
Positive Parenting Behaviors and Child Development in Ceará, Brazil: A Population-Based Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Assessment
2.3. Statistical Analysis
2.4. Ethics
3. Results
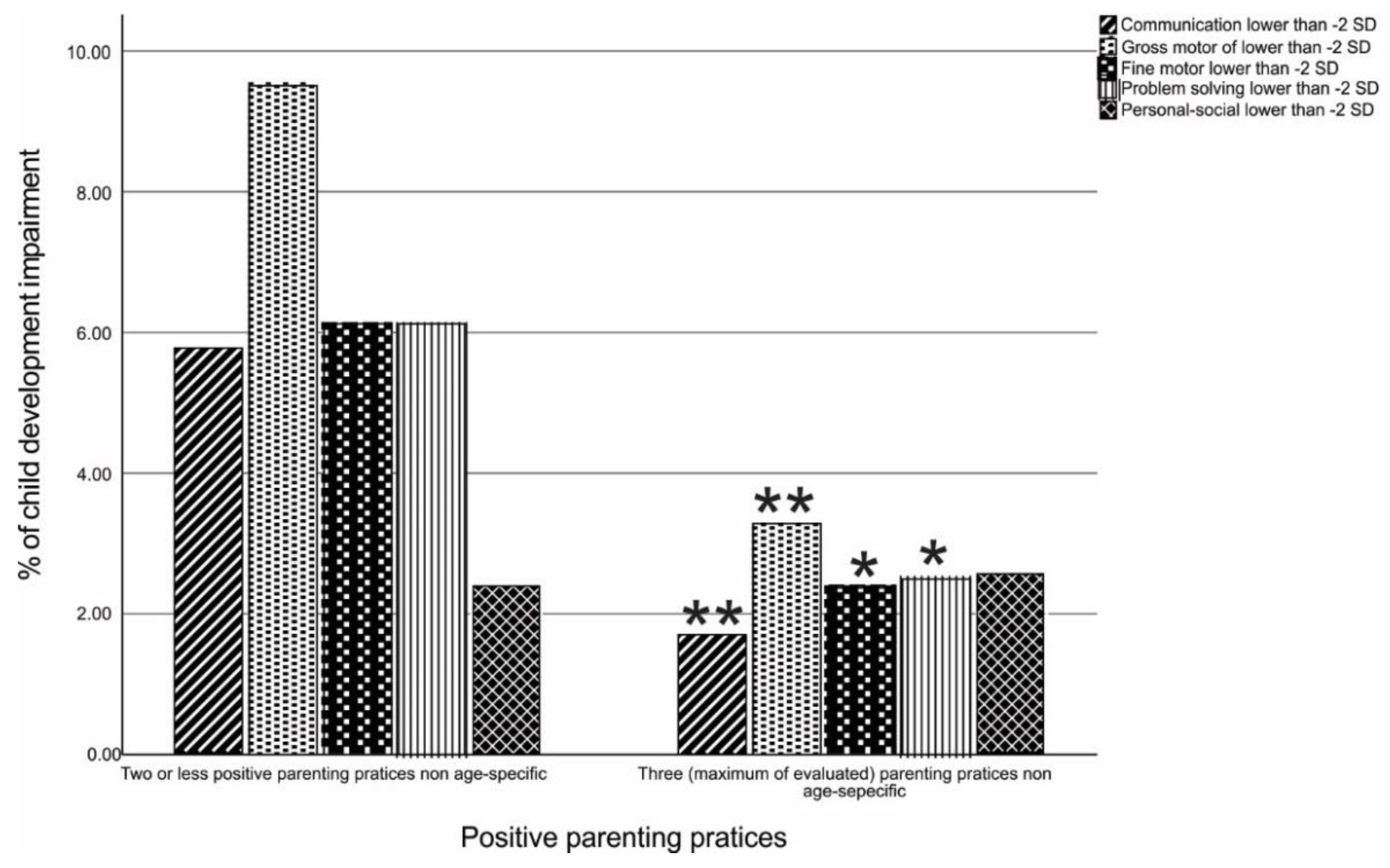
Association of Positive Parenting Behaviors and Child Development
4. Discussion
5. Conclusions
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olusanya, B.O.; Davis, A.C.; Wertlieb, D.; Boo, N.Y.; Nair, M.K.C.; Halpern, R.; Kuper, H.; Breinbauer, C.; de Vries, P.J.; Gladstone, M.; et al. Developmental disabilities among children younger than 5 years in 195 countries and territories, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Glob. Health 2018, 6, e1100–e1121. [Google Scholar] [CrossRef]
- Black, M.M.; Walker, S.P.; Fernald, L.C.H.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [PubMed]
- World Health Organization. Nurturing Care for Early Childhood Development: A Framework for Helping Children Survive and Thrive to Transform Health and Human Potential; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Grantham-McGregor, S.; Cheung, Y.B.; Cueto, S.; Glewwe, P.; Richter, L.; Strupp, B.; International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. Lancet 2007, 369, 60–70. [Google Scholar] [CrossRef]
- Smith, J. The Impact of Childhood Health on Adult Labor Market Outcomes. Rev. Econ. Stat. 2009, 91, 478–489. [Google Scholar] [CrossRef]
- Fay-Stammbach, T.; Hawes, D.J.; Meredith, P. Parenting Influences on Executive Function in Early Childhood: A Review. Child Dev. Perspect. 2014, 8, 258–264. [Google Scholar] [CrossRef]
- Coplan, R.J.; Hastings, P.D.; Lagacé-Séguin, D.G.; Moulton, C.E. Authoritative and Authoritarian Mothers’ Parenting Goals, Attributions, and Emotions Across Different Childrearing Contexts. Parenting 2002, 2, 1–26. [Google Scholar]
- Elkins, R.; Schurer, S. Exploring the role of parental engagement in non-cognitive skill development over the lifecourse. J. Popul. Econ. 2020, 33, 957–1004. [Google Scholar] [CrossRef]
- Osher, D.; Cantor, P.; Berg, J.; Steyer, L.; Rose, T. Drivers of human development: How relationships and context shape learning and development. Appl. Dev. Sci. 2020, 24, 6–36. [Google Scholar] [CrossRef]
- Meredith, L.R.; Catherine, E.S. Analyzing input quality along three dimensions: Interactive, linguistic, and conceptual. J. Child Lang. 2020, 47, 5–21. [Google Scholar]
- Cabrera, N.J.; Fitzgerald, H.E.; Bradley, R.H.; Roggman, L. The ecology of father-child relationships: An expanded model. J. Fam. Theory Rev. 2014, 6, 336–354. [Google Scholar]
- Kaur, S.; Randhawa, R.K. Effect of Biological Risk Factors and Home Environment on Motor Development in Early Child-Hood. Int. J. Med. Res. Health Sci. 2021, 10, 38–45. [Google Scholar]
- Jeong, J.; Franchett, E.E.; Ramos de Oliveira, C.V.; Rehmani, K.; Yousafzai, A.K. Parenting interventions to promote early child development in the first three years of life: A global systematic review and meta-analysis. PLoS Med. 2021, 18, e1003602. [Google Scholar] [CrossRef] [PubMed]
- Knauer, H.A.; Ozer, E.J.; Dow, W.H.; Fernald, L.C. Parenting quality at two developmental periods in early childhood and their association with child development. Early Child. Res. Q. 2019, 47, 396–404. [Google Scholar] [CrossRef]
- Correia, L.L.; Rocha, H.A.L.; Rocha, S.G.M.O.; Do Nascimento, L.S.; e Silva, A.C.; Campos, J.S.; Leite, Á.J. M. Methodology of Maternal and Child Health Populational Surveys: A Statewide Cross-sectional Time Series Carried Out in Ceará, Brazil, from 1987 to 2017, with Pooled Data Analysis for Child Stunting. Ann. Glob. Health 2019, 85. [Google Scholar] [CrossRef]
- de Araujo, J.A.; de Sampaio Morais, G.A.; Cruz, M.S. Estudo da pobreza multidimensional no Estado do Ceará. Rev. Ciências Adm. 2013, 19, 85–120. [Google Scholar]
- ABEP. Critério de Classificação Econômica Brasil: Associação Brasileira de Empresas de Pesquisa (ABEP); ABEP: Batangas, Philippines, 2013. [Google Scholar]
- World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- World Health Organization. Family and Community Practices that Promote Child Survival, Growth and Development: A Review of the Evidence; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Squires, J.; Bricker, D.D.; Twombly, E. Ages & Stages Questionnaires; Paul H. Brookes: Baltimore, MD, USA, 2009. [Google Scholar]
- Filgueiras, A.; Landeira-Fernandez, J. Adaptação Transcultural e Avaliação Psicométrica do Ages and Stages Questionnaires (ASQ) em Creches Públicas da Cidade do Rio de Janeiro; PUC-Rio: Psicologia, PUC-Rio Rio de Janeiro, Brazil, 2011. [Google Scholar]
- Silva, S.R.P. Validação Concorrente do Ages &Stages Questionnairescom o Screeningtestda Bayley Scales of Infant and Toddler Development III no Programa de Saúde da Família. Ph.D. Thesis, Universidade Federal de Pernambuco, Recife, Brazil, 2013. [Google Scholar]
- Filgueiras, A.; Pires, P.; Maissonette, S.; Landeira-Fernandez, J. Psychometric properties of the Brazilian-adapted version of the Ages and Stages Questionnaire in public child daycare centers. Early Hum. Dev. 2013, 89, 561–576. [Google Scholar] [CrossRef]
- Janson, H.; Squires, J. Parent-completed developmental screening in a Norwegian population sample: A comparison with US normative data. Acta Paediatr. 2007, 93, 1525–1529. [Google Scholar] [CrossRef]
- Walker, S.P.; Wachs, T.D.; Gardner, J.M.; Lozoff, B.; Wasserman, G.A.; Pollitt, E.; Carter, J.A.; International Child Development Steering Group. Child development: Risk factors for adverse outcomes in developing countries. Lancet 2007, 369, 145–157. [Google Scholar] [CrossRef]
- Britto, P.R.; Lye, S.J.; Proulx, K.; Yousafzai, A.K.; Matthews, S.G.; Vaivada, T.; Perez-Escamilla, R.; Rao, N.; Frcpch, P.I.; Fernald, L.C.H.; et al. Nurturing care: Promoting early childhood development. Lancet 2017, 389, 91–102. [Google Scholar] [CrossRef]
- Kaminski, J.W.; Valle, L.A.; Filene, J.H.; Boyle, C.L. A Meta-analytic Review of Components Associated with Parent Training Program Effectiveness. J. Abnorm. Child Psychol. 2008, 36, 567–589. [Google Scholar] [CrossRef]
- Miranda, A.O.; Estrada, D.; Firpo-Jimenez, M. Differences in Family Cohesion, Adaptability, and Environment among Latino Families in Dissimilar Stages of Acculturation. Fam. J. 2000, 8, 341–350. [Google Scholar] [CrossRef]
- Glassy, D.; Romano, J. Selecting Appropriate Toys for Young Children: The Pediatrician’s Role. Pediatrics 2003, 111, 911. [Google Scholar] [CrossRef] [PubMed]
- Trawick-Smith, J.; Russell, H.; Swaminathan, S. Measuring the effects of toys on the problem-solving, creative and social behaviours of preschool children. Early Child Dev. Care 2011, 181, 909–927. [Google Scholar] [CrossRef]
- Kordi, A.; Baharudin, R. Parenting Attitude and Style and Its Effect on Children’s School Achievements. Int. J. Psychol. Stud. 2010, 2, 217. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Mean ± SD or n (%) |
|---|---|
| Maternal and household characteristics | |
| Maternal age, years | 28.6 ± 7.2 |
| Maternal schooling, years | 4.4 ± 2.8 |
| Marital status | |
| Single | 780 (22.3) |
| Married | 1159 (33.2) |
| Stable relationship | 1370 (39.2) |
| Divorced | 162 (4.6) |
| Widowed | 22 (0.6) |
| Occupational status | |
| Homemaker | 2365 (68.2) |
| Works outside the home | 640 (18.4) |
| Works at home, for delivery services | 351 (10.1) |
| Does not work | 114 (3.3) |
| Monthly household income in Brazilian Reais in the past month | 1090.4 ± 1017.9 |
| Recipient of the Brazilian conditional cash transfer program | 1943 (54.5) |
| Child characteristics | |
| Stunting (HAZ < −2) | 293 (8.2) |
| Wasting (WHZ < −2) | 76 (2.1) |
| Underweight (WAZ < −2) | 107 (3.0) |
| Male child | 1786 (50.0%) |
| Child age | 31.8 ± 23.1 |
| Child ASQ-BR scores | |
| Communication | 52.2 ± 11.5 |
| Gross motor | 55.4 ± 9.3 |
| Fine motor | 49.7 ± 13.7 |
| Problem solving | 50.7 ± 12.5 |
| Personal–social | 50.1 ± 11.7 |
| Communication | Gross Motor | Fine Motor | Problem Solving | Personal–Social | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SMD for Each Additional Parenting Behavior 1 | p-Value | SMD for Each Additional Parenting Behavior 1 | p-Value | SMD for Each Additional Parenting Behavior 1 | p-Value | SMD for Each Additional Parenting Behavior 1 | p-Value | SMD for Each Additional Parenting Behavior 1 | p-Value | ||
| Children 0 to 1 year old | |||||||||||
| Number of age-specific positive parenting behaviors (4 maximum) | |||||||||||
| Median | 3 | 0.32 (0.24, 0.41) | <0.001 | 0.18 (0.11, 0.25) | <0.001 | 0.14 (0.06, 0.22) | <0.001 | 0.38 (0.24, 0.52) | 0.001 | 0.11 (0.06, 0.17) | <0.001 |
| (IQR) | (1–4) | ||||||||||
| Children 1–2 years old | |||||||||||
| Number of age-specific positive parenting behaviors (5 maximum) | |||||||||||
| Median | 5 | 0.05 (0.00, 0.10) | 0.06 | 0.06 (0.02, 0.10) | <0.006 | 0.08 (0.02, 0.14) | <0.01 | 0.12 (0.06, 0.17) | <0.001 | 0.09 (0.03, 0.14) | <0.002 |
| (IQR) | (4–5) | ||||||||||
| Children 3–4 years old | |||||||||||
| Number of age-specific positive parenting behaviors (6 maximum) | |||||||||||
| Median | 6 | 0.12 (0.05, 0.18) | <0.001 | 0.08 (0.00, 0.16) | <0.001 | 0.16 (0.10, 0.23) | <0.001 | 0.10 (0.03, 0.17) | <0.001 | 0.12 (0.04, 0.20) | <0.001 |
| (IQR) | (4–6) | ||||||||||
| Children 4–6 years old | |||||||||||
| Number of age-specific positive parenting behaviors (5 maximum) | |||||||||||
| Median | 5 | 0.22 (0.13, 0.32) | <0.001 | 0.19 (−0.02, 0.39) | <0.07 | 0.13 (−0.3, 0.29) | <0.11 | 0.21 (0.10, 0.32) | <0.001 | 0.26 (0.17, 0.36) | <0.001 |
| (IQR) | (4–5) | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rocha, H.A.L.; Correia, L.L.; Leite, Á.J.M.; Rocha, S.G.M.O.; Albuquerque, L.d.S.; Machado, M.M.T.; Campos, J.S.; e Silva, A.C.; Sudfeld, C.R. Positive Parenting Behaviors and Child Development in Ceará, Brazil: A Population-Based Study. Children 2022, 9, 1246. https://doi.org/10.3390/children9081246
Rocha HAL, Correia LL, Leite ÁJM, Rocha SGMO, Albuquerque LdS, Machado MMT, Campos JS, e Silva AC, Sudfeld CR. Positive Parenting Behaviors and Child Development in Ceará, Brazil: A Population-Based Study. Children. 2022; 9(8):1246. https://doi.org/10.3390/children9081246
Chicago/Turabian StyleRocha, Hermano A. L., Luciano L. Correia, Álvaro J. M. Leite, Sabrina G. M. O. Rocha, Lucas de S. Albuquerque, Márcia M. T. Machado, Jocileide S. Campos, Anamaria C. e Silva, and Christopher R. Sudfeld. 2022. "Positive Parenting Behaviors and Child Development in Ceará, Brazil: A Population-Based Study" Children 9, no. 8: 1246. https://doi.org/10.3390/children9081246
APA StyleRocha, H. A. L., Correia, L. L., Leite, Á. J. M., Rocha, S. G. M. O., Albuquerque, L. d. S., Machado, M. M. T., Campos, J. S., e Silva, A. C., & Sudfeld, C. R. (2022). Positive Parenting Behaviors and Child Development in Ceará, Brazil: A Population-Based Study. Children, 9(8), 1246. https://doi.org/10.3390/children9081246