Suicide in Japan During the COVID-19 Pandemic vs. Previous Years. JAMA Netw. Open 2021, 4, e2037378. [Google Scholar] [CrossRef] [PubMed]
- Ueda, M.; Nordstrom, R.; Matsubayashi, T. Suicide and mental health during the COVID-19 pandemic in Japan. J. Public Health 2022, 44, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Tanaka, H. Increased suicide mortality in Japan during the COVID-19 pandemic in 2020. Psychiatry Res. 2022, 309, 114422. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, M.; Yamasaki, S.; Endo, K.; Ando, S.; Sakai, M.; Yoshii, H.; Nishida, A. Suicide rates during the COVID-19 pandemic in Japan from April 2020 to December 2021. Psychiatry Res. 2022, 316, 114774. [Google Scholar] [CrossRef]
- NPA. Suicide Statistics (SSNPA). Available online: https://www.npa.go.jp/publications/statistics/safetylife/jisatsu.html (accessed on 30 March 2023).
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child. Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.; Benros, M.E.; Klein, R.S.; Vinkers, C.H. How COVID-19 shaped mental health: From infection to pandemic effects. Nat. Med. 2022, 28, 2027–2037. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nat. Rev. Dis. Primers 2019, 5, 74. [Google Scholar] [CrossRef]
- Foulkes, L.; Blakemore, S.J. Individual differences in adolescent mental health during COVID-19: The importance of peer relationship quality. Neuron 2021, 109, 3203–3205. [Google Scholar] [CrossRef]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J.; Collaboration, C.-S.P.R. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef]
- Kawohl, W.; Nordt, C. COVID-19, unemployment, and suicide. Lancet Psychiatry 2020, 7, 389–390. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Wu, K.C.; Yousuf, S.; Yip, P.S. Suicide in Asia: Opportunities and challenges. Epidemiol. Rev. 2012, 34, 129–144. [Google Scholar] [CrossRef] [PubMed]
- Goto, R.; Okubo, Y.; Skokauskas, N. Reasons and trends in youth’s suicide rates during the COVID-19 pandemic. Lancet Reg. Health West. Pac. 2022, 27, 100567. [Google Scholar] [CrossRef] [PubMed]
- Koda, M.; Harada, N.; Eguchi, A.; Nomura, S.; Ishida, Y. Reasons for Suicide During the COVID-19 Pandemic in Japan. JAMA Netw. Open 2022, 5, e2145870. [Google Scholar] [CrossRef] [PubMed]
- Cha, C.B.; Franz, P.J.; Guzmán, E.M.; Glenn, C.R.; Kleiman, E.M.; Nock, M.K. Annual Research Review: Suicide among youth-epidemiology, (potential) etiology, and treatment. J. Child Psychol. Psychiatry 2018, 59, 460–482. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.L.; Horowitz, L.M.; Ackerman, J.P.; Adrian, M.C.; Campo, J.V.; Bridge, J.A. Suicide in young people: Screening, risk assessment, and intervention. BMJ 2023, 381, e070630. [Google Scholar] [CrossRef]
- Yu, B.; Chen, X. Age and Birth Cohort-Adjusted Rates of Suicide Mortality Among US Male and Female Youths Aged 10 to 19 Years From 1999 to 2017. JAMA Netw. Open 2019, 2, e1911383. [Google Scholar] [CrossRef]
- Shiratori, Y.; Tachikawa, H.; Nemoto, K.; Endo, G.; Aiba, M.; Matsui, Y.; Asada, T. Network analysis for motives in suicide cases: A cross-sectional study. Psychiatry Clin. Neurosci. 2014, 68, 299–307. [Google Scholar] [CrossRef]
- MHLW. 2021 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2021.html (accessed on 1 April 2023).
- SBMIAC. Surveys of Population, Population Change and the Number of Households Based on the Basic Resident Registration. Available online: https://www.e-stat.go.jp/en/statistics/00200241 (accessed on 1 June 2023).
- MHLW. Basic Survey on Wage Structure. Available online: https://www.e-stat.go.jp/en/statistics/00450091 (accessed on 1 August 2023).
- Cabinet Office. The White Paper on Gender Equality 2023. Available online: https://www.gender.go.jp/about_danjo/whitepaper/r05/gaiyou/pdf/r05_gaiyou_en.pdf (accessed on 1 August 2023).
- Cabinet Office. The White Paper on Gender Equality 2021. Available online: https://www.gender.go.jp/about_danjo/whitepaper/r03/zentai/index.html (accessed on 1 August 2023).
- Cabinet Office. The White Paper on Gender Equality 2022. Available online: https://www.gender.go.jp/about_danjo/whitepaper/r04/gaiyou/pdf/r04_gaiyou_en.pdf (accessed on 1 August 2023).
- MHLW. Labour Force Survey. Available online: https://www.e-stat.go.jp/en/statistics/00200531 (accessed on 1 February 2022).
- NCI. Joinpoint Regression Program ver5.0.2. Available online: https://surveillance.cancer.gov/joinpoint/ (accessed on 26 June 2023).
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Katsumata, Y.; Hachisuka, H.; Sago, N.; Shimizu, Y.; Oikawa, K.; Horii, S.; Kimata, S. Use of Telephone Crisis Hotline by Callers with Suicidality in Japan during the COVID-19 Pandemic. Arch. Suicide Res. 2023, 10, 1–6. [Google Scholar] [CrossRef]
- Chang, Y.H.; Lin, C.Y.; Liao, S.C.; Chen, Y.Y.; Shaw, F.F.; Hsu, C.Y.; Gunnell, D.; Chang, S.S. Societal factors and psychological distress indicators associated with the recent rise in youth suicide in Taiwan: A time trend analysis. Aust. N. Z. J. Psychiatry 2023, 57, 537–549. [Google Scholar] [CrossRef]
- Forum, W.E. Global Gender Gap Report 2023. Available online: https://www.weforum.org/reports/global-gender-gap-report-2023/ (accessed on 1 August 2023).
- Bianchi, S.M.; Sayer, L.C.; Milkie, M.A.; Robinson, J.P. Housework: Who Did, Does or Will Do It, and How Much Does It Matter? Soc. Forces 2012, 91, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Kawase, K.; Kwong, A.; Yorozuya, K.; Tomizawa, Y.; Numann, P.J.; Sanfey, H. The attitude and perceptions of work-life balance: A comparison among women surgeons in Japan, USA, and Hong Kong China. World J. Surg. 2013, 37, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Johnston, E.; Johnson, A. Balancing life and work by unbending gender: Early American women psychologists’ struggles and contributions. J. Hist. Behav. Sci. 2017, 53, 246–264. [Google Scholar] [CrossRef] [PubMed]
- Xue, B.; Fleischmann, M.; Head, J.; McMunn, A.; Stafford, M. Work-Family Conflict and Work Exit in Later Career Stage. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 716–727. [Google Scholar] [CrossRef] [PubMed]
- Templeton, K.; Nilsen, K.M.; Walling, A. Issues Faced by Senior Women Physicians: A National Survey. J. Women’s Health 2020, 29, 980–988. [Google Scholar] [CrossRef]
- Nakamoto, M.; Nakagawa, T.; Murata, M.; Okada, M. Impacts of Dual-Income Household Rate on Suicide Mortalities in Japan. Int. J. Environ. Res. Public Health 2021, 18, 5670. [Google Scholar] [CrossRef]
- Minami, U.; Suzuki, H.; Kuraoka, M.; Koike, T.; Kobayashi, E.; Fujiwara, Y. Older Adults Looking for a Job through Employment Support System in Tokyo. PLoS ONE 2016, 11, e0159713. [Google Scholar] [CrossRef]
- Frank, E.; Zhao, Z.; Fang, Y.; Rotenstein, L.S.; Sen, S.; Guille, C. Experiences of Work-Family Conflict and Mental Health Symptoms by Gender among Physician Parents during the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2134315. [Google Scholar] [CrossRef]
- Kushner, H.I.; Sterk, C.E. The limits of social capital: Durkheim, suicide, and social cohesion. Am. J. Public Health 2005, 95, 1139–1143. [Google Scholar] [CrossRef]
- Raley, S.; Bianchi, S.M.; Wang, W. When Do Fathers Care? Mothers’ Economic Contribution and Fathers’ Involvement in Child Care. Am. J. Soc. 2012, 117, 1422–1459. [Google Scholar] [CrossRef]
- MHLW. Patient Survey. Available online: https://www.e-stat.go.jp/en/statistics/00450022 (accessed on 31 January 2023).
- Benarous, X.; Consoli, A.; Cohen, D.; Renaud, J.; Lahaye, H.; Guile, J.M. Suicidal behaviors and irritability in children and adolescents: A systematic review of the nature and mechanisms of the association. Eur. Child Adolesc. Psychiatry 2019, 28, 667–683. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Green, J.G.; Hwang, I.; McLaughlin, K.A.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: Results from the National Comorbidity Survey Replication Adolescent Supplement. JAMA Psychiatry 2013, 70, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Thibodeau, M.A.; Welch, P.G.; Sareen, J.; Asmundson, G.J. Anxiety disorders are independently associated with suicide ideation and attempts: Propensity score matching in two epidemiological samples. Depress. Anxiety 2013, 30, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Wade, T.J.; Cairney, J.; Pevalin, D.J. Emergence of gender differences in depression during adolescence: National panel results from three countries. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Sands, A.; van Dijk, M.T.; Abraham, E.; Yangchen, T.; Talati, A.; Weissman, M.M. The Long-Term Outcomes of Prepubertal Depression and Internalizing Problems: A Scoping Review. Harv. Rev. Psychiatry 2022, 30, 163–180. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Platt, J.M. Annual Research Review: Sex, gender, and internalizing conditions among adolescents in the 21st century—Trends, causes, consequences. J. Child Psychol. Psychiatry 2023. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Rao, D. On the self-stigma of mental illness: Stages, disclosure, and strategies for change. Can. J. Psychiatry 2012, 57, 464–469. [Google Scholar] [CrossRef]
- Grafova, I.B.; Clifford, P.R.; Hudson, S.V.; Steinberg, M.B.; O’Malley, D.M.; Elliott, J.; Llanos, A.A.M.; Saraiya, B.; Duberstein, P.R. Disease and debt: Findings from the 2019 Panel Study of Income Dynamics in the United States. Prev. Med. 2022, 164, 107248. [Google Scholar] [CrossRef]
- Lin, Y.; Callahan, C.P.; Moser, J.S. A mind full of self: Self-referential processing as a mechanism underlying the therapeutic effects of mindfulness training on internalizing disorders. Neurosci. Biobehav. Rev. 2018, 92, 172–186. [Google Scholar] [CrossRef]
- Donolato, E.; Cardillo, R.; Mammarella, I.C.; Melby-Lervag, M. Research Review: Language and specific learning disorders in children and their co-occurrence with internalizing and externalizing problems: A systematic review and meta-analysis. J. Child Psychol. Psychiatry 2022, 63, 507–518. [Google Scholar] [CrossRef]
- Sweet, E. “Like you failed at life”: Debt, health and neoliberal subjectivity. Soc. Sci. Med. 2018, 212, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Fancourt, D.; Steptoe, A.; Bu, F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: A longitudinal observational study. Lancet Psychiatry 2021, 8, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Anindyajati, G.; Wiguna, T.; Murtani, B.J.; Christian, H.; Wigantara, N.A.; Putra, A.A.; Hanafi, E.; Minayati, K.; Ismail, R.I.; Kaligis, F.; et al. Anxiety and Its Associated Factors During the Initial Phase of the COVID-19 Pandemic in Indonesia. Front. Psychiatry 2021, 12, 634585. [Google Scholar] [CrossRef] [PubMed]
- Min, S.; Jeong, Y.H.; Kim, J.; Koo, J.W.; Ahn, Y.M. The Aftermath: Post-pandemic Psychiatric Implications of the COVID-19 Pandemic, a South Korean Perspective. Front. Psychiatry 2021, 12, 671722. [Google Scholar] [CrossRef]
- Khera, G.; Chandrika Yelisetty, R.; Spence, G.M.; AlAhbabi, W.; Dadzie, V.B. Impact of the COVID-19 pandemic on the well-being of preschoolers: A parental guide. Heliyon 2023, 9, e14332. [Google Scholar] [CrossRef]
- Zhu, X.; Xu, J. After the pandemic is before the pandemic: Rethinking urban priorities, assumptions and planning approaches. Heliyon 2023, 9, e20763. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, R.; Motomura, E.; Onitsuka, T.; Okada, M. Trends in Suicidal Mortality and Motives among Working-Ages Individuals in Japan during 2007–2022. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 2795-2810. https://doi.org/10.3390/ejihpe13120193
Matsumoto R, Motomura E, Onitsuka T, Okada M. Trends in Suicidal Mortality and Motives among Working-Ages Individuals in Japan during 2007–2022. European Journal of Investigation in Health, Psychology and Education. 2023; 13(12):2795-2810. https://doi.org/10.3390/ejihpe13120193
Chicago/Turabian StyleMatsumoto, Ryusuke, Eishi Motomura, Toshiaki Onitsuka, and Motohiro Okada. 2023. "Trends in Suicidal Mortality and Motives among Working-Ages Individuals in Japan during 2007–2022" European Journal of Investigation in Health, Psychology and Education 13, no. 12: 2795-2810. https://doi.org/10.3390/ejihpe13120193
APA StyleMatsumoto, R., Motomura, E., Onitsuka, T., & Okada, M. (2023). Trends in Suicidal Mortality and Motives among Working-Ages Individuals in Japan during 2007–2022. European Journal of Investigation in Health, Psychology and Education, 13(12), 2795-2810. https://doi.org/10.3390/ejihpe13120193