
Does a Gluten-Free Diet Affect BMI and Glycosylated Hemoglobin in Children and Adolescents with Type 1 Diabetes and Asymptomatic Celiac Disease? A Meta-Analysis and Systematic Review

 ,
,  , , and
, , and
Abstract
1. Introduction
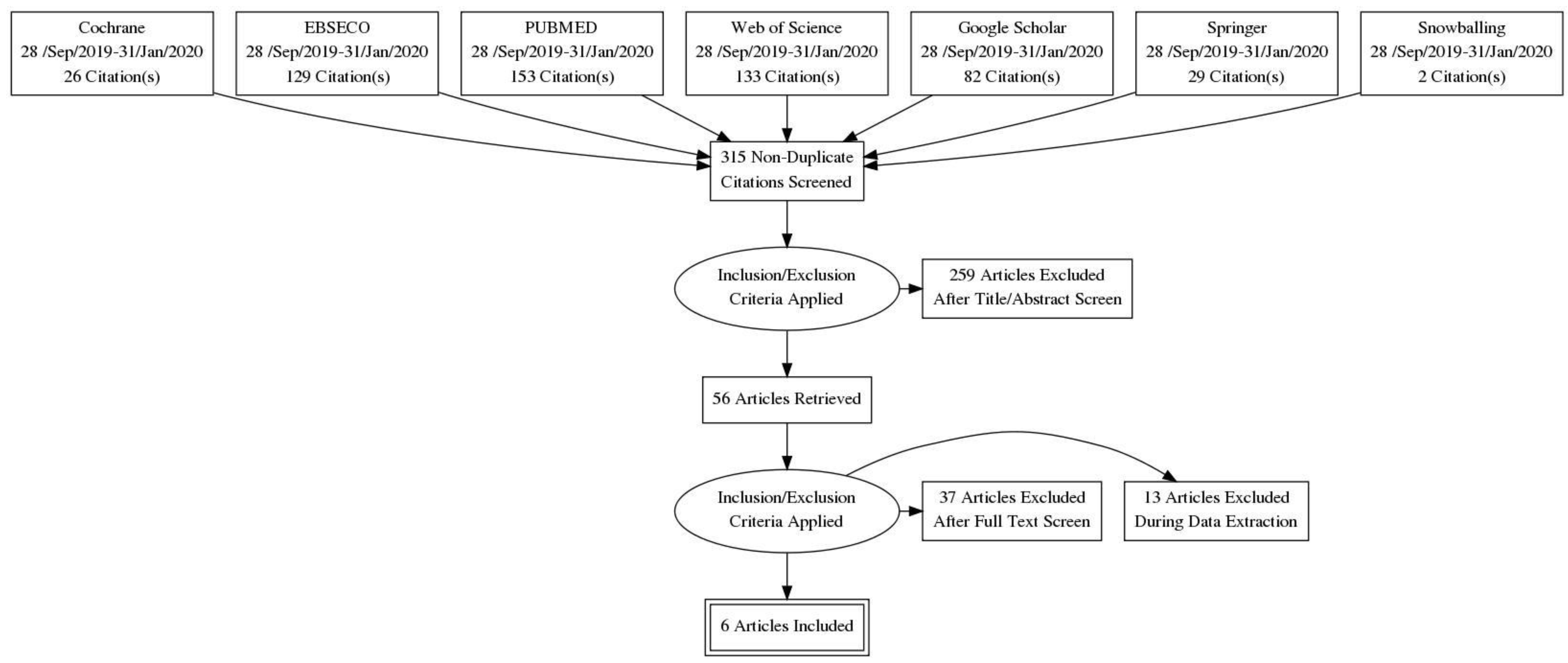
2. Materials and Methods
3. Statistical Analysis
4. Results
4.1. Characteristics of Included Studies
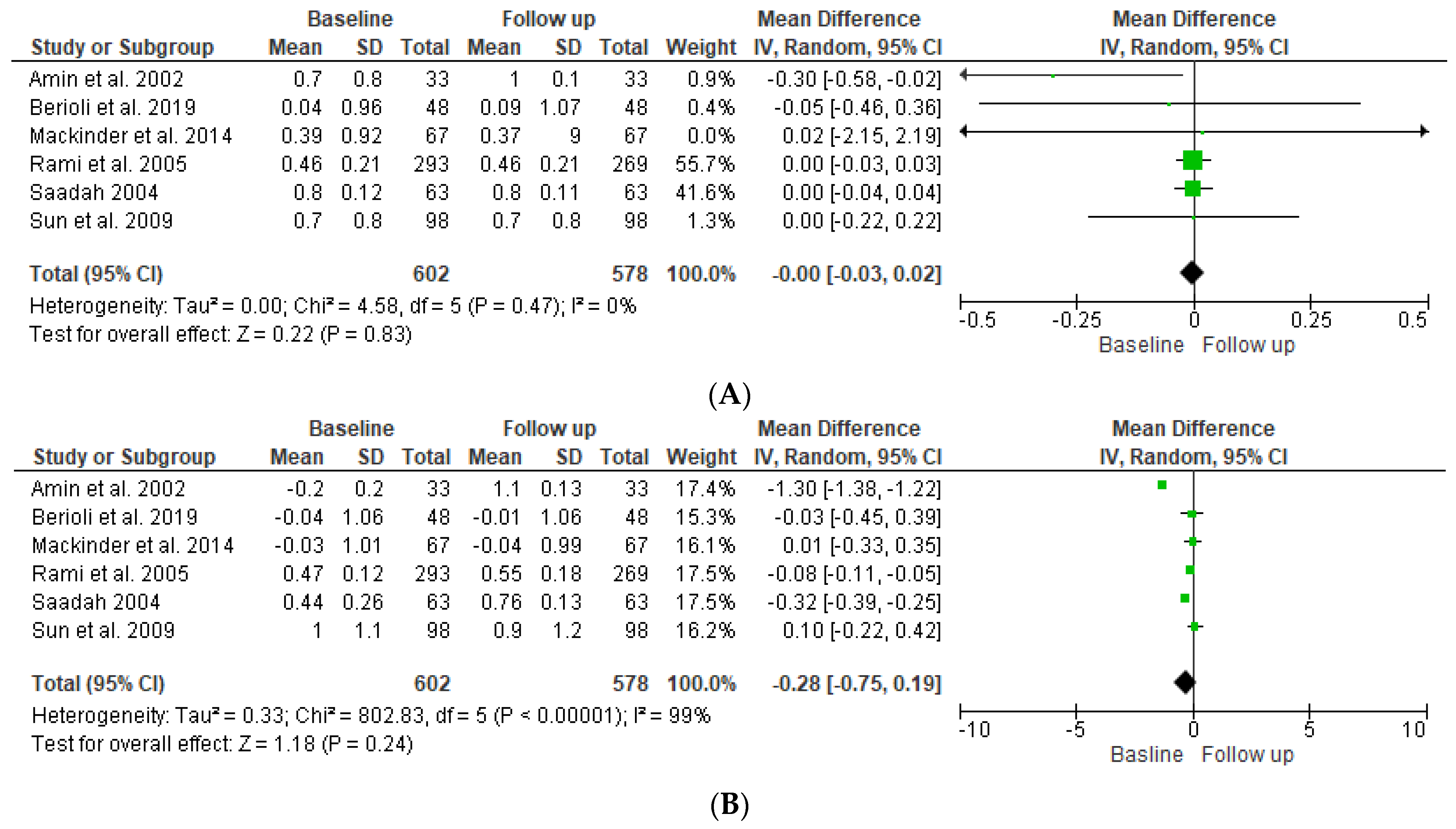
4.2. Body Mass Index—SDS
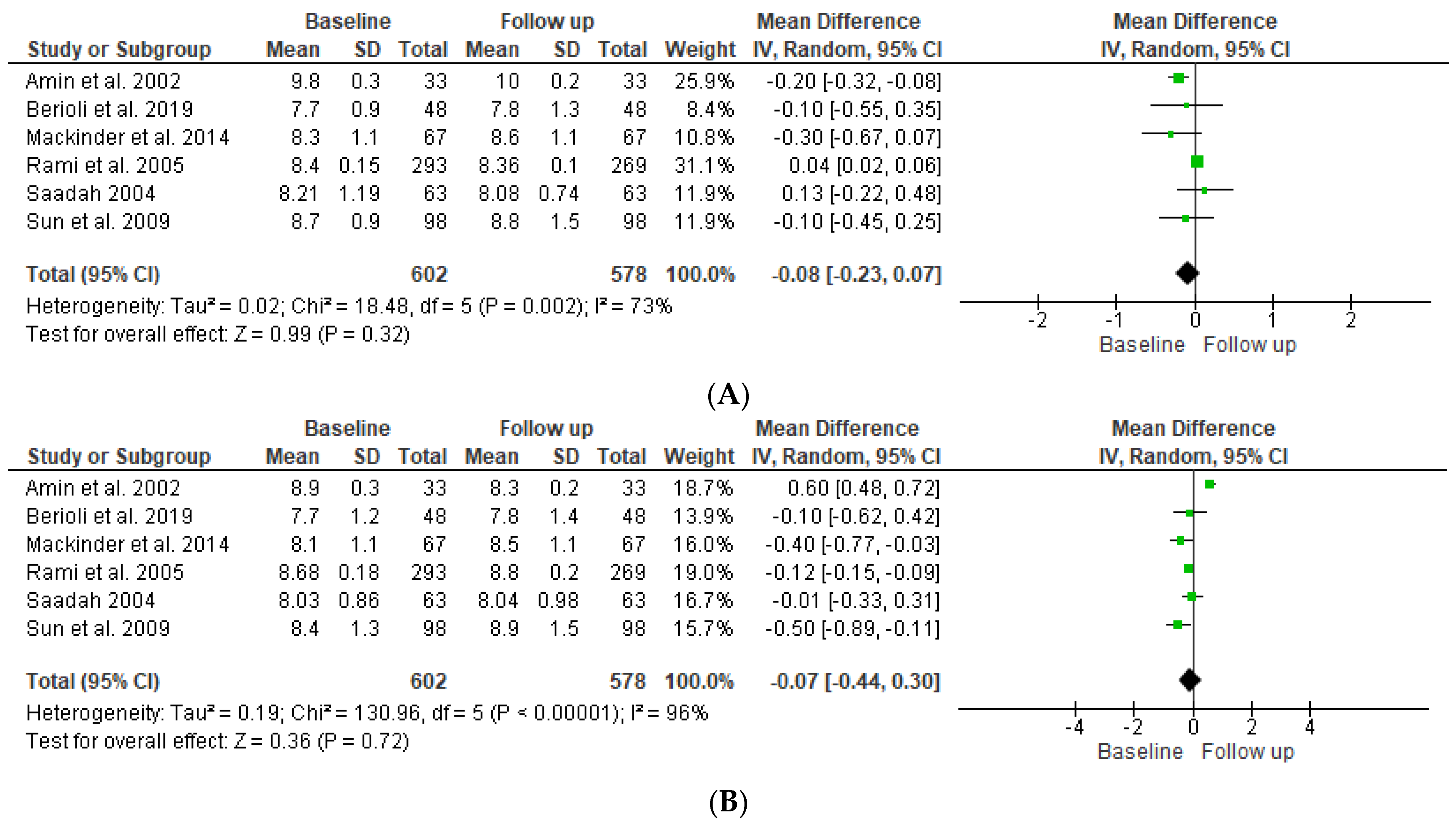
4.3. Glycosylated Hemoglobin
4.4. Lipid Profile, Hemoglobin Levels, Diabetic Renopathy, and Retinopathy
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- A.
- Cochrane: Strategy #1
- Search Query:#1 (“coeliac disease”):ti,ab,kw OR (“celiac disease”):ti,ab,kw OR (“coeliac diseases”):ti,ab,kw OR (“gluten-sensitive enteropathies”):ti,ab,kw OR (“gluten-sensitive enteropathies”):ti,ab,kw#2 (“diabetes mellitus type 1”):ti,ab,kw OR (“DM 1”):ti,ab,kw OR (“DM-1”):ti,ab,kw OR (“juvenile diabetes”):ti,ab,kw OR (“juvenile diabetes mellitus”):ti,ab,kw#3 MeSH descriptor: [Celiac Disease] explode all trees#4 MeSH descriptor: [Diabetes Mellitus, Type 1] explode all trees#5 (“gluten free diet”):ti,ab,kw OR (“gluten free diets”):ti,ab,kw OR (“gluten-free”):ti,ab,kw OR (“gluten free”):ti,ab,kw#6 MeSH descriptor: [Diet, Gluten-Free] explode all trees#7 (#4 OR #2) AND (#6 OR #5)#8 ((#4 OR #2) AND (#1 OR #3)) AND (#5 OR #6)
- Time of Search:September 28, 2019, 12:54:31.
- Results:
| BMC Gastroenterology (2015) 15:181 |
| BMJ Open 2015;5:e008097 |
| ClinicalTrials.gov Identifier: NCT02605564 |
| ClinicalTrials.gov Identifier: NCT02867436 |
| Diabetes Care. 1999 Oct;22(10):1747-8 |
| ClinicalTrials.gov Identifier: NCT03037190 |
| Diabetes Care 25:1111–1116, 2002 |
| ClinicalTrials.gov Identifier: NCT02605148 |
| ClinicalTrials.gov Identifier: NCT02680054 |
- Search Query:#1 (“coeliac disease”):ti,ab,kw OR (“celiac disease”):ti,ab,kw OR (“coeliac diseases”):ti,ab,kw OR (“gluten-sensitive enteropathies”):ti,ab,kw OR (“gluten-sensitive enteropathies”):ti,ab,kw#2 (“diabetes mellitus type 1”):ti,ab,kw OR (“DM 1”):ti,ab,kw OR (“DM-1”):ti,ab,kw OR (“juvenile diabetes”):ti,ab,kw OR (“juvenile diabetes mellitus”):ti,ab,kw#3 MeSH descriptor: [Celiac Disease] explode all trees#4 MeSH descriptor: [Diabetes Mellitus, Type 1] explode all trees#5 (“gluten free diet”):ti,ab,kw OR (“gluten free diets”):ti,ab,kw OR (“gluten-free”):ti,ab,kw OR (“gluten free”):ti,ab,kw#6 MeSH descriptor: [Diet, Gluten-Free] explode all trees#7 (#4 OR #2) AND (#6 OR #5)#8 ((#4 OR #2) AND (#1 OR #3)) AND (#5 OR #6)
- Time of Search:September 28, 2019, 12:54:31.
- Results:
| BMC Gastroenterology (2015) 15:181 |
| BMJ Open 2015;5:e008097 |
| ClinicalTrials.gov Identifier: NCT03037190 |
| Diabetes Care 1999 Oct;22(10):1747-8 |
| Diabetes Care 25:1111–1116, 2002 |
- Search Query:#1 MeSH descriptor: [Celiac Disease] explode all trees 338#2 MeSH descriptor: [Diabetes Mellitus, Type 1] explode all trees 5369#3 MeSH descriptor: [Diet, Gluten-Free] explode all trees 84#4 MeSH descriptor: [Glycated Hemoglobin A] explode all trees 5489#5 MeSH descriptor: [Bone Density] explode all trees 4536#6 MeSH descriptor: [Quality of Life] explode all trees 22705#7 MeSH descriptor: [Growth] explode all trees 19573#8 MeSH descriptor: [Anemia, Iron-Deficiency] explode all trees 1269#9 (Celiac):ti,ab,kw OR (Coeliac):ti,ab,kw OR (Gluten sensitive Enteropathy):ti,ab,kw 1261#10 (T1DM):ti,ab,kw OR (Type 1 DM):ti,ab,kw OR (Type 1 Diabetes Mellitus):ti,ab,kw OR (Juvenile Diabetes):ti,ab,kw OR (Insulin Dependent Diabetes):ti,ab,kw 38096#11 (GFD):ti,ab,kw OR (Gluten Free):ti,ab,kw 550#12 (Glycemic control):ti,ab,kw OR (HbA1C):ti,ab,kw 25407#13 (BMD):ti,ab,kw OR (Bone Mineral Density):ti,ab,kw OR (Bone Density):ti,ab,kw 12701#14 (QOL):ti,ab,kw OR (Quality of Life):ti,ab,kw 112273#15 (Growth):ti,ab,kw 45637#16 (Iron Deficiency Anemia):ti,ab,kw 2988#17 (#1 OR #9) AND (#2 OR #10) AND (#3 OR #11) AND (#4 OR #5 OR #6 OR #7 OR #8 OR #12 OR #13 OR #14 OR #15 OR #16) 12
- Time of Search:February 7, 2020, 15:33:48.
- Results:
| BMJ open, 2015, 5(5), e008097 |
| BMC gastroenterology, 2015, 15, 181 |
| BMJ open, 2015, 5(5), e008097 |
| Journal of pediatric gastroenterology and nutrition, 2017, 64(2), 175-179 |
| Pediatric diabetes 2018;19:49 |
| https://clinicaltrials.gov/show/NCT01566110, 2012 |
| BMC gastroenterology 2015;15(1): Article number: 181 |
| Pediatric diabetes 2014; 15: 114 |
| https://www.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2018/06/014508 |
| Diabetes care, 2011, 34(6), 1301-1305 |
| Pediatric Diabetes 2016;17(S24):33-34 |
| Diabetes care 1999;22(10):1747-1748 |
- B.
- EBSCO:
- Search Query:S1: diabetes mellitus type 1 OR dm type 1 OR juvenile diabetes OR insulin dependent diabetes OR iddmS2: celiac disease OR gluten sensitive OR gluten enteropathy OR coeliac diseaseS3: gluten free diet OR special diets OR gluten free OR gfdS4: glycemic control OR hba1c OR glucosetolerance test OR blood glucose levels OR quality of lifeS5: S1 AND S3 AND S4S6: S1 AND S2 S3 AND S4*Limit for paper date: 1 January 2011–31 December 2020.*Databases Searched: Business Source Complete, Academic Search Ultimate, Art & Architecture Complete, MEDLINE Complete, Education Research Complete, Communication & Mass Media Complete, Environment Complete, Computers & Applied Sciences Complete, Legal Collection, Energy & Power Source, Research Starters—Education, Research Starters—Business.
- Time of Search:October 11, 2019, 5:13:41 AM.
- Results:
| Food Reviews International. 2019, Vol. 35 Issue 6, p587-608 |
| SpringerPlus (2016) 5:994 |
| BMC Res Notes (2019) 12:50 |
| BMC Gastroenterology (2015) 15:181 |
| Indian J Med Res 149, January 2019, pp 18-25 |
| BMJ Open 2015;5:e008097 |
| BMC Gastroenterology 2014, 14:99 |
| Diabetes Ther (2019) 10:1151–1161 |
| British Journal of Nursing, 2019, Vol 28, No 15, 1015-1019 |
| Diabetes Therapy. Feb2019, Vol. 10 Issue 1, p119-134 |
| Acta Diabetol (2017) 54:889–894 |
| PLoS ONE. Nov2013, Vol. 8 Issue 11, p1-9 |
| Diabetic Medicine: A Journal Of The British Diabetic Association [Diabet Med] 2014 Feb; Vol. 31 (2), pp. 208-12 |
| Ethiop J Health Sci. Vol. 29, No. 4, 447-452 |
| Pediatric Diabetes [Pediatr Diabetes] 2011 Jun; Vol. 12 (4 Pt 1), pp. 322-5 |
| Journal of Diabetes Research. 12/20/2018, p1-11 |
| J Diabetes Investig 2019; 10: 104–107 |
| Turk J Endocrinol Metab 2017;21:127-130 |
| BMJ Case Reports 2012; doi:10.1136/bcr.02.2012.5878 |
| JURNALUL PEDIATRULUI – Year XVII, Vol. XVII, Supplement 1, 2014 |
| Pediatric Diabetes [Pediatr Diabetes] 2012 Dec; Vol. 13 (8), pp. 597-606 |
| Acta Diabetol (2013) 50:319–324 |
| Pediatric Diabetes [Pediatr Diabetes] 2012 Mar; Vol. 13 (2), pp. 163-9 |
| Scientific Reports volume7, Article number: 45286 (2017) |
| Diabetes Obes Metab. 2019;21:1769–1779 |
| Diabetes Care 34:2158-2163, 2011 |
| Journal of Diabetes 9 (2017), 865–873 |
| Diabetes Care 2015;38:801–807 |
| Diabetes Ther (2017) 8:875–886 |
| Diabetol Metab Syndr (2016) 8:51 |
| International Journal of Health Sciences Vol. 11, Issue 2 (April–June 2017), 65-71 |
| Nutrition & Metabolism (2019) 16:60 |
| ANNALS VOL 23, ISSUE 3, JULY–SEPT. 2017, 289-293 |
| Dig Dis Sci (2012) 57:1314–1320 |
| Nutrition & Metabolism (2017) 14:11 |
| JAMA August 15, 2017 Volume 318, Number 7, 637-646 |
| Aust N Z J Obstet Gynaecol 2019; 59: 208–214 |
| Indian Journal of Endocrinology and Metabolism (2016), 443-450 |
| Am J Clin Nutr 2019;109:288–296 |
| Nutrition Journal 2013, 12:29 |
| Pediatric Diabetes [Pediatr Diabetes] 2016 May; Vol. 17 (3), pp. 191-8 |
| Diabetic Medicine. Jul2013, Vol. 30 Issue 7, p835-839 |
| Lipids in Health and Disease (2016) 15:78 |
| Food & Nutrition Research 2016, 60: 32594 |
| Diabetic Medicine. May2018, Vol. 35 Issue 5, p541-547 |
| Nutrition Journal (2018) 17:42 |
| Asia Pac J Clin Nutr 2018;27(3):728-734 |
| Vojnosanit Pregl 2012; 69(10): 858–863 |
| J Community Health (2016) 41:584–592 |
| Diabet. Med. 36, 653–654 (2019) |
| Pediatric Diabetes. Sep2013, Vol. 14 Issue 6, p455-458 |
| Diabetes Care 2016;39:808–815 |
| J Nippon Med Sch 2013; 80 (3) |
| Journal of Nutrition & Metabolism. 2012, p1-21 |
| International Journal of Endocrinology. 2013, p1-7 |
| Eur J Nutr (2013) 52:813–824 |
| Journal of Jahrom University of Medical Sciences. 2012, Vol. 9 Issue 4, following p7-7 |
| Am J Clin Nutr 2017;106:1394–400 |
| Diabetes 2017;66:1373–1379 |
| Nutrition & Metabolism (2018) 15:80 |
| Diabetic Medicine. Nov2017, Vol. 34 Issue 11, p1554-1567 |
| Journal of Human Nutrition & Dietetics. Jun2017, Vol. 30 Issue 3, p385-393 |
| Diabetic Medicine. Sep2015, Vol. 32 Issue 9, p1149-1155 |
| Journal of Clinical Pharmacy and Therapeutics (2011) 36, 592–601 |
| BMC Public Health (2018) 18:525 |
| Diabetes 2017;66:627–639 |
| British Journal of Nutrition (2018), 119, 910–917 |
| Diabetes, Obesity & Metabolism. Jul2014, Vol. 16 Issue 7, p577-587 |
| Journal of Human Nutrition & Dietetics. Apr2014 Supplement, p21-27 |
| Diabetes 2017;66:75–86 |
| Ann Nutr Metab 2011;58:74–78 |
| British Journal of Nursing, 2017, Vol 26, No 10, 543-551 |
| Diabetes Care 2014;37:1824–1830 |
| Diabetes Care 2016;39:893–901 |
| South African Journal of Clinical Nutrition. 2016, Vol. 29 Issue 2, p90-94 |
| Australian and New Zealand Journal of Obstetrics and Gynaecology 2016; 56: 333–335 |
| Geriatr Gerontol Int 2012; 12 (Suppl. 1): 41–49 |
| Journal of Cystic Fibrosis 15 (2016) 261–262 |
| ACP Journal Club. 2/17/2015, Vol. 162 Issue 4, p1-1 |
| American Journal of Clinical Nutrition. Mar2013, Vol. 97 Issue 3, p453-454 |
| Diabetes Health. Oct/Nov2011, Vol. 20 Issue 5, p20-20 |
- Search Query:S1: diabetes mellitus type 1 OR dm type 1 OR juvenile diabetes OR insulin dependent diabetes OR iddmS2: celiac disease OR gluten sensitive OR gluten enteropathy OR coeliac diseaseS3: gluten free diet OR special diets OR gluten free OR gfdS4: glycemic control OR hba1c OR glucosetolerance test OR blood glucose levels OR quality of lifeS5: S1 AND S3 AND S4S6: S1 AND S2 S3 AND S4*Limit for paper date: 1 January 2011–31 December 2020*Databases Searched: Business Source Complete, Academic Search Ultimate, Art & Architecture Complete, MEDLINE Complete, Education Research Complete, Communication & Mass Media Complete, Environment Complete, Computers & Applied Sciences Complete, Legal Collection, Energy & Power Source, Research Starters—Education, Research Starters—Business
- Time of Search:October 11, 2019, 5:13:41 AM.
- Results:
| Food Reviews International 2019, Vol. 35 Issue 6, p587-608 |
| Indian J Med Res 149, January 2019, pp 18-25 |
| BMJ Open 2015;5:e008097 |
| BMC Gastroenterology (2015) 15:181 |
| BMC Gastroenterology 2014, 14:99 |
| Acta Diabetol (2017) 54:889–894 |
| Diabetic Medicine: A Journal Of The British Diabetic Association [Diabet Med] 2014 Feb;Vol. 31 (2), pp. 208-12 |
| Pediatric Diabetes [Pediatr Diabetes] 2011 Jun; Vol. 12 (4 Pt 1), pp. 322-5 |
| Scientific Reports volume7, Article number: 45286 (2017) |
| Pediatric Diabetes [Pediatr Diabetes] 2012 Dec; Vol. 13 (8), pp. 597-606 |
| Diabetes Care 34:2158-2163, 2011 |
| Pediatric Diabetes [Pediatr Diabetes] 2012 Mar; Vol. 13 (2), pp. 163-9 |
| Diabetes Care 2015;38:801–807 |
| Dig Dis Sci (2012) 57:1314–1320 |
| Pediatric Diabetes [Pediatr Diabetes] 2016 May; Vol. 17 (3), pp. 191-8 |
| Turk J Endocrinol Metab 2017;21:127-130 |
| Diabetol Metab Syndr (2016) 8:51 |
| JURNALUL PEDIATRULUI – Year XVII, Vol. XVII, Supplement 1, 2014 |
| Acta Diabetol (2013) 50:319–324 |
| ANNALS VOL 23, ISSUE 3, JULY–SEPT. 2017 |
| Diabetic Medicine. Jul2013, Vol. 30 Issue 7, p835-839 |
| BMJ Case Reports 2012; doi:10.1136/bcr.02.2012.5878 |
| Pediatric Diabetes. Sep2013, Vol. 14 Issue 6, p455-458 |
| Diabetes Health. Oct/Nov2011, Vol. 20 Issue 5, p20-20 |
- Search Query:S1: Celiac OR Coeliac OR Gluten Sensitive EnteropathyS2: T1DM OR Type 1 DM OR Type 1 Diabetes Mellitus OR Juvenile Diabetes OR Insulin Dependent DiabetesS3: GFD OR Gluten FreeS4: Glycemic Control OR HBA1C OR BMD OR Bone Mineral Density OR Bone Density OR QOL OR Quality of Life OR Growth OR Iron Deficiency AnemiaS5: S1 AND S2 AND S3 AND S4*Databases Searched: MEDLINE Complete, eBook Collection (EBSCOhost), MEDLINE, eBook Academic Collection (EBSCOhost), CINAHL Plus with Full Text
- Time of Search:January 31, 2020. 3:00 PM.
- Results:
| Diabetic Medicine Dec2009; 26(12): 1250-1254 |
| Journal of Pediatric Gastroenterology & Nutrition Feb2017; 64(2): 175-179 |
| BMC Gastroenterology 12/21/2015; 15: 181 |
| Pediatric Diabetes Dec2012; 13(8): 597-606 |
| Diabetic Medicine Jul2013; 30(7): 835-839 |
| Acta Paediatrica Apr 2017; 106(4): 639-646 |
| Diabetes Care Jul2002; 25(7): 1117-1122 |
| Pediatric Diabetes Jun2011; 12(4pt1): 322-325 |
| Pediatric Diabetes May2016; 17(3): 191-198 |
| Healy, Shavonne Access Nov2014; 28(9): 14-15 NLM UID: 9885733 |
| Diabetic Medicine Aug2005; 22(8): 1079-1082 |
| http://dx.doi.org/10.1136/bcr-2013-200472 |
| Archives of Disease in Childhood Sep2004; 89(9): 871-876 |
| Diabetes Care Oct2011; 34(10): 2158-2163. |
| Turkish Journal of Endocrinology & Metabolism 2017; 21(4): 127-130 |
| Digestive Diseases & Sciences May2012; 57(5): 1314-1320 |
| BMC Gastroenterology 2014; 14(1): 99 https://doi.org/10.1186/1471-230X-14-99 |
| Practical Diabetes International Apr2011; 28(3): 110-112 |
| http://dx.doi.org/10.1136/adc.87.6.495 |
| Gastroenterology & Hepatology from Bed to Bench Autumn2014; 7(4): 189-197 |
| Pediatric Diabetes Mar2012; 13(2): 163-169 |
| BioMed Research International 2013; 2013: 127589-127589 |
| Clinical Medicine & Research Oct2007; 5(3): 184-192 |
| British Journal of Diabetes & Vascular Disease Mar2008; 8(2): 67-71 |
- C.
- Pubmed:
- Search Query:(((“Diabetes Mellitus, Type 1”[MeSH Terms] AND (“Diet, Gluten-Free”[MeSH Terms] OR “Foods, Specialized”[MeSH Terms] OR “specialized diet”[All Fields]OR “special diet”[All Fields] OR “modified diet”[All Fields] OR “selective diet”[All Fields] OR “restrictive diet”[All Fields] OR “restricted diet”[All Fields] OR “restricted food intake”[All Fields] OR “restricted dietary intake”[All Fields] OR (restricted[All Fields] AND (“diet”[MeSH Terms] OR “diet”[All Fields] OR “dietary”[All Fields]) AND practices[All Fields]))) AND (“Blood Glucose”[MeSH Terms] OR “Hyperglycemia”[MeSH Terms] OR “Glucose Tolerance Test”[MeSH Terms] OR “Glycated Hemoglobin A”[MeSH Terms] OR “Diabetes Complications”[MeSH Terms] OR “Quality of Life”[MeSH Terms] OR “Life Style”[MeSH Terms] OR “Hospitalization”[MeSH Terms] OR “glycemic control”[All Fields] OR “re admission”[All Fields] OR “blood sugar control”[All Fields] OR “blood glucose control”[All Fields] OR “hospital admission”[All Fields])) AND (“humans”[MeSH Terms] AND (“infant”[MeSH Terms] OR “child”[MeSH Terms] OR “adolescent”[MeSH Terms]))) OR (((((“celiac”[All Fields] OR “coeliac”[All Fields] OR “celiac sprue”[All Fields] OR “nontropical sprue”[All Fields] OR (gluten-sensitive[All Fields] AND enteropath[All Fields]) OR “gluten-induced enteropathy”[All Fields] OR “gluten induced enteropathy”[All Fields]) OR (“type 1 diabetes mellitus”[All Fields] OR “type 1 diabetes”[All Fields] OR “juvenile diabetes”[All Fields] OR “t1dm”[All Fields] OR “t1d”[All Fields] OR “type-1 diabetes”[All Fields] OR “insulin dependent diabetes”[All Fields] OR “insulin dependant diabetes”[All Fields] OR “insulin-dependent diabetes”[All Fields] OR “insulin-dependant diabetes”[All Fields])) AND (“gluten-free diet”[All Fields] OR “gfd”[All Fields] OR “gluten free diet”[All Fields] OR “specialized diet”[All Fields] OR “restrictive diet”[All Fields] OR “restricted diet”[All Fields] OR “special diet”[All Fields] OR “gf diet”[All Fields] AND “specialized diet”[All Fields] OR “special diet”[All Fields] OR “modified diet”[All Fields] OR “selective diet”[All Fields] OR “restrictive diet”[All Fields] OR “restricted diet”[All Fields] OR “restricted food intake”[All Fields] OR “restricted dietary intake”[All Fields] OR (restricted[All Fields] AND (“diet”[MeSH Terms] OR “diet”[All Fields] OR “dietary”[All Fields]) AND practices[All Fields]))) AND (“blood glucose”[All Fields] OR “hyperglycemia”[All Fields] OR “glucose tolerance test”[All Fields] OR “glycated hemoglobin A”[All Fields] OR “diabetes complications “[All Fields] OR “quality of life”[All Fields] OR “Life Style”[All Fields] OR “hospitalization”[All Fields] OR “glycemic control”[All Fields] OR “re admission”[All Fields] OR “blood sugar control”[All Fields] OR “blood glucose control”[All Fields] OR “hospital admission”[All Fields] OR “qol”[All Fields] OR “hba1c”[All Fields] OR “blood sugar”[All Fields] OR “re admission”[All Fields] OR (hemoglobyn[All Fields] AND a1c[All Fields]))) NOT medline[sb]) AND (“humans”[MeSH Terms] AND (“infant”[MeSH Terms] OR “child”[MeSH Terms] OR “adolescent”[MeSH Terms]))
- Time of Search:October 4, 2019.
- Results:
| Scientific Reports | 7:45286, 2017, 1-7 |
| J Pediatr. 2016 Dec;179:131-138 |
| Kylökäs et al. BMC Gastroenterology (2016) 16:76 |
| Assor et al. BMC Gastroenterology (2015) 15:181, 1-10 |
| Diabet Med. 2016 Jul;33(7):947-55 |
| Nutr Hosp. 2015;32(2):634-637 |
| BMJ Open 2015;5:e008097, 1-8 |
| BMC Gastroenterology 2014, 14:99, 1-8 |
| J Obstet Gynecol Neonatal Nurs. 2013 Nov-Dec;42(6):619-28 |
| Diabet Med. 2014 Feb;31(2):208-12 |
| Pediatr Diabetes 2013 Sep;14(6):455-8 |
| BMJ Case Reports 2012, 1-3 |
| Pediatr Diabetes 2012 Dec;13(8):597-606 |
| Dig Dis Sci. 2012 May;57(5):1314-20 |
| DIABETES CARE, VOLUME 34, OCTOBER 2011, 2158-2163 |
| Pediatr Diabetes. 2012 Mar;13(2):163-9 |
| J Pediatr Endocrinol Metab. 2010 Nov;23(11):1169-73 |
| Dtsch Med Wochenschr. 2011 Feb;136(5):172-5 |
| Acta Biomed. 2010 Dec;81(3):165-70 |
| Diabet Med. 2009 Dec;26(12):1250-4 |
| Diabetologia (2009) 52:798–800 |
| Rev Latino-am Enfermagem 2005 janeiro-fevereiro; 14(1) |
| European Journal of Clinical Nutrition (2004) 58, 1429–1431 |
| Atherosclerosis. 1999 Aug;145(2):389-97 |
| J Am Diet Assoc. 1996 May;96(5):458-63 |
| Nurse Pract Forum. 1991 Sep;2(3):193-5 |
| Diabetes Care. 1987 Jan-Feb;10(1):33-8 |
| Zentralbl Gynakol. 1986;108(11):691-8 |
| Diabetes. 1975 Jul;24(7):672-9 |
- Search Query”(“Celiac Disease”[Mesh] AND “Diabetes Mellitus, Type 1”[Mesh]) AND (“Diet Therapy”[Mesh] OR “diet therapy”[Subheading]) AND (“2009/12/03”[PDat]: “2019/11/30”[PDat] AND (“infant”[MeSH Terms] OR “child”[MeSH Terms] OR “adolescent”[MeSH Terms]))
- Time of Search:November 30, 2019.
- Results:
| Indian J Med Res. 2019 Jan;149(1):18-25 |
| Pediatr Diabetes. 2019 May;20(3):293-303 |
| Can J Diet Pract Res. 2018 Sep 1;79(3):118-124 |
| Acta Diabetol. 2017 Oct;54(10):889-894 |
| Sci Rep. 2017 Mar 24;7:45286 |
| J Pediatr Gastroenterol Nutr. 2017 Aug;65(2):195-199 |
| J Pediatr. 2016 Dec;179:131-138 |
| BMC Gastroenterol. 2016 Jul 25;16(1):76 |
| Rev Gaucha Enferm. 2016 Mar;37(1):e53787 |
| J Diabetes Complications. 2016 Mar;30(2):295-9 |
| BMC Gastroenterol. 2015 Dec 21;15:181 |
| Lik Sprava. 2015 Jan-Mar;(1-2):167-9 |
| BMJ Open. 2015 May 11;5(5):e008097 |
| Diabetes Care. 2015 May;38(5):760-6 |
| Diabetes Care. 2014 Sep;37(9):e194-5 |
| J Paediatr Child Health. 2014 Oct;50(10):811-6 |
| BMC Gastroenterol. 2014 May 28;14:99 |
| Nutrients. 2013 Nov 18;5(11):4540-52 |
| Eur J Clin Invest. 2014 Jan;44(1):74-82 |
| Diabet Med. 2014 Feb;31(2):208-12 |
| Indian J Gastroenterol. 2013 Sep;32(5):330-4 |
| Pediatr Diabetes. 2013 Sep;14(6):455-8 |
| Indian J Gastroenterol. 2014 Mar;33(2):188-9 |
| J Gastroenterol Hepatol. 2013 Jan;28(1):99-105 |
| Indian J Gastroenterol. 2013 Mar;32(2):98-102 |
| Pediatr Diabetes. 2012 Dec;13(8):597-606 |
| Clin Exp Immunol. 2012 Feb;167(2):226-34 |
| Dig Dis Sci. 2012 May;57(5):1314-20 |
| Diabetes Care. 2011 Oct;34(10):2158-63 |
| Transl Res. 2011 Sep;158(3):140-5 |
| Pediatr Diabetes. 2012 Mar;13(2):163-9 |
| Pediatr Diabetes. 2011 Jun;12(4 Pt 1):322-5 |
| Diabetes Care. 2011 Jun;34(6):1301-5 |
| J Pediatr Endocrinol Metab. 2010 Nov;23(11):1169-73 |
| J Gastroenterol Hepatol. 2011 Feb;26(2):378-81 |
| Diabetes Res Clin Pract. 2011 Apr;92(1):53-6 |
| Acta Biomed. 2010 Dec;81(3):165-70 |
| J Pediatr. 2011 Feb;158(2):276-81.e1 |
| Gastroenterol Clin Biol. 2010 Apr-May;34(4-5):319-20. |
| Rheumatol Int. 2010 Apr;30(6):793-5 |
- Search Query((((((“diabetes mellitus, type 1”[mesh]) and “celiac disease”[mesh]))) AND (((((“diet therapy”[mesh]) or “nutrition therapy”[mesh]) or “diet, gluten-free”[mesh]))))) AND (((((((readmission) OR hospital readmission*s) OR “Patient Readmission”[Mesh]) OR patient readmission)) OR ((((((blood glucose) OR “Blood Glucose”[Mesh]) OR hypoglycemic control) OR glycemic control) OR diabetes management)) OR ((((((quality of life) OR “Quality of Life”[Mesh]) OR life quality) OR health quality)))) OR ((“diabetes “ and “celiac “ and “gluten” and “diet” NOT medline[sb]))
- Time of Search:November 18, 2019.
- Results:
| Diabetes Care. 2016 Aug;39(8):e119-20. |
| JAMA. 2016 Sep 20;316(11):1181-1192. |
| World J Diabetes. 2013 Aug 15;4(4):130-4. |
| doi: 10.2174/0929867326666190409120716. |
| Gastroenterol Hepatol Bed Bench. 2014 Fall;7(4):189-97. |
| World J Diabetes. 2015 Jun 10;6(5):707-14. |
| Horm Res Paediatr. 2019 Oct 8:1-8. |
| Diseases. 2015 Jun 19;3(2):111-121 |
| Clin Diabetes Endocrinol. 2018 Dec 19;4:24. |
| Exp Ther Med. 2014 Dec;8(6):1906-1908. Epub 2014 Oct 15. |
| Pak J Med Sci. 2014 Mar;30(2):287-90. |
| Case Rep Med. 2012;2012:813461. |
| Prz Gastroenterol. 2018;13(3):249-250 |
| J Clin Gastroenterol. 2019 Nov/Dec;53(10):e416-e423. |
| Clin Exp Gastroenterol. 2014 Dec 29;8:43-8 |
| Eat Weight Disord. 2018 Oct 27. |
| Case Rep Pediatr. 2012;2012:269689 |
| Middle East J Dig Dis. 2011 Mar;3(1):5-12. |
| Front Neurosci. 2017 Mar 27;11:155. |
| Case Rep Endocrinol. 2017;2017:2652403. |
| Ont Health Technol Assess Ser. 2011;11(3):1-63. Epub 2011 Jul 1. |
| J Community Hosp Intern Med Perspect. 2019 Feb 11;9(1):22-24 |
| Mayo Clin Proc. 2016 Dec 5. pii: S0025-6196(16)30634-6. |
| Clin Transl Gastroenterol. 2019 May 22;10(5):1-10. |
| United European Gastroenterol J. 2018 Aug;6(7):1022-1031 |
| Ann Hepatol. 2016 Jul–Aug;15(4):588-591. |
| Indian J Gastroenterol. 2019 Jun;38(3):263-267. |
| Nutrients. 2019 Aug 16;11(8). pii: E1925. |
| Indian J Med Res. 2019 Jan;149(1):18-25. |
| Hum Mol Genet. 2019 Sep 15;28(18):3037-3042 |
| Acta Paediatr. 2019 Apr;108(4):676-680 |
| J Clin Gastroenterol. 2019 Oct 31. |
| J Pediatr. 2016 Dec;179:131-138.e1 |
| BMC Gastroenterol. 2015 Dec 21;15:181 |
| Sci Rep. 2017 Mar 24;7:45286 |
| Can J Diet Pract Res. 2018 Sep 1;79(3):118-124. |
| Pediatr Diabetes. 2012 Mar;13(2):163-9 |
| Dig Dis Sci. 2012 May;57(5):1314-20. |
| Pediatr Diabetes. 2011 Jun;12(4 Pt 1):322-5 |
| Indian J Med Res. 2019 Jan;149(1):18-25. |
| Nutr Diabetes. 2017 Jan 9;7(1):e239 |
| Ann Hepatol. 2016 Jul-Aug;15(4):588-91 |
| BMJ Open. 2015 May 11;5(5):e008097. |
| Vnitr Lek. 2014 Jul-Aug;60(7-8):562-6 |
| J Paediatr Child Health. 2014 Oct;50(10):811-6. |
| BMC Gastroenterol. 2014 May 28;14:99. |
| Nutrients. 2013 Nov 27;5(12):4869-79. |
| Eur J Clin Invest. 2014 Jan;44(1):74-82 |
| Pediatr Diabetes. 2013 Sep;14(6):455-8 |
| Diabetes Educ. 2013 Jul-Aug;39(4):532-40 |
| Diabet Med. 2013 Jul;30(7):835-9 |
| Pediatr Diabetes. 2012 Dec;13(8):597-606 |
| Acta Diabetol. 2013 Jun;50(3):319-24 |
| Diabetes Care. 2011 Oct;34(10):2158-63 |
| Pediatr Diabetes. 2011 Jun;12(4 Pt 1):322-5 |
| Atherosclerosis. 2011 Aug;217(2):531-5. |
| J Pediatr Endocrinol Metab. 2010 Nov;23(11):1169-73. |
| Acta Biomed. 2010 Dec;81(3):165-70. |
| Tunis Med. 2010 Jan;88(1):18-22. |
| Przegl Lek. 2009;66(4):170-5. |
| Diabetologia. 2009 May;52(5):798-800 |
| Bone. 2008 Aug;43(2):322-6 |
| Diabetes Care. 2002 Jul;25(7):1117-22. |
- Search Query:((“Celiac Disease”[Mesh] AND “Diabetes Mellitus, Type 1”[Mesh]) AND “Diet, Gluten-Free”[Mesh]) AND ((((“Glycated Hemoglobin A”[Mesh] OR “Bone Density”[Mesh]) OR “Quality of Life”[Mesh]) OR “Growth”[Mesh]) OR “Anemia, Iron-Deficiency”[Mesh])
- Time of Search:February 8, 2020. 11:54 AM.
- Results:
| Nutr Diabetes. 2017 Jan 9;7(1):e239 |
| J Pediatr. 2016 Dec;179:131-138 |
| BMC Gastroenterol. 2015 Dec 21;15:181 |
| BMJ Open. 2015 May 11;5(5):e008097 |
| Diabetes Care. 2015 May;38(5):801-7 |
| BMC Gastroenterol. 2014 May 28;14:99 |
| Diabet Med. 2014 Feb;31(2):208-12 |
| Diabet Med. 2013 Jul;30(7):835-9 |
| Pediatr Diabetes. 2012 Dec;13(8):597-606 |
| Acta Diabetol. 2013 Jun;50(3):319-24 |
| Dig Dis Sci. 2012 May;57(5):1314-20 |
| Pediatr Diabetes. 2012 Mar;13(2):163-9 |
| Atherosclerosis. 2011 Aug;217(2):531-5 |
| J Pediatr Endocrinol Metab. 2010 Nov;23(11):1169-73 |
| J Gastroenterol Hepatol. 2011 Feb;26(2):378-81 |
| Acta Biomed. 2010 Dec;81(3):165-70 |
| Tunis Med. 2010 Jan;88(1):18-22 |
| Diabet Med. 2009 Dec;26(12):1250-4 |
- Search Query:(“Celiac” OR “Coeliac” OR “Gluten Sensitive Enteropathy”) AND (“T1DM” OR “Type 1 DM” OR “Type 1 Diabetes Mellitus” OR “Juvenile Diabetes” OR “Insulin Dependent Diabetes”) AND (“GFD” OR “Gluten Free”) AND (“Glycemic Control” OR “HbA1C” OR “BMD” OR “Bone Mineral Density” OR “Bone Density” OR “QOL” OR “Quality of Life” OR “Growth” OR “Iron Deficiency Anemia”) NOT Medline[Sb]
- Time of Search:February 9, 2020. 6:59 PM.
- Results:
| Diabetol Metab Syndr. 2016 Jul 29;8:51 |
| World J Diabetes. 2015 Jun 10;6(5):707-14 |
| World J Diabetes. 2013 Aug 15;4(4):130-4 |
- D.
- Web of Science:
- Search Query:TS=(“type 1 diabetes mellitus” OR “dm type 1” OR “dmt1” OR “juvenile diabetes” OR “insulin-dependent diabetes mellitus” OR “diabetes mellitus type 1” OR “type 1 diabetes”) AND TS=(“gluten-free diet” OR “gluten free” OR “gfd” OR “special diet” OR “gluten free diet” OR “gluten-free”) AND ALL=(glycemic control OR blood glucose OR hba1c OR glucose tolerance test OR quality of life)Timespan: 2011-2019.Indexes: SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI.
- Time of Search:October 18, 2019.
- Results:
| International Journal of Endocrinology Volume 2019, 1-9 |
| Pediatric Diabetes. 2019;1–10 |
| European Journal of Inflammation,2019, Volume 17: 1–5 |
| Journal of Functional Foods Volume 56, May 2019, Pages 163-170 |
| PAEDIATRICS AND INTERNATIONAL CHILD HEALTH 2019, VOL. 39, NO. 1, 23–31 |
| John Wiley & Sons Ltd. 2018 107, pp. 1879–1887 |
| Velasco-Benítez CA/et al/Colombia Médica - Vol. 49 Nº4 2018 (Oct-Dec), 273-279 |
| Pediatric Diabetes October 2018; 19 (Suppl. 27); 275-286 |
| Diabetes Research and Clinical Practice Volume 143, September 2018, Pages 282-287 |
| United European Gastroenterology Journal 2018, Vol. 6(7) 1022–1031 |
| Journal of Child Psychology and Psychiatry, 60, 7, (803-812), (2018) |
| J Endocrinol Metab. 2018;8(2-3):37-42 |
| The Lancet Child & Adolescent Health Volume 2, Issue 2, February 2018, Pages 133-143 |
| Dig Dis 2018;36:399–408 |
| British Journal of Hospital Medicine,2017, Vol. 78, No. 10 |
| Acta Diabetologica October 2017, Volume 54, Issue 10, pp 889–894 |
| ANNALS OF KING EDWARD MEDICAL UNIVERSITY LAHORE PAKISTAN, 2017, Volume: 23 Issue: 3 Pages: 307-311 |
| Scientific Reports | 7:45286, 2017, 1-7 |
| Adv Nutr 2017;8:356–61 |
| JPGN Volume 64, Number 2, February 2017, 175-179 |
| Nutrition & Diabetes (2017) 7, e239, 1-6 |
| The Journal of Pediatrics Volume 179, December 2016, Pages 131-138 |
| Indian Journal of Gastroenterology September 2016, Volume 35, Issue 5, pp 372–378 |
| Diabetol Metab Syndr (2016) 8:51 |
| SpringerPlus (2016) 5:994 |
| ANNALS OF HEPATOLOGY,2016, Volume: 15 Issue: 4 Pages: 588-591 |
| Gastroenterology (2015) 15:181 |
| Canadian Journal of Diabetes Volume 39, Issue 6, December 2015, Pages 513-519 |
| Nature Reviews Gastroenterology & Hepatology volume 12, pages 580–591 (2015) |
| Nutrients 2015, 7, 8733–8751 |
| Nature Reviews Gastroenterology & Hepatology volume 12, pages 507–515 (2015) |
| WORLD JOURNAL OF DIABETES,2015, Volume: 6 Issue: 5 Pages: 707-714 |
| Diabetes Care 2015;38:760–766 |
| United European Gastroenterology Journal 2015, Vol. 3(2) 106–120 |
| Journal of Pediatric Nursing Volume 30, Issue 2, March–April 2015, Pages 353-363 |
| BMJ Open 2015;5:e008097, 1-8 |
| Diabetes, Obesity and Metabolism 17: 3–8, 2015 |
| Scandinavian Journal of Gastroenterology. 2014; 49: 1304–1310 |
| J Paediatr Child Health,2014, 50: 811-816 |
| Pediatr Diabetes,2014, 15: 270-278 |
| BMC Gastroenterology 2014, 14:99 |
| PLOS ONE, November 2013 | Volume 8 | Issue 11, 1-9 |
| Acta Diabetologica October 2013, Volume 50, Issue 5, pp 821–822 |
| Acta Diabetologica June 2013, Volume 50, Issue 3, pp 319–324 |
| Der Diabetologe March 2013, Volume 9, Issue 2, pp 128–134 |
| Pediatric Diabetes,2012, Volume 13, Issue 8, 597-606 |
| Italian Journal of Pediatrics 2012, 38:10 |
| Pediatric Diabetes,2012, 13: 163-169 |
| European Journal of Gastroenterology & Hepatology: December 2011 - Volume 23 - Issue 12 - p 1270–1272 |
| Diabetes Care 34:2158–2163, 2011 |
| Atherosclerosis Volume 217, Issue 2, August 2011, Pages 531-535 |
| Pediatric Diabetes,2011, 12: 322-325 |
| J Pediatr. 2011 February; 158(2): 276–281 |
- Search Query:#1 (TS=(Celiac OR Coeliac OR Gluten Sensitive Enteropathy)) AND LANGUAGE: (English) AND DOCUMENT TYPES: (Article)Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCITimespan=All years#2 (TS=(T1DM OR Type 1 DM OR Type 1 Diabetes Mellitus OR Juvenile Diabetes OR Insulin Dependent Diabetes)) AND LANGUAGE: (English) AND DOCUMENT TYPES: (Article)Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCITimespan=All years#3 (TS=(GFD OR Gluten Free)) AND LANGUAGE: (English) AND DOCUMENT TYPES: (Article)Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCITimespan=All years#4 (TS=(Glycemic Control OR HbA1C OR BMD OR Bone Mineral Density OR Bone Density OR QOL OR Quality of Life OR Growth OR Iron Deficiency Anemia)) AND LANGUAGE: (English) AND DOCUMENT TYPES: (Article)Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCITimespan=All years#5 #4 AND #3 AND #2 AND #1Indexes=SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCITimespan=All years
- Time of Search:January 31, 2020. 4:38 PM.
- Results:
| PEDIATRICS DEC 2005;116(6):E754-E759 |
| DIABETES CARE NOV 2006;29(11):2452-2456 |
| CURRENT OPINION IN GASTROENTEROLOGY MAR 2010;26(2):116-122 |
| AMERICAN JOURNAL OF CLINICAL NUTRITION MAR 1998;67(3):477-481 |
| JOURNAL OF PEDIATRIC GASTROENTEROLOGY AND NUTRITION OCT 2001;33(4):462-465 |
| CANADIAN JOURNAL OF GASTROENTEROLOGY AND HEPATOLOGY MAY 2001;15(5):297-301 |
| DIABETES CARE JUL 2002;25(7):1117-1122 |
| DIABETES CARE OCT 2011;34(10):2158-2163 |
| ARCHIVES OF DISEASE IN CHILDHOOD SEP 2004;89(9):871-876 |
| GASTROENTEROLOGY APR 2005;128(4)(suppl. 1):S52-S56 |
| JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM MAY-JUN 1999;12(3):433-442 |
| HEPATO-GASTROENTEROLOGY MAR-APR 2001;48(38):462-464 |
| DIABETIC MEDICINE AUG 2005;22(8):1079-1082 |
| POSTGRADUATE MEDICAL JOURNAL FEB 2007;83(976):132-136 |
| ALIMENTARY PHARMACOLOGY & THERAPEUTICS APR 15 2009;29(8):898-905 |
| JOURNAL OF PEDIATRIC GASTROENTEROLOGY AND NUTRITION SEP 2005;41(3):317-321 |
| ACTA PAEDIATRICA 2002;91(3):297-302 |
| JOURNAL OF PEDIATRICS MAY 2007;150(5):461-466 |
| JOURNAL OF GASTROENTEROLOGY AND HEPATOLOGY FEB 2011;26(2):378-381 |
| PEDIATRIC DIABETES JUN 2011;12(4pt1):322-325 |
| ATHEROSCLEROSIS AUG 2011;217(2):531-535 |
| PEDIATRIC DIABETES JUN 2007;8(3):171-176 |
| WORLD JOURNAL OF GASTROENTEROLOGY AUG 28 2012;18(32):4399-4403 |
| JOURNAL OF PEDIATRICS FEB 2011;158(2):276-U141 |
| DIABETES CARE MAY 2015;38(5):760-766 |
| PEDIATRICS SEP 2009;124(3):E489-E495 |
| PEDIATRIC DIABETES DEC 2012;13(8):597-606 |
| JOURNAL OF PEDIATRICS APR 2011;158(4):589-U94 |
| DIABETIC MEDICINE DEC 2009;26(12):1250-1254 |
| JOURNAL OF PEDIATRIC HEMATOLOGY ONCOLOGY FEB 2003;25(2):169-172 |
| JOURNAL OF CLINICAL GASTROENTEROLOGY MAY-JUN 2008;42(5):460-465 |
| CLINICAL AND EXPERIMENTAL RHEUMATOLOGY JAN-FEB 2012;30(1):126-131 |
| DIABETOLOGIA JUL 2014;57(7):1339-1345 |
| PEDIATRIC DIABETES AUG 2008;9(4pt1):277-284 |
| DIABETIC MEDICINE JUL 2005;22(7):889-892 |
| ACTA DIABETOLOGICA JUN 2013;50(3):319-324 |
| HORMONE AND METABOLIC RESEARCH APR 2002;34(4):192-195 |
| BEST PRACTICE & RESEARCH CLINICAL GASTROENTEROLOGY JUN 2005;19(3):479-486 |
| PEDIATRIC DIABETES MAR 2012;13(2):163-169 |
| SCANDINAVIAN JOURNAL OF GASTROENTEROLOGY MAR 3 2016;51(3):288-294 |
| PEDIATRICS INTERNATIONAL FEB 2015;57(1):107-112 |
| BMJ Open. 2015 May 11;5(5):e008097 |
| JOURNAL OF PEDIATRIC GASTROENTEROLOGY AND NUTRITION FEB 2017;64(2):175-179 |
| DIABETES EDUCATOR JUL 2013;39(4):532-540 |
| JOURNAL OF PEDIATRICS 2016 Dec;179:131-138 |
| PEDIATRICS INTERNATIONAL AUG 2010;52(4):579-583 |
| BONE AUG 2008;43(2):322-326 |
| JOURNAL OF PEDIATRIC GASTROENTEROLOGY AND NUTRITION SEP 2015;61(3):297-302 |
| JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM NOV-DEC 2000;13(9):1629-1631 |
| Bratisl Lek Listy. 2009;110(4):258-62 |
| SAUDI MEDICAL JOURNAL DEC 2002;23(12):1514-1517 |
| BMC Gastroenterol. 2014 May 28;14:99 |
| ACTA DIABETOLOGICA OCT 2017;54(10):889-894 |
| ACTA DIABETOLOGICA DEC 2015;52(6):1167-1174 |
| JOURNAL OF PAEDIATRICS AND CHILD HEALTH OCT 2014;50(10):811-816 |
| EUROPEAN JOURNAL OF GASTROENTEROLOGY & HEPATOLOGY NOV 2011;23(12):1270-1272 |
| DIABETIC MEDICINE DEC 2014;31(12):E33-E36 |
| JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM NOV 2010;23(11):1169-1173 |
| ACTA PAEDIATRICA APR 2017;106(4):639-646 |
| JOURNAL OF PEDIATRIC NURSING-NURSING CARE OF CHILDREN & FAMILIES MAR-APR 2015;30(2):353-363 |
| PEDIATRIC DIABETES JUN 2018;19(4):741-748 |
| PEDIATRIC DIABETES JUN 2018;19(4):749-755 |
| Nutr Diabetes. 2017 Jan 9;7(1):e239 |
| CANADIAN JOURNAL OF DIABETES SEP 2011;35(4):334-339 |
| DIABETES RESEARCH AND CLINICAL PRACTICE SEP 2018;143():282-287 |
| JOURNAL OF ENDOCRINOLOGY AND METABOLISM MAY 2018;8(2-3):37-42 |
| INDIAN JOURNAL OF GASTROENTEROLOGY SEP 2016;35(5):372-378 |
| Book (Capter 10:Extraintestinal Manifestations of Celiac Disease and Associated Disorders) https://doi.org/10.3926/oms.258 |
| Book (Chapter: Celiac Disease in Adults) https://doi.org/10.3926/oms.233 |
| Int J Endocrinol. 2019 Sep 19;2019:7895207 |
| PEDIATRIC DIABETES DEC 2019;20(8):1100-1109 |
| EUROPEAN JOURNAL OF INFLAMMATION JUN 2019;17():- |
| JOURNAL OF PEDIATRIC ENDOCRINOLOGY & METABOLISM JAN 2019;32(1):89-93 |
| COLOMBIA MEDICA OCT-DEC 2018;49(4):273-279 |
| PEDIATRIC GASTROENTEROLOGY HEPATOLOGY & NUTRITION DEC 2017;20(4):222-226 |
| ANNALS OF KING EDWARD MEDICAL UNIVERSITY LAHORE PAKISTAN JUL-SEP 2017;23(3):307-311 |
| GAZZETTA MEDICA ITALIANA ARCHIVIO PER LE SCIENZE MEDICHE MAY 2017;176(5):308-313 |
| Book (Chapter 9.3: Coeliac Disease and diabetes) https://doi.org/10.1002/9781119121725.ch32 |
| Book (Chapter:Extraintestinal Manifestations and Associated Diseases) https://doi.org/10.3926/oms.215 |
| Przegląd Gastroenterologiczny 2011; 6 (4): 209–212 |
- A.
- Google Scholar:
- Search Query:with all of the words:“diabetes mellitus type 1” “gluten free” “glycemic” “glucose” celiac childrenwith the exact phrase:gluten-free dietwith at least one of the words:without the words:where my words occur:Return articles authored by:Return articles published in:Return articles dated between:2011–2020
- Time of Search:October 18, 2019.
- Results:
| Nutrients 2015, 7, 7143-7162 |
| Pediatr Diabetes. 2018 October; 19(Suppl 27): 275–286 |
| Pediatr Diabetes. 2015 November; 16(7): 485–492 |
| Ann. Pak. Inst. Med. Sci. 2018, 47-51 |
| Human and Veterinary Medicine; Cluj-Napoca Vol. 9, Iss. 1, (Mar 2017): 11-15 |
| Clinical Biochemistry 54 (2018) 11–17 |
| European Journal of Endocrinology (2016) 174, R127–R138 |
| Nat. Rev. Gastroenterol. Hepatol. 8, 405–415 (2011) |
| Google E-book Autoimmune associated diseases in pediatric patients with type 1 diabetes mellitus according to hla-dq genetic polymorphism |
| Oman Medical Journal (2015), Vol. 30, No. 2: 83–89 |
| Autoimmunity Reviews 16 (2017) 712–721 |
| The Impact of Coexisting Coeliac Disease on Type 1 Diabetes By Anna Pham-Short |
| American Society for Nutrition. Adv. Nutr. 4: 277–286, 2013 |
| Diabetes Research and Clinical Practice Volume 123, January 2017, Pages 63-74 |
| book Diabetic bone disease: Basic and translational research and clinical applications (pp.3-24) |
| Bakker-van Waarde, W. M. (2006). Bile salt and cholesterol metabolism in diabetes mellitus type 1 |
| Google E-book Medical Management of Type 1 Diabetes Sixth Edition American Diabetes Association |
| Ontario Health Technology Assessment Series 2011; Vol. 11, No. 3, 1-63 |
| Children 2018, 5, 169, 1-13 |
| Book STUDY ON THE GLYCAEMIC CONTROL AND RELATED COMPLICATIONS IN TYPE 1 DIABETIC CHILDREN By Dr. HEMA G. R. MBBS |
| Google E-book Glucose Regulation, an issue of nursing clinics by Celia M. Levesque |
| Physiol. Res. 67 (Suppl. 3): S441-S454, 2018 |
| Current Diabetes Reports October 2017, 17:83 |
| Journal of Pediatric Endocrinology and Metabolism Volume 20, Issue 12 |
| Feingold KR, Anawalt B, Boyce A et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000- |
| Feingold KR, Anawalt B, Boyce A et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000- |
| The Diabetes Textbook,2019, pp 941-966 |
| Hindawi Publishing Corporation Journal of Diabetes Research Volume 2015, 1-20 |
| A Practical Approach to Adolescent Bone Health,2018, pp 179-218 |
| Book Wheat Syndromes How Wheat, Gluten and ATI Cause Inflammation, IBS and Autoimmune Diseases |
| Journal of Pediatric Endocrinology and Metabolism Volume 22, Issue 12 |
| Critical Reviews™ in Immunology Volume 33, 2013 Issue 3, 245-281 |
| Book MUDr. Michal Huml Dizertační práce: Vliv Gastrointestinálního traktu na kompenzaci diabetes mellitus typu 1 v dětském věku Gastrointestinální hormony |
| Diabetol Metab Syndr 2018, 10(Suppl 1):27 |
| Current Opinion in Pediatrics: August 2010 - Volume 22 - Issue 4 - p 545–558 |
| Zsu, Hma, Pzheng - pdfs.semantischolar.org (Link not found) |
| Book MA Weinberg, SL Segelnick, JS Insler, S Kramer -2015 Wiley online library (File not found) |
| Book Endocrinology A methodological approach towards integrative understanding BOLK’S COMPANIONS ON THE PRACTICE OF MEDICINE |
| Book COMPARATIVE ANALYSIS OF THE SOLUBLE WHEAT PROTEINS AND HUMAN HEALTH Nhu Tuyen Vu The University of Sydney March 2014 |
| Book Analyza wybranych czynikow u dzieci z nowo rozpoznana cukryca typu 1 i ich wplyw na przebieg kliniczny choroby |
- Search Query:with all of the words → celiac diabeteswith the exact phrase → gluten free dietwith at least one of the words → pediatrics children infants adolescent “diabetes type 1” “type 1 diabetes” “gluten free” diet regimen2011-2020*Results listed below (42 references) include results of this search strategy plus papers retrieved through snowballing.
- Time of Search:
- Results:
| Diabetes Care 2011 Oct; 34(10): 2158-2163 |
| World J Diabetes. Aug 15, 2013; 4(4): 130-134 |
| Acta Diabetologica; Heidelberg Vol. 50, Iss. 5, (Oct 2013): 821-2. |
| Nutrients 2015, 7(9), 7143-7162 |
| J Pediatr. 2011 February; 158(2): 276–281 |
| The Journal of Pediatrics. April 2011, 158, (4):Pages 589-593.e2 |
| Pediatr Diabetes. 2011 Jun;12(4 Pt 1):322-5 |
| Pediatr Diabetes. 2012 Dec;13(8):597-606. |
| Diabetes Care 2015 May; 38(5): 760-766. |
| BMC Gastroenterology volume 14, Article number: 99 (2014) |
| BMC Gastroenterol. 2015 Dec 21;15:181 |
| Diabetes Care 2016 Aug; 39(8): e119-e120 |
| Acta Bio Med 2011, 81, 165-170 |
| Journal of Pediatric Gastroenterology and Nutrition. 41(3):317-321, SEPTEMBER 2005 |
| Pediatric Diabetes. 10():92–93, SEPTEMBER 2009 |
| J ASEAN Fed Endocr Soc, 2016, 31(1): 5-9 |
| Berioli, M. G., Mancini, G., Principi, N., Santi, E., Ascenzi, M., Rogari, F., … Esposito, S. (2019). Growth and glycemic control in children with type 1 diabetes and asymptomatic celiac disease treated with a gluten -free diet for 1 year. European Journal of Inflammation. https://doi.org/10.1177/2058739219855574 |
| Gastroenterology Rev 2018; 13 (3): 249–250 |
| AGA.May 2009,136, (5)(Suppl 1):A-473, |
| Diabetes Research and Clinical Practice,June 2009,84,(3), 332-334 |
| The Journal of Clinical Endocrinology & Metabolism, Volume 88, Issue 1, 1 January 2003, Pages 162–165, |
| Gastroenterol Clin Biol. 2010 Apr-May;34(4-5):319-20 |
| Clin Nutr. 2004 Apr;23(2):281-2. |
| La Pediatria Medica e Chirurgica: Medical and Surgical Pediatrics, 01 Mar 2007, 29(2):99-104 |
| Pediatric Diabetes, 2(3), 95–97 |
| Journal of Pediatric Endocrinology & Metabolism, 9, 101-111 (1996) |
| pediatric diabetes Volume12, Issue4pt1 June 2011 |
| Clin Pediatr Endocrinol 1998; 7(2), 125-129 |
| Hormone Research. February 2002; 57,(Suppl. 1):97-100 |
| Diabetic Medicne.December 2009, 26;(12): 1250-1254 |
| Diabetes Care 1998 Aug; 21(8): 1379-1380. |
| Diabetes Care 2006 Nov; 29(11): 2452-2456. |
| Diabetic medicine.1998;15,(1):38-44 |
| Diabetic Medicine. 2005;22(8),1079-1082 |
| acta paediatrica. March 2002;91(3):297-302 |
| Journal of Pediatric Endocrinology & Metabolism, 12,433-442 (1999) |
| World J Diabetes. 2013 Aug 15; 4(4): 130–134. |
| Acta Biomed. 2010 Dec;81(3):165-70 |
| Acta Diabetol 2013;50:319–324 |
| BMC Gastroenterology,December 2014, 14:99 |
| Prz Gastroenterol. 2018;13(3):249-250 |
| J Pediatr Endocrinol Metab. 2010 Nov;23(11):1169-73 |
- B.
- Springer:
- Search Query:(diabetes mellitus type 1 OR juvenile diabetes OR dmt1 OR dm-1 OR insulin dependent diabetes) AND (Celiac OR coeliac OR gluten sensitive OR gluten enteropathy) AND (gluten free OR gfd OR special diet) AND (glycemic control OR hba1c OR blood glucose OR glucose tolerance test OR blood glucose control)Limiters used: ‘Article Type’ ‘English Language’ ‘2011–2020′
- Time of Search:October 12, 2019.
- Results:
| Diabetologia September 2019, Volume 62, Supplement 1, pp 1–600 |
| Diabetologia (2014) 57:[Suppl1]S1–S566 |
| Internal and Emergency Medicine December 2012, Volume 7, Supplement 4, pp 361–568 |
| Journal of General Internal Medicine May 2019, Volume 34, Supplement 2, pp 99–867 |
| Internal and Emergency Medicine December 2011, Volume 6, Supplement 2, pp 191–392 |
| Journal of General Internal Medicine,2017, Vol. 32, Issue 2, S83-S808 |
| European Journal of Pediatrics November 2016, Volume 175, Issue 11, pp 1393–1880 |
| Journal of General Internal Medicine,2014, Vol. 29, Issue 1, S1- S545 |
| Journal of General Internal Medicine, 2018, Vol. 33, Issue. 2, S1- S758 |
| Journal of General Internal Medicine, 2015, Vol. 30, Issue. 2, S45-S551 |
| Hepatology International June 2013, Volume 7, Supplement 1, pp 1–754 |
| Journal of General Internal Medicine, 2016, Vol. 31, Issue. 2, S85-S922 |
| Obesity Surgery August 2011, Volume 21, Issue 8, pp 956–1156 |
| Journal of General Internal Medicine June 2013, Volume 28, Supplement 1, pp 1–489 |
| Osteoporosis International April 2018, Volume 29, Supplement 1, pp 149–565 |
| Indian Journal of Gastroenterology October 2018, Volume 37, Supplement 1, pp 1–137 |
| Internal and Emergency Medicine December 2011, Volume 6, Supplement 2, pp 141–190 |
| Inflammation Research June 2011, Volume 60, Supplement 1, pp 1–321 |
| Hepatology International March 2015, Volume 9, Supplement 1, pp 1–391 |
| Journal of Inherited Metabolic Disease September 2015, Volume 38, Supplement 1, pp 35–378 |
| Journal of Neurology June 2013, Volume 260, Supplement 1, pp 1–280 |
| Journal of Inherited Metabolic Disease September 2016, Volume 39, Supplement 1, pp 35–284 |
| Internal and Emergency Medicine December 2012, Volume 7, Supplement 4, pp 309–359 |
| Journal of Neurology June 2012, Volume 259, Supplement 1, pp 1–236 |
| Indian Journal of Gastroenterology November 2013, Volume 32, Supplement 1, pp 1–132 |
| Italian Journal of Pediatrics 2017, 43(Suppl 2):110, 1-42 |
| Journal of Inherited Metabolic Disease September 2018, Volume 41, Supplement 1, pp 37–219 |
| Irish Journal of Medical Science (1971 -) March 2018, Volume 187, Supplement 3, pp 17–113 |
| Advances in Rheumatology 2018, 58(Suppl 1):23, 1-115 |
- Results:
| J Pediatr Gastroenterol Nutr. 2001 Jan;32(1):37-40. |
| Endocrine Abstracts (2011);27:58 |

{kind=link}
{kind=link}
{kind=link}
| Reference | Sun et al., 2009 [12] | Mackinder et al., 2014 [13] | Rami et al., 2005 [14] | Amin et al., 2002 [15] | Berioli et al., 2019 [17] | Saadah et al., 2004 [16] |
|---|---|---|---|---|---|---|
| Study Design | Observational | Observational | Observational | Observational | Observational | Observational |
| Risk of Bias | None Found | None Found | None found | Not serious | Serious | Serious |
| Inconsistency | None | None | None | Serious | Not serious | Not serious |
| Indirectness | None | None | None | |||
| Imprecision | None | None | None | Serious | Serious | Serious |
| Publication Bias | None | None | None | None | None | None |
| Large Effect | No | No | No | No | No | No |
| Dose Response (Gradient) | Yes (A 5-year gradient is shown) | Yes (A 4-year gradient is shown) | Yes | Yes | Yes | Yes |
| All Plausible Confounding | - | - | - | - | - | - |
| Strength | Moderate (3) | Moderate (3) | Moderate (3) | Low (2) | Low (2) | Low (2) |
References
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition guidelines for diagnosing coeliac disease 2019. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef]
- Riechmann, E.R.; de Villasante, G.C.; Pascual, M.L.C.; Aliaga, E.D.; Allué, I.P.; Sánchez-Valverde, F.; Koninckx, C.R. Rational application of the new European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) 2020 criteria for the diagnosis of coeliac disease. An. Pediatría 2020, 92, 110.e1–110.e9. [Google Scholar] [CrossRef]
- Picarelli, A.; Di Tola, M.; Sabbatella, L.; Mercuri, V.; Pietrobono, D.; Bassotti, G.; D’Amico, T.; Donato, G.; Picarelli, G.; Marino, M.; et al. Type 1 diabetes mellitus and celiac disease: Endothelial dysfunction. Acta Diabetol. 2013, 50, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Elfström, P.; Sundström, J.; Ludvigsson, J.F. Systematic review with meta-analysis: Associations between coeliac disease and type 1 diabetes. Aliment. Pharmacol. Ther. 2014, 40, 1123–1132. [Google Scholar] [CrossRef] [PubMed]
- Assor, E.; Marcon, M.A.; Hamilton, N.; Fry, M.; Cooper, T.; Mahmud, F.H. Design of a dietary intervention to assess the impact of a gluten-free diet in a population with type 1 Diabetes and Celiac Disease. BMC Gastroenterol. 2015, 15, 181. [Google Scholar] [CrossRef]
- Al, H.E.T. Cölyak Tanı Guideline I. J. Pediatr. Gastroenterol. Nutr. 2005, 40, 1–19. [Google Scholar]
- Taler, I.; Phillip, M.; Lebenthal, Y.; de Vries, L.; Shamir, R.; Shalitin, S. Growth and metabolic control in patients with type 1 diabetes and celiac disease: A longitudinal observational case-control study. Pediatr. Diabetes 2012, 13, 597–606. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 372, n71. [Google Scholar] [CrossRef]
- Brannsether, B.; Eide, G.E.; Roelants, M.; Bjerknes, R.; Júlíusson, P.B. BMI and BMI SDS in childhood: Annual increments and conditional change. Ann. Hum. Biol. 2017, 44, 28–33. [Google Scholar] [CrossRef]
- Satya Krishna, S.; Kota, S.; Modi, K. Glycemic variability: Clinical implications. Indian J. Endocrinol. Metab. 2013, 17, 611. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Puttha, R.; Ghezaiel, S.; Skae, M.; Cooper, C.; Amin, R. The effect of biopsy-positive silent coeliac disease and treatment with a gluten-free diet on growth and glycaemic control in children with Type 1 diabetes. Diabet. Med. 2009, 26, 1250–1254. [Google Scholar] [CrossRef]
- Mackinder, M.; Allison, G.; Svolos, V.; Buchanan, E.; Johnston, A.; Cardigan, T.; Laird, N.; Duncan, H.; Fraser, K.; Edwards, C.A.; et al. Nutritional status, growth and disease management in children with single and dual diagnosis of type 1 diabetes mellitus and coeliac disease. BMC Gastroenterol. 2014, 14, 99. [Google Scholar] [CrossRef] [PubMed]
- Rami, B.; Sumnik, Z.; Schober, E.; Waldhör, T.; Battelino, T.; Bratanic, N.; Kürti, K.; Lebl, J.; Limbert, C.; Madacsy, L.; et al. Screening detected celiac disease in children with type 1 diabetes mellitus: Effect on the clinical course (a case control study). J. Pediatr. Gastroenterol. Nutr. 2005, 41, 317–321. [Google Scholar] [CrossRef]
- Amin, R.; Murphy, N.; Edge, J.; Ahmed, M.L.; Acerini, C.L.; Dunger, D.B. A longitudinal study of the effects of a gluten-free diet on glycemic control and weight gain in subjects with type 1 diabetes and celiac disease. Diabetes Care 2002, 25, 1117–1122. [Google Scholar] [CrossRef] [PubMed]
- Saadah, O.I.; Zacharin, M.; O’Callaghan, A.; Oliver, M.R.; Catto-Smith, A.G. Effect of gluten-free diet and adherence on growth and diabetic control in diabetics with coeliac disease. Arch. Dis. Child. 2004, 89, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Berioli, M.G.; Mancini, G.; Principi, N.; Santi, E.; Ascenzi, M.; Rogari, F.; Ceccarini, G.; Grohmann, U.; Esposito, S. Growth and glycemic control in children with type 1 diabetes and asymptomatic celiac disease treated with a gluten -free diet for 1 year. Eur. J. Inflamm. 2019, 17, 1–5. [Google Scholar] [CrossRef]
- Warncke, K.; Liptay, S.; Fröhlich-Reiterer, E.; Scheuing, N.; Schebek, M.; Wolf, J.; Rohrer, T.R.; Meissner, T.; Holl, R.W. Vascular risk factors in children, adolescents, and young adults with type 1 diabetes complicated by celiac disease: Results from the DPV initiative. Pediatr. Diabetes 2016, 17, 191–198. [Google Scholar] [CrossRef]
- Nagl, K.; Bollow, E.; Liptay, S.; Rosenbauer, J.; Koletzko, S.; Pappa, A.; Näke, A.; Fröhlich-Reiterer, E.; Döring, C.; Wolf, J.; et al. Lower HbA1c in patients with type 1 diabetes and celiac disease who reached celiac-specific antibody-negativity—A multicenter DPV analysis. Pediatr. Diabetes 2019, 20, 1100–1109. [Google Scholar] [CrossRef]
- Salardi, S.; Maltoni, G.; Zucchini, S.; Iafusco, D.; Zanfardino, A.; Confetto, S.; Toni, S.; Zioutas, M.; Marigliano, M.; Cauvin, V.; et al. Whole lipid profile and not only HDL cholesterol is impaired in children with coexisting type 1 diabetes and untreated celiac disease. Acta Diabetol. 2017, 54, 889–894. [Google Scholar] [CrossRef]
- Hansen, D.; Brock-Jacobsen, B.; Lund, E.; Bjørn, C.; Hansen, L.P.; Nielsen, C.; Fenger, C.; Lillevang, S.T.; Husby, S. Clinical benefit of a gluten-free diet in type 1 diabetic children with screening-detected celiac disease: A population-based screening study with 2 years’ follow-up. Diabetes Care 2006, 29, 2452–2456. [Google Scholar] [CrossRef] [PubMed]
- Gutch, M.; Avinash, A.; Sukriti, K.; Syed, R.M.; Keshav, G.K.; Abhinav, G. Impact of a gluten-free diet on several growth parameters in children with type 1 diabetes mellitus and celiac disease in western Uttar Pradesh, India. J. ASEAN Fed. Endocr. Soc. 2016, 31, 5–9. [Google Scholar] [CrossRef][Green Version]
- Pham-Short, A.; Donaghue, K.C.; Ambler, G.; Chan, A.K.; Hing, S.; Cusumano, J.; Craig, M.E. Early elevation of albumin excretion rate is associated with poor gluten-free diet adherence in young people with coeliac disease and diabetes. Diabet. Med. 2014, 31, 208–212. [Google Scholar] [CrossRef]
- Gopee, E.; van den Oever, E.L.; Cameron, F.; Thomas, M.C. Coeliac disease, gluten-free diet and the development and progression of albuminuria in children with type 1 diabetes. Pediatr. Diabetes 2013, 14, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Malalasekera, V.; Cameron, F.; Grixti, E.; Thomas, M.C. Potential reno-protective effects of a gluten-free diet in type 1 diabetes. Diabetologia 2009, 52, 798–800. [Google Scholar] [CrossRef] [PubMed]
- Bakker, S.F.; Tushuizen, M.E.; Von Blomberg, M.E.; Mulder, C.J.; Simsek, S. Type 1 diabetes and celiac disease in adults: Glycemic control and diabetic complications. Acta Diabetol. 2013, 50, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Uchigata, Y. Diabetes in childhood and adolescence. J. Jpn. Diabetes Soc. 2004, 47, 895–897. [Google Scholar]
- Wherrett, D.; Huot, C.; Mitchell, B.; Pacaud, D. Type 1 Diabetes in Children and Adolescents. Can. J. Diabetes 2013, 37 (Suppl. S1), S153–S162. [Google Scholar] [CrossRef]
- DeMelo, E.N.; McDonald, C.; Saibil, F.; Marcon, M.A.; Mahmud, F.H. Celiac Disease and Type 1 Diabetes in Adults: Is This a High-Risk Group for Screening? Can. J. Diabetes 2015, 39, 513–519. [Google Scholar] [CrossRef]
- Kaur, N.; Bhadada, K.; Minz, R.W. Interplay between Type 1 Diabetes Mellitus and Celiac Disease: Implications in Treatment. Dig. Dis. 2018, 160012, 399–408. [Google Scholar] [CrossRef]
- Goh, V.L.; Elizabeth Estrada, D.; Lerer, T.; Balarezo, F.; Sylvester, F.A. Effect of gluten-free diet on growth and glycemic control in children with type 1 diabetes and asymptomatic celiac disease. J. Pediatr. Endocrinol. Metab. 2010, 23, 1169–1173. [Google Scholar] [CrossRef] [PubMed]
- Kaur, P.; Agarwala, A.; Makharia, G.; Bhatnagar, S.; Tandon, N. Effect of gluten-free diet on metabolic control and anthropometric parameters in type 1 diabetes with subclinical celiac disease: A randomized controlled trial. Endocr. Pract. 2020, 26, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Arató, A.; Körner, A.; Verès, G.; Dezsöfi, A.; Ujpál, I.; Madácsy, L. Frequency of coeliac disease in Hungarian children with type 1 diabetes mellitus. Eur. J. Pediatr. 2003, 162, 1–5. [Google Scholar] [CrossRef]
- Packer, S.C.; Dornhorst, A.; Frost, G.S. The glycaemic index of a range of gluten-free foods. Diabet. Med. 2000, 17, 657–660. [Google Scholar] [CrossRef]
- Beisswenger, P.J.; Howell, S.K.; Russell, G.B.; Miller, M.E.; Rich, S.S.; Mauer, M. Early progression of diabetic nephropathy correlates with methylglyoxal-derived advanced glycation end products. Diabetes Care 2013, 36, 3234–3239. [Google Scholar] [CrossRef] [PubMed]
- Kiayias, J.A.; Vlachou, E.D.; Lakka-Papadodima, E. Venlafaxine HCl in the Treatmant of Painful Peripheral Diabetic Neuropathy. Diabetes Care 2000, 23, 699–715. [Google Scholar] [CrossRef] [PubMed]
- Mohn, A.; Cerruto, M.; Iafusco, D.; Prisco, F.; Tumini, S.; Stoppoloni, O.; Chiarelli, F. Celiac disease in children and adolescents with type I diabetes: Importance of hypoglycemia. J. Pediatr. Gastroenterol. Nutr. 2001, 32, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich-Reiterer, E.E.; Kaspers, S.; Hofer, S.; Schober, E.; Kordonouri, O.; Pozza, S.B.D.; Holl, R.W. Anthropometry, metabolic control, and follow-up in children and adolescents with type 1 diabetes mellitus and biopsy-proven celiac disease. J. Pediatr. 2011, 158, 589–593.e2. [Google Scholar] [CrossRef]
- Narula, P.; Porter, L.; Langton, J.; Rao, V.; Davies, P.; Cummins, C.; Kirk, J.; Barrett, T.; Protheroe, S. Gastrointestinal symptoms in children with type 1 diabetes screened for celiac disease. Pediatrics 2009, 124, e489–e495. [Google Scholar] [CrossRef]
- Acerini, C.L.; Ahmed, M.L.; Ross, K.M.; Sullivan, P.B.; Bird, G.; Dunger, D.B. Coeliac diseaese in children and adolescents with IDDM: Clinical characteristics and response to Gluten-free diet. Diabet. Med. 1998, 15, 38–44. [Google Scholar] [CrossRef]
- Telega, G.; Bennet, T.R.; Werlin, S. Emerging new clinical patterns in the presentation of celiac disease. Arch. Pediatr. Adolesc. Med. 2008, 162, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Forde, L.; McGrath, N.; Devaney, D.; Awadalla, S.; McDonnell, C.M.; Murphy, N.P. Coeliac screening in a high-risk population: Paediatric type 1 diabetes—A review of current guidelines and practice. Ir. J. Med. Sci. 2019, 188, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Patton, S.R. Adherence to Diet in Youth with Type 1 Diabetes. J. Am. Diet. Assoc. 2011, 111, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Glissen Brown, J.R.; Singh, P. Coeliac disease. Paediatr. Int. Child Health 2019, 39, 23–31. [Google Scholar] [CrossRef]
- Westman, E.; Ambler, G.R.; Royle, M.; Peat, J.; Chan, A. Children with coeliac disease and insulin dependent diabetes mellitus—Growth, diabetes control and dietary intake. J. Pediatr. Endocrinol. Metab. 1999, 12, 433–442. [Google Scholar] [CrossRef]
- Kaukinen, K.; Peräaho, M.; Collin, P.; Partanen, J.; Woolley, N.; Kaartinen, T.; Nuutinen, T.; Halttunen, T.; Mäki, M.; Korponay-Szabo, I. Small-bowel mucosal transglutaminase 2-specific IgA deposits in coeliac disease without villous atrophy: A prospective and randomized clinical study. Scand. J. Gastroenterol. 2005, 40, 564–572. [Google Scholar] [CrossRef]
- Fuchs, V.; Kurppa, K.; Huhtala, H.; Mäki, M.; Kekkonen, L.; Kaukinen, K. Delayed celiac disease diagnosis predisposes to reduced quality of life and incremental use of health care services and medicines: A prospective nationwide study. United Eur. Gastroenterol. J. 2018, 6, 567–575. [Google Scholar] [CrossRef]
- Sanchez-Albisua, I.; Wolf, J.; Neu, A.; Geiger, H.; Wäscher, I.; Stern, M. Coeliac disease in children with Type 1 diabetes mellitus: The effect of the gluten-free diet. Diabet. Med. 2005, 22, 1079–1082. [Google Scholar] [CrossRef]
- Sponzilli, I.; Chiari, G.; Iovane, B.; Scarabello, C.; Gkliati, D.; Monti, G.; Fanciullo, L.; de’ Angelis, G.L.; Vanelli, M. Celiac disease in children with type 1 diabetes: Impact of gluten free diet on diabetes management. Acta Biomed. 2010, 81, 165–170. [Google Scholar]
- Hu, F.B.; Van Dam, R.M.; Liu, S. Diet and risk of Type II diabetes: The role of types of fat and carbohydrate. Diabetologia 2001, 44, 805–817. [Google Scholar] [CrossRef]
- Valerio, G.; Spadaro, R.; Iafusco, D.; Lombardi, F.; Del Puente, A.; Esposito, A.; De Terlizzi, F.; Prisco, F.; Troncone, R.; Franzese, A. The influence of gluten free diet on quantitative ultrasound of proximal phalanxes in children and adolescents with type 1 diabetes mellitus and celiac disease. Bone 2008, 43, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Elmarakby, A.A.; Abdelsayed, R.; Liu, J.Y.; Mozaffari, M.S. Inflammatory cytokines as predictive markers for early detection and progression of diabetic nephropathy. EPMA J. 2010, 1, 117–129. [Google Scholar] [CrossRef]
- Abid, N.; Mcglone, O.; Cardwell, C.; Mccallion, W.; Carson, D. Clinical and metabolic effects of gluten free diet in children with type 1 diabetes and coeliac disease. Pediatr. Diabetes 2011, 12, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Simmons, J.H.; Klingensmith, G.J.; McFann, K.; Rewers, M.; Ide, L.M.; Taki, I.; Liu, E.; Hoffenberg, E.J. Celiac autoimmunity in children with type 1 diabetes: A two-year follow-up. J. Pediatr. 2011, 158, 276–281.e1. [Google Scholar] [CrossRef]
- Kordonouri, O.; Klingensmith, G.; Knip, M.; Holl, R.W.; Aanstoot, H.J.; Menon, P.S.N.; Craig, M.E. Other complications and diabetes-associated conditions in children and adolescents. Pediatr. Diabetes 2014, 15 (Suppl. S20), 270–278. [Google Scholar] [CrossRef]



| Sun et al., 2009 [12] | Mackinder et al., 2014 [13] | Rami et al., 2005 [14] | Amin et al., 2002 [15] | Saadah et al., 2004 [16] | Berioli et al., 2019 [17] | |
|---|---|---|---|---|---|---|
| Country | United Kingdom | United Kingdom | Europe | United Kingdom | Australia | Italy |
| Study design | Prospective case–control | Retrospective case–control | Prospective case–control | Prospective case–control | Prospective case–control | Prospective case–control |
| Year | 2009 | 2014 | 2005 | 2002 | 2004 | 2019 |
| Number of participants/controls | 49/49 | 18/9 | 98/195 | 22/11 | 21/42 | 16/32 |
| Recruitment of cases and controls | Pediatric diabetic units in North West England | Outpatient clinic at Royal Hospital for Sick Children Glasgow | Ten pediatric diabetic centers around Europe | Pediatric Diabetic clinic at John Radcliffe Hospital, Oxford | Royal Children’s Hospital Melbourne | Regional Centre for Children with T1DM at the Pediatric Clinic of Universita Degli Studi di, Perugia |
| Female (%) in the cases/comparators | 63/63 | 52/52 | 45/50 | 54/54 | 62/62 | 56/56 |
| The average age of cases/control (years) at the diagnosis of DM | 5.9/6 | 5.3/5 | 6.5/6.5 | 8.1/7.4 | 4/NA | 7.97/7.91 |
| The average age of cases (years) at the diagnosis of CD | 9.1 | 10.8 | 10 | 13.8 | 7.5 | 11.3 |
| Follow up after diagnosis of CD (years) | 2 | 2 | 1 | 4 | 1 | 1 |
| The quality assessment GRADE system | Moderate | Moderate | Moderate | Low | Low | Low |
| Number of patients baseline/follow up | 98/98 | 67/67 | 293/269 | 33/33 | 63/63 | 48/48 |
| Study | [N] | Effect of GFD | p-Value |
|---|---|---|---|
| Warnecke et al., 2016 [16] * | 974 | Improvement of HDL levels Improvement in HA1C Improvement in BMI SDS. | < 0.01 <0.0001 <0.0001 |
| Nagl et al., 2019 [17] | 608 | Improvement in Height SDS Improvement in Weight SDS | 0.001 0.001 |
| Salardi et al., 2017 [18] | 201 | Improvement in Total Cholesterol Improvement in Triglyceride | <0.025 <0.005 |
| Hansen et al., 2006 [19] | 33 | Improvement in Weight SDS Mean Corpuscle Volume Hemoglobin | 0.002 0.02 0.001 |
| Gutch et al., 2016 [20] | 24 | Improvement in Weight SDS Improvement in Hemoglobin Improvement in serum Iron Improvement in Calcium | <0.05 <0.05 <0.05 <0.05 |
| Acerini et al., 1998 [21] * | 7 | Effect on growth parameters or glycemic control | NS |
| Taler et al., 2012 [27] | 68 | No significant effect on growth and glycemic control | NS |
| Goh et al., 2010 [28] | 29 | There was no significant effect on growth parameters or glycemic control. | NS |
| Westman et al., 1999 [29] | 20 | Effect on growth parameters or glycemic control | NS |
| Sanchez-Albisua et al., 2005 [30] | 9 | Improvement in Height SDS. | 0.03 |
| Sponzilli et al., 2010 [31] * | 12 | Increase in Insulin requirement Increase in HA1C | 0.02 <0.001 |
| Valerio et al., 2008 [32] | 57 | Bone density improved significantly with strict glycemic control and adherence to GFD. | 0.015 |
| Malalasekera et al., 2009 [33] | 21 | Shows renoprotection of GFD | 0.04 |
| Gopee et al., 2013 [34] | 24 | Shows renoprotection of GFD | 0.01 |
| Mohn et al., 2001 [35] | 20 | Increase in Insulin requirements | 0.05 |
| Frohlich-Reiterer et al., 2011 [36] | 411 | Improvement in Weight SDS Improvement in Height SDS. | 0.001 0.001 |
| Narula et al., 2009 [37] * | 8 | Improvement in Weight-SDS Improvement in BMI-SDS | 0.008 0.02 |
| Abid et al., 2011 [38] | 22 | Increase in Insulin requirements | <0.005 |
| Pham-short et al., 2014 [39] | 129 | Non-adherence to GFD was associated with early evidence of renal disease | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burayzat, S.; Elsahoryi, N.; Freitekh, A.; Alzoubi, O.; Al-Najjar, R.; Tayyem, R. Does a Gluten-Free Diet Affect BMI and Glycosylated Hemoglobin in Children and Adolescents with Type 1 Diabetes and Asymptomatic Celiac Disease? A Meta-Analysis and Systematic Review. Children 2022, 9, 1247. https://doi.org/10.3390/children9081247
Burayzat S, Elsahoryi N, Freitekh A, Alzoubi O, Al-Najjar R, Tayyem R. Does a Gluten-Free Diet Affect BMI and Glycosylated Hemoglobin in Children and Adolescents with Type 1 Diabetes and Asymptomatic Celiac Disease? A Meta-Analysis and Systematic Review. Children. 2022; 9(8):1247. https://doi.org/10.3390/children9081247
Chicago/Turabian StyleBurayzat, Salma, Nour Elsahoryi, Ali Freitekh, Osama Alzoubi, Rahaf Al-Najjar, and Reema Tayyem. 2022. "Does a Gluten-Free Diet Affect BMI and Glycosylated Hemoglobin in Children and Adolescents with Type 1 Diabetes and Asymptomatic Celiac Disease? A Meta-Analysis and Systematic Review" Children 9, no. 8: 1247. https://doi.org/10.3390/children9081247
APA StyleBurayzat, S., Elsahoryi, N., Freitekh, A., Alzoubi, O., Al-Najjar, R., & Tayyem, R. (2022). Does a Gluten-Free Diet Affect BMI and Glycosylated Hemoglobin in Children and Adolescents with Type 1 Diabetes and Asymptomatic Celiac Disease? A Meta-Analysis and Systematic Review. Children, 9(8), 1247. https://doi.org/10.3390/children9081247