Application of an In Vitro Psoriatic Skin Model to Study Cutaneous Metabolization of Tazarotene



 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Cell Culture Media
2.3. Cell Culture
2.4. Production of Tissue-Engineered Substitutes
2.5. Histological Analyses
2.6. Immunofluorescence Analyses
2.7. Percutaneous Absorption
2.8. Statistical Analyses
3. Results
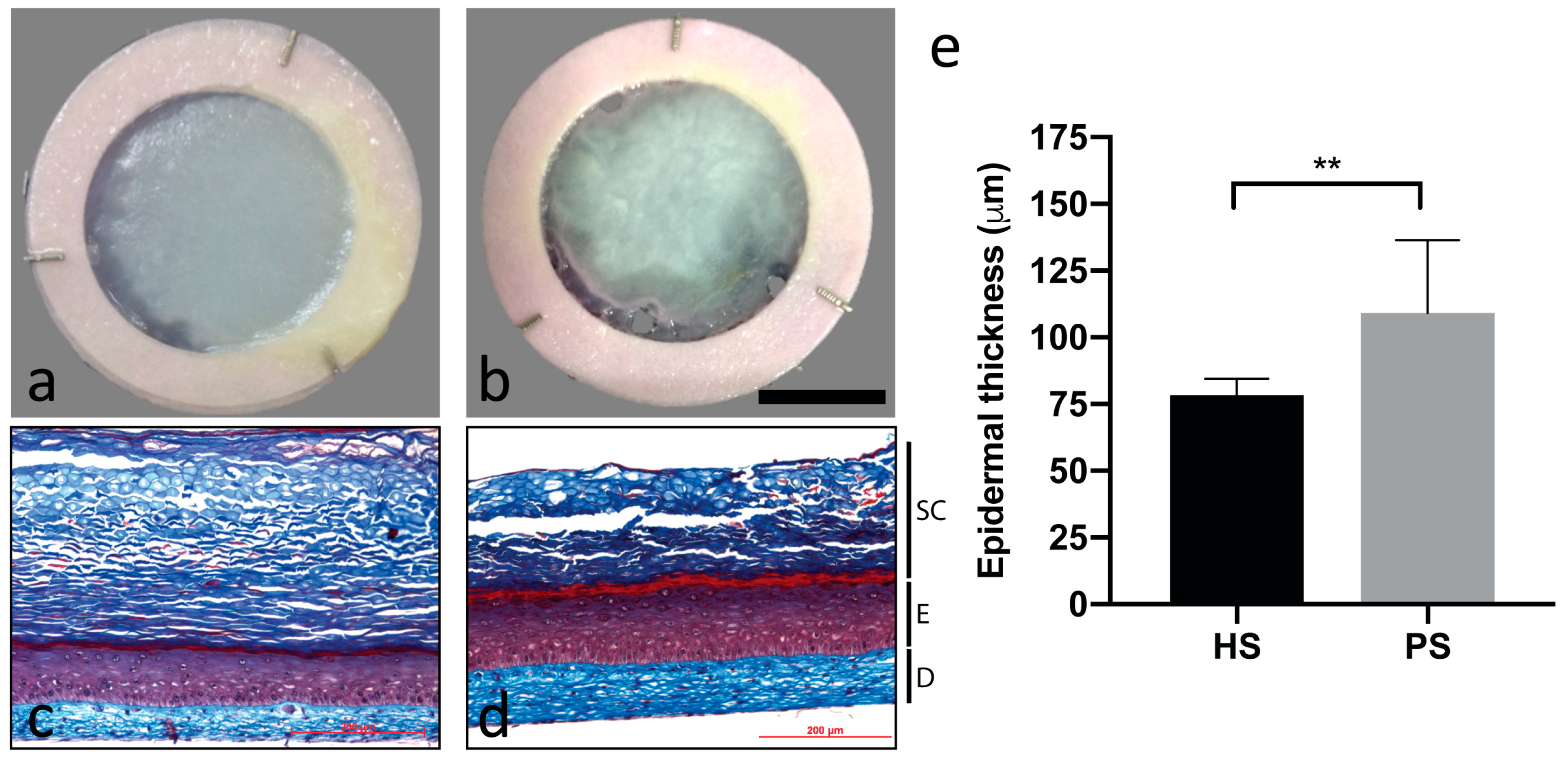
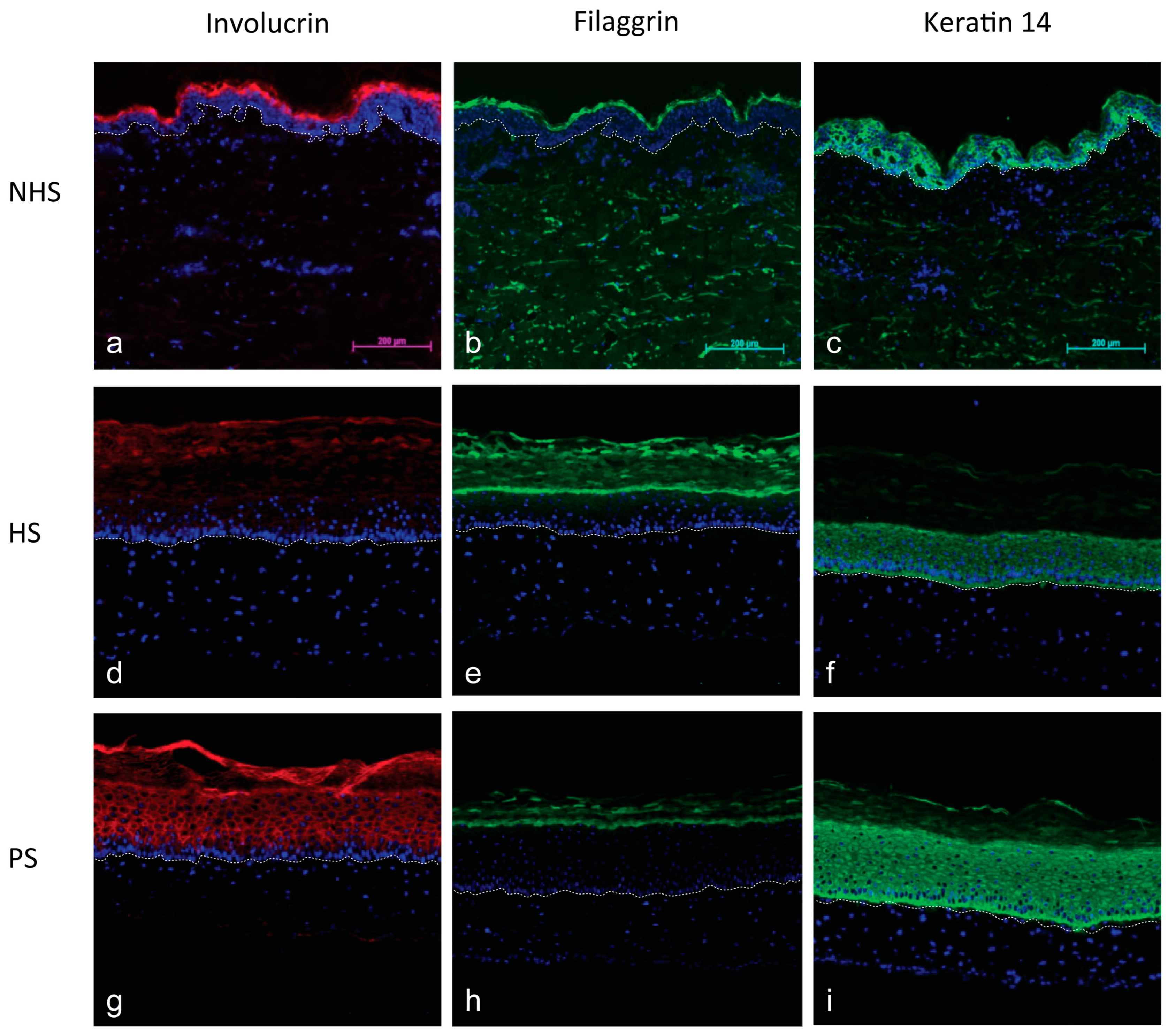
3.1. Morphology of the Psoriatic Skin Substitutes Produced by Tissue Engineering
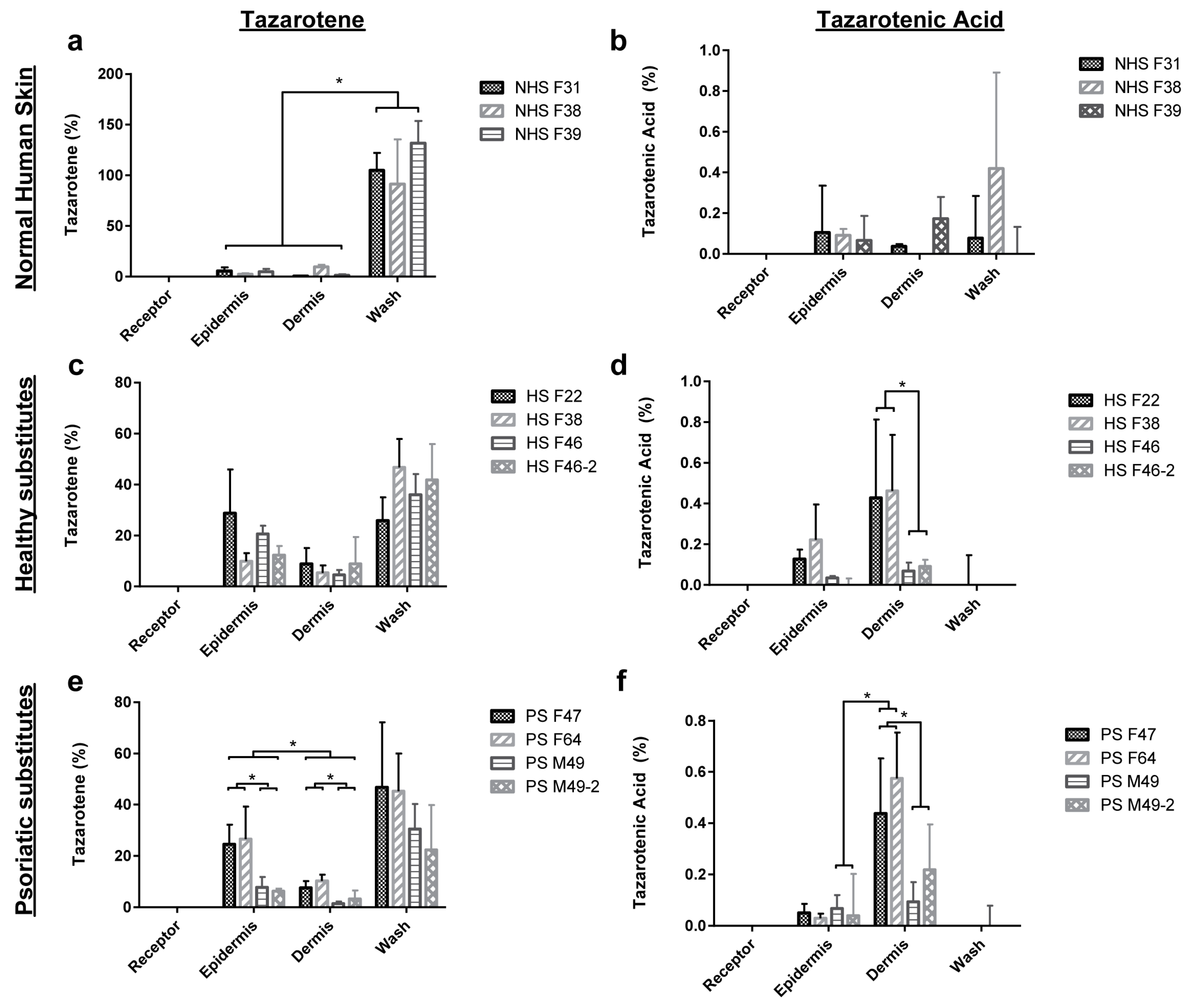
3.2. Percutaneous Absorption of Tazarotene
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Raychaudhuri, S.; Farber, E. The prevalence of psoriasis in the world. J. Eur. Acad. Dermatol. Venereol. 2001, 15, 16–17. [Google Scholar] [CrossRef] [PubMed]
- Freinkel, R.K.; Woodley, D.T. The Biology of the Skin; CRC Press: Boca Raton, FL, USA, 2001. [Google Scholar]
- Guilhou, J.-J. Pathogénie du psoriasis. Med. Sci. 1993, 9, 412–416. [Google Scholar] [CrossRef]
- Braun-Falco, O. The initial psoriatic lesion. In Proceedings of the Second International Symposium, Stanford, CA, USA, 12–15 July 1976; pp. 1–11. [Google Scholar]
- Rongioletti, F.; Fiorucci, C.; Parodi, A. Psoriasis induced or aggravated by drugs. J. Rheumatol. 2009, 83, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Lowes, M.A.; Bowcock, A.M.; Krueger, J.G. Pathogenesis and therapy of psoriasis. Nature 2007, 445, 866–873. [Google Scholar] [CrossRef]
- Lowes, M.A.; Suarez-Farinas, M.; Krueger, J.G. Immunology of psoriasis. Annu. Rev. Immunol. 2014, 32, 227–255. [Google Scholar] [CrossRef]
- Duvic, M.; Nagpal, S.; Asano, A.T.; Chandraratna, R.A. Molecular mechanisms of tazarotene action in psoriasis. J. Am. Acad. Dermatol. 1997, 37, S18–S24. [Google Scholar] [CrossRef]
- Wickett, R.R.; Visscher, M.O. Structure and function of the epidermal barrier. Am. J. Infect. Control 2006, 34, S98–S110. [Google Scholar] [CrossRef]
- Nicolas, J.-F.; Thivolet, J. Psoriasis: De la Clinique à la Thérapeutique; John Libbey Eurotext: Montrouge, France, 1997; p. 241. [Google Scholar]
- Lebwohl, M.G.; Bachelez, H.; Barker, J.; Girolomoni, G.; Kavanaugh, A.; Langley, R.G.; Paul, C.F.; Puig, L.; Reich, K.; van de Kerkhof, P.C. Patient perspectives in the management of psoriasis: Results from the population-based Multinational Assessment of Psoriasis and Psoriatic Arthritis Survey. J. Am. Acad. Dermatol. 2014, 70, 871–881. [Google Scholar] [CrossRef]
- Chandra, A.; Ray, A.; Senapati, S.; Chatterjee, R. Genetic and epigenetic basis of psoriasis pathogenesis. Mol. Immunol. 2015, 64, 313–323. [Google Scholar] [CrossRef]
- Gollnick, H.; Menter, A. Combination therapy with tazarotene plus a topical corticosteroid for the treatment of plaque psoriasis. Br. J. Dermatol. Suppl. 1999, 140, 18–23. [Google Scholar] [CrossRef]
- Tanghetti, E.; Lebwohl, M.; Stein Gold, L. Tazarotene Revisited: Safety and Efficacy in Plaque Psoriasis and Its Emerging Role in Treatment Strategy. J. Drugs Dermatol. 2018, 17, 1280–1287. [Google Scholar] [PubMed]
- Barker, C.L.; Clothier, R.H. Human keratinocyte cultures as models of cutaneous esterase activity. Toxicol. In Vitro Int. J. Publ. Assoc. Bibra 1997, 11, 637–640. [Google Scholar] [CrossRef]
- Kamili, Q.U.; Menter, A. Topical treatment of psoriasis. Curr. Probl. Dermatol. 2009, 38, 37–58. [Google Scholar] [CrossRef] [PubMed]
- Talpur, R.; Cox, K.; Duvic, M. Efficacy and safety of topical tazarotene: A review. Expert Opin. Drug Metab. Toxicol. 2009, 5, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, S.; Patel, S.; Asano, A.T.; Johnson, A.T.; Duvic, M.; Chandraratna, R.A.S. Tazarotene-Induced Gene 1 (TIG1), a Novel Retinoic Acid Receptor-Responsive Gene in Skin. J. Investig. Derm. 1996, 106, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Chandraratna, R.A.S. Tazarotene: The first receptor-selective topical retinoid for the treatment of psoriasis. J. Am. Acad. Dermatol. 1997, 37, S12–S17. [Google Scholar] [CrossRef]
- Germain, L.; Rouabhia, M.; Guignard, R.; Carrier, L.; Bouvard, V.; Auger, F. Improvement of human keratinocyte isolation and culture using thermolysin. Burns 1993, 19, 99–104. [Google Scholar] [CrossRef]
- Auger, F.A.; Valle, C.A.L.; Guignard, R.; Tremblay, N.; Noel, B.; Goulet, F.; Germain, L. Skin equivalent produced with human collagen. In Vitro Cell. Dev. Biol. Anim. 1995, 31, 432–439. [Google Scholar] [CrossRef]
- Franz, T.J. Percutaneous absorption on the relevance of in vitro data. J. Investig. Dermatol. 1975, 64, 190–195. [Google Scholar] [CrossRef]
- Simard, M.; Julien, P.; Fradette, J.; Pouliot, R. Modulation of the Lipid Profile of Reconstructed Skin Substitutes after Essential Fatty Acid Supplementation Affects Testosterone Permeability. Cells 2019, 8. [Google Scholar] [CrossRef]
- Iizuka, H.; Ishida-Yamamoto, A.; Honda, H. Epidermal remodelling in psoriasis. Br. J. Dermatol. 1996, 135, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Mils, V.; Basset-Séguin, N.; Molès, J.-P.; Tesnière, A.; Leigh, I.; Guilhou, J.-J. Comparative analysis of normal and psoriatic skin both in vivo and in vitro. Differentiation 1994, 58, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Stoler, A.; Kopan, R.; Duvic, M.; Fuchs, E. Use of monospecific antisera and cRNA probes to localize the major changes in keratin expression during normal and abnormal epidermal differentiation. J. Cell Biol. 1988, 107, 427–446. [Google Scholar] [CrossRef] [PubMed]
- Van de Kerkhof, P.C. Textbook of Psoriasis, 2nd ed.; Wiley: Hoboken, NJ, USA, 2003. [Google Scholar]
- Thewes, M.; Stadler, R.; Korge, B.; Mischke, D. Normal psoriatic epidermis expression of hyperproliferation-associated keratins. Arch Derm. Res 1991, 283, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, R.; Jagannatha, R.K.; Basavaraj, K.H. A comprehensive review on biomarkers in psoriasis. Clin. Exp. Dermatol. 2009, 34, 658–663. [Google Scholar]
- McKay, I.A.; Leigh, I.M. Altered keratinocyte growth and differentiation in psoriasis. Clin. Dermatol. 1995, 13, 105–114. [Google Scholar] [CrossRef]
- Niehues, H.; van den Bogaard, E.H. Past, present and future of in vitro 3D reconstructed inflammatory skin models to study psoriasis. Exp. Dermatol. 2018, 27, 512–519. [Google Scholar] [CrossRef]
- Rioux, G.; Pouliot-Berube, C.; Simard, M.; Benhassine, M.; Soucy, J.; Guerin, S.L.; Pouliot, R. The Tissue-Engineered Human Psoriatic Skin Substitute: A Valuable In Vitro Model to Identify Genes with Altered Expression in Lesional Psoriasis. Int. J. Mol. Sci. 2018, 19. [Google Scholar] [CrossRef]
- Khan, G.M.; Frum, Y.; Sarheed, O.; Eccleston, G.M.; Meidan, V.M. Assessment of drug permeability distributions in two different model skins. Int. J. Pharm. 2005, 303, 81–87. [Google Scholar] [CrossRef]
- Lombardi Borgia, S.; Schlupp, P.; Mehnert, W.; Schafer-Korting, M. In vitro skin absorption and drug release—A comparison of six commercial prednicarbate preparations for topical use. Eur. J. Pharm. Biopharm. 2008, 68, 380–389. [Google Scholar] [CrossRef]
- Alonso, C.; Carrer, V.; Espinosa, S.; Zanuy, M.; Cordoba, M.; Vidal, B.; Dominguez, M.; Godessart, N.; Coderch, L.; Pont, M. Prediction of the skin permeability of topical drugs using in silico and in vitro models. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2019, 136, 104945. [Google Scholar] [CrossRef] [PubMed]
- Supp, D.M.; Boyce, S.T. Engineered skin substitutes: Practices and potentials. Clin. Dermatol. 2005, 23, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.-H.; Fang, J.-Y. Drug delivery and formulations for the topical treatment of psoriasis. Expert Opin. Drug Deliv. 2008, 5, 235–249. [Google Scholar] [CrossRef] [PubMed]
- Diane, D.-S.; Matsumoto, R.M.; Usansky, J.I. Clinical pharmacokinetics and drug metabolism of tazarotene. Clin. Pharmacokinet. 1999, 37, 273–287. [Google Scholar]
- Li, L.; Zhang, M.; Ma, P.; Qian, K. Development of a simple method for simultaneous determination of tazarotene and betamethasone dipropionate and their metabolites using LC-MS method and its application to dermatopharmacokinetic study. Biomed. Chromatogr. 2019, 33, e4557. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, P.G.; Perkins, J.; Hotchkiss, S.A.M. Metabolism of Fluroxypyr, Fluroxypyr Methyl Ester, and the Herbicide Fluroxypyr Methylheptyl Ester. I: During Percutaneous Absorption through Fresh Rat and Human Skin In Vitro. Drug Metab. Dispos. 2000, 28, 748–754. [Google Scholar]
- Sondell, B.; Thornell, L.-E.; Egelrud, T. Evidence That Stratum Corneum Chymotryptic Enzyme Is Transported to the Stratum Corneum Extracellular Space Via Lamellar Bodies. J. Investig. Dermatol. 1995, 104, 819–823. [Google Scholar] [CrossRef]
- Beisson, F.; Aoubala, M.; Marull, S.; Moustacas-Gardies, A.-M.; Voultoury, R.; Verger, R.; Arondel, V. Use of the Tape Stripping Technique for Directly Quantifying Esterase Activities in Human Stratum Corneum. Anal. Biochem. 2001, 290, 179–185. [Google Scholar] [CrossRef]
- Oesch, F.; Fabian, E.; Guth, K.; Landsiedel, R. Xenobiotic-metabolizing enzymes in the skin of rat, mouse, pig, guinea pig, man, and in human skin models. Arch. Toxicol. 2014, 88, 2135–2190. [Google Scholar] [CrossRef]
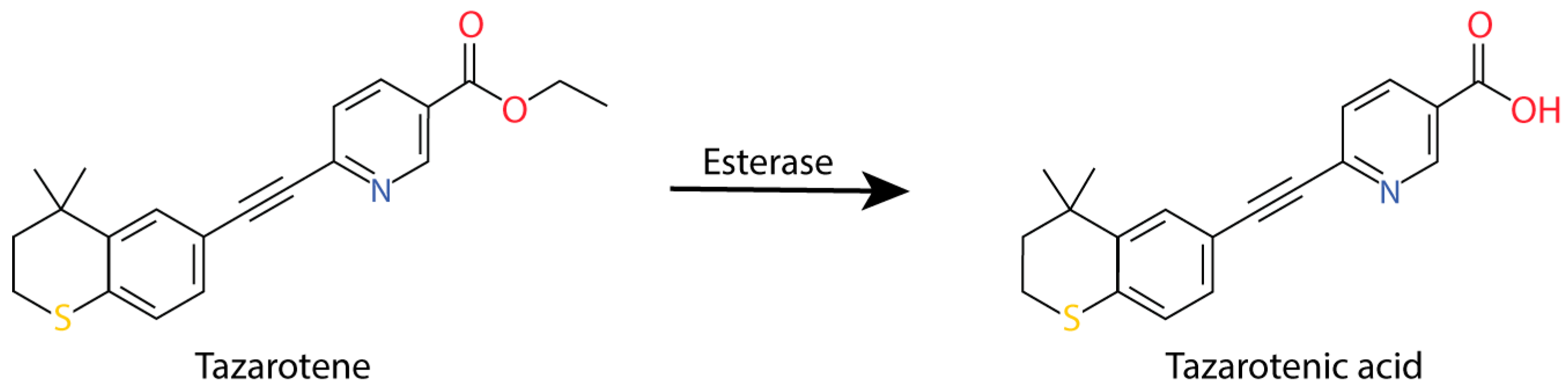
- Madhu, C.; Duff, S.; Baumgarten, V.; Rix, P.; Small, D.; Tang-Liu, D. Metabolic deesterification of tazarotene in human blood and rat and human liver microsomes. J. Pharm. Sci. 1997, 86, 972–974. [Google Scholar] [CrossRef]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morin, A.; Simard, M.; Rioux, G.; Grenier, A.; Morin, S.; Pouliot, R. Application of an In Vitro Psoriatic Skin Model to Study Cutaneous Metabolization of Tazarotene. Processes 2019, 7, 871. https://doi.org/10.3390/pr7120871
Morin A, Simard M, Rioux G, Grenier A, Morin S, Pouliot R. Application of an In Vitro Psoriatic Skin Model to Study Cutaneous Metabolization of Tazarotene. Processes. 2019; 7(12):871. https://doi.org/10.3390/pr7120871
Chicago/Turabian StyleMorin, Alexandre, Mélissa Simard, Geneviève Rioux, Alexe Grenier, Sophie Morin, and Roxane Pouliot. 2019. "Application of an In Vitro Psoriatic Skin Model to Study Cutaneous Metabolization of Tazarotene" Processes 7, no. 12: 871. https://doi.org/10.3390/pr7120871
APA StyleMorin, A., Simard, M., Rioux, G., Grenier, A., Morin, S., & Pouliot, R. (2019). Application of an In Vitro Psoriatic Skin Model to Study Cutaneous Metabolization of Tazarotene. Processes, 7(12), 871. https://doi.org/10.3390/pr7120871