The Effectiveness of Mindfulness-Based Interventions on Anxiety Disorders. A Systematic Meta-Review




Abstract
1. Introduction
2. Materials and Methods
2.1. Sources/Literature Research
2.2. Selection Criteria
2.3. Exclusion Criteria
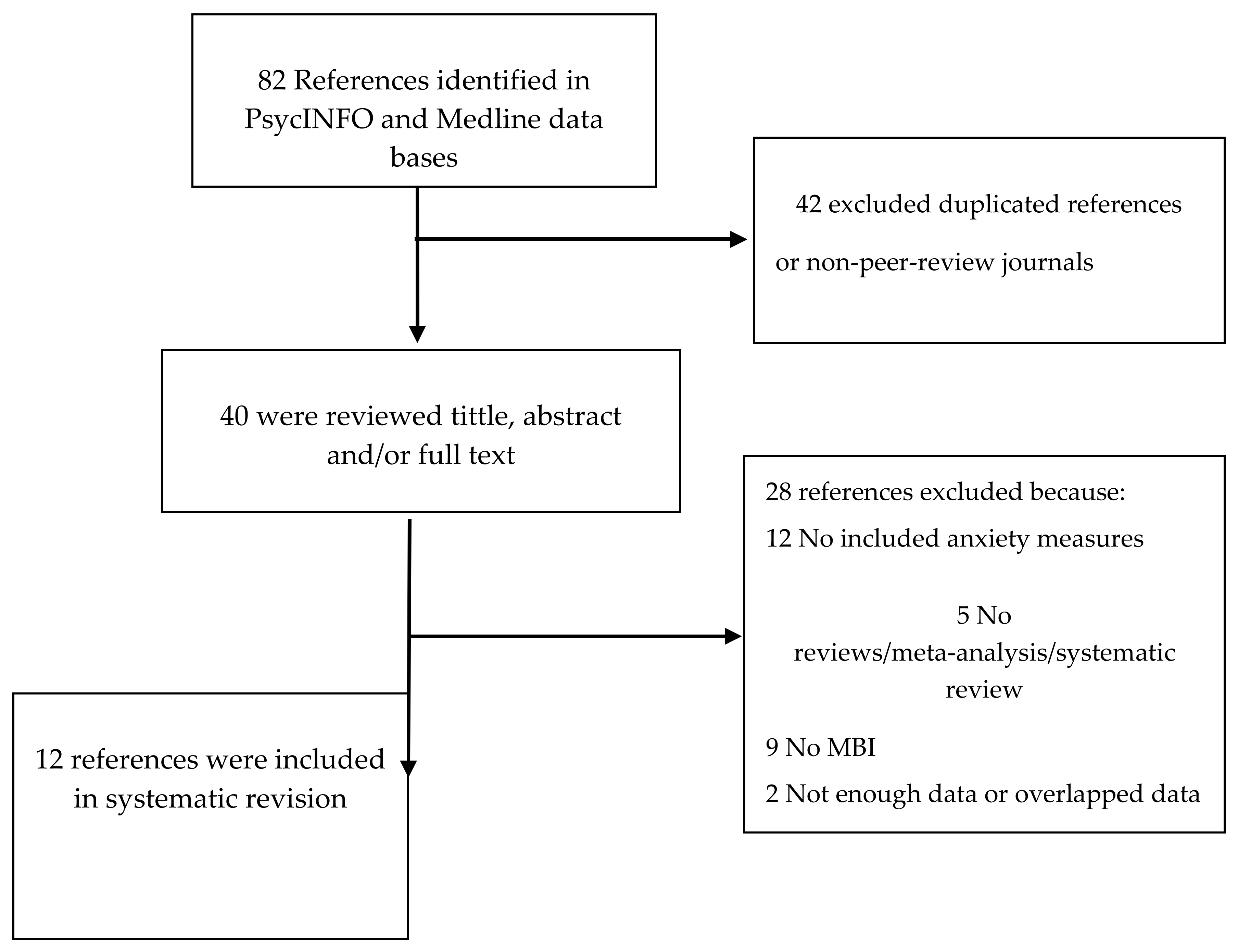
2.4. Study Selection and Data Extraction
2.5. Data Analysis and Synthesis
3. Results
3.1. Descriptive Characteristics
3.2. MBI Effectiveness
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Williams, J.M.G.; Kabat-Zinn, J. Mindfulness: Diverse perspectives on its meaning, origins, and multiple applications at the intersection of science and dharma. Contemp. Buddhism. 2011, 12, 1–18. [Google Scholar] [CrossRef]
- Crane, R.S.; Brewer, J.; Feldman, C.; Kabat-Zinn, J.; Santorelli, S.; Williams, J.M.G.; Kuyken, W. What defines mindfulness-based programs? The warp and the weft. Psychol. Med. 2017, 47, 990–999. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Asmundson, G.J. Acceptance and mindfulness-based therapy: New wave or old hat? Clin. Psychol. Rev. 2008, 28, 1–16. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen. Hosp. Psychiat. 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Ritter, A.; Alvarez, I. Mindfulness and Executive Functions: Making the Case for Elementary School Practice. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 544–553. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness; Piatkus: London, UK, 1996. [Google Scholar]
- Segal, Z.V.; Teasdale, J.D.; Williams, J.M.; Gemar, M.C. The mindfulness-based cognitive therapy adherence scale: Inter-rater reliability, adherence to protocol and treatment distinctiveness. Clin. Psychol. Psychot. 2002, 9, 131–138. [Google Scholar] [CrossRef]
- Roemer, L.; Orsillo, S.M. Mindfulness- and Acceptance-Based Behavioral Therapies in Practice; Guilford Press: New York, NY, USA, 2009. [Google Scholar] [CrossRef]
- Germer, C.K.; Neff, K.D. Self-compassion in clinical practice. J. Clin. Psychol. 2013, 69, 856–867. [Google Scholar] [CrossRef]
- Perestelo-Perez, L.; Barraca, J.; Peñate, W.; Rivero-Santana, A.; Alvarez-Perez, Y. Mindfulness-based interventions for the treatment of depressive rumination: Systematic review and meta-analysis. Int. J. Clin. Health Psychol. 2017, 17, 282–295. [Google Scholar] [CrossRef]
- Gotink, R.A.; Chu, P.; Busschbach, J.J.; Benson, H.; Fricchione, G.L.; Hunink, M.M. Standardised mindfulness-based interventions in healthcare: An overview of systematic reviews and meta-analyses of RCTs. PLoS ONE 2015, 10, e0124344. [Google Scholar] [CrossRef] [PubMed]
- Strauss, C.; Cavanagh, K.; Oliver, A.; Pettman, D. Mindfulness-based interventions for people diagnosed with a current episode of an anxiety or depressive disorder: A meta-analysis of randomised controlled trials. PLoS ONE. 2014, 9, e96110. [Google Scholar] [CrossRef]
- Piet, J.; Hougaard, E. The effect of mindfulness-based cognitive therapy for prevention of relapse in recurrent major depressive disorder: A systematic review and meta-analysis. Clin. Psychol. Rev. 2011, 31, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Veehof, M.M.; Oskam, M.J.; Schreurs, K.M.; Bohlmeijer, E.T. Acceptance-based interventions for the treatment of chronic pain: A systematic review and meta-analysis. Pain 2011, 152, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Roche, A.I.; Kroska, E.B.; Denburg, N.L. Acceptance-and mindfulness-based interventions for health behavior change: Systematic reviews and meta-analyses. J. Contextual Behav. Sci. 2019, 13, 74–93. [Google Scholar] [CrossRef]
- Kreplin, U.; Farias, M.; Brazil, I.A. The limited prosocial effects of meditation: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 2403. [Google Scholar] [CrossRef] [PubMed]
- Cebolla, A.; Demarzo, M.; Martins, P.; Soler, J.; Garcia-Campayo, J. Unwanted effects: Is there a negative side of meditation? A multicentre survey. PLoS ONE 2017, 12, e0183137. [Google Scholar] [CrossRef]
- Regehr, C.; Glancy, D.; Pitts, A. Interventions to reduce stress in university students: A review and meta-analysis. J. Affect. Disorders 2013, 148, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Halladay, J.E.; Dawdy, J.L.; McNamara, I.F.; Chen, A.J.; Vitoroulis, I.; McInnes, N.; Munn, C. Mindfulness for the Mental Health and Well-Being of Post-Secondary Students: A Systematic Review and Meta-Analysis. Mindfulness 2019, 10, 397–414. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Tucker, R.P.; Greene, P.A.; Davidson, R.J.; Wampold, B.E.; Kearney, D.J.; Simpson, T.L. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2018, 59, 52–60. [Google Scholar] [CrossRef]
- Chiesa, A.; Serretti, A. Mindfulness based cognitive therapy for psychiatric disorders: A systematic review and meta-analysis. Psychiat. Res. 2011, 187, 441–453. [Google Scholar] [CrossRef]
- Khoury, B.; Lecomte, T.; Fortin, G.; Masse, M.; Therien, P.; Bouchard, V.; Chapleau, M.A.; Paquin, K.; Hofmann, S.G. Mindfulness-based therapy: A comprehensive meta-analysis. Clin. Psychol. Rev. 2013, 33, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Singh, S.; Sibinga, E.M.; Gould, N.F.; Rowland-Seymour, A.; Sharma, R.; Berger, Z.; Sleicher, D.; Maron, D.D.; Shihab, H.M.; et al. Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.G.; Pérez-Fuentes, M.C.; Molero, M.M.; Tortosa, B.M.; González, A. Beneficios de las intervenciones psicológicas en relación al estrés y ansiedad: Revisión sistemática y metaanálisis. Eur. J. Investig. Health Psychol. Educ. 2019, 12, 191–206. [Google Scholar] [CrossRef]
- Baer, R.A. Mindfulness training as a clinical intervention: A conceptual and empirical review. Clin. Psychol. Sci. Pract. 2003, 10, 125–143. [Google Scholar] [CrossRef]
- Kabat-Zinn, J.; Maisson, A.O.; Kristeller, J.; Gay Peterson, L.; Fletcher, K.E.; Pbert, L.; Lenderking, W.R.; Santorelli, S.F. Effectiveness of a Meditation Based Stress Reduction program in the treatment of anxiety disorders. Am. J. Psychiatry 1992, 149, 936–943. [Google Scholar] [CrossRef]
- Miller, J.J.; Fletcher, K.; Kabat-Zinn, J. Three-year follow-up and clinical implications of a mindfulness meditation-based stress reduction intervention in the treatment of anxiety disorders. Gen. Hosp. Psychiatry 1995, 17, 192–200. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [Google Scholar] [CrossRef]
- Vøllestad, J.; Nielsen, M.B.; Nielsen, G.H. Mindfulness and acceptance based interventions for anxiety disorders: A systematic review and meta-analysis. Brit. J. Clin. Psychol. 2012, 51, 239–260. [Google Scholar] [CrossRef]
- Galante, J.; Iribarren, S.J.; Pearce, P.F. Effects of mindfulness-based cognitive therapy on mental disorders: A systematic review and meta-analysis of randomised controlled trials. J. Res. Nurs. 2013, 18, 133–155. [Google Scholar] [CrossRef]
- Hodann-Caudevilla, R.M.; Serrano-Pintado, I. Revisión sistemática de la eficacia de los tratamientos basados en mindfulness para los trastornos de ansiedad [Systematic review of the efficacy of mindfulness-based therapy for anxiety disorders]. Ansiedad Estrés 2016, 22, 39–45. [Google Scholar] [CrossRef]
- Kishita, N.; Takei, Y.; Stewart, I. A meta-analysis of third wave mindfulness-based cognitive behavioral therapies for older people. Int. J. Geriatr. Psych. 2017, 32, 1352–1361. [Google Scholar] [CrossRef]
- Spijkerman, M.P.J.; Pots, W.T.M.; Bohlmeijer, E.T. Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin. Psychol. Rev. 2016, 45, 102–114. [Google Scholar] [CrossRef]
- Singh, S.K.; Gorey, K.M. Relative effectiveness of mindfulness and cognitive behavioral interventions for anxiety disorders: Meta-analytic review. Soc. Work Ment. Health. 2018, 16, 238–251. [Google Scholar] [CrossRef]
- Abreu-Costa, M.; de Oliveira, G.S.D.A.; Tatton-Ramos, T.; Manfro, G.G.; Salum, G.A. Anxiety and Stress-Related Disorders and Mindfulness-Based Interventions: A systematic review and multilevel Meta-analysis and Meta-regression of multiple outcomes. Mindfulness 2019, 10, 996–1005. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epid. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Hamel, C.; Wells, G.A.; Bouter, L.M.; Kristjansson, E.; Grimshaw, J.; Henry, D.A.; Boers, M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J. Clin. Epid. 2009, 62, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.W.; Berger, C.C.; Manheimer, E.; Forde, D.; Magidson, J.; Dachman, L.; Lejuez, C.W. Meditative therapies for reducing anxiety: A systematic review and meta-analysis of randomized controlled trials. Depress. Anxiety 2012, 29, 545–562. [Google Scholar] [CrossRef] [PubMed]
- Carsley, D.; Khoury, B.; Heath, N.L. Effectiveness of mindfulness Interventions for mental health in schools: A comprehensive meta-analysis. Mindfulness 2018, 9, 693–707. [Google Scholar] [CrossRef]
- Norton, A.R.; Abbott, M.J.; Norberg, M.M.; Hunt, C. A systematic review of mindfulness and acceptance-based treatments for social anxiety disorder. J. Clin. Psychol. 2015, 71, 283–301. [Google Scholar] [CrossRef]
- Pulido-Acosta, F.; Herrera-Clavero, F. Anxiety and happiness as opposite emotional states in childhood. Eur. J. Investig. Health Psychol. Educ. 2018, 8, 65–77. [Google Scholar] [CrossRef]
- Pagnini, F.; Cavalera, C.; Rovaris, M.; Mendozzi, L.; Molinari, E.; Phillips, D.; Langerb, E. Longitudinal associations between mindfulness and well-being in people with multiple sclerosis. Int. J. Clin. Health. Psychol. 2019, 19, 22–30. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| First Author and Year | Studies Included | Target Population | Implemented Intervention | Comparison Group | Effect Size | Main Results |
|---|---|---|---|---|---|---|
| [26] | 21 uncontrolled and controlled studies, but only two were based on anxiety disorder | Anxiety clinical sample | MBSR | None | d = 0.70 | Kabat-Zinn et al. [27] examined patients with generalized anxiety and panic disorders and found significant improvements (also at 3-month follow-up). Miller, Fletcher, and Kabat-Zinn [28] reported a 3-year follow-up of the same participants and results were maintained. |
| [29] | 39 uncontrolled and controlled studies | Anxiety clinical sample | MBSR or MBCT | None, TAU, educational social support with relaxation, anxiety education program, waiting list | For anxiety disorders, ES estimates suggest that mindfulness-based therapy was moderately effective for improving anxiety (Hedges’ g = 0.63; 95% CI = 0.47 to 0.87) from pre- to post-treatment in the overall sample | The uncontrolled pre-post ES estimates were in the moderate range for reducing anxiety symptoms. MBT in patients with anxiety disorders was associated with a large ES. |
| [30] | 19 controlled and uncontrolled trials | Individuals with clinical levels of anxiety | Multi-component acceptance-based interventions (CBT) | Stand-alone mindfulness | Between groups Hedges’ g = −0.83; 95% CI = −1.62 to −0.04 | MBIs are associated with robust and substantial reductions in symptoms of anxiety. No significant differences emerged between stand-alone mindfulness interventions and multi-component treatment packages. |
| [31] | 11 randomized controlled trials | Patients diagnosed with anxiety disorders | MBCT | TAU | The average degree of anxiety decreased compared to TAU (Hedges’ g = −0.42; 95% CI = −0.74 to −0.09) | Anxiety obtained significant but unstable results in sensitivity analyses comparing additive MBCT against usual treatment. |
| [23] | 209 waiting list-controlled studies but only 32 focused on anxiety | Medical conditions and non-clinical population with elevated initial anxiety | MBI | Pre-post studies, waiting list controlled and psycho-educational interventions, supportive therapies, relaxation and imagery/suppression technique | The SMD was large (10 studies pre-post) for anxiety studies (Hedges’ g = 0.89; 95% CI = 0.71 to 1.08) and for 4 waitlist-controlled studies (Hedges’ g = 0.96 (95% CI = 0.67 to 1.24) | MBT is moderately effective in pre-post comparisons, in comparisons with waitlist controls and when compared with other active treatments, including other psychological treatments. MBT did not differ from traditional CBT or behavioral therapies or pharmacological treatment. MBT was associated with the largest mean ES for anxiety. |
| [13] | 12 randomized controlled trials; 9 included a measure of anxiety symptoms | Full diagnostic criteria for anxiety | MBCT, MBSR and person-based cognitive therapy | Active control conditions (psychoeducation) and inactive control conditions (waiting list, aerobic exercise) | There was a non-significant post-MBI between-group difference in anxiety symptom severity (Hedges’ g = −0.52; 95% CI = −1.11 to 0.06). MBCT vs. inactive control (Hedges’ g = −1.03; 95% CI = −0.40 to −1.66). MBCT vs. active control (Hedges’ g = 0.03; 95% CI = 0.54 to −0.48). | There were no significant post-intervention between-group benefits of MBIs relative to inactive control conditions on anxiety symptom severity nor was there was an active control. |
| [32] | 8 randomized and non-randomized clinical trials | Anxiety clinical sample | ACT, MBCT, MBSR | Waiting list, TAU, psychoeducation, CBT, aerobic exercises, relaxation | It was suggested that psychological interventions based on mindfulness constitute an effective treatment for GAD (from d = 0.92 to d = 3.4), SP (from d = 0.41 to d = 0.78), and PTSD (d = 0.63) when used as adjuncts to pharmacological treatment | The interventions based on mindfulness constitute an effective treatment for GAD, SP, and PTSD, when used as adjuncts to pharmacological treatment. However, an ES that combines the significant differences obtained for each of the disorders is not provided. For the comparison between treatments based on mindfulness and other treatments for anxiety (CBT, applied relaxation, and aerobic exercise), it is suggested that the former is not superior to the latter in terms of efficacy. Both MBSR and MBCT seem highly efficient interventions. |
| [33] | 7 randomized controlled trials (RCTs) | Anxiety symptoms with a wide range of physical and psychological conditions | MCBT and ACT | Pre-post studies, control and active control groups | ES varied from not effective (Hedges’ g = 0.23) to large and positive (Hedges’ g = 1.90). The random effect model showed an overall moderate ES (Hedges’ g = 0.58; 95% CI = 0.27 to 0.88) of mindfulness-based CBT for anxiety symptoms among older adults | Effect-size estimates suggest that mindfulness-based CBT is moderately effective on anxiety symptoms in older adults (g = 0.58) |
| [34] | 15 RCTs, 11 comparisons on anxiety | Anxiety clinical sample | ACT, MBCT, MBSR, Internet-based Mindfulness treatment | Control group | Based on 11 comparisons, a significant, small ES was found for online MBIs on anxiety, with g = 0.22 (95% CI = 0.05 to 0.39, p = 0.010) and no outliers. After removal of low-quality studies from the analysis, the ES was virtually the same (g = 0.21, 95% CI = 0.03 to 0.40, p = 0.022). | A small but significant ES was found on anxiety. The online MBIs are not as effective as traditional face-to-face MBIs in reducing anxiety. |
| [21] | 142 randomized clinical trials (18 based on anxiety disorders) | Anxiety clinical sample | MBI | No treatment, specific active control, evidence-based treatment | For anxiety, MBIs were equivalent to the comparison group (d = 0.15 (95% CI = −0.16 to 0.46) and were equivalent to EBTs (d = −0.18 (95% CI = −0.41 to 0.06) | Mindfulness-based interventions were equivalent to the comparison group and EBTs for anxiety |
| [35] | 9 randomized trials | Anxiety clinical sample | MBI | CBT (active control groups) | Between groups Cohen’s d = −0.02; 95% CI = −0.16 to 0.12 | No statistically or practically significant differences between mindfulness and cognitive behavioral intervention |
| [36] | 10 randomized controlled trials | Anxiety clinical sample | MBCT and MBSR | Control conditions, CBT | MBIs were superior to control interventions for internalizing (SE = 0.26; 95% CI = 0.64 to 0.12; p = 0.00) and distress (SE = 0.12; 95% CI = 0.7 to 0.21; p = 0.00), but not for fear symptoms (SE = 0.22; 95% CI = 0.45 to 0.4; p = 0.90). A significant difference that favor CBT over MBIs for the fear domain symptoms were found (SE = 0.1; 95% CI = 0.1 to 0.46; p = 0.00). No evidence for superiority of CBT over MBIs was found. | MBIs were superior to control interventions for internalizing and distress, but not for fear symptoms. CBT was superior to MBIs for fear symptoms but not for internalizing and distress. |
| AMSTAR Items | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| First Author and Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total YES |
| [26] | YES | NO | YES | NO | NO | YES | NO | NO A | YES | NO | C N A | 4 |
| [29] | YES | YES | YES | NO | NO | YES | YES | YES | YES | NO | YES | 8 |
| [30] | YES | YES | YES | NO | NO | YES | NO | NO A | YES | YES | C N A | 6 |
| [31] | YES | YES | YES | NO | NO | YES | NO A | NO A | YES | YES | YES | 7 |
| [23] | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | YES | 9 |
| [13] | YES | C N A | YES | YES | NO | YES | YES | C N A | YES | YES | C N A | 7 |
| [32] | YES | C N A | YES | NO | NO | YES | NO | NO A | N A | NO | YES | 4 |
| [33] | YES | YES | YES | YES | NO | YES | C N A | YES | YES | YES | YES | 9 |
| [34] | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | C N A | 8 |
| [21] | YES | YES | YES | YES | NO | YES | YES | YES | YES | NO | YES | 9 |
| [35] | YES | C N A | YES | NO | NO | YES | NO | N A | YES | YES | C N A | 5 |
| [36] | YES | YES | YES | NO | NO | YES | YES | YES | YES | YES | YES | 9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fumero, A.; Peñate, W.; Oyanadel, C.; Porter, B. The Effectiveness of Mindfulness-Based Interventions on Anxiety Disorders. A Systematic Meta-Review. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 704-719. https://doi.org/10.3390/ejihpe10030052
Fumero A, Peñate W, Oyanadel C, Porter B. The Effectiveness of Mindfulness-Based Interventions on Anxiety Disorders. A Systematic Meta-Review. European Journal of Investigation in Health, Psychology and Education. 2020; 10(3):704-719. https://doi.org/10.3390/ejihpe10030052
Chicago/Turabian StyleFumero, Ascensión, Wenceslao Peñate, Cristián Oyanadel, and Bárbara Porter. 2020. "The Effectiveness of Mindfulness-Based Interventions on Anxiety Disorders. A Systematic Meta-Review" European Journal of Investigation in Health, Psychology and Education 10, no. 3: 704-719. https://doi.org/10.3390/ejihpe10030052
APA StyleFumero, A., Peñate, W., Oyanadel, C., & Porter, B. (2020). The Effectiveness of Mindfulness-Based Interventions on Anxiety Disorders. A Systematic Meta-Review. European Journal of Investigation in Health, Psychology and Education, 10(3), 704-719. https://doi.org/10.3390/ejihpe10030052