
Health Literacy in Early Childhood: A Systematic Review of Empirical Studies


Abstract
:1. Introduction
- What knowledge is available regarding the health literacy of children under eight?
- In which areas of health literacy has research been conducted among young children?
- What are the issues that require further exploration?
- What kind of methods are used to explore health literacy in early childhood?
- What are the achieved outcomes of applied interventions related to the health literacy of young children?
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
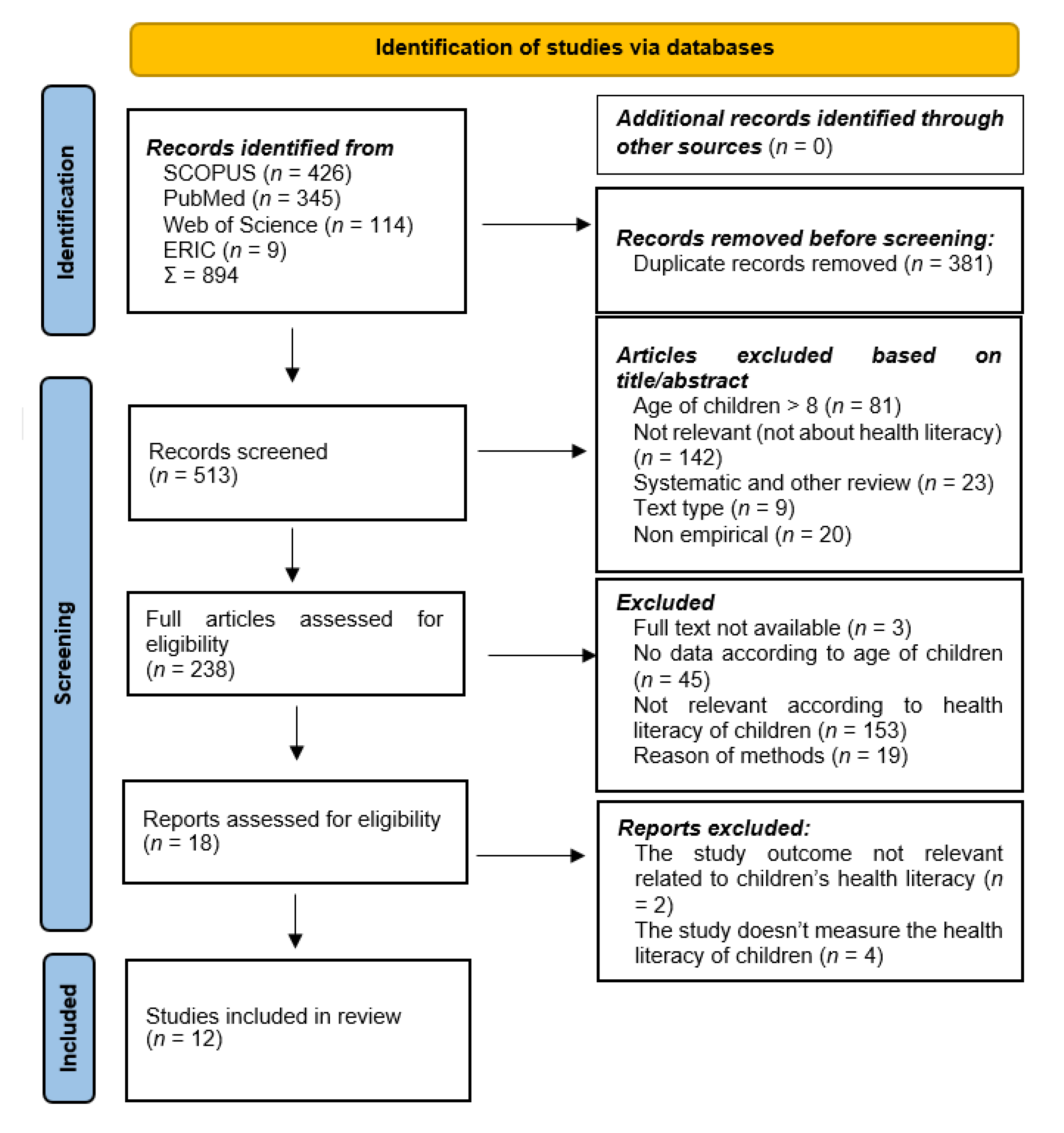
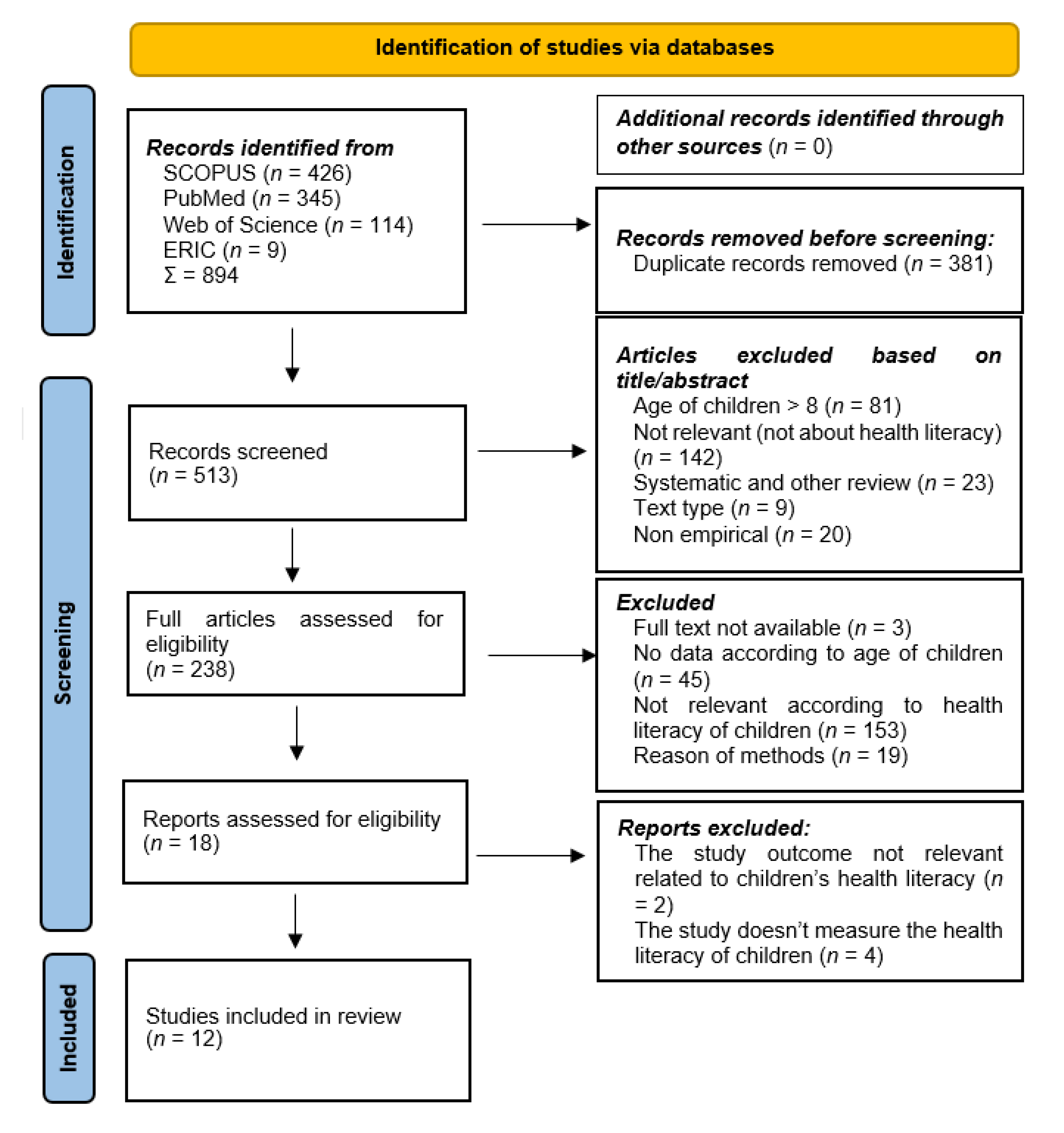
2.3. Selection Process
2.4. Quality Assessment
3. Results
3.1. Characteristics of Included Studies
3.2. Health Literacy in Early Childhood
3.2.1. Health Care
3.2.2. Food Literacy
3.2.3. Oral Health Literacy
3.2.4. Health Promotion
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frisch, A.L.; Camerini, L.; Diviani, N.; Schulz, P.J. Defining and measuring health literacy: How can we profit from other literacy domains? Health Promot. Int. 2012, 27, 117–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bröder, J.; Okan, O.; Bauer, U.; Bruland, D.; Schlupp, S.; Bollweg, T.M.; Saboga-Nunes, L.; Bond, E.; Sørensen, K.; Bitzer, E.M. Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health 2017, 17, 361. [Google Scholar] [CrossRef]
- Dawson-McClure, S.; Brotman, L.M.; Theise, R.; Palamar, J.J.; Kamboukos, D.; Barajas, R.G.; Calzada, E.J. Early childhood obesity prevention in low-income, urban communities. J. Prev. Interv. Community 2014, 42, 152–166. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Valerio, G.; Daniele, O.; Di Mauro, V.; Forte, S.; Muscariello, E.; Ricchiuti, R.; Sensi, S.; Balia, M.; Liguori, G.; et al. Multidisciplinary Treatment for Childhood Obesity: A Two-Year Experience in the Province of Naples, Italy. Children 2022, 9, 834. [Google Scholar] [CrossRef] [PubMed]
- Wakschlag, L.S.; Roberts, M.Y.; Flynn, R.M.; Smith, J.D.; Krogh-Jespersen, S.; Kaat, A.J.; Gray, L.; Walkup, J.; Marino, B.S.; Norton, E.S.; et al. Future Directions for Early Childhood Prevention of Mental Disorders: A Road Map to Mental Health, Earlier. J. Clin. Child Adolesc. Psychol. 2019, 48, 539–554. [Google Scholar] [CrossRef] [PubMed]
- Herr, R.M.; Diehl, K.; Schneider, S.; Osenbruegge, N.; Memmer, N.; Sachse, S.; Hoffmann, S.; Wachtler, B.; Herke, M.; Pischke, C.R.; et al. Which Meso-Level Characteristics of Early Childhood Education and Care Centers Are Associated with Health, Health Behavior, and Well-Being of Young Children? Findings of a Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 4973. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, H.D.; Kennett, A.R.; Kerling, E.H.; Yu, Q.; Gajewski, B.; Ptomey, L.T.; Sullivan, D.K. Assessing the Nutrition Literacy of Parents and Its Relationship with Child Diet Quality. J. Nutr. Educ. Behav. 2016, 48, 505–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, P.C.; Chang, I.H.; Chen, R.S. Online Learning Communities and Mental Health Literacy for Preschool Teachers: The Moderating Role of Enthusiasm for Engagement. Int. J. Environ. Res. Public Health 2019, 16, 4448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johri, M.; Subramanian, S.V.; Kone, G.K.; Dudeja, S.; Chandra, D.; Minoyan, N.; Sylvestre, M.P.; Pahwa, S. Maternal Health Literacy Is Associated with Early Childhood Nutritional Status in India. J. Nutr. 2016, 146, 1402–1410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogenchuk, M.; Graham, J.; Uswak, G.; Graham, H.; Weiler, R.; Ramsden, V.R. Pediatric oral health: Community-based participatory research. BMC Pediatr. 2022, 22, 93. [Google Scholar] [CrossRef]
- Ring-Dimitriou, S.; Freudenthaler, T.; Aistleitner, V.; Horvath, G.; Stallinger, J.; Dimitriou, M.; Ardelt-Gattinger, E.; Weghuber, D. SALTO—Study Protocol and Rationale of a Community-Oriented Obesity Prevention Program in the Kindergarten. Obes. Facts 2018, 11, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Sántha, Á. The Sociodemographic Determinants of Health Literacy in the Ethnic Hungarian Mothers of Young Children in Eastern Europe. Int. J. Environ. Res. Public Health 2021, 18, 5517. [Google Scholar] [CrossRef] [PubMed]
- Vann, W.F.; Divaris, K.; Gizlice, Z.; Baker, A.D.; Lee, J.Y. Caregivers’ Health Literacy and Their Young Children’s Oral-health–related Expenditures. J. Dent. Res. 2013, 92 (Suppl. S7), S55–S62. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Csima, M.; Fináncz, J.; Nyitrai, Á.; Podráczky, J. Research on the health literacy of professionals working in early childhood education. Kontakt 2018, 20, e356–e362. [Google Scholar] [CrossRef]
- Otten, C.; Nash, R.; Patterson, K. HealthLit4Kids: Teacher experiences of health literacy professional development in an Australian primary school setting. Health Promot. Int. 2022, daac053. [Google Scholar] [CrossRef]
- Cormier, E.; Park, H.; Schluck, G. eMental Health Literacy and Knowledge of Common Child Mental Health Disorders among Parents of Preschoolers. Issues Ment. Health Nurs. 2020, 41, 540–551. [Google Scholar] [CrossRef]
- Huang, L.; Hiscock, H.; Dalziel, K.M. Parents’ perception of children’s mental health: Seeing the signs but not the problems. Arch. Dis. Child. 2019, 104, 1102–1104. [Google Scholar] [CrossRef] [PubMed]
- Montes, G.R.; Bonotto, D.V.; Ferreira, F.M.; Menezes, J.V.N.B.; Fraiz, F.C. Caregiver’s oral health literacy is associated with prevalence of untreated dental caries in preschool children. Ciênc. Saúde Colet. 2019, 24, 2737–2744. [Google Scholar] [CrossRef] [Green Version]
- Opydo-Szymaczek, J.; Borysewicz-Lewicka, M.; Andrysiak, K.; Witkowska, Z.; Hoffmann-Przybylska, A.; Przybylski, P.; Walicka, E.; Gerreth, K. Clinical Consequences of Dental Caries, Parents’ Perception of Child’s Oral Health and Attitudes towards Dental Visits in a Population of 7-Year-Old Children. Int. J. Environ. Res. Public Health 2021, 18, 5844. [Google Scholar] [CrossRef]
- Sanders, L.M.; Perrin, E.M.; Yin, H.S.; Delamater, A.M.; Flower, K.B.; Bian, M.A.; Schildcrout, J.S.; Rothman, R.L.; Greenlight Study Team. A Health-Literacy Intervention for Early Childhood Obesity Prevention: A Cluster-Randomized Controlled Trial. Pediatrics 2021, 147, e2020049866. [Google Scholar] [CrossRef] [PubMed]
- Hiu Fong Lai, S.; Kok Wun Wong, M.; Ming Wong, H.; Kar Yung Yiu, C. Parental Oral Health Literacy of children with severe early childhood caries in Hong Kong. Eur. J. Paediatr. Dent. 2017, 18, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Wong, H.M.; McGrath, C.P. Parental Compliance towards Oral Health Education among Preschoolers with Special Healthcare Needs. Int. J. Environ. Res. Public Health 2021, 18, 7323. [Google Scholar] [CrossRef] [PubMed]
- Emmerton, L.; Chaw, X.Y.; Kelly, F.; Kairuz, T.; Marriott, J.; Wheeler, A.; Moles, R. Management of children’s fever by parents and caregivers: Practical measurement of functional health literacy. J. Child Health Care 2014, 18, 302–313. [Google Scholar] [CrossRef] [Green Version]
- Wallenstein, M.B.; Schroeder, A.R.; Hole, M.K.; Ryan, C.; Fijalkowski, N.; Alvarez, E.; Carmichael, S.L. Fever literacy and fever phobia. Clin. Pediatr. 2013, 52, 254–259. [Google Scholar] [CrossRef]
- Krajnović, D.; Ubavić, S.; Bogavac-Stanojević, N. Pharmacotherapy Literacy and Parental Practice in Use of Over-the-Counter Pediatric Medicines. Medicina 2019, 26, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ubavić, S.; Bogavac-Stanojević, N.; Jović-Vraneš, A.; Krajnović, D. Understanding of Information about Medicines Use among Parents of Pre-School Children in Serbia: Parental Pharmacotherapy Literacy Questionnaire (PTHL-SR). Int. J. Environ. Res. Public Health 2018, 15, 977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohns, M.J. Identifying the Preferred Method to Educate Low Income Caregivers About Common Childhood Illnesses: A Step Toward Health Literacy Through a Focus Group Study. J. Pediatr. Nurs. 2019, 47, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Gallego, G. Parents’ ability to access community health occupational therapy services in a disadvantaged area: A proof of concept study. Aust. Occup. Ther. J. 2020, 68, 54–64. [Google Scholar] [CrossRef]
- Bollweg, T.M.; Okan, O.; Pinheiro, P.; Bröder, J.; Bruland, D.; Fretian, A.; Domanska, O.; Jordan, S.; Bauer, U. Adapting the European Health Literacy Survey Questionnaire for 4th-grade Students in Germany: Questionnaire Development and Qualitative Pretest. HLRP Health Lit. Res. Pract. 2019, 4, e119–e128. [Google Scholar] [CrossRef]
- Rademakers, J.; Hahnraths, M.T.H.; van Schayck, O.C.P.; Heijmans, M. Children’s Health Literacy in Relation to Their BMI z-Score, Food Intake, and Physical Activity: A Cross-Sectional Study among 8–11-Year-Old Children in The Netherlands. Children 2022, 9, 925. [Google Scholar] [CrossRef] [PubMed]
- Sanders, L.M.; Federico, S.; Klass, P.; Abrams, M.A.; Dreyer, B. Literacy and child health: A systematic review. Arch. Pediatr. Adolesc. Med. 2009, 163, 131–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fok, M.S.M.; Wong, T.K.S. What does health literacy mean to children? Contemp. Nurse 2002, 13, 249–258. [Google Scholar] [CrossRef]
- Brown, S.L.; Teufel, J.A.; Birch, D.A. Early adolescents perceptions of health and health literacy. J. Sch. Health 2007, 77, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Chu-Ko, F.; Chong, M.L.; Chung, C.J.; Chang, C.C.; Liu, H.Y.; Huang, L.C. Exploring the factors related to adolescent health literacy, health-promoting lifestyle profile, and health status. BMC Public Health 2021, 21, 2196. [Google Scholar] [CrossRef] [PubMed]
- Lubman, D.I.; Berridge, B.J.; Blee, F.; Jorm, A.F.; Wilson, C.J.; Allen, N.B.; McKay-Brown, L.; Proimos, J.; Cheetham, A.; Wolfe, R. A school-based health promotion programme to increase help-seeking for substance use and mental health problems: Study protocol for a randomised controlled trial. Trials 2016, 17, 393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paakkari, O.; Torppa, M.; Villberg, J.; Kannas, L.; Paakkari, L. Subjective health literacy among school-aged children. Health Educ. 2018, 5, 182–195. [Google Scholar] [CrossRef] [Green Version]
- Sukys, S.; Trinkuniene; Tilindiene, I. Subjective Health Literacy among School-Aged Children: First Evidence from Lithuania. Int. J. Environ. Res. Public Health 2019, 13, 3397. [Google Scholar] [CrossRef] [Green Version]
- Office of the High Commissioner for Human Rights. Conventions on the Rights of the Child Fortieth Session. Geneva, 12–30 September 2005. Available online: https://www2.ohchr.org/english/bodies/crc/docs/AdvanceVersions/GeneralComment7Rev1.pdf (accessed on 15 June 2022).
- Heckman, J.J.; Moon, S.H.; Pinto, R.; Savelyev, P.A.; Yavitz, A. The Rate of Return to the High/Scope Perry Preschool Program. J. Public Econ. 2010, 94, 114–128. [Google Scholar] [CrossRef] [Green Version]
- Pascal, C.; Bertram, T. The Impact of Early Education as a Strategy in Countering Socio-Economic Disadvantage. Research Paper for Ofsted’s ‘Access and Achievement in Education 2013 Review’; Centre for Research in Early Childhood (CREC), 2013; Available online: https://docplayer.net/7001127-The-impact-of-early-education-as-a-strategy-in-countering-socio-economic-disadvantage.html (accessed on 22 June 2022).
- Anwar, N.H.; Nor, N.A.M.; Yusof, Z.Y.M. Effect of the SIMS program on oral hygiene levels of 5–6-year-old children in the Kampar District, Malaysia: A cluster-randomized controlled trial. Makara J. Health Res. 2020, 24. [Google Scholar] [CrossRef]
- Brega, A.G.; Thomas, J.F.; Henderson, W.G.; Batliner, T.S.; Quissell, D.O.; Braun, P.A.; Wilson, A.; Bryant, L.L.; Nadeau, K.J.; Albino, J. Association of parental health literacy with oral health of Navajo Nation preschoolers. Health Educ. Res. 2016, 31, 70–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charsley, J.S.; Collins, S.C.; Hill, A.J. The bigger picture: Young children’s perception of fatness in the context of other physical differences. Pediatr. Obes. 2018, 13, 558–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derwig, M.; Tiberg, I.; Hallström, I. Elucidating the child’s perspective in health promotion: Children’s experiences of child-centred health dialogue in Sweden. Health Promot. Int. 2021, 36, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.; Drummond, C. My dad’s a “barbie” man and my mum’s the cooking girl. J. Child Health Care 2013, 19, 279–292. [Google Scholar] [CrossRef]
- Privitera, G.J.; Phillips, T.E.; Zuraikat, F.M.; Paque, R. Emolabeling increases healthy food choices among grade school children in a structured grocery aisle setting. Appetite 2015, 92, 173–177. [Google Scholar] [CrossRef]
- Stålberg, A.; Sandberg, A.; Söderbäck, M. Younger children’s (three to five years) perceptions of being in a health-care situation. Early Child Dev. Care 2016, 186, 832–844. [Google Scholar] [CrossRef]
- Tabacchi, G.; Battaglia, G.; Alesi, M.; Paoli, A.; Palma, A.; Bellafiore, M. Food literacy predictors and associations with physical and emergent literacy in pre-schoolers: Results from the Training-to-Health Project. Public Health Nutr. 2019, 23, 356–365. [Google Scholar] [CrossRef] [Green Version]
- Tabacchi, G.; Battaglia, G.; Messina, G.; Paoli, A.; Palma, A.; Bellafiore, M. Validity and internal consistency of the preschool-flat, a new tool for the assessment of food literacy in young children from the training-to-health project. Int. J. Environ. Res. Public Health 2020, 17, 2759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabacchi, G.; Petrigna, L.; Battaglia, G.; Navarra, G.; Palma, A.; Bellafiore, M. An Interaction Path of Mothers’ and Preschoolers’ Food- and Physical Activity-Related Aspects in Disadvantaged Sicilian Urban Areas. Int. J. Environ. Res. Public Health 2021, 18, 2875. [Google Scholar] [CrossRef]
- Tsakpounidou, K.; Psomiadis, S.; Pourliaka, T.; Akritidou, M.; Proios, H. Baseline Stroke Literacy of Young Children Based on “FAST 112 Heroes” Program. Front. Public Health 2021, 14, 638516. [Google Scholar] [CrossRef]
- Zhou, N.; Wong, H.M.; McGrath, C. Efficacy of Social Story Intervention in Training Toothbrushing Skills Among Special-Care Children With and Without Autism. Autism Res. 2020, 13, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Systematic Review-Research Guide. Available online: https://libguides.murdoch.edu.au/systematic/PICO (accessed on 6 July 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 9, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quality Assessment for the Systematic Review of Qualitative Evidence. Available online: https://www.ncbi.nlm.nih.gov/books/NBK262835/ (accessed on 8 July 2022).
- A Guide to Evidence Synthesis: 9. Risk of Bias Assessment. Available online: https://guides.library.cornell.edu/evidence-synthesis/bias (accessed on 8 July 2022).
- Bélanger, M.; Humbert, L.; Vatanparast, H.; Ward, S.; Muhajarine, N.; Chow, A.F.; Engler-Stringer, R.; Donovan, D.; Carrier, N.; Leis, A. A multilevel intervention to increase physical activity and improve healthy eating and physical literacy among young children (ages 3–5) attending early childcare centres: The Healthy Start-Départ Santé cluster randomised controlled trial study protocol. BMC Public Health 2016, 16, 313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Po’e, E.K.; Heerman, W.J.; Mistry, R.S.; Barkin, S.L. Growing Right Onto Wellness (GROW): A family-centered, community-based obesity prevention randomized controlled trial for preschool child-parent pairs. Contemp. Clin. Trials 2013, 36, 436–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yusof, Z.Y.M.; Anwar, N.H.; Mohd Nor, N.A.; Nor, M.M.; Mustafa, S.E. The effect of the SIMS Programme versus existing preschool oral healthcare programme on oral hygiene level of preschool children: Study protocol for a cluster randomised controlled trial. Trials 2021, 22, 156. [Google Scholar] [CrossRef]
- Freeman, R. Storytelling, sugar snacking, and toothbrushing rules: A proposed theoretical and developmental perspective on children’s health and oral health literacy. Int. J. Paediatr. Dent. 2015, 25, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Noble, K.; Fetherston, H.; Jackson, J.; Craike, M. Effective Integration of Health Promotion in Early Childhood Education and Care Settings; Policy Paper 2020-02; Australian Health Policy Collaboration: Melbourne, Australia; Mitchell Institute, Victoria University: Melbourne, Australia, 2020. [Google Scholar]
- López-Escribano, C.; Valverde-Montesino, S.; García-Ortega, V. The Impact of E-Book Reading on Young Children’s Emergent Literacy Skills: An Analytical Review. Int. J. Environ. Res. Public Health 2021, 18, 6510. [Google Scholar] [CrossRef]
- Blewitt, C.; O’Connor, A.; Morris, H.; Nolan, A.; Mousa, A.; Green, R.; Ifanti, A.; Jackson, K.; Skouteris, H. “It’s Embedded in What We Do for Every Child”: A Qualitative Exploration of Early Childhood Educators’ Perspectives on Supporting Children’s Social and Emotional Learning. Int. J. Environ. Res. Public Health 2021, 18, 1530. [Google Scholar] [CrossRef]
- Herrmann, C.; Bretz, K.; Kühnis, J.; Seelig, H.; Keller, R.; Ferrari, I. Connection between Social Relationships and Basic Motor Competencies in Early Childhood. Children 2021, 8, 53. [Google Scholar] [CrossRef] [PubMed]
- Iivonen, S.; Kettukangas, T.; Soini, A.; Viholainen, H. Sand Play for 0–8-Year-Old Children’s Health and Development: A Systematic Review Protocol. Int. J. Environ. Res. Public Health 2021, 18, 10112. [Google Scholar] [CrossRef] [PubMed]
- Carbone, S.; Del Buono, M.G.; Ozemek, C.; Lavie, C.J. Obesity, risk of diabetes and role of physical activity, exercise training and cardiorespiratory fitness. Progr. Cardiovasc. Dis. 2019, 62, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Wagner, N.; Meusel, D.; Höger, C.; Kirch, W. Health promotion in kindergarten children: An assessment of evaluated projects in Germany. J. Public Health 2005, 13, 291–295. [Google Scholar] [CrossRef]
- Pierce, J.P.; White, V.M.; Emery, S.L. What public health strategies are needed to reduce smoking initiation? Tobacco Control 2012, 21, 258–264. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author/Year | Country | Title | Journal Source | General HL Dimesion * | Specific HL ** Dimension |
|---|---|---|---|---|---|
| Anwar et al. (2020) [42] | Malaysia | Effect of the SIMS program on oral hygiene levels of 5–6-year-old children in the Kampar District, Malaysia: A randomized children in the Kampar District, Malaysia: A cluster-randomized controlled trial | Makara Journal of Health Research | Disease prevention | Oral health |
| Brega et al. (2016) [43] | USA, Colorado | Association of parental health literacy with oral health of Navajo Nation preschoolers | Health Education Research | General HL among parents | OHL among children and parents |
| Charsley et al. (2018) [44] | UK | The bigger picture: young children’s perception of fatness in the context of other physical differences | Pediatric Obesity | Health promotion | Food literacy |
| Derwig et al. (2020) [45] | Sweden | Elucidating the child’s perspective in health promotion: Children’s experiences of child-centred health dialogue in Sweden | Health Promotion International | Health promotion | Food literacy |
| Drummond et al. (2013) [46] | Australia | My dad’s a ‘barbie’ man and my mum’s the cooking girl: Boys and the social construction of food and nutrition | Journal of Child Healthcare | Health promotion | Food literacy |
| Privitera et al. (2015) [47] | USA |
Emolabeling increases healthy food choices among grade school children in a structured grocery aisle setting | Appetite | Health promotion | Food literacy |
| Stålberg et al. (2016) [48] | Sweden | Younger children’s (three to five years) perceptions of being in a health-care situation | Early Child Development and Care | General HL-Health care | - |
| Tabacchi et al. (2019) [49] | Italy | Food literacy predictors and associations with physical and emergent literacy in pre-schoolers: results from the Training-to-Health Project | Public Health Nutrition | Health promotion | Food literacy-knowledge |
| Tabacchi et al. (2020) [50] | Italy | Validity and Internal Consistency of the Preschool-FLAT, a New Tool for the Assessment of Food Literacy in Young Children from the Training-To-Health Project | International Journal of Environmental Research and Public Health | Health promotion | Food literacy |
| Tabacchi et al. (2021) [51] | Italy | An Interaction Path of Mothers’ and Preschoolers’ Food- and Physical Activity-Related Aspects in Disadvantaged Sicilian Urban Areas | International Journal of Environmental Research and Public Health | Health promotion | Food literacy |
| Tsakpounidou et al. (2021) [52] | Greece | Baseline Stroke Literacy of Young Children Based on “FAST 112 Heroes” Program | Frontiers in Pubic Health | Health promotion | Stroke literacy |
| Zhou et al. (2020) [53] | Hong Kong | Efficacy of Social Story Intervention in Training Toothbrushing SkillsAmong Special-Care Children With and Without Autism | Autism Research | Disease prevention | Oral literacy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bánfai-Csonka, H.; Betlehem, J.; Deutsch, K.; Derzsi-Horváth, M.; Bánfai, B.; Fináncz, J.; Podráczky, J.; Csima, M. Health Literacy in Early Childhood: A Systematic Review of Empirical Studies. Children 2022, 9, 1131. https://doi.org/10.3390/children9081131
Bánfai-Csonka H, Betlehem J, Deutsch K, Derzsi-Horváth M, Bánfai B, Fináncz J, Podráczky J, Csima M. Health Literacy in Early Childhood: A Systematic Review of Empirical Studies. Children. 2022; 9(8):1131. https://doi.org/10.3390/children9081131
Chicago/Turabian StyleBánfai-Csonka, Henrietta, József Betlehem, Krisztina Deutsch, Martina Derzsi-Horváth, Bálint Bánfai, Judit Fináncz, Judit Podráczky, and Melinda Csima. 2022. "Health Literacy in Early Childhood: A Systematic Review of Empirical Studies" Children 9, no. 8: 1131. https://doi.org/10.3390/children9081131
APA StyleBánfai-Csonka, H., Betlehem, J., Deutsch, K., Derzsi-Horváth, M., Bánfai, B., Fináncz, J., Podráczky, J., & Csima, M. (2022). Health Literacy in Early Childhood: A Systematic Review of Empirical Studies. Children, 9(8), 1131. https://doi.org/10.3390/children9081131