
Association between Suicide Rate and Human Development Index, Income, and the Political System in 46 Muslim-Majority Countries: An Ecological Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. List of the Muslim Majority Countries
2.2. Suicide Rate, WHO Region, Continent, and Income
2.3. Human Development Index (HDI)
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Suicide Rate in Muslim Countries
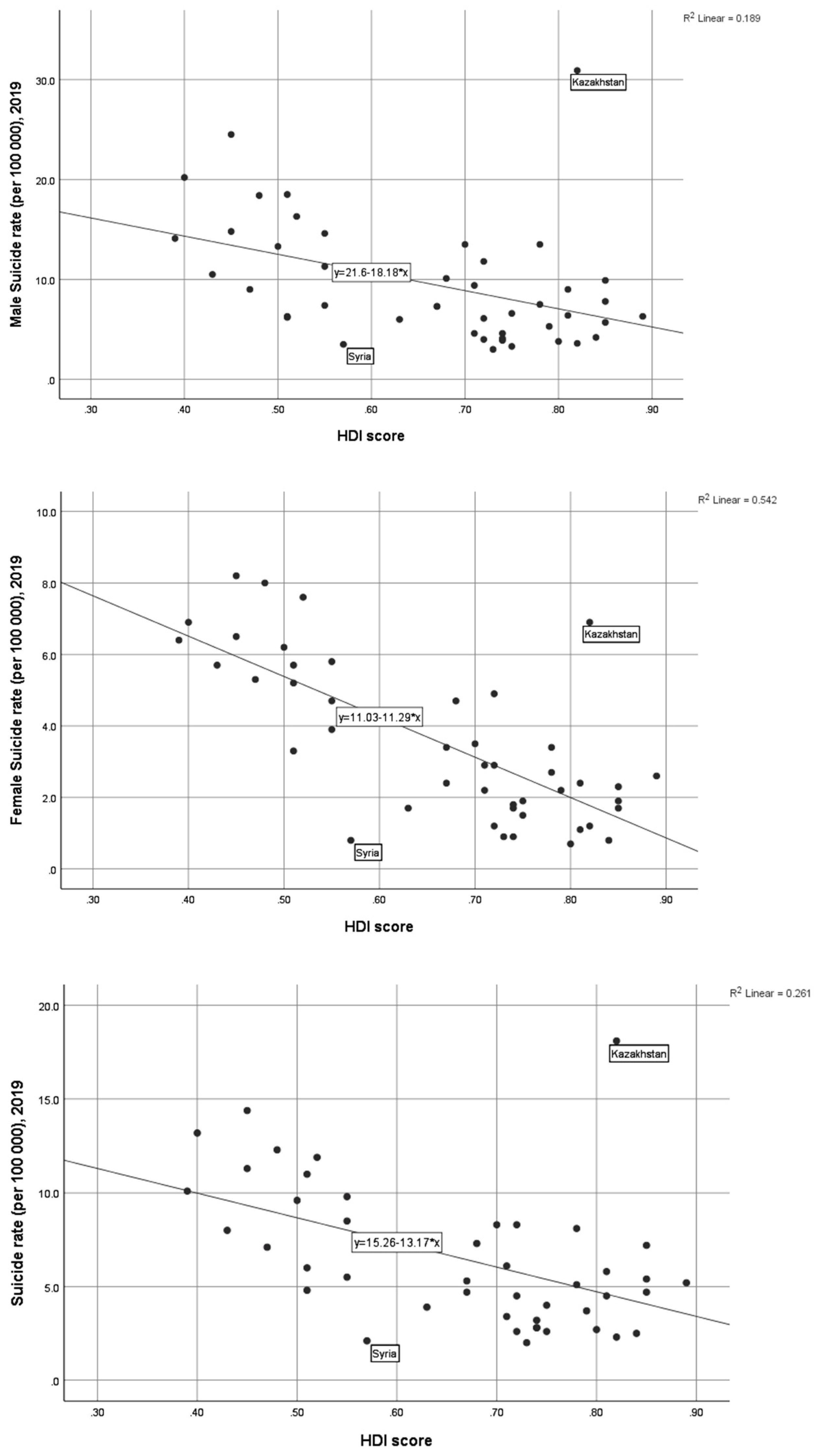
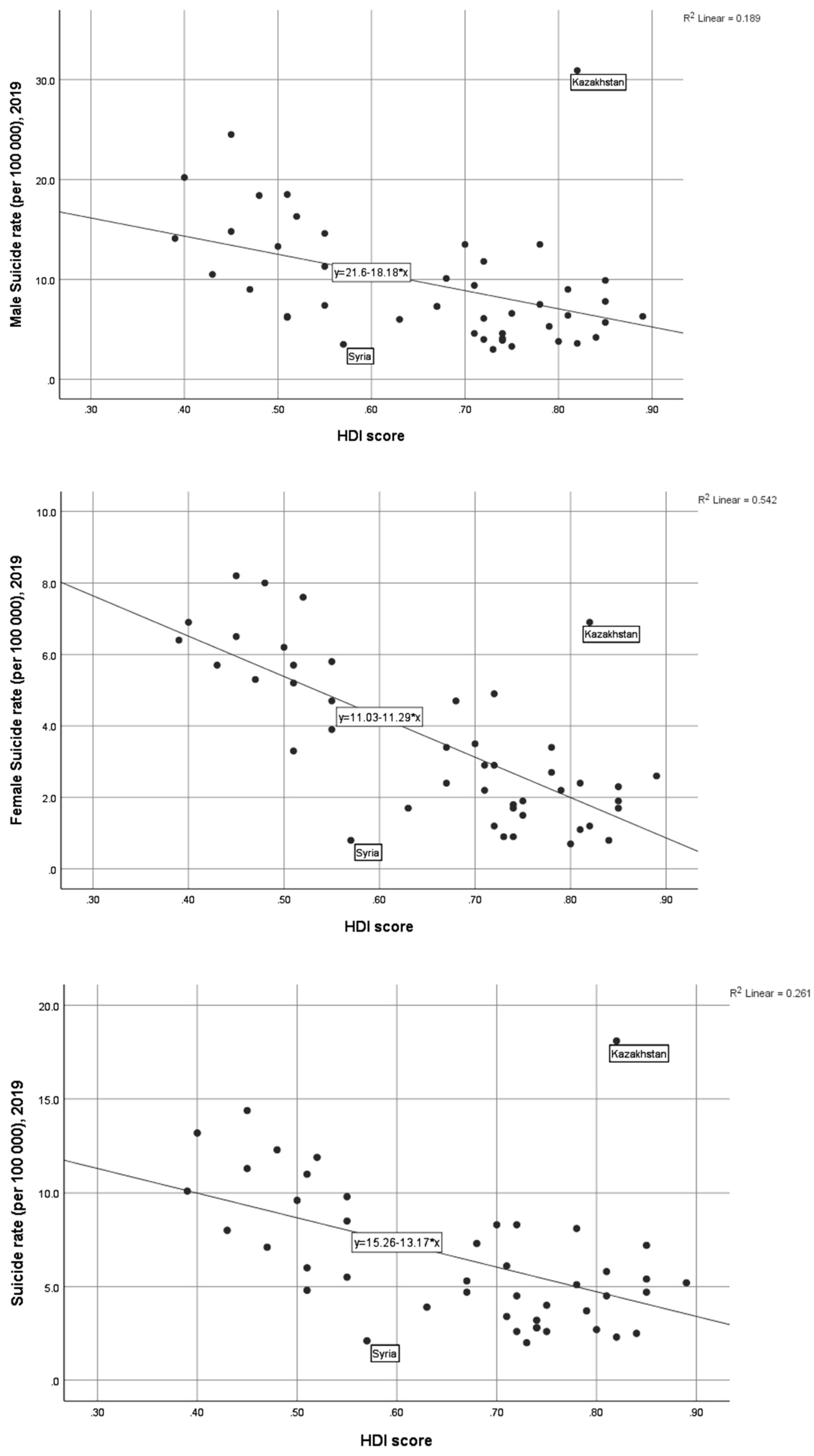
3.2. Association between Suicide Rate and Ecological Variables
4. Discussion
4.1. Major Findings
4.2. Implications
4.3. What Is Already Known
4.4. What This Study Adds
4.5. Strength of the Study
4.6. Limitations of the Study
4.7. Future Lines of Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Suicide Worldwide in 2019: Global Health Estimates; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240026643 (accessed on 15 September 2021).
- World Health Organization. Preventing Suicide: A Global Imperative; WHO: Geneva, Switzerland, 2014; Available online: https://apps.who.int/iris/handle/10665/131056 (accessed on 14 June 2021).
- Zalsman, G.; Hawton, K.; Wasserman, D.; van Heeringen, K.; Arensman, E.; Sarchiapone, M.; Carli, V.; Höschl, C.; Barzilay, R.; Balazs, J.; et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry 2016, 3, 646–659. [Google Scholar] [CrossRef]
- Knipe, D.; Williams, A.J.; Hannam-Swain, S.; Upton, S.; Brown, K.; Bandara, P.; Chang, S.-S.; Kapur, N. Psychiatric morbidity and suicidal behaviour in low- and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2019, 16, e1002905. [Google Scholar] [CrossRef] [PubMed]
- Milner, A.; Sveticic, J.; De Leo, D. Suicide in the absence of mental disorder? A review of psychological autopsy studies across countries. Int. J. Soc. Psychiatry 2013, 59, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, J.T.O.; Carson, A.J.; Sharpe, M.; Lawrie, S.M. Psychological autopsy studies of suicide: A systematic review. Psychol. Med. 2003, 33, 395–405. [Google Scholar] [CrossRef]
- Cho, S.E.; Na, K.S.; Cho, S.J.; Im, J.S.; Kang, S.G. Geographical and temporal variations in the prevalence of mental disorders in suicide: Systematic review and meta-analysis. J. Affect. Disord. 2016, 190, 704–713. [Google Scholar] [CrossRef] [PubMed]
- Arafat, S.Y.; Menon, V.; Varadharajan, N.; Kar, S.K. Psychological Autopsy Studies of Suicide in South East Asia. Indian J. Psychol. Med. 2022, 44, 4–9. [Google Scholar] [CrossRef]
- Arafat, S.M.Y.; Khan, M.M.; Menon, V.; Ali, S.-Z.; Rezaeian, M.; Shoib, S. Psychological autopsy study andrisk factors for suicide in Muslim countries. Health Sci. Rep. 2021, 4, e414. [Google Scholar] [CrossRef]
- World Population Review. Muslim Majority Countries 2021. Available online: https://worldpopulationreview.com/country-rankings/muslim-majority-countries (accessed on 15 June 2021).
- United for Global Mental Health. Decriminalising Suicide: Saving Lives, Reducing Stigma. 2021. Available online: https://unitedgmh.org/sites/default/files/2021-09/UNITEDGMH%20Suicide%20Report%202021%C6%92.pdf (accessed on 15 September 2021).
- Mishara, B.L.; Weisstub, D.N. The legal status of suicide: A global review. Int. J. Law Psychiatry 2016, 44, 54–74. [Google Scholar] [CrossRef]
- Lew, B.; Lester, D.; Kõlves, K.; Yip, P.S.F.; Chen, Y.-Y.; Chen, W.S.; Hasan, M.T.; Koenig, H.G.; Wang, Z.Z.; Fariduddin, M.N.; et al. An analysis of age-standardized suicide rates in Muslim-majority countries in 2000–2019. BMC Public Health 2022, 22, 882. [Google Scholar] [CrossRef]
- Shah, A.; Chandia, M. The relationship between suicide and Islam: A cross-national study. J. Inj. Violence Res. 2010, 2, 93–97. [Google Scholar] [CrossRef]
- Hajiyousouf, I.I.; Bulut, S. Mental Health, Religion and Suicide. Open J. Med Psychol. 2022, 11, 12–27. [Google Scholar] [CrossRef]
- World Population Review. List Of Countries by Continent 2021. Available online: https://worldpopulationreview.com/country-rankings/list-of-countries-by-continent (accessed on 1 November 2021).
- McLaren, L.; Hawe, P. Ecological perspectives in health research. J. Epidemiol. Community Health 2005, 59, 6–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519 (accessed on 21 January 2022).
- United Nations Development Programme. Global Human Development Indicators. Available online: http://hdr.undp.org/en/countries (accessed on 1 November 2021).
- Human Development Index. Human Development Reports (undp.org). Available online: https://hdr.undp.org/data-center/human-development-index#/indicies/HDI (accessed on 29 June 2022).
- Pritchard, C.; Amanullah, S. An analysis of suicide and undetermined deathsin 17 predominantly Islamic countries contrasted with the UK. Psychol. Med. 2007, 37, 421430. [Google Scholar] [CrossRef] [PubMed]
- Tondo, L.; Albert, M.J.; Baldessarini, R.J. Suicide rates in relation to health careaccess in the United States: An ecological study. J. Clin. Psychiatry 2006, 67, 517–523. [Google Scholar] [CrossRef]
- Fukuda, Y.; Nakamura, K.; Takano, T. Cause-specific mortality differences across socio economic position of municipalities in Japan, 1973–1977 and 1993–1998: Increased importance of injury and suicide in inequality for ages under 75. Int. J. Epidemiol. 2005, 34, 100–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, R.; Page, A.; Morrell, S.; Harrison, J.; Carter, G. Mental health and socio-economic variations in Australian suicide. Soc. Sci. Med. 2005, 61, 1551–1559. [Google Scholar] [CrossRef]
- Rezaeian, M.; Dunn, G.; St Leger, S.; Appleby, L. Ecological association between suicide rates and indices of deprivation in the north west region of England: The importance of the size of the administrative unit. J. Epidemiol. Community Health 2006, 60, 956–961. [Google Scholar]
- Pompili, M.; Innamorati, M.; Vichi, M.; Masocco, M.; Vanacore, N.; Lester, D.; Serafini, G.; Tatarelli, R.; De Leo, D.; Girardi, P. Inequalities and Impact of Socioeconomic-Cultural Factors in Suicide Rates Across Italy. Crisis 2011, 32, 178–185. [Google Scholar] [CrossRef]
- Khazaei, S.; Armanmehr, V.; Nematollahi, S.; Rezaeian, S.; Khazaei, S. Suicide rate in relation to the Human Development Index and other health related factors: A global ecological study from 91 countries. J. Epidemiol. Glob. Health 2017, 7, 131–134. [Google Scholar] [CrossRef]
- Knipe, D.W.; Carroll, R.; Thomas, K.H.; Pease, A.; Gunnell, D.; Metcalfe, C. Association of socio-economic position and suicide/attempted suicide in low and middle income countries in South and South-East Asia—A systematic review. BMC Public Health 2015, 15, 1055. [Google Scholar]
- Yip, P.S.F.; Zheng, Y. The Impact of Suicide on Life Expectancy. Crisis 2021, 42, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Sagna, A.; Kemp, M.; DiNitto, D.; Choi, N. Impact of suicide mortality on life expectancy in the United States, 2011 and 2015: Age and sex decomposition. Public Health 2020, 179, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Näher, A.-F.; Rummel-Kluge, C.; Hegerl, U. Associations of Suicide Rates with Socioeconomic Status and Social Isolation: Findings From Longitudinal Register and Census Data. Front. Psychiatry 2020, 10, 898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pompili, M.; Vichi, M.; Qin, P.; Innamorati, M.; De Leo, D.; Girardi, P. Does the level of education influence completed suicide? A nationwide register study. J. Affect. Disord. 2013, 147, 437–440. [Google Scholar] [CrossRef]
- Øien-Ødegaard, C.; Hauge, L.J.; Reneflot, A. Marital status, educational attainment, and suicide risk: A Norwegian register-based population study. Popul. Health Metrics 2021, 19, 33. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ecological systems theory. In Six Theories of Child Development: Revised Formulations and Current Issues; Vasta, R., Ed.; Jessica Kingsley Publishers: London, UK, 1992; pp. 187–249. [Google Scholar]

{kind=link}
| SN | Country | Muslim Population (2021) (Million) | Total Population (2021) (Million) | Muslim % | Suicide Rate (per 100,000), 2019 | Male Suicide Rate (per 100,000), 2019 | Female Suicide Rate (per 100,000), 2019 | Number of Suicides | Continent | WHO Region | Income Group | HDI Score | Political System |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Afghanistan | 34.84 | 39.84 | 99.6 | 6 | 6.2 | 5.7 | 1573 | Asia | EMR | LI | 0.51 | Sharia |
| 2 | Albania | 1.8 | 2.87 | 58.8 | 3.7 | 5.3 | 2.2 | 125 | Europe | EUR | UMI | 0.79 | Democracy |
| 3 | Algeria | 41.24 | 44.62 | 99 | 2.6 | 3.3 | 1.9 | 1072 | Africa | AFR | LMI | 0.75 | Democracy |
| 4 | Azerbaijan | 9.74 | 10.22 | 96.9 | 4 | 6.6 | 1.5 | 411 | Asia | EUR | UMI | 0.75 | Democracy |
| 5 | Bahrain | 1.06 | 1.75 | 73.7 | 7.2 | 9.9 | 2.3 | 145 | Asia | EMR | HI | 0.85 | Monarchy |
| 6 | Bangladesh | 153.7 | 166.3 | 90.4 | 3.9 | 6 | 1.7 | 5998 | Asia | SEAR | LMI | 0.63 | Democracy |
| 7 | Bosnia and Herzegovina | 1.96 | 3.26 | 50.7 | 8.2 | 13.5 | 3.4 | 361 | Europe | EUR | UMI | 0.78 | Democracy |
| 8 | Brunei | 0.36 | 0.44 | 78.8 | 2.5 | 4.2 | 0.8 | 12 | Asia | WPR | HI | 0.84 | Monarchy |
| 9 | Burkina Faso | 12.14 | 21.5 | 61.5 | 14.4 | 24.5 | 6.5 | 1521 | Africa | AFR | LI | 0.45 | Democracy |
| 10 | Chad | 9.18 | 16.91 | 58 | 13.2 | 20.2 | 6.9 | 1027 | Africa | AFR | LI | 0.4 | Democracy |
| 11 | Comoros | 0.81 | 0.89 | 98.3 | 8.5 | 11.3 | 5.8 | 46 | Africa | AFR | LMI | 0.55 | Democracy |
| 12 | Djibouti | 0.86 | 1 | 97 | 11.9 | 16.3 | 7.6 | 94 | Africa | EMR | LMI | 0.52 | Democracy |
| 13 | Egypt | 87.50 | 104.26 | 92.35 | 3.4 | 4.6 | 2.2 | 3022 | Africa | EMR | LMI | 0.71 | Military |
| 14 | Gambia | 2 | 2.49 | 95.7 | 9.6 | 13.3 | 6.2 | 113 | Africa | AFR | LI | 0.5 | Democracy |
| 15 | Guinea | 10.56 | 13.5 | 89.1 | 12.3 | 18.4 | 8 | 892 | Africa | AFR | LI | 0.48 | Democracy |
| 16 | Indonesia | 229 | 276.36 | 87.2 | 2.6 | 4 | 1.2 | 6544 | Asia | SEAR | UMI | 0.72 | Democracy |
| 17 | Iran | 82.5 | 85.03 | 99.4 | 5.1 | 7.5 | 2.7 | 4334 | Asia | EMR | UMI | 0.78 | Democracy |
| 18 | Iraq | 38.47 | 4.12 | 95.7 | 4.7 | 7.3 | 2.4 | 1418 | Asia | EMR | UMI | 0.67 | Democracy |
| 19 | Jordan | 10.17 | 10.27 | 97.2 | 2 | 3 | 0.9 | 165 | Asia | EMR | UMI | 0.73 | Monarchy |
| 20 | Kazakhstan | 13.16 | 18.99 | 70.2 | 18.1 | 30.9 | 6.9 | 3256 | Asia | EUR | UMI | 0.82 | Democracy |
| 21 | Kuwait | 2.18 | 0.43 | 74.6 | 2.7 | 3.8 | 0.7 | 122 | Asia | EMR | HI | 0.8 | Monarchy |
| 22 | Kyrgyzstan | 4.68 | 6.63 | 80 | 8.3 | 13.5 | 3.5 | 474 | Asia | EUR | LMI | 0.7 | Democracy |
| 23 | Lebanon | 3.52 | 6.77 | 57.7 | 2.8 | 3.9 | 1.7 | 190 | Asia | EMR | UMI | 0.74 | Democracy |
| 24 | Libya | 6.55 | 6.96 | 97 | 4.5 | 6.1 | 2.9 | 304 | Africa | EMR | UMI | 0.72 | Democracy |
| 25 | Malaysia | 16.32 | 32.78 | 61.3 | 5.8 | 9 | 2.4 | 1823 | Asia | WPR | UMI | 0.81 | Democracy |
| 26 | Maldives | 0.39 | 0.54 | 98.4 | 2.8 | 4.1 | 0.9 | 15 | Asia | SEAR | UMI | 0.74 | Democracy |
| 27 | Mali | 17.51 | 20.86 | 95 | 8 | 10.5 | 5.7 | 806 | Africa | AFR | LI | 0.43 | Democracy |
| 28 | Mauritania | 3.84 | 4.78 | 100 | 5.5 | 7.4 | 3.9 | 141 | Africa | AFR | LMI | 0.55 | Democracy |
| 29 | Morocco | 37.93 | 37.34 | 99 | 7.3 | 10.1 | 4.7 | 2617 | Africa | EMR | LMI | 0.68 | Monarchy |
| 30 | Niger | 21.1 | 25.13 | 98.3 | 10.1 | 14.1 | 6.4 | 1227 | Africa | AFR | LI | 0.39 | Democracy |
| 31 | Oman | 2.43 | 5.22 | 85.9 | 4.5 | 6.4 | 1.1 | 241 | Asia | EMR | HI | 0.81 | Monarchy |
| 32 | Pakistan | 200.4 | 225.2 | 96.5 | 9.8 | 14.6 | 4.7 | 19,331 | Asia | EMR | LMI | 0.55 | Democracy |
| 33 | Qatar | 1.57 | 2.93 | 77.5 | 4.7 | 5.7 | 1.7 | 165 | Asia | EMR | HI | 0.85 | Monarchy |
| 34 | Saudi Arabia | 31.88 | 35.34 | 97.1 | 5.4 | 7.8 | 1.9 | 2046 | Asia | EMR | HI | 0.85 | Monarchy |
| 35 | Senegal | 15.11 | 17.2 | 96.1 | 11 | 18.5 | 5.2 | 978 | Africa | AFR | LMI | 0.51 | Democracy |
| 36 | Sierra Leone | 6.07 | 8.14 | 78.6 | 11.3 | 14.8 | 8.2 | 521 | Africa | AFR | LI | 0.45 | Democracy |
| 37 | Somalia | 10.98 | 16.36 | 99.8 | 14.7 | 22.8 | 7.1 | 1219 | Africa | EMR | LI | Democracy | |
| 38 | Sudan | 39.59 | 44.91 | 97 | 4.8 | 6.3 | 3.3 | 1644 | Africa | EMR | LI | 0.51 | Authoritarian |
| 39 | Syria | 16.7 | 18.28 | 93 | 2.1 | 3.5 | 0.8 | 333 | Asia | EMR | LI | 0.57 | Authoritarian |
| 40 | Tajikistan | 7.62 | 9.75 | 96.7 | 5.3 | 7.3 | 3.4 | 399 | Asia | EUR | LI | 0.67 | Democracy |
| 41 | Tunisia | 11.19 | 11.94 | 99.8 | 3.2 | 4.6 | 1.8 | 383 | Africa | EMR | LMI | 0.74 | Democracy |
| 42 | Turkey | 79.85 | 85.04 | 99.2 | 2.3 | 3.6 | 1.2 | 2003 | Asia | EUR | UMI | 0.82 | Democracy |
| 43 | Turkmenistan | 4.83 | 6.12 | 93.3 | 6.1 | 9.4 | 2.9 | 337 | Asia | EUR | UMI | 0.71 | Democracy |
| 44 | United Arab Emirates | 4.62 | 9.99 | 76 | 5.2 | 6.3 | 2.6 | 628 | Asia | EMR | HI | 0.89 | Monarchy |
| 45 | Uzbekistan | 26.55 | 33.94 | 96.5 | 8.3 | 11.8 | 4.9 | 2653 | Asia | EUR | LMI | 0.72 | Democracy |
| 46 | Yemen | 27.78 | 30.49 | 99.1 | 7.1 | 9 | 5.3 | 1699 | Asia | EMR | LI | 0.47 | Democracy |
| Total Suicide Rate | Suicide Rate in Male | Suicide Rate in Female | ||||
|---|---|---|---|---|---|---|
| Statistics | p-Value | Statistics | p-Value | Statistics | p-Value | |
| Muslim population | rs = −0.06 | 0.64 | rs= −0.05 | 0.7 | rs = 0.03 | 0.83 |
| Total population | rs = 0.009 | 0.001 | rs = −0.003 | 0.98 | rs = 0.08 | 0.56 |
| Muslim percentage | rs = −0.08 | 0.55 | rs = −0.12 | 0.41 | rs = 0.07 | 0.61 |
| Number of suicide | rs = 0.18 | 0.22 | rs = 0.19 | 0.18 | rs = 0.20 | 0.17 |
| Continent | X2(2) = 8.1 | 0.01 | X2 (2) = 6.74 | 0.03 | X2 (2) = 15.01 | 0.001 |
| Income group | X2(2) = 10.89 | 0.01 | X2(2) = 8.02 | 0.04 | X2(2) = 19.6 | 0.001 |
| HDI Score | rs = −0.52 | 0.001 | rs= −0.47 | 0.001 | rs = −0.67 | 0.001 |
| Political system * | U = 1679 | 0.015 | U = 1679 | 0.001 | U = 1678 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arafat, S.M.Y.; Marthoenis, M.; Khan, M.M.; Rezaeian, M. Association between Suicide Rate and Human Development Index, Income, and the Political System in 46 Muslim-Majority Countries: An Ecological Study. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 754-764. https://doi.org/10.3390/ejihpe12070055
Arafat SMY, Marthoenis M, Khan MM, Rezaeian M. Association between Suicide Rate and Human Development Index, Income, and the Political System in 46 Muslim-Majority Countries: An Ecological Study. European Journal of Investigation in Health, Psychology and Education. 2022; 12(7):754-764. https://doi.org/10.3390/ejihpe12070055
Chicago/Turabian StyleArafat, S. M. Yasir, Marthoenis Marthoenis, Murad M. Khan, and Mohsen Rezaeian. 2022. "Association between Suicide Rate and Human Development Index, Income, and the Political System in 46 Muslim-Majority Countries: An Ecological Study" European Journal of Investigation in Health, Psychology and Education 12, no. 7: 754-764. https://doi.org/10.3390/ejihpe12070055
APA StyleArafat, S. M. Y., Marthoenis, M., Khan, M. M., & Rezaeian, M. (2022). Association between Suicide Rate and Human Development Index, Income, and the Political System in 46 Muslim-Majority Countries: An Ecological Study. European Journal of Investigation in Health, Psychology and Education, 12(7), 754-764. https://doi.org/10.3390/ejihpe12070055