

Mid–Long-Term Outcomes of Surgical Treatment of Legg-Calvè-Perthes Disease: A Systematic Review

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
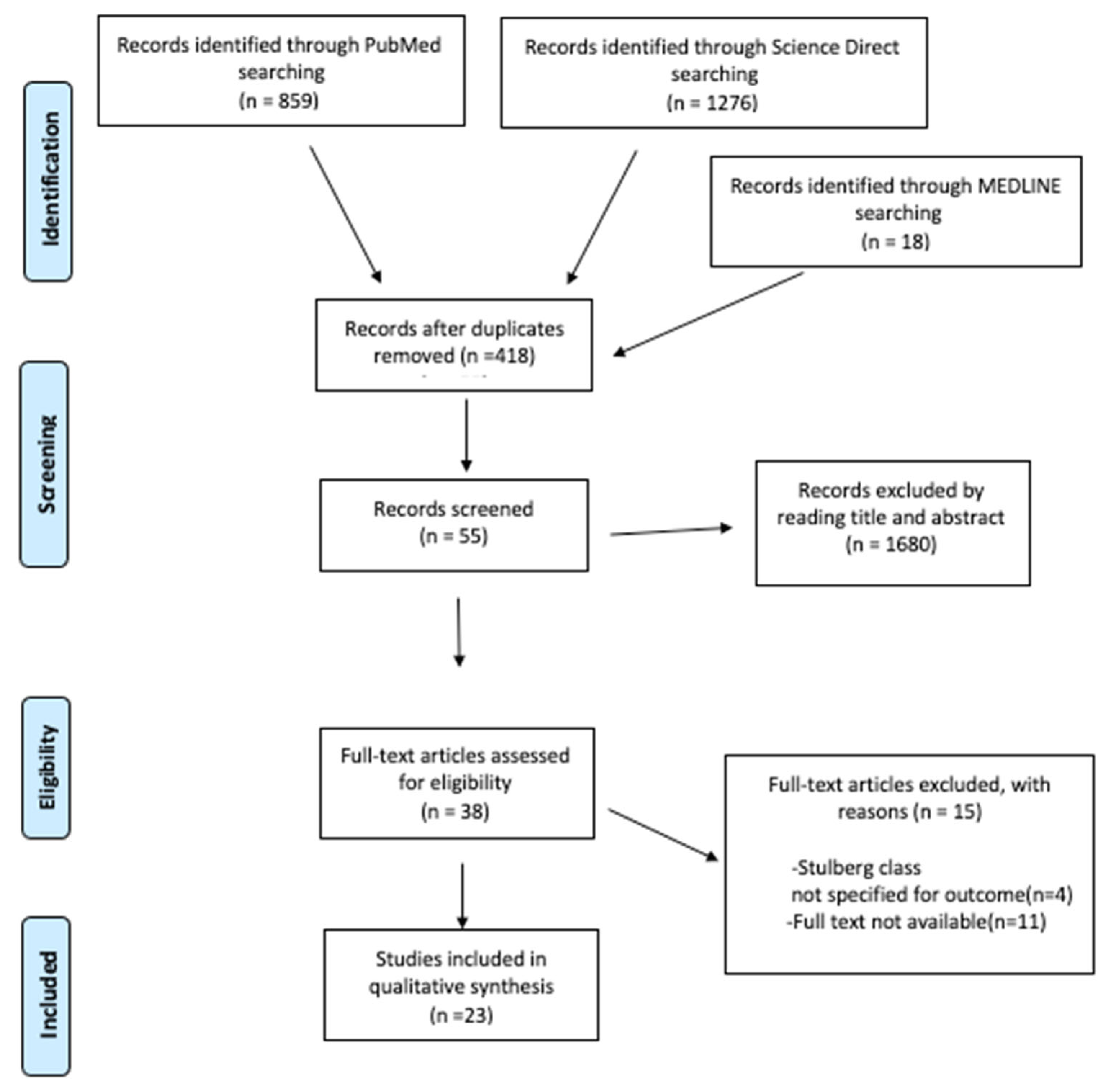
2.1. Search Selection
2.2. Study Selection
2.3. Data Extraction
2.4. Outcome Measures
3. Results
3.1. Demographics
3.2. Surgical Treatment
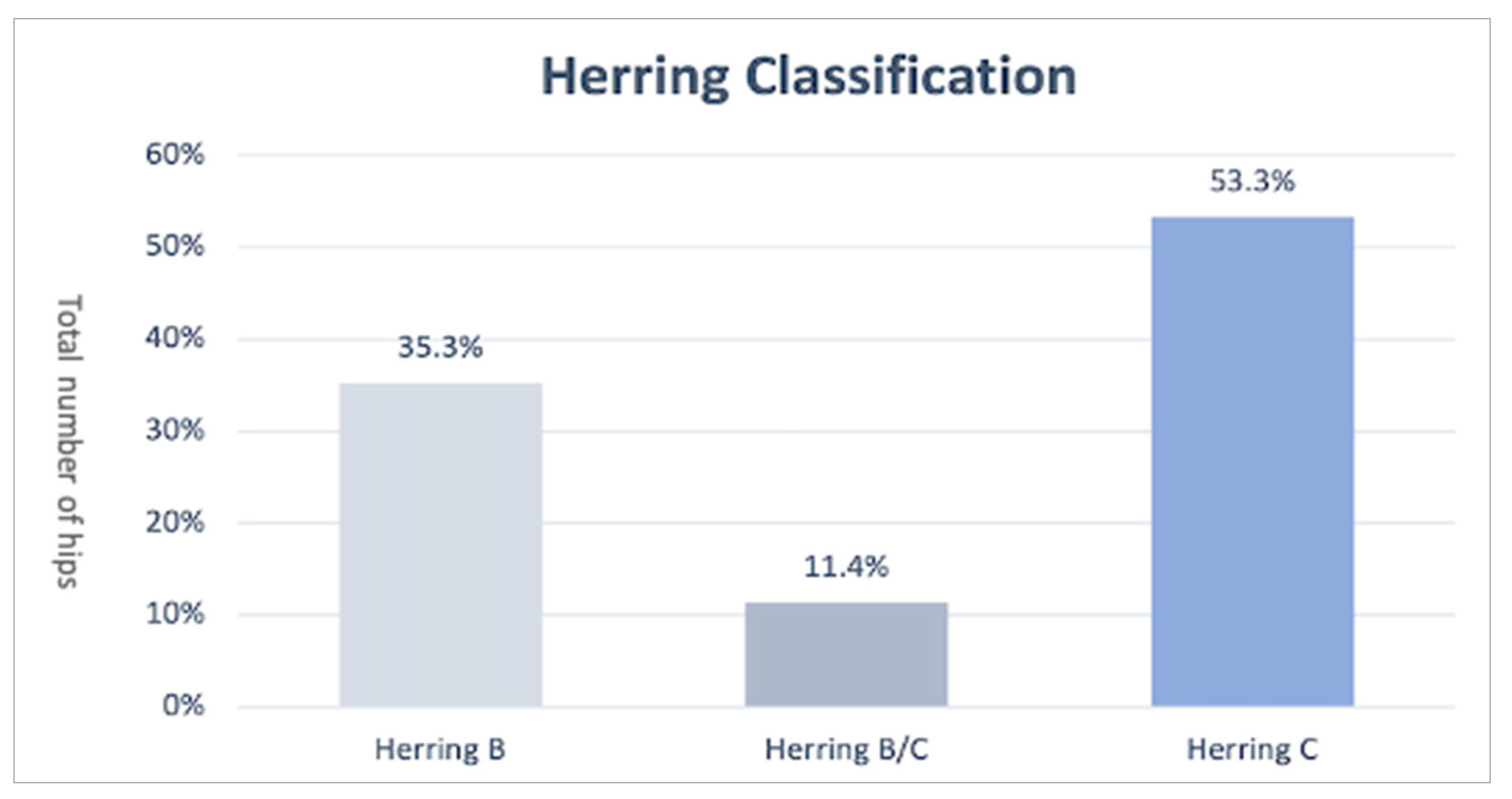
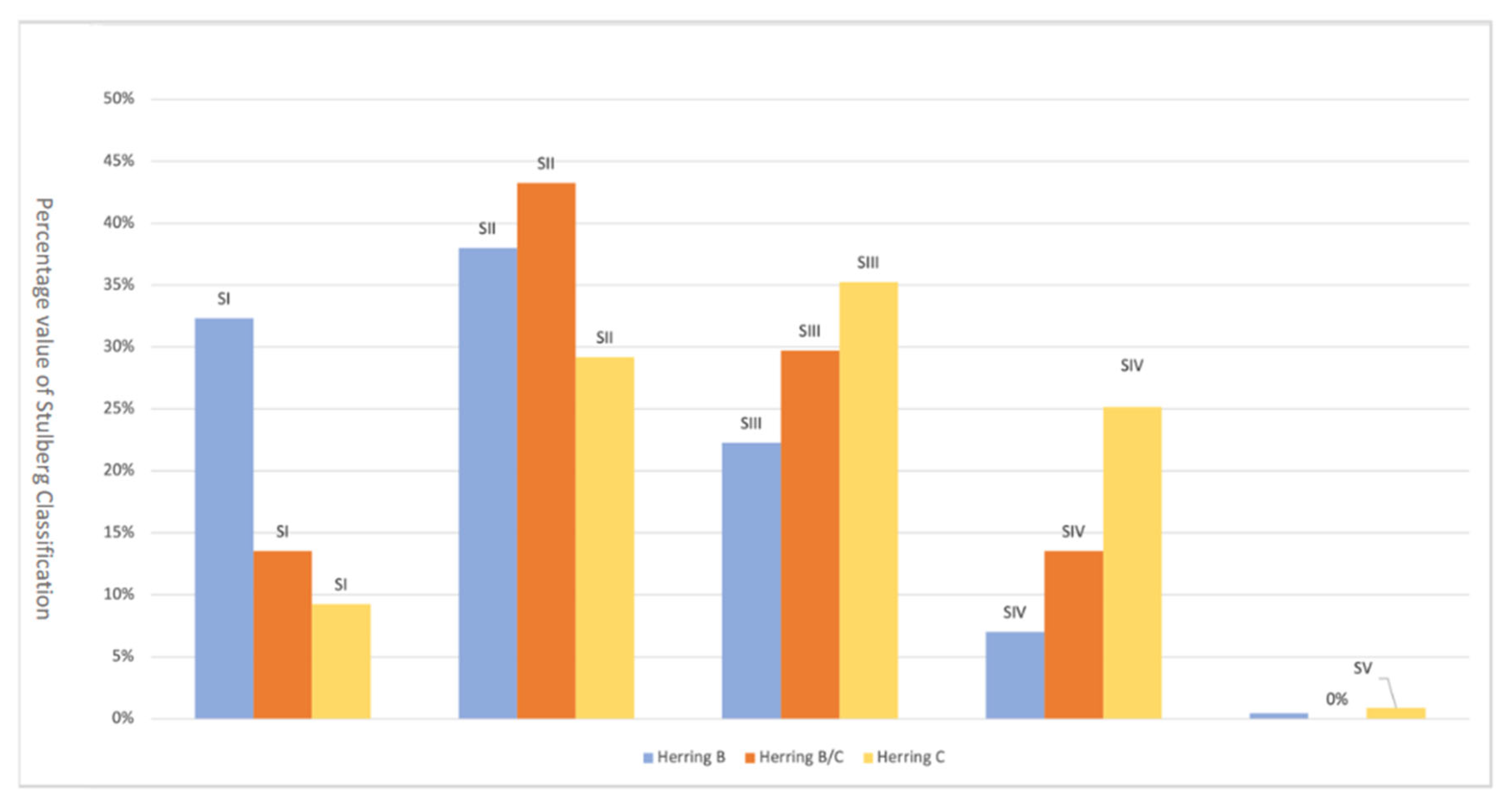
3.3. Herring Classification Related to Stulberg Classification
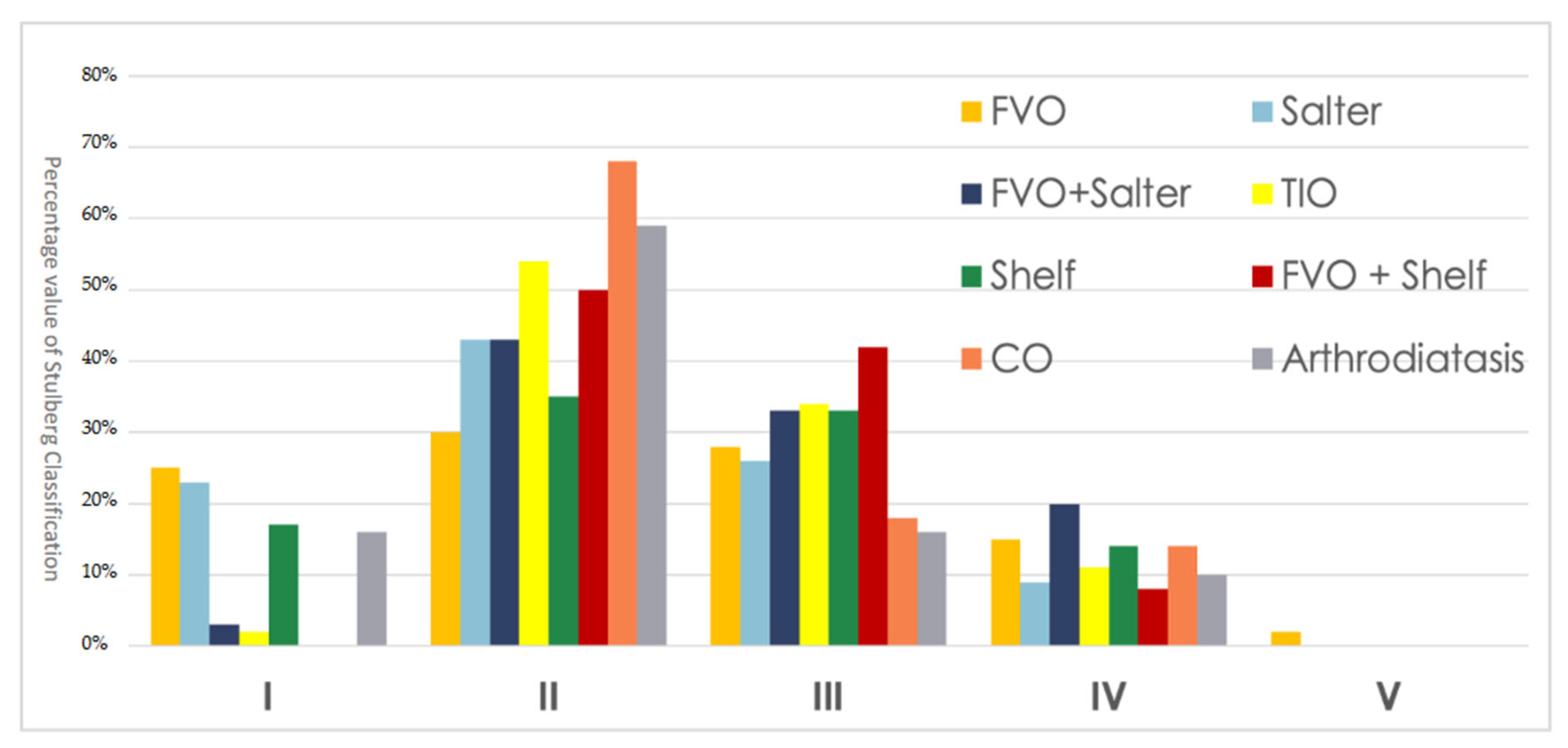
3.4. Radiographic Stulberg Outcome of the Single Surgical Techniques
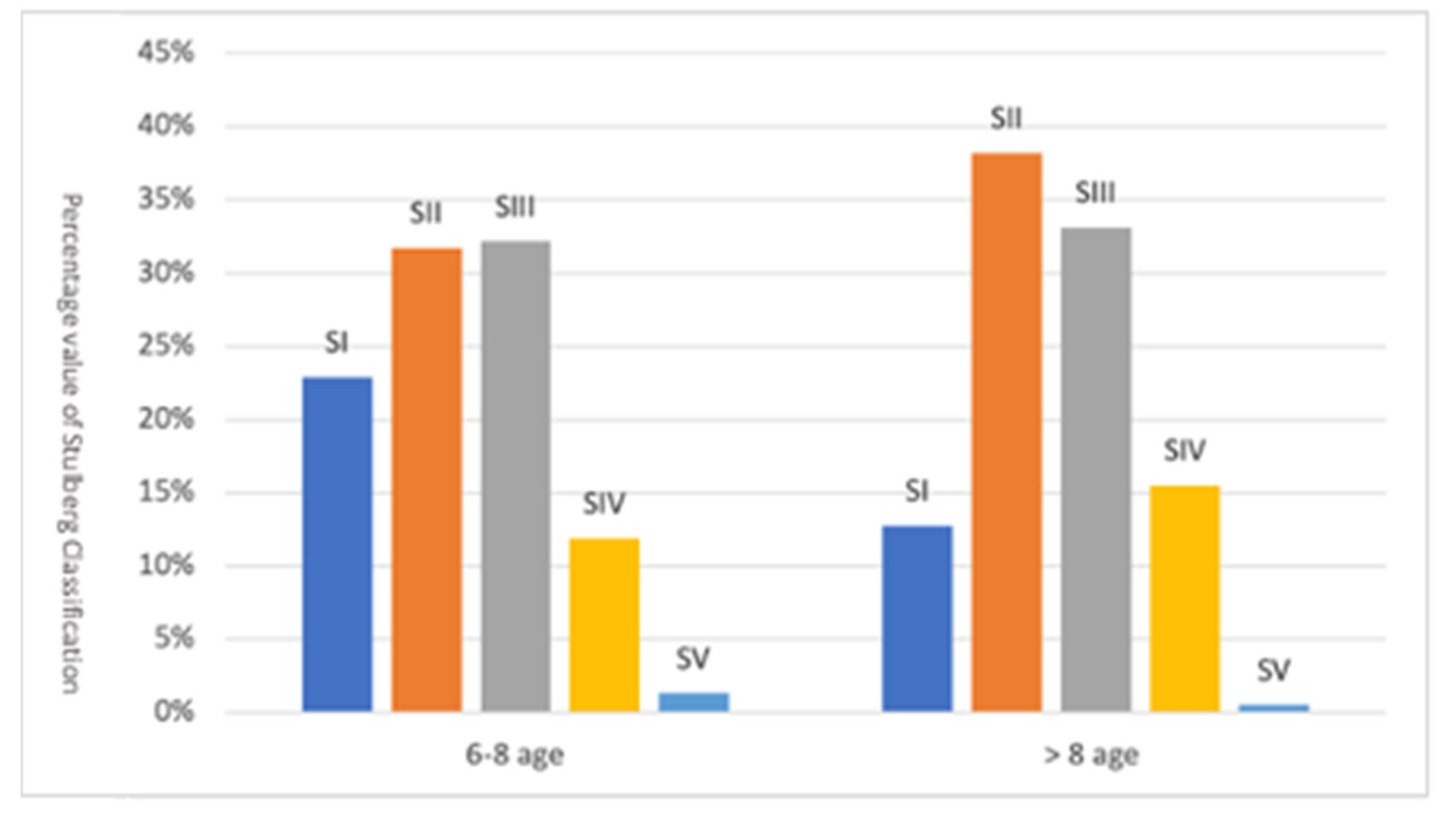
3.5. Radiographic Stulberg Outcome Correct for Age at Onset
3.6. Arthroplasty Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thompson, G.H.; Choi, I.H. Legg-Calve-Perthes Disease Centenary. J. Pediatr. Orthop. 2011, 31, S129. [Google Scholar] [CrossRef] [PubMed]
- Perry, D.C.; Machin, D.M.G.; Pope, D.; Bruce, C.E.; Dangerfield, P.; Platt, M.J.; Hall, A.J. Racial and Geographic Factors in the Incidence of Legg-Calvé-Perthes’ Disease: A Systematic Review. Am. J. Epidemiol. 2012, 175, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Legg, A.T. THE CLASSIC: An Obscure Affection of the Hip Joint. Clin. Orthop. 2006, 451, 11–13. [Google Scholar] [CrossRef]
- Calvé, J. The Classic: On a Particular Form of Pseudo-Coxalgia Associated with a Characteristic Deformity of the Upper End of the Femur. Clin. Orthop. 2006, 451, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Perthes, G. The Classic: On Juvenile Arthritis Deformans. Clin. Orthop. 2012, 470, 2349–2368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavone, V.; Chisari, E.; Vescio, A.; Lizzio, C.; Sessa, G.; Testa, G. Aetiology of Legg-Calvé-Perthes Disease: A Systematic Review. World J. Orthop. 2019, 10, 145–165. [Google Scholar] [CrossRef]
- Al Kaissi, A.; Ghachem, M.B.; Kenis, V.; Melchenko, E.; Grill, F.; Ganger, R.; Kircher, S.G. A Constellation of Orthopaedic Deformities in Connection with Cartilage Oligomeric Matrix Protein Mutation. Afr. J. Paediatr. Surg. AJPS 2019, 16, 23–28. [Google Scholar] [CrossRef]
- Cook, P.C. Transient Synovitis, Septic Hip, and Legg-Calvé-Perthes Disease. Pediatr. Clin. N. Am. 2014, 61, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Lecuire, F. The Long-Term Outcome of Primary Osteochondritis of the Hip (Legg-Calvé-Perthes’ Disease). J. Bone Jt. Surg. Br. 2002, 84-B, 636–640. [Google Scholar] [CrossRef]
- Chell, J.; Flowers, M.J. Stulberg Classification System. J. Bone Jt. Surg. Am. Vol. 2000, 82, 1517. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.; Price, C.T. Principles of Containment Treatment Aimed at Preventing Femoral Head Deformation in Perthes Disease. Orthop. Clin. N. Am. 2011, 42, 317–327. [Google Scholar] [CrossRef]
- Thompson, G.H. Salter Osteotomy in Legg-Calvé-Perthes Disease. J. Pediatr. Orthop. 2011, 31, S192–S197. [Google Scholar] [CrossRef]
- Beer, Y.; Smorgick, Y.; Oron, A.; Mirovsky, Y.; Weigl, D.; Agar, G.; Shitrit, R.; Copeliovitch, L. Long-Term Results of Proximal Femoral Osteotomy in Legg-Calvé-Perthes Disease. J. Pediatr. Orthop. 2008, 28, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; da Cunha, A.M.; Browne, R.; Kim, H.T.; Herring, J.A. How Much Varus Is Optimal with Proximal Femoral Osteotomy to Preserve the Femoral Head in Legg-Calvé-Perthes Disease? J. Bone Jt. Surg.-Am. Vol. 2011, 93, 341–347. [Google Scholar] [CrossRef]
- Leroux, J.; Abu Amara, S.; Lechevallier, J. Legg-Calvé-Perthes Disease. Orthop. Traumatol. Surg. Res. 2018, 104, S107–S112. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating Guidance for Reporting Systematic Reviews: Development of the PRISMA 2020 Statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, J.K.; Weiner, D.S. Radiographic Results of Proximal Femoral Varus Osteotomy in Legg-Calvé-Perthes Disease. J. Pediatr. Orthop. 2000, 20, 566–571. [Google Scholar] [CrossRef]
- Talkhani, I.S.; Moore, D.P.; Dowling, F.E.; Fogarty, E.E. Neck-Shaft Angle Remodelling after Derotation Varus Osteotomy for Severe Perthes Disease. Acta Orthop. Belg. 2001, 67, 248–251. [Google Scholar] [PubMed]
- Noonan, K.J.; Price, C.T.; Kupiszewski, S.J.; Pyevich, M. Results of Femoral Varus Osteotomy in Children Older than 9 Years of Age with Perthes Disease. J. Pediatr. Orthop. 2001, 21, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Van Der Geest, I.C.; Kooijman, M.A.; Spruit, M.; Anderson, P.G.; De Smet, P.M. Shelf Acetabuloplasty for Perthes’ Disease: 12-Year Follow-Up. Acta Orthop. Belg. 2001, 67, 126–131. [Google Scholar]
- Reddy, R.R.; Morin, C. Chiari Osteotomy in Legg–Calvé–Perthes Disease. J. Pediatr. Orthop. B 2005, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, M.C.; Cankus, M.C.; Alanay, A.; Yazici, M.; Caglar, O.; Alpaslan, A.M. Radiological Outcome of Proximal Femoral Varus Osteotomy for the Treatment of Lateral Pillar Group-C Legg-Calvé-Perthes Disease. J. Pediatr. Orthop. Part B 2005, 14, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Sarassa, C.A.; Herrera, A.M.; Carvajal, J.; Gomez, L.F.; Lopez, C.A.; Rojas, A.F. Early Clinical and Radiological Outcomes after Double Osteotomy in Patients with Late Presentation Legg-Calvé-Perthes Disease. J. Child. Orthop. 2008, 2, 425–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, R.T.; Wainwright, A.M.; Theologis, T.N.; Benson, M.K. The Outcome of Patients with Hinge Abduction in Severe Perthes Disease Treated by Shelf Acetabuloplasty. J. Pediatr. Orthop. 2008, 28, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Aly, T.A.; Amin, O.A. Arthrodiatasis for the Treatment of Perthes’ Disease. Orthopedics 2009, 32, 817. [Google Scholar] [CrossRef] [PubMed]
- Javid, M.; Wedge, J.H. Radiographic Results of Combined Salter Innominate and Femoral Osteotomy in Legg-Calvé-Perthes Disease in Older Children. J. Child. Orthop. 2009, 3, 229–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, W.J.; Choi, I.H.; Cho, T.-J.; Chung, C.Y.; Shin, Y.-W.; Shin, S.J. Shelf Acetabuloplasty for Children with Perthes’ Disease and Reducible Subluxation of the Hip: Prognostic Factors Related to Hip Remodelling. J. Bone Jt. Surg. Br. 2009, 91, 1383–1387. [Google Scholar] [CrossRef]
- Ghanem, I.; Haddad, E.; Haidar, R.; Haddad-Zebouni, S.; Aoun, N.; Dagher, F.; Kharrat, K. Lateral Shelf Acetabuloplasty in the Treatment of Legg–Calvé–Perthes Disease: Improving Mid-Term Outcome in Severely Deformed Hips. J. Child. Orthop. 2010, 4, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Pecquery, R.; Laville, J.-M.; Salmeron, F. Legg-Calvé-Perthes Disease Treatment by Augmentation Acetabuloplasty. Orthop. Traumatol. Surg. Res. OTSR 2010, 96, 166–174. [Google Scholar] [CrossRef] [Green Version]
- Hosny, G.A.; El-Deeb, K.; Fadel, M.; Laklouk, M. Arthrodiastasis of the Hip. J. Pediatr. Orthop. 2011, 31, S229–S234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakashima, Y.; Kubota, H.; Yamamoto, T.; Mawatari, T.; Motomura, G.; Iwamoto, Y. Transtrochanteric Rotational Osteotomy for Late-Onset Legg-Calve-Perthes Disease. J. Pediatr. Orthop. 2011, 31, S223–S228. [Google Scholar] [CrossRef]
- Farsetti, P.; Benedetti-Valentini, M.; Potenza, V.; Ippolito, E. Valgus Extension Femoral Osteotomy to Treat “Hinge Abduction” in Perthes’ Disease. J. Child. Orthop. 2012, 6, 463–469. [Google Scholar] [CrossRef] [Green Version]
- Grzegorzewski, A.; Synder, M.; Kmieć, K.; Krajewski, K.; Polguj, M.; Sibiński, M. Shelf Acetabuloplasty in the Treatment of Severe Legg-Calvé-Perthes Disease: Good Outcomes at Midterm Follow-Up. BioMed Res. Int. 2013, 2013, 859483. [Google Scholar] [CrossRef]
- Yavuz, U.; Demir, B.; Yildirim, T.; Beng, K.; Karakas, E.S. Salter Innominate Osteotomy in the Treatment of Late Presentation Perthes Disease. Hip Int. J. Clin. Exp. Res. Hip Pathol. Ther. 2014, 24, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.S.; Shim, J.S. Outcomes of Combined Shelf Acetabuloplasty with Femoral Varus Osteotomy in Severe Legg-Calve-Perthes (LCP) Disease: Advanced Containment Method for Severe LCP Disease. Clin. Orthop. Surg. 2015, 7, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Carsi, B.; Judd, J.; Clarke, N.M.P. Shelf Acetabuloplasty for Containment in the Early Stages of Legg-Calve-Perthes Disease. J. Pediatr. Orthop. 2015, 35, 151–156. [Google Scholar] [CrossRef]
- Li, W.-C.; Xu, R.-J. Lateral Shelf Acetabuloplasty for Severe Legg-Calvé-Perthes Disease in Patients Older than 8 Years: A Mean Eleven-Year Follow-Up. Medicine 2016, 95, e5272. [Google Scholar] [CrossRef] [PubMed]
- Stepanovich, M.; Upasani, V.V.; Bomar, J.D.; Wenger, D.R. Advanced Containment with Triple Innominate Osteotomy in Legg-Calve-Perthes Disease: A Viable Option Even in Severe Cases. J. Pediatr. Orthop. 2017, 37, 563–569. [Google Scholar] [CrossRef]
- Park, K.S.; Cho, K.J.; Yang, H.Y.; Eshnazarov, K.E.; Yoon, T.R. Long-Term Results of Modified Salter Innominate Osteotomy for Legg-Calvé-Perthes Disease. Clin. Orthop. Surg. 2017, 9, 397–404. [Google Scholar] [CrossRef]
- Kollitz, K.M.; Gee, A.O. Classifications in Brief: The Herring Lateral Pillar Classification for Legg-Calvé-Perthes Disease. Clin. Orthop. 2013, 471, 2068–2072. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, N.-A.T.; Klein, G.; Dogbey, G.; McCourt, J.B.; Mehlman, C.T. Operative Versus Nonoperative Treatments for Legg-Calvé-Perthes Disease: A Meta-Analysis. J. Pediatr. Orthop. 2012, 32, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Braito, M.; Wolf, S.; Dammerer, D.; Giesinger, J.; Wansch, J.; Biedermann, R. Global Differences in the Treatment of Legg–Calvé–Perthes Disease: A Comprehensive Review. Arch. Orthop. Trauma Surg. 2021, 141, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Herring, J.A.; Kim, H.T.; Browne, R. Legg-Calve-Perthes Disease. Part I: Classification of Radiographs with Use of the Modified Lateral Pillar and Stulberg Classifications. J. Bone Jt. Surg. Am. 2004, 86, 2103–2120. [Google Scholar] [CrossRef] [Green Version]
- Wiig, O.; Terjesen, T.; Svenningsen, S. Prognostic Factors and Outcome of Treatment in Perthes’ Disease: A prospective study of 368 patients with five-year follow-up. J. Bone Jt. Surg. Br. 2008, 90-B, 1364–1371. [Google Scholar] [CrossRef] [PubMed]
- Maleki, A.; Qoreishy, S.M.; Bahrami, M.N. Surgical Treatments for Legg-Calvé-Perthes Disease: Comprehensive Review. Interact. J. Med. Res. 2021, 10, e27075. [Google Scholar] [CrossRef] [PubMed]
- Vukasinovic, Z.; Slavkovic, S.; Milickovic, S.; Siqeca, A. Combined Salter Innominate Osteotomy with Femoral Shortening Versus Other Methods of Treatment for Legg-Calvé-Perthes Disease. J. Pediatr. Orthop. B 2000, 9, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Olney, B.W.; Asher, M.A. Combined Innominate and Femoral Osteotomy for the Treatment of Severe Legg-Calvé-Perthes Disease. J. Pediatr. Orthop. 1985, 5, 645–651. [Google Scholar] [CrossRef]
- Perpich, M.; McBeath, A.; Kruse, D. Long-Term Follow-up of Perthes Disease Treated with Spica Casts. J. Pediatr. Orthop. 1983, 3, 160–165. [Google Scholar] [CrossRef] [PubMed]
- McAndrew, M.P.; Weinstein, S.L. A Long-Term Follow-up of Legg-Calvé-Perthes Disease. J. Bone Jt. Surg. 1984, 66, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Froberg, L.; Christensen, F.; Pedersen, N.W.; Overgaard, S. The Need for Total Hip Arthroplasty in Perthes Disease: A Long-Term Study. Clin. Orthop. 2011, 469, 1134–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref | Author | N. of Hip | Surgical Treatment | FU (y) | Stulberg Class | N. of THA | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | ||||||
| [17] | Friedlander JK et al. (2000) | 98 | FVO | 6.9 | 31 | 19 | 39 | 7 | 2 | 8 |
| [18] | Talkhani IS et al. (2001) | 16 | FVO | 7 | 3 | 8 | 3 | 2 | 0 | 2 |
| [19] | Noonan KJ et al. (2001) | 18 | FVO | 10 | 3 | 3 | 4 | 8 | 0 | 1 |
| [20] | Van Der Geest IC et al. (2001) | 21 | Shelf | 12 | 3 | 6 | 10 | 2 | 0 | 1 |
| [21] | Reddy RR et al. (2005) | 22 | CO | 6.1 | 0 | 15 | 4 | 3 | 0 | 1 |
| [22] | Aksoy MC et al. (2005) | 26 | FVO | 13.3 | 2 | 4 | 14 | 5 | 1 | 1 |
| [23] | Sarassa CA et al. (2008) | 10 | FVO + SO | 7 | 1 | 5 | 3 | 1 | 0 | 1 |
| [24] | Freeman RT et al. (2008) | 27 | Shelf | 5.2 | 14 | 0 | 10 | 3 | 0 | 1 |
| [25] | Aly TA et al. (2009) | 22 | Arthrodiatasis | 7 | 0 | 20 | 1 | 1 | 0 | - |
| [26] | Javid M et al. (2009) | 20 | FVO + SO | 5.5 | 0 | 6 | 9 | 5 | 0 | - |
| [27] | Yoo WJ et al. (2009) | 25 | Shelf | 6.7 | 1 | 8 | 13 | 3 | 0 | - |
| [28] | Ghanem I et al. (2010) | 30 | Shelf | 9.5 | 5 | 14 | 6 | 5 | 0 | - |
| [29] | Pecquery R et al. (2010) | 21 | Shelf | 4.3 | 2 | 12 | 1 | 5 | 1 | - |
| [30] | Hosny GA et al. (2011) | 29 | Arthrodiatasis | 7.5 | 8 | 9 | 7 | 4 | 1 | - |
| [31] | Nakashima Y et al. (2011) | 14 | TRO | 12 | 0 | 5 | 2 | 7 | 0 | - |
| [32] | Farsetti P et al. (2012) | 16 | TRO | 6.5 | 0 | 2 | 10 | 4 | 0 | - |
| [33] | Grzegorzewski A et al. (2013) | 23 | Shelf | 5.8 | 2 | 13 | 6 | 2 | 0 | - |
| [34] | Yavuz U et al. (2013) | 18 | SO | 6.5 | 2 | 8 | 7 | 1 | 0 | - |
| [35] | Lim KS et al. (2015) | 12 | Shelf + FVO | 10.1 | 0 | 4 | 7 | 1 | 0 | - |
| [36] | Carsi B et al. (2015) | 45 | Shelf | 11 | 4 | 12 | 21 | 7 | 0 | - |
| [37] | Li WC et al. (2016) | 51 | Shelf | 11 | 11 | 19 | 14 | 7 | 0 | - |
| [38] | Stepanovich M et al. (2017) | 56 | TIO | 8.5 | 1 | 35 | 14 | 6 | 0 | - |
| [39] | Park KS et al. (2017) | 29 | SO | 12.9 | 9 | 9 | 8 | 3 | 0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caldaci, A.; Testa, G.; Dell’Agli, E.; Sapienza, M.; Vescio, A.; Lucenti, L.; Pavone, V. Mid–Long-Term Outcomes of Surgical Treatment of Legg-Calvè-Perthes Disease: A Systematic Review. Children 2022, 9, 1121. https://doi.org/10.3390/children9081121
Caldaci A, Testa G, Dell’Agli E, Sapienza M, Vescio A, Lucenti L, Pavone V. Mid–Long-Term Outcomes of Surgical Treatment of Legg-Calvè-Perthes Disease: A Systematic Review. Children. 2022; 9(8):1121. https://doi.org/10.3390/children9081121
Chicago/Turabian StyleCaldaci, Alessia, Gianluca Testa, Eleonora Dell’Agli, Marco Sapienza, Andrea Vescio, Ludovico Lucenti, and Vito Pavone. 2022. "Mid–Long-Term Outcomes of Surgical Treatment of Legg-Calvè-Perthes Disease: A Systematic Review" Children 9, no. 8: 1121. https://doi.org/10.3390/children9081121
APA StyleCaldaci, A., Testa, G., Dell’Agli, E., Sapienza, M., Vescio, A., Lucenti, L., & Pavone, V. (2022). Mid–Long-Term Outcomes of Surgical Treatment of Legg-Calvè-Perthes Disease: A Systematic Review. Children, 9(8), 1121. https://doi.org/10.3390/children9081121