
Psychometric Testing of the Modified Dental Anxiety Scale among Iranian Adolescents during COVID-19 Pandemic

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
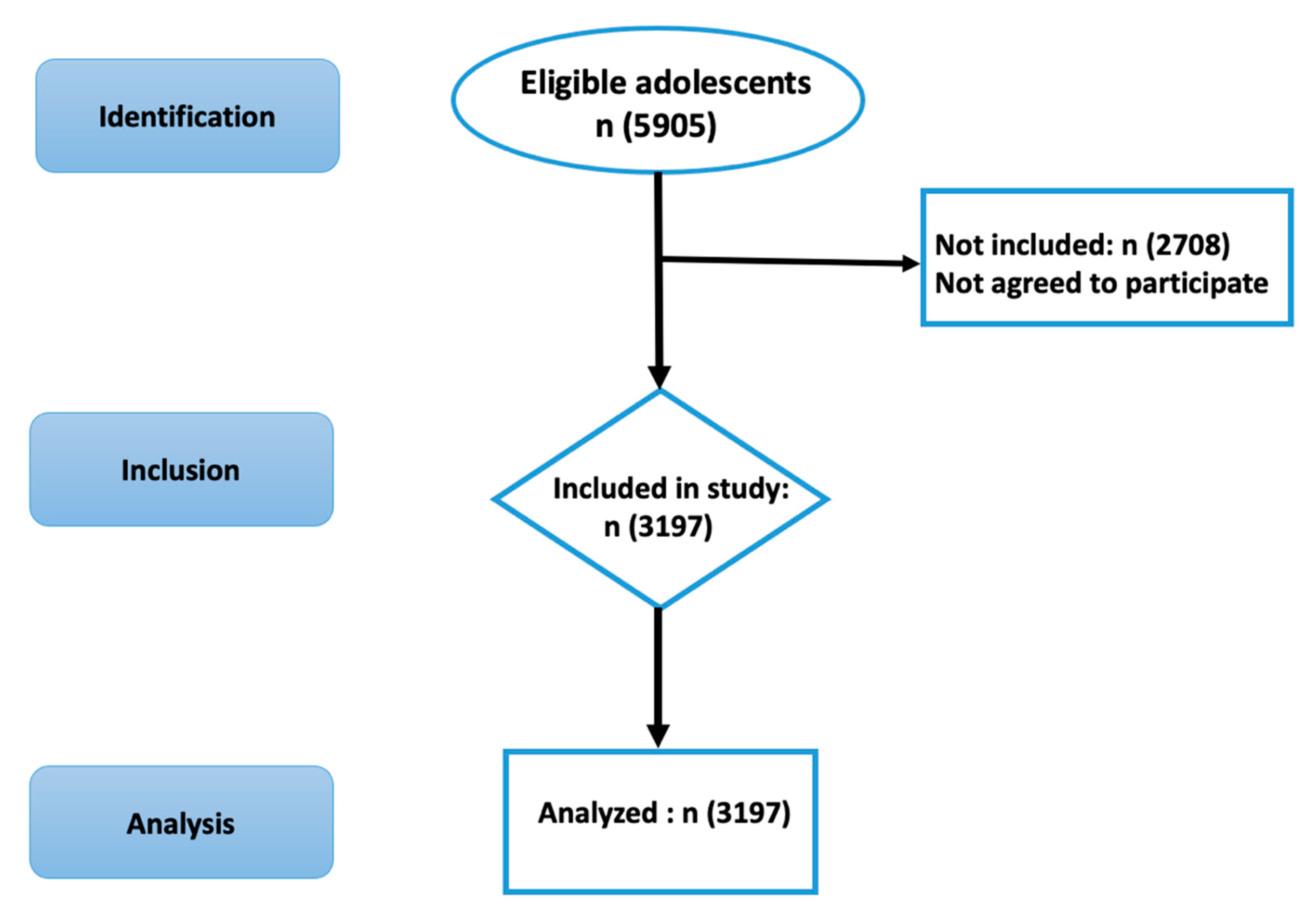
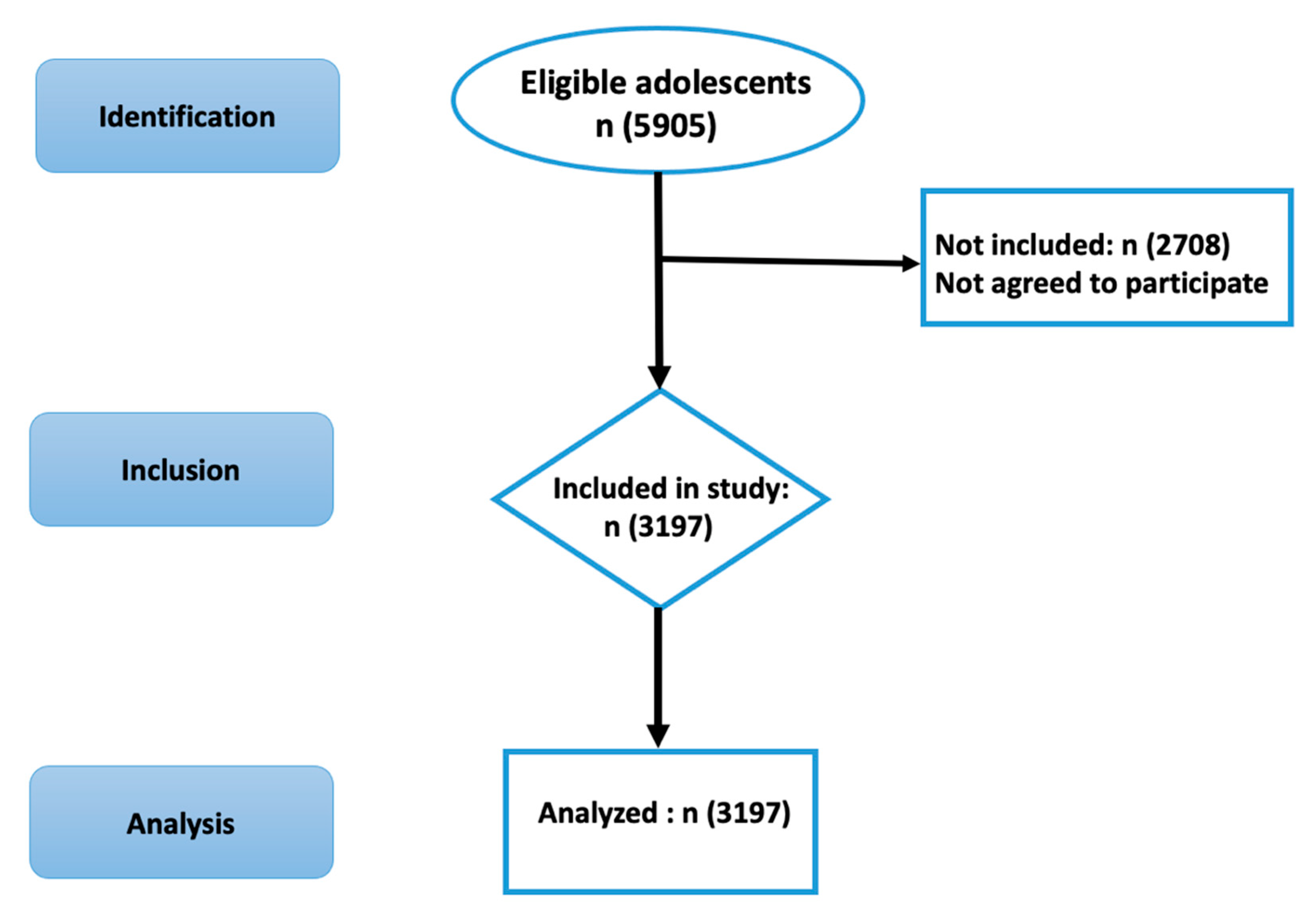
2.1. Participants
2.2. Procedures
2.3. Measures
2.4. Data Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alijanzadeh, M.; Harati, T. The role of social capital in the implementation of social distancing during the COVID-19 pandemic. Asian J. Soc. Health Behav. 2021, 4, 45–46. [Google Scholar] [CrossRef]
- Ashraf, A.; Ali, I.; Ullah, F. Domestic and gender-Based violence: Pakistan scenario amidst COVID-19. Asian J. Soc. Health Behav. 2021, 4, 47–50. [Google Scholar] [CrossRef]
- Olashore, A.A.; Akanni, O.O.; Fela-Thomas, A.L.; Khutsafalo, K. The psychological impact of COVID-19 on health-care workers in African Countries: A systematic review. Asian J. Soc. Health Behav. 2021, 4, 85–97. [Google Scholar]
- Patil, S.T.; Datar, M.C.; Shetty, J.V.; Naphade, N.M. “Psychological consequences and coping strategies of patients undergoing treatment for COVID-19 at a tertiary care hospital”: A qualitative study. Asian J. Soc. Health Behav. 2021, 4, 62–68. [Google Scholar]
- Rajabimajd, N.; Alimoradi, Z.; Griffiths, M.D. Impact of COVID-19-related fear and anxiety on job attributes: A systematic review. Asian J. Soc. Health Behav. 2021, 4, 51–55. [Google Scholar] [CrossRef]
- Sharma, R.; Bansal, P.; Chhabra, M.; Bansal, C.; Arora, M. Severe acute respiratory syndrome coronavirus-2-associated perceived stress and anxiety among Indian medical students: A cross-sectional study. Asian J. Soc. Health Behav. 2021, 4, 98–104. [Google Scholar]
- Armitage, R.; Nellums, L.B. Considering inequalities in the school closure response to COVID-19. Lancet Glob. Health 2020, 8, e644. [Google Scholar] [CrossRef] [Green Version]
- Lian, X.; Huang, J.; Huang, R.; Liu, C.; Wang, L.; Zhang, T. Impact of city lockdown on the air quality of COVID-19-hit of Wuhan city. Sci. Total Environ. 2020, 742, 140556. [Google Scholar] [CrossRef]
- Venkatesh, A.; Edirappuli, S. Social distancing in covid-19: What are the mental health implications? BMJ 2020, 369, m1379. [Google Scholar] [CrossRef] [Green Version]
- Heller, L.; Mota, C.R.; Greco, D.B. COVID-19 faecal-oral transmission: Are we asking the right questions? Sci. Total Environ. 2020, 729, 138919. [Google Scholar] [CrossRef]
- Olszewska, A.; Rzymski, P. Children’s Dental Anxiety during the COVID-19 Pandemic: Polish Experience. J. Clin. Med. 2020, 9, 2751. [Google Scholar] [CrossRef]
- Buldur, B.; Güvendi, O.N. Conceptual modelling of the factors affecting oral health-related quality of life in children: A path analysis. Int. J. Paediatr. Dent. 2020, 30, 181–192. [Google Scholar] [CrossRef]
- Ogawa, M.; Sago, T.; Furukawa, H. The Reliability and Validity of the Japanese Version of the Modified Dental Anxiety Scale among Dental Outpatients. Sci. World J. 2020, 2020, 8734946. [Google Scholar] [CrossRef]
- Dahlander, A.; Soares, F.; Grindefjord, M.; Dahllöf, G. Factors Associated with Dental Fear and Anxiety in Children Aged 7 to 9 Years. Dent. J. 2019, 7, 68. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.L.W.; Lai, S.H.F.; Wong, H.M.; Yang, Y.X.; Yiu, C.K.Y. Dental anxiety in Hong Kong preschool children: Prevalence and associated factors. Adv. Pediatr. Res. 2017, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Humphris, G.M.; Morrison, T.; Lindsay, S.J. The Modified Dental Anxiety Scale: Validation and United Kingdom Norms. Commun. Dent. Health. 1995, 12, 143–150. [Google Scholar]
- Bahammam, M.A.; Hassan, M.H. Validity and reliability of an Arabic version of the modified dental anxiety scale in Saudi adults. Saudi Med. J. 2014, 35, 1384–1389. [Google Scholar]
- Giri, J.; Pokharel, P.R.; Gyawali, R.; Bhattarai, B. Translation and Validation of Modified Dental Anxiety Scale: The Nepali Version. Int. Sch. Res. Not. 2017, 2017, 5495643. [Google Scholar] [CrossRef] [Green Version]
- Humphris, G.M.; Dyer, T.A.; Robinson, P.G. The modified dental anxiety scale: UK general public population norms in 2008 with further psychometrics and effects of age. BMC Oral Health 2009, 9, 20. [Google Scholar] [CrossRef] [Green Version]
- Paglia, L.; Gallus, S.; de Giorgio, S.; Cianetti, S.; Lupatelli, E.; Lombardo, G.; Montedori, A.; Euseb, P.; Gatto, R.; Caruso, S. Reliability and validity of the Italian versions of the Children’s Fear Survey Schedule—Dental Subscale and the Modified Child Dental Anxiety Scale. Eur. J. Paediatr. Dent. 2017, 18, 305–312. [Google Scholar] [CrossRef]
- Saatchi, M.; Abtahi, M.; Mohammadi, G.; Mirdamadi, M.; Binandeh, E.S. The prevalence of dental anxiety and fear in patients referred to Isfahan Dental School, Iran. Dent. Res. J. 2015, 12, 248. [Google Scholar]
- Lin, C.Y.; Griffiths, M.D.; Pakpour, A.H. Psychometric evaluation of Persian Nomophobia Questionnaire: Differential item functioning and measurement invariance across gender. J. Behav. Addict. 2018, 7, 100–108. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.P.; Luh, W.M.; Yang, A.L.; Su, C.T.; Lin, C.Y. Agreement of children and parents scores on Chinese version of Pediatric Quality of Life Inventory Version 4.0: Further psychometric development. Appl. Res. Qual. Life 2016, 11, 891–906. [Google Scholar] [CrossRef]
- Lin, C.Y.; Broström, A.; Griffiths, M.D.; Pakpour, A.H. Psychometric evaluation of the Persian eHealth Literacy Scale (eHEALS) among elder Iranians with heart failure. Eval. Health Prof. 2020, 43, 222–229. [Google Scholar] [CrossRef] [Green Version]
- Nejati, B.; Fan, C.W.; Boone, W.J.; Griffiths, M.D.; Lin, C.Y.; Pakpour, A.H. Validating the Persian Intuitive Eating Scale-2 Among Breast Cancer Survivors Who Are Overweight/Obese. Eval. Health Prof. 2020. [CrossRef]
- Bagheri, Z.; Jafari, P.; Tashakor, E.; Kouhpayeh, A.; Riazi, H. Assessing whether measurement invariance of the KIDSCREEN-27 across child-parent dyad depends on the child gender: A multiple group confirmatory factor analysis. Glob. J. Health Sci. 2014, 6, 142–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.F. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct. Equ. Model. Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Lin, C.Y.; Imani, V.; Griffiths, M.D.; Pakpour, A.H. Validity of the Yale Food Addiction Scale for Children (YFAS-C): Classical test theory and item response theory of the Persian YFAS-C. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2021, 26, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Hamzah, S.H.; Yiu, C.K.; McGrath, C.; King, N.M. Dental fear and anxiety in children and adolescents: Qualitative study using YouTube. J. Med. Internet Res. 2013, 15, e29. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Authors | Year | Objective | Merits | Demerits | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ogawa et al. [13] | 2020 | 1. Examine the reliability and validity of the Japanese MDAS. 2. Compare the prevalence of dental anxiety between Japan and other countries | Using CTT to test the psychometric properties for the Japanese MDAS among dental outpatients | Having no evidence in corrected item-total correlation, test–retest reliability, measurement invariance, known-group validity, and Rasch analysis. | Y | N | N | Y | N | N | N |
| Bahammam & Hassan [17] | 2014 | Examine the reliability and validity of the Arabic MDAS. | Using CTT to test the psychometric properties for the Arabic MDAS among dental outpatients | Having no evidence in test–retest reliability, factor analysis, measurement invariance, known-group validity, and Rasch analysis. | Y | Y | N | N | N | N | N |
| Giri et al. [18] | 2017 | Examine the reliability and validity of the Nepali MDAS. | Using CTT to test the psychometric properties for the Nepali MDAS among dental outpatients | Having no evidence in measurement invariance, known-group validity, and Rasch analysis. | Y | Y | Y | Y | N | N | N |
| Humphris et al. [19] | 2009 | 1. Confirm factor structure of the MDAS. 2. Establish an UK norm of dental fear | Using CTT to test the psychometric properties for the British MDAS among general population | Having no evidence in corrected item-total correlation, test–retest reliability, measurement invariance, known-group validity, and Rasch analysis. | Y | N | N | Y | N | N | N |
| Paglia et al. [20] | 2017 | 1. Examine the reliability and validity of the Italian MDAS for children version. 2. Compare the difference between child-rated and parent-rated MDAS. 3. Quantify the prevalence of dental fear among children. | Using CTT to test the psychometric properties for the Italian MDAS among pediatric population with the use of parent-proxy reports | Having no evidence in factor analysis, measurement invariance, and Rasch analysis. | Y | Y | Y | N | N | Y | N |
| Saatchi et al. [21] | 2015 | Evaluate the dental anxiety and fear in dental patients | Having the psychometric evidence of internal consistency in Iranian dental patients | Having no evidence in corrected item-total correlation, test–retest reliability, factor analysis, measurement invariance, known-group validity, and Rasch analysis. | Y | N | N | N | N | N | N |
| n (%) or Mean ± SD | |
|---|---|
| Age | 15.10 ± 1.62 |
| Gender (male) | 1507 (47.1%) |
| Number of family members | |
| ≤4 | 2292 (71.7%) |
| 5–7 | 552 (17.3%) |
| >7 | 353 (11.0%) |
| Years of education completed by father | 9.79 ± 5.11 |
| Years of education completed by mother | 7.74 ± 5.01 |
| Time since last dental visit | |
| <6 months | 396 (12.4%) |
| 6 months to 1 year | 604 (18.9%) |
| 1 to 2 years | 797 (30.6%) |
| >2 years | 641 (20.1%) |
| Never | 577 (18.0%) |
| Frequency of toothbrushing | |
| Never | 267 (8.4%) |
| Less than once per month | 199 (6.2%) |
| Less than once per week | 170 (5.3%) |
| Once per week | 509 (15.9%) |
| Once per day | 1442 (64.2%) |
| Twice per day | 610 (19.1%) |
| Frequency of using dental floss | |
| Never | 1583 (49.5%) |
| Less than once per month | 334 (10.4%) |
| Less than once per week | 323 (10.1%) |
| Once per week | 451 (14.1%) |
| Once per day | 506 (15.9%) |
| Item # | Analyses from Classical Test Theory | Rasch Analyses | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Factor Loading *,† | Item-Total Correlation | Test–Retest Reliability ‡ | S | K | Infit MnSq | Outfit MnSq | Difficulty | Discrimination | DIF Contrast across Gender §,¶ | DIF Contrast across Dental Visit §,# | |
| MDAS1 | 0.870 | 0.717 | 0.721 | −0.854 | −0.176 | 1.01 | 1.00 | −0.76 | 0.99 | −0.10 | −0.10 |
| MDAS2 | 0.981 | 0.782 | 0.779 | −0.788 | −0.294 | 0.80 | 0.84 | −0.52 | 1.20 | −0.09 | −0.08 |
| MDAS3 | 0.919 | 0.692 | 0.812 | −0.157 | −1.090 | 1.06 | 1.08 | 0.49 | 0.92 | 0.09 | 0.13 |
| MDAS4 | 0.962 | 0.705 | 0.863 | −0.364 | −0.880 | 1.11 | 1.10 | 0.28 | 0.89 | 0.02 | 0.00 |
| MDAS5 | 0.973 | 0.737 | 0.794 | −0.232 | −0.937 | 0.91 | 0.93 | 0.51 | 1.05 | 0.00 | 0.02 |
| Psychometric Testing | MDAS |
|---|---|
| Composite Reliability | 0.975 |
| Average Variance Extracted | 0.887 |
| Internal consistency (Cronbach’s α) | 0.887 |
| Internal consistency (McDonald’s ω) | 0.851 |
| Item separation reliability from Rasch | 1.00 |
| Item separation index from Rasch | 19.87 |
| Person separation reliability from Rasch | 0.83 |
| Person separation index from Rasch | 2.23 |
| Configural Model | Metric | Scalar | Strict | |
|---|---|---|---|---|
| Gender (males vs. females) | ||||
| Χ2(df)/(ΔΧ2 [Δdf]) | 80.531 (10)/-- | 82.074 (14)/1.543 (4) | 85.011 (18)/2.937 (4) | 85.924 (23)/0.913 (5) |
| p-value for ΔΧ2 | -- | 0.82 | 0.57 | 0.97 |
| CFI/(ΔCFI) | 0.994/-- | 0.994/0.000 | 0.994/0.000 | 0.994/0.000 |
| RMSEA/(ΔRMSEA) | 0.066/-- | 0.055/−0.011 | 0.048/−0.007 | 0.041/−0.007 |
| SRMR/(ΔSRMR) | 0.047/-- | 0.048/0.001 | 0.042/−0.006 | 0.042/0.000 |
| Time since last dental visit (adolescents visited a dentist in the past six months vs. adolescents not visited a dentist in the past six months) | ||||
| Χ2(df)/(ΔΧ2 [Δdf]) | 80.342 (10)/-- | 81.210 (14)/0.868 (4) | 84.721 (18)/3.511 (4) | 88.676 (23)/3.955 (5) |
| p-value | -- | 0.93 | 0.48 | 0.56 |
| CFI/(ΔCFI) | 0.994/-- | 0.994/0.000 | 0.994/0.000 | 0.994/0.000 |
| RMSEA/(ΔRMSEA) | 0.066/-- | 0.055/−0.011 | 0.048/−0.007 | 0.042/−0.006 |
| SRMR/(ΔSRMR) | 0.048/-- | 0.048/0.000 | 0.042/−0.006 | 0.043/0.001 |
| AIC | BIC | SSABIC | Entropy | LMR Test (p-Value) | |
|---|---|---|---|---|---|
| Class 1 | 47,710.753 | 47,832.152 | 47,768.604 | n/a | n/a |
| Class 2 | 41,152.266 | 41,401.135 | 41,270.860 | 0.940 | 6561.768 (<0.0001) |
| Class 3 | 39,708.981 | 40,085.319 | 39,888.319 | 0.864 | 1476.572 (0.0337) |
| Class 4 | 39,011.515 | 35,515.322 | 39,251.596 | 0.875 | 735.128 (0.6277) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-Y.; Tofangchiha, M.; Scheerman, J.F.M.; Tadakamadla, S.K.; Chattu, V.K.; Pakpour, A.H. Psychometric Testing of the Modified Dental Anxiety Scale among Iranian Adolescents during COVID-19 Pandemic. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1269-1279. https://doi.org/10.3390/ejihpe11040092
Lin C-Y, Tofangchiha M, Scheerman JFM, Tadakamadla SK, Chattu VK, Pakpour AH. Psychometric Testing of the Modified Dental Anxiety Scale among Iranian Adolescents during COVID-19 Pandemic. European Journal of Investigation in Health, Psychology and Education. 2021; 11(4):1269-1279. https://doi.org/10.3390/ejihpe11040092
Chicago/Turabian StyleLin, Chung-Ying, Maryam Tofangchiha, Janneke F. M. Scheerman, Santosh Kumar Tadakamadla, Vijay Kumar Chattu, and Amir H. Pakpour. 2021. "Psychometric Testing of the Modified Dental Anxiety Scale among Iranian Adolescents during COVID-19 Pandemic" European Journal of Investigation in Health, Psychology and Education 11, no. 4: 1269-1279. https://doi.org/10.3390/ejihpe11040092
APA StyleLin, C.-Y., Tofangchiha, M., Scheerman, J. F. M., Tadakamadla, S. K., Chattu, V. K., & Pakpour, A. H. (2021). Psychometric Testing of the Modified Dental Anxiety Scale among Iranian Adolescents during COVID-19 Pandemic. European Journal of Investigation in Health, Psychology and Education, 11(4), 1269-1279. https://doi.org/10.3390/ejihpe11040092