1. Introduction
Coronaviruses are a large family of viruses known to cause diseases ranging from the common colds to more serious diseases, such as Middle Eastern Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) [
1]. A new coronavirus outbreak started in Wuhan city, Hubei Province, China, in December 2019 and January 2020, and has spread widely across the world since then. The Coronavirus disease 2019 (COVID-19) evolved as a public health emergency due to its spread within most countries, and was declared a pandemic by the World Health Organization (WHO) on 11 March 2020 [
2]. This Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) has infected 219,189,790 individuals globally, with 4,544,789 deaths, as of 3 September 2021. In Portugal, the pandemic of COVID-19 has infected 1,042,322 infected individuals, with 17,766 mortalities [
3].
Being highly infectious, the virus has put pressure on health systems everywhere, stretching them beyond their capacity and pushing them to disruption [
4]. While authorities strive to monitor outbreak trends and mitigate the pandemic’s impact on health systems, the economy has been suffering a strong negative impact worldwide, especially in countries relying on services [
5]. This is also the case in Portugal, where whole industries and jobs are threatened, such as the travel and tourism-related businesses, which accounted for more than 19% of exports and over 8% of gross domestic product (GDP) in 2019 [
6]. This unsettling scenario has several direct and indirect effects, including on physical and mental health [
7,
8,
9]. The outbreak has a psychological impact on individuals and society [
10], as has been reported in different studies, namely, regarding depression, anxiety, stress [
7,
11], risk-attitudes [
12], fear [
13], perceived risk [
14] and coronophobia [
15]. In fact, Deng and colleagues [
9] found that 45% of COVID-19 patients experience depression, 47% anxiety and 34% sleep disturbances. Additionally, Wang and colleagues [
16] found that the most common psychological problems were somatization symptoms, depression, anxiety, problems of insomnia, and self-mutilating or suicidal thoughts. Cielo and colleagues [
11] found a negative psychological impact and a high vulnerability of the young in the development of psychological distress, highlighting the need for structured and tailored psychological support. However, Prati and Mancini [
17] stated that the psychological impact of COVID-19 lockdowns is small in magnitude and highly heterogeneous, suggesting that most people are psychologically resilient to their effects. In Portugal, there are almost no validated instruments specifically designed from scratch to assess the psychological impact of COVID-19. The aim of this study is to validate the COVID-19 Perceived Risk Scale (C19PRS) and the COVID-19 Phobia Scale (C19PS) in the Portuguese population.
Risk perception is the subjective assessment that people perform about something, concerning its characteristics, severity, and ways in which the risk can be managed [
18]. A higher level of perceived risk was found in relation to COVID-19 as compared to other potential health threats [
19]. According to Slovic [
20], the characteristics of risk perception include (1) voluntariness (the risk of COVID-19 is imposed by external forces and is uncontrollable, thus being perceived as greater); (2) knowledge (COVID-19 is mostly unknown and unusual, making the perceived risk more frightening); (3) visibility (COVID-19 is an invisible risk, making it perceived as more hazardous than a visible one); (4) trust (the unknown nature of the disease, its repercussion in the mass media) [
19]. The high numbers of infected and dead people, and the difficulty in having a common strategy, decrease people’s confidence in the management of the pandemic, which leads to a higher perception of risk. COVID-19 constitutes itself as a risk event that is related not only to people’s event-related risk perception, but also to their general risk perception [
21]. Bruine de Bruin [
22] stated that older age was associated with perceiving larger risks of dying if getting COVID-19, but with perceiving less risk of getting COVID-19, getting quarantined, or running out of money, as well as less depression and anxiety. Accordingly, He and colleagues [
23] found that the perceived risk of getting COVID-19 increased by 4.9% for every one-year increase in age. Siegrist et al. [
24] considered that perceived risks are important drivers for the acceptance of the government’s implemented measures to control COVID-19, and for more precautionary behavior.
A misperception of risk in relation to the real risk may lead people to the development of disruptive cognitive, affective, or behavioral responses to the COVID-19 pandemic, namely, coronaphobia. Fear is an adaptive animal defense mechanism fundamental for survival; however, if it is chronic or disproportionate, it may become harmful and can lead to the development of various psychiatric disorders [
25]. According to Amin [
26], coronaphobia is a persistent and excessive fear of the novel coronavirus, being classified as a particular type of DSM-5-specific phobia. Arpaci et al. [
15] stated that natural disasters, such as the COVID-19 pandemic, can trigger phobic conditions with severe consequences for mental health. Lee et al. [
27] found that coronaphobia explained additional variance in depression, generalized anxiety, and death anxiety, above sociodemographics, COVID-19 factors, and the vulnerability factors of neuroticism, health anxiety, and reassurance-seeking behaviors. Additionally, Lee and Crunk [
28] reported that neuroticism, coronaphobia, and hypochondriasis were fear factors that predicted pandemic-related psychopathology in adults. Toprak et al. [
29] found that individuals who stayed at home had higher coronaphobia than individuals who continued to work during the 3-month COVID-19 pandemic lockdown. According to Cihan and Durmaz [
30], phobia scores were significantly higher in women, singles, people living alone, those living in an apartment, and those with higher economic and educational levels. Durmu and Durar [
31] found a significant negative relationship between spiritual meaning and individuals’ fear of coronavirus, and between peace and fear of coronavirus. Individuals’ spirituality increases as fear of coronavirus decreases. Aware of the negative psychological impact of the pandemic on people, and aware of the importance of determining the specificity of that impact, Yıldırım and Güler [
14] developed the COVID-19 Perceived Risk Scale (C19PRS), and Arpaci et al. [
15] conceived the COVID-19 Phobia Scale (C19PS). Besides this, Yildirim et al. [
32] found that perceived risk and fear can significantly increase engagement in preventive behaviors. However, Yildirim and Guler [
33] found that COVID-19 perceived risk increases death distress and reduces happiness. Arpaci and colleagues [
34] found a significant positive correlation between coronaphobia and state anxiety. Additionally, Arpaci and colleagues [
35] found that people were afraid of being infected, and those who got infected were afraid of death. In Portugal, there are no validated instruments to assess these dimensions; therefore, the aim of this study is to adapt the C19PRS and the C19PS to the Portuguese population.
4. Discussion
The psychological impact of the COVID-19 pandemic has been studied by different authors with the aim of improving the psychological assessment and intervention of people most affected by COVID-19. To this end, validated instruments are needed to diagnose and intervene in a timely and appropriate manner. Therefore, the aim of this study was to validate two instruments for the general Portuguese population, using a sample of Portuguese adults: COVID-19 Perceived Risk Scale (C19PRS) [
14] and COVID-19 Phobia scale (C19PS) [
15].
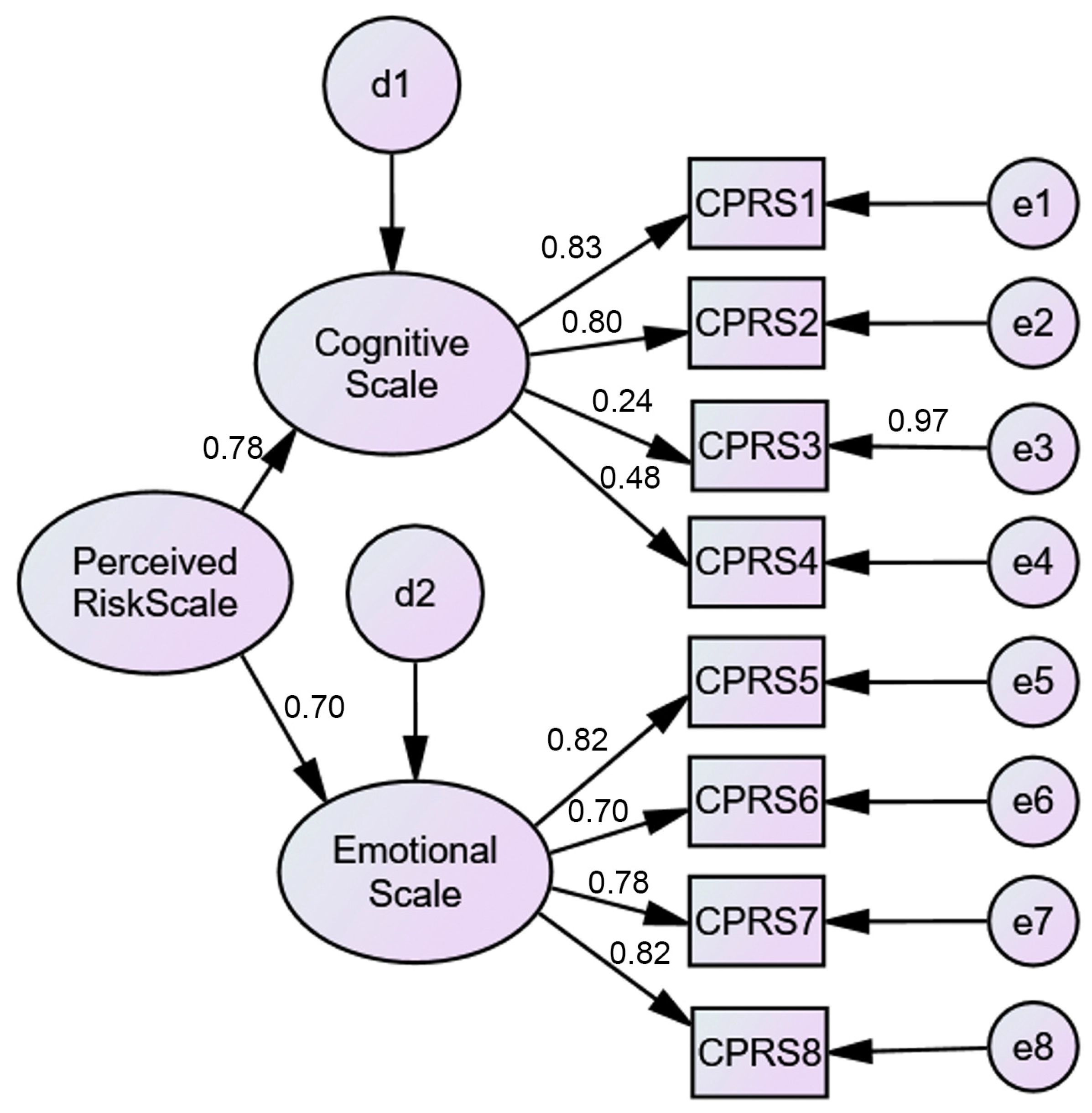
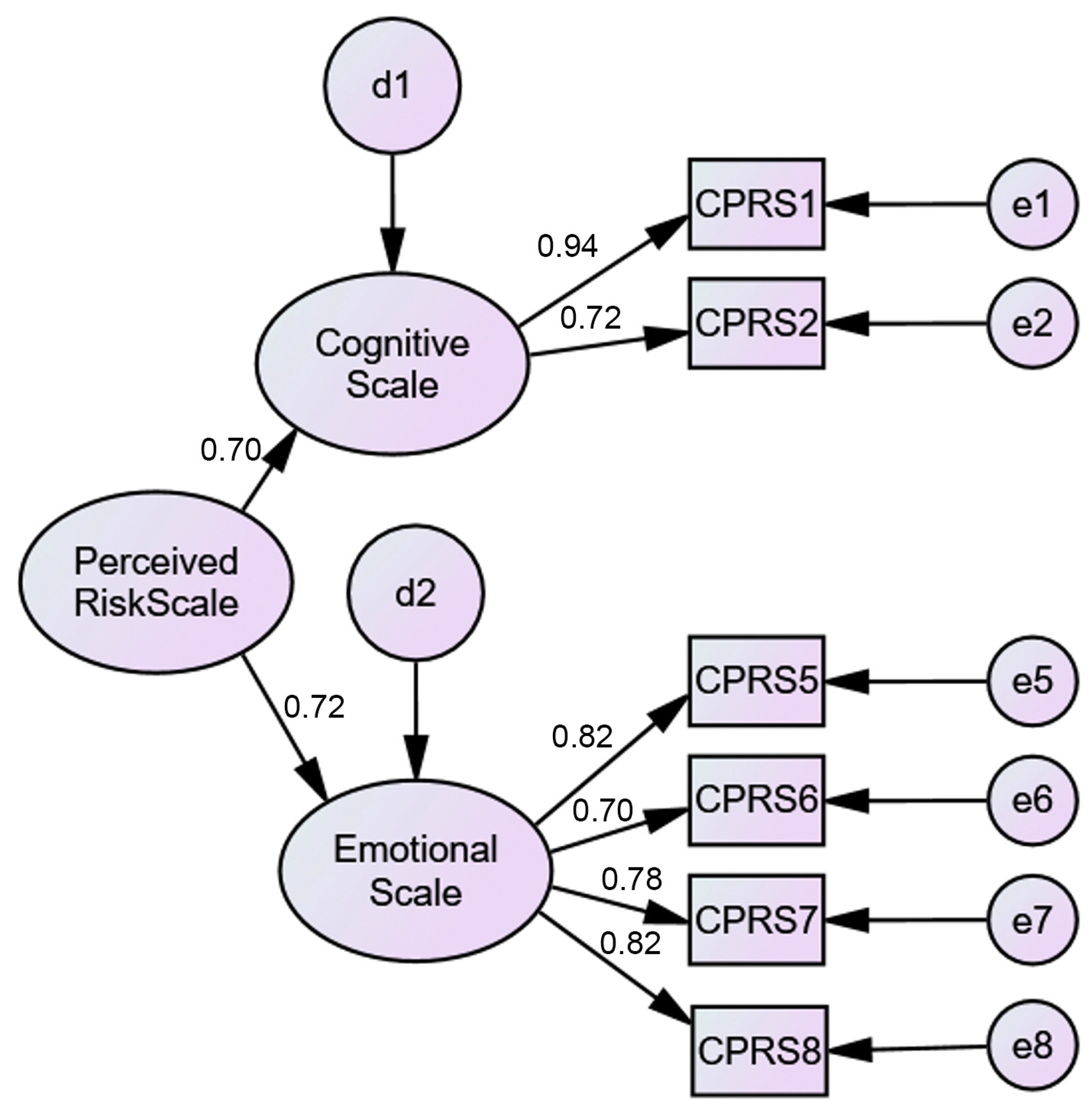
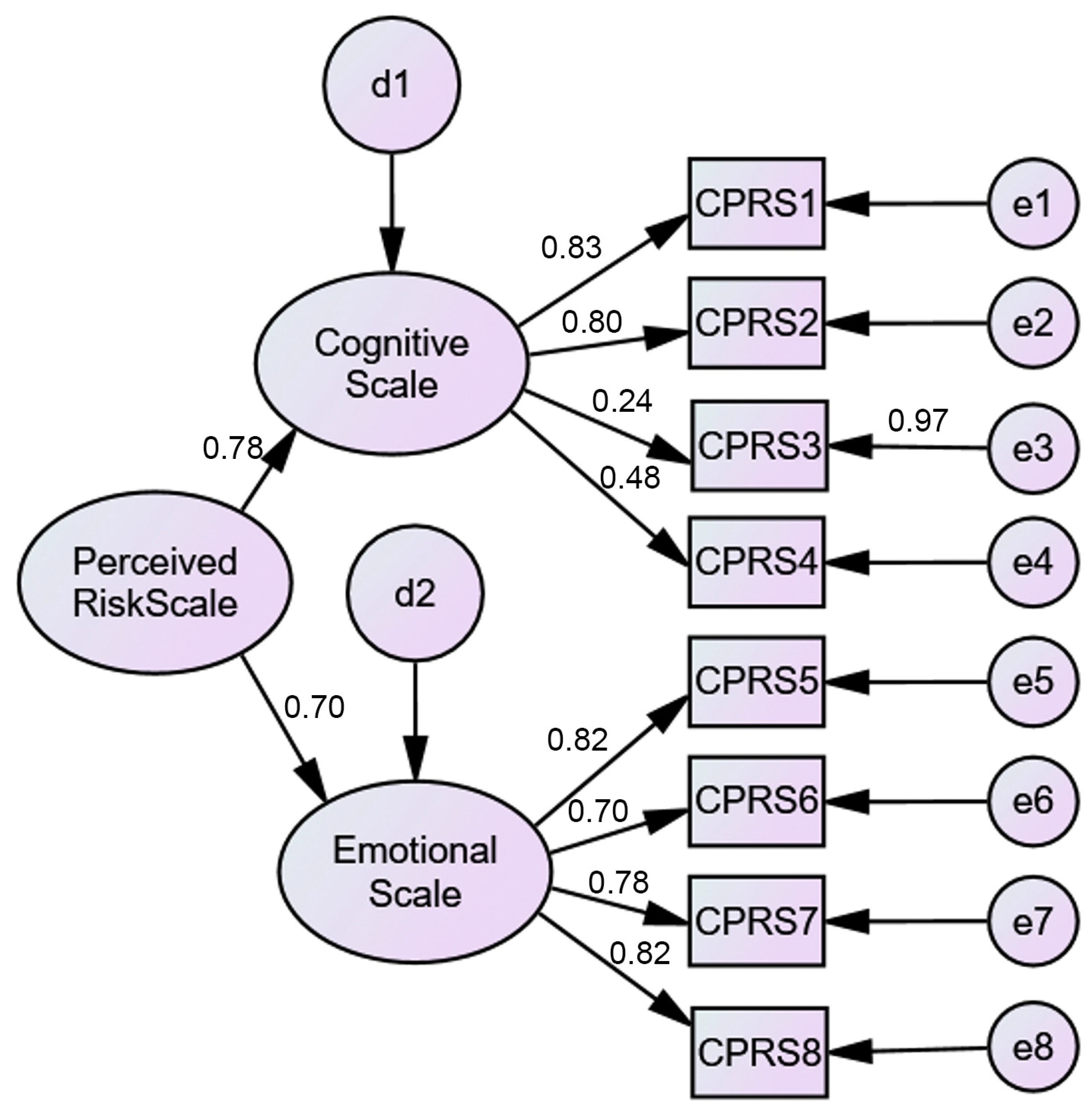
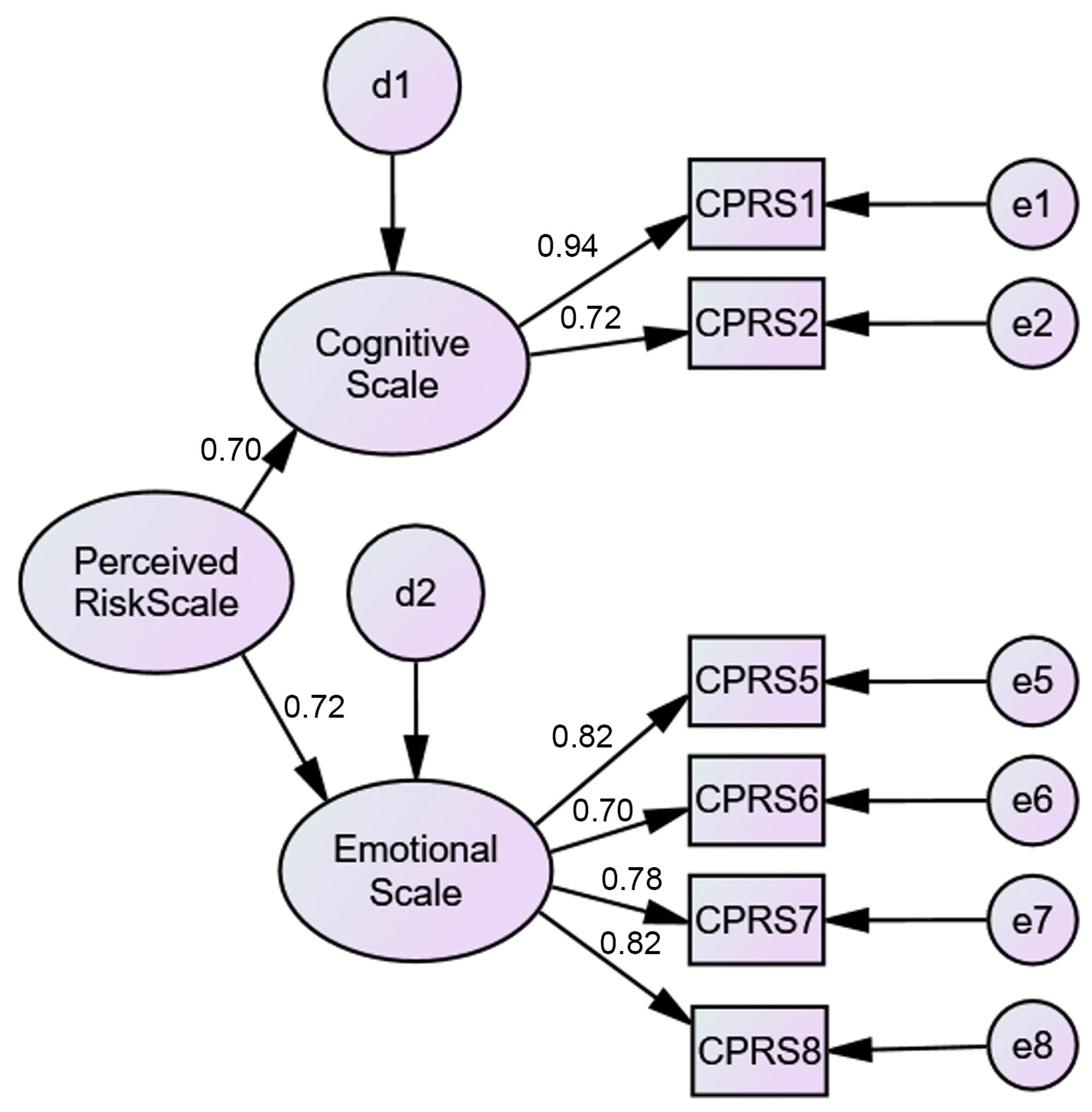
The validation of the C19PRS did not confirm the original structure proposed by the authors (eight items evenly distributed by two factors). In fact, the structure of this construct, in the Portuguese version, excludes two items (item 3 and item 4) from factor 1 (cognitive), with factor 2 (emotional) remaining the same as the original. In the Portuguese version, it is suggested that the C19PRS be a multidimensional scale, including cognitive and emotive aspects of perceived personal risk related to COVID-19. The Portuguese version showed good internal consistency, reliability, convergent validity, and evidence of gender differences in the C19PRS total and subscales.
C19PRS correlates positively and significantly with fear, anxiety, and phobia related to COVID-19: the higher the perceived risk of contracting COVID-19, the higher the fear, anxiety, and phobia in relation to COVID-19. These results corroborate those of Amin [
26], Arpaci et al. [
15], Cori et al. [
18], Ho et al. [
10], Lee [
41], Lee and Crunk [
28], Lee et al. [
27], Magano et al. [
13], Paulino et al. [
7], Wang et al. [
47], Yıldırım and Güler [
14] and Zhong et al. [
19]. Deng and colleagues [
9] found that most COVID-19 patients experience depression, anxiety, and sleep disturbances. Cielo and colleagues [
11] found a negative psychological impact on, and high vulnerability in, the young in the context of developing psychological distress. The adaptation of the C19PS [
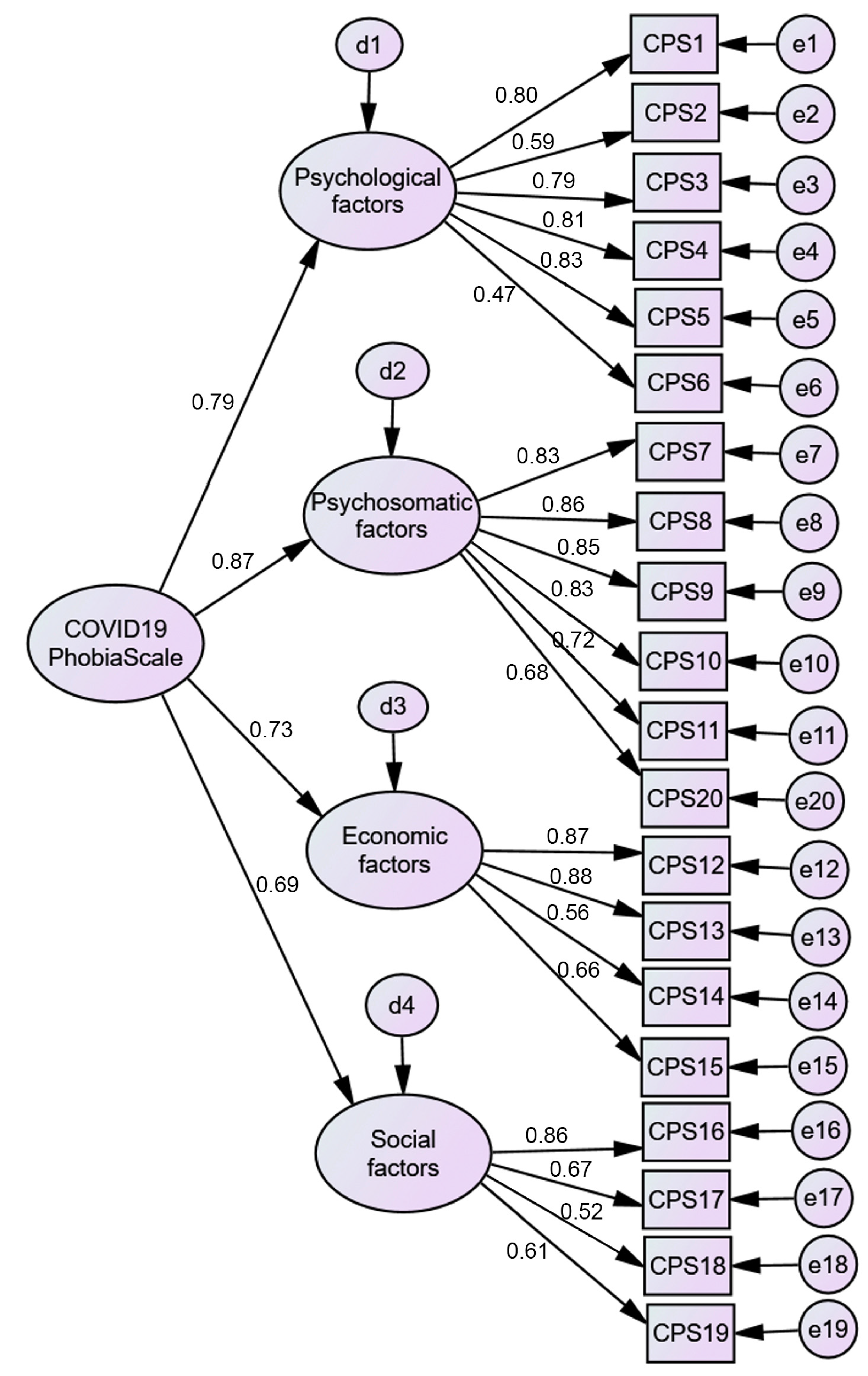
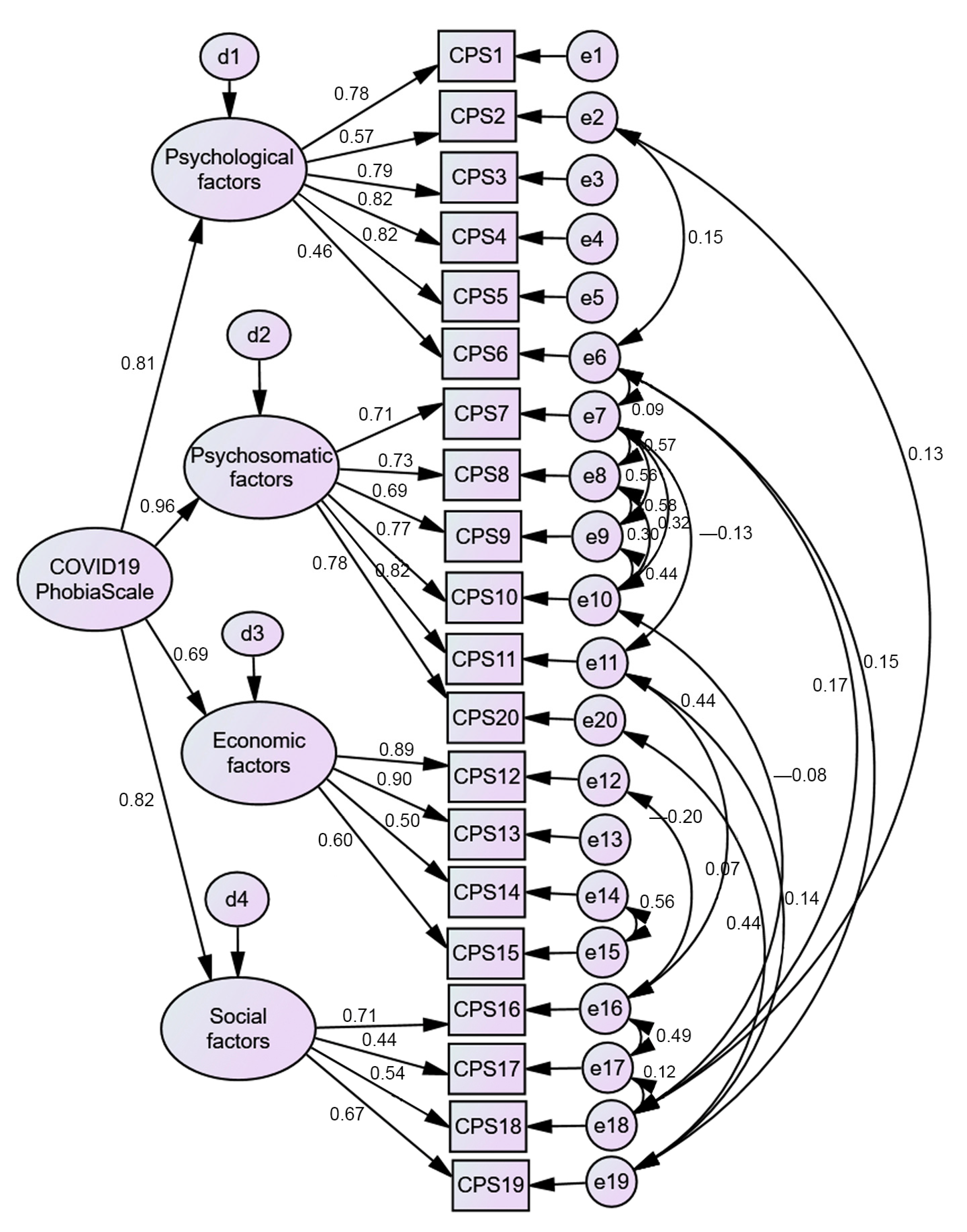
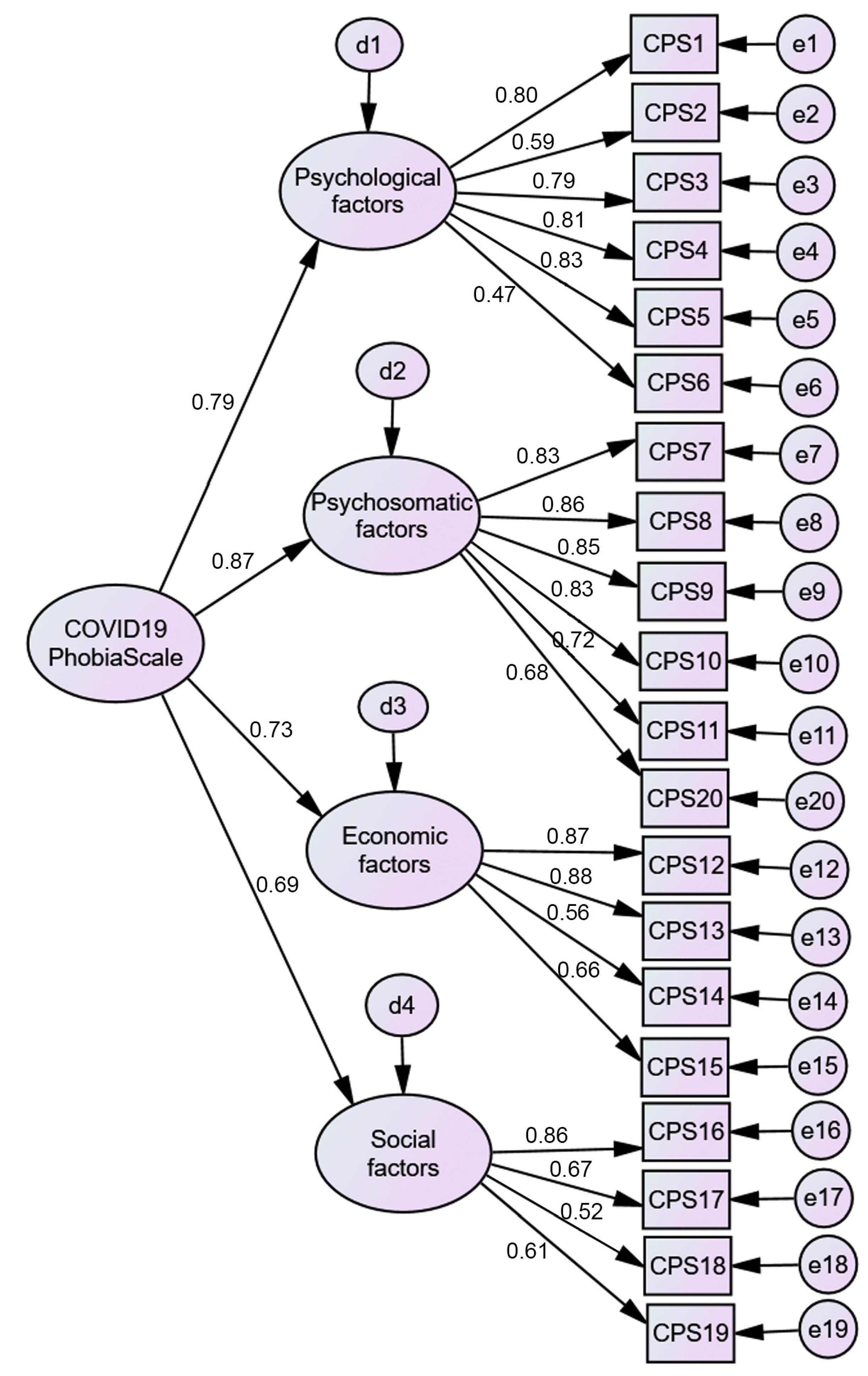
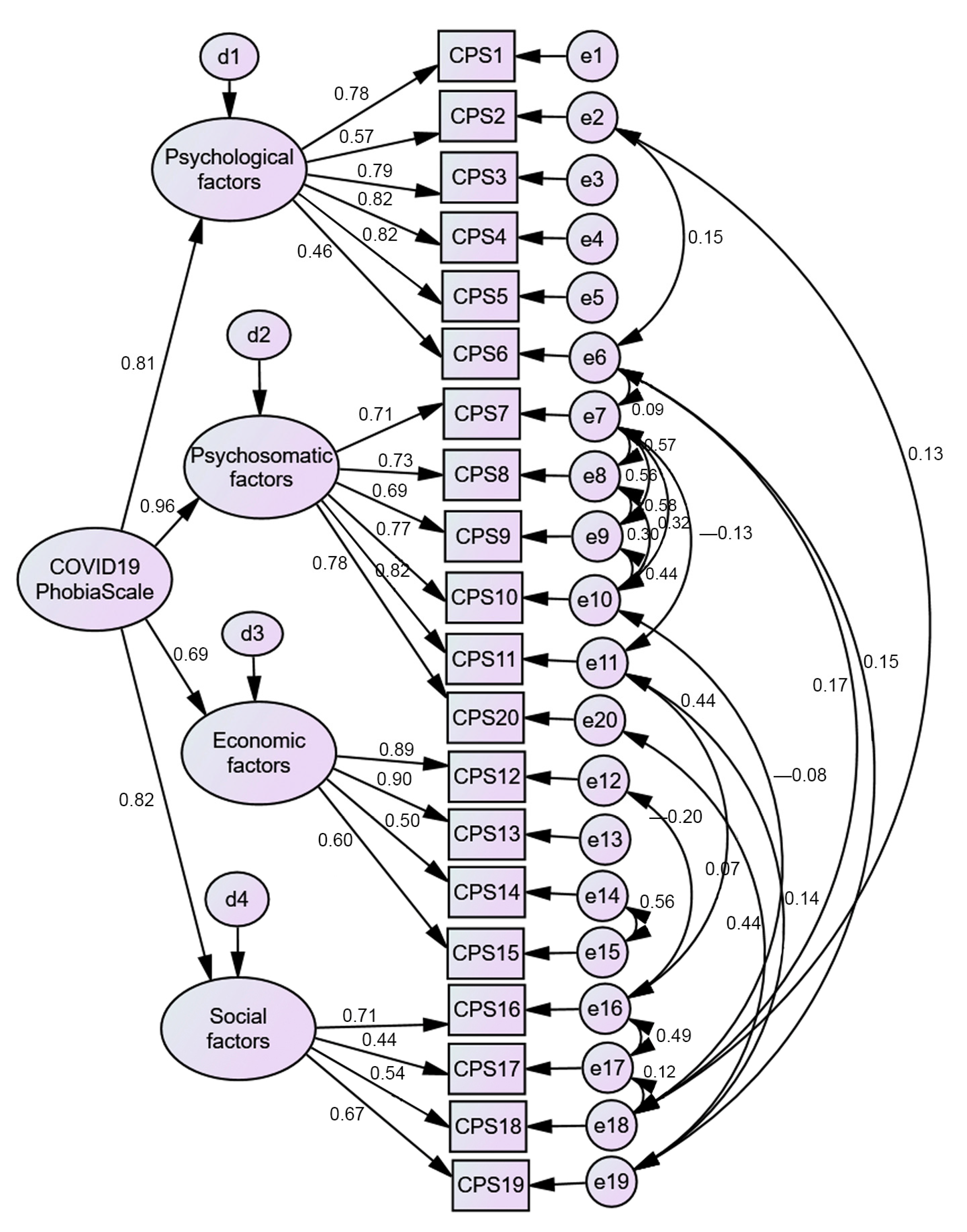
15] confirmed the original structure proposed by the authors (20 items distributed by four factors—psychological, psychosomatic, economic, and social factors), although item 20 (“I am unable to curb my anxiety of catching coronavirus from others”), in the original version, saturated in factor 4 (social factor), and in this study, it saturated in factor 1 (psychosomatic factor). In fact, the content of the item can be referred to as a social factor (
getting the virus from others), but it can also be addressed as a psychosocial factor (
I can’t control the anxiety). In our study, this item clearly saturated in the psychosomatic factor and, in addition, if it was removed from this factor, the value of the Cronbach’s alpha decreased. Therefore, the authors decided to keep it in this factor. Good model adjustment was obtained only after the establishment of several correlations between item errors. The Portuguese version showed good internal consistency, reliability, convergent validity, and evidence of gender differences in the C19PS total and its subscales. C19PS correlates positively and significantly with fear, anxiety, and risk perception related to COVID-19: the higher the phobia of COVID-19, the higher the fear, anxiety, and risk perception in relation to COVID-19. These results are also in line with those of Amin [
26], Arpaci et al. [
15], Ho et al. [
10], Lee [
41], Lee and Crunk [
28], Lee et al. [
27], Magano et al. [
13], Paulino et al. [
7], Toprak Celenay et al. [
29], and Wang et al. [
47].
Gender differences were found in the values of C19PRS and C19PS, with women scoring higher, which is in line with the results of Cihan and Durmaz [
30], who found phobia scores significantly higher in women. Additionally, Rodriguez-Besteiro et al. [
48] found that females presented a higher perception of danger (assessed by the risk perception scale) related to the COVID-19 virus than males. Concerning age, Bruine de Bruin [
22] and He and colleagues [
23] found that older people perceived larger risks of dying from getting COVID-19, but perceived less risk of getting COVID-19, getting quarantined, or running out of money, as well as less depression and anxiety.
The implications of this study include the empowerment of Portuguese psychologists, who now have an instrument to assess COVID-19-related risk perception and phobia. Future studies with these instruments should be based on representative samples of the Portuguese population.
This study presents some limitations: (1) the participants belong to the general Portuguese population, but they are not representative of it; (2) the perceived risk and phobia related to COVID-19 are self-reported, and some respondents may have provided the desired social responses; (3) the professional distribution in the present study was unequal, with 83.1% active, which might affect the psychometric evaluation; finally, (4) convenience sampling may skew the results.



 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}