
Specific Learning Disorder in Children and Adolescents, a Scoping Review on Motor Impairments and Their Potential Impacts

Abstract
1. Introduction
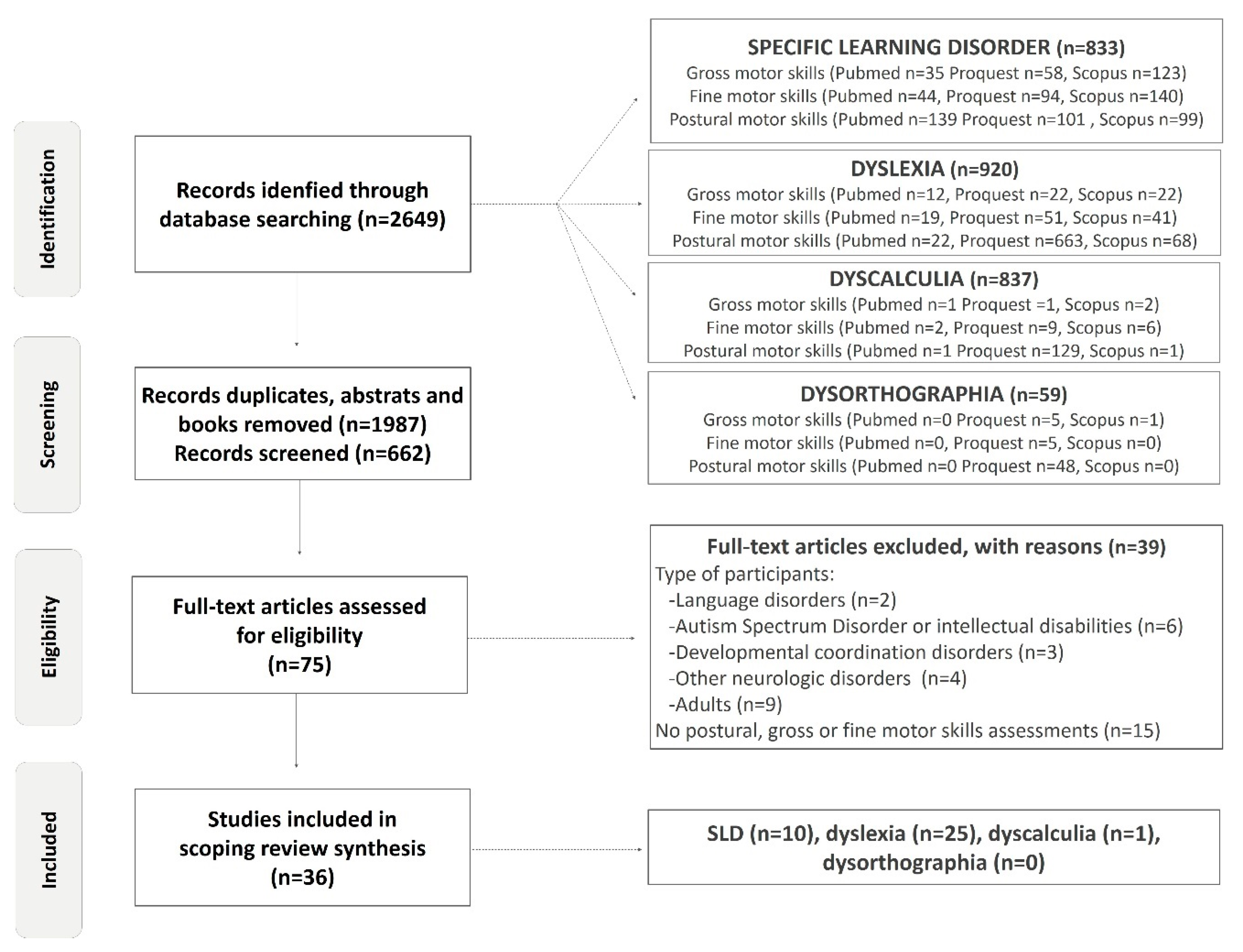
2. Materials and Methods
3. Results
3.1. Motor Assessment Results in Mixed Group of Learning Disabilities
3.1.1. Standard Qualitative Motor Assessment Batteries in Mixed Group of Learning Disabilities
3.1.2. Quantitative Postural Control Assessment in Mixed Group of Learning Disabilities
3.1.3. Quantitative Assessment of Fine Motor Skills in Mixed Group of Learning Disabilities
3.2. Motor Assessment Results in Dyslexia
3.2.1. Standard Qualitative Motor Assessment Batteries in Dyslexia
3.2.2. Quantitative Gross Motor Assessment in Dyslexia
3.2.3. Quantitative Postural Motor Assessment in Dyslexia
3.2.4. Quantitative Assessments of Fine Motor Skills in Dyslexia
3.3. Motor Assessments Results in Dyscalculia
Qualitative Standard Motor Assessment Batteries in Dyscalculia
3.4. Lifestyle Behavior and Physical Fitness in Children and Adolescents with SLD
- (1)
- A total of 73% of participants with an SLD and 39% of participants with an SLD and ADHD were less likely to meet physical activity recommendations than their peers (demographic variables and medication use were controlled).
- (2)
- Participants with an SLD have a significantly higher sedentary rate, i.e., nearly two additional hours per day versus participants with only ADHD.
- (3)
- Preadolescents and adolescents in the three groups (SLD only, ADHD only and SLD/ADHD) were significantly less likely to meet the recommendations for vigorous physical activity compared to their peers (three days per week or more for a minimum of 30 min), both before and after controlling for demographic variables.
- (4)
- Individuals with SLD are 46% more likely to be obese than people with typical development [91].
4. Discussion
4.1. Motor Control Impairments in Children and Adolescents with SLDs without Comorbidities
4.2. Which Motor Mechanisms Are Possibly Altered in SLDs?
4.3. The Necessity to Investigate the Comorbidity
4.4. A Relevant Systematic Clinical Investigation of Motor Skills in Children with SLDs as an Early Indicator of Developmental Process Impairments
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; APA: Washington, DC, USA, 1994; p. 886. [Google Scholar]
- Canadian ADHD Resource Alliance (CADDRA). Canadian ADHD Practice Guidelines, ADHD Also Has a Specific Learning Disability, 4th ed.; CADDRA: Toronto, ON, Canada, 2014; pp. 65–70. [Google Scholar]
- Kulkarni, M.; Kalantre, S.; Upadhyem, S.; Karande, S.; Ahuja, S. Approach to learning disability. Indian J. Pediatr. 2001, 68, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Koppitze, M. The Bender-Gestalt test and learning disturbance in young children. J. Clin. Psychol. 1958, 14, 292–295. [Google Scholar] [CrossRef]
- Pyfer, J.L.; Carlson, B.R. Characteristic motor development of children with learning disabilities. Percept. Mot. Ski. 1972, 35, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Bruininks, V.L.; Bruininks, R.J. Motor proficiency and learning disabled and nondisabled students. Percept. Mot. Ski. 1977, 44, 1131–1137. [Google Scholar] [CrossRef]
- Haubenstricker, J.L. Motor Development in Children with Learning Disabilities. J. Phys. Educ. Recreat. Dance 1982, 53, 41–43. [Google Scholar] [CrossRef]
- Baharudin, N.R.; Harun, D.; Kadar, M. An Assessment of the Movement and Function of Children with Specific Learning Disabilities: A Review of Five Standardised Assessment Tools. J. Med. Sci. 2020, 27, 21–36. [Google Scholar] [CrossRef]
- Rochelle, K.S.H.; Talcott, J.B. Impaired balance in developmental dyslexia? A meta-analysis of the contending evidence. J. Child Psychol. Psychiatry 2006, 47, 1159–1166. [Google Scholar] [CrossRef]
- Quercia, P.; Seigneuric, A.S.; Chariot, P.; Vernet, T.; Pozzo, A.; Bron, C.; Creuzot-Garcher; Robichon, F. Ocular proprioception and developmental dyslexia. Sixty clinical observations. J. Fr. Ophtalmol. 2005, 28, 713–723. [Google Scholar] [CrossRef]
- Westendorp, M.; Hartman, E.; Houwen, S.; Smith, J.; Visscher, C. The relationship between gross motor skills and academic achievement in children with learning disabilities. Res. Dev. Disabil. 2011, 32, 2773–2779. [Google Scholar] [CrossRef]
- Westendorp, M.; Hartman, E.; Houwen, S.; Huijgen, B.C.; Smith, J.; Visscher, C.A. Longitudinal study on gross motor development in children with learning disorders. Res. Dev. Disabil. 2014, 35, 357–363. [Google Scholar] [CrossRef]
- Cignetti, F.; Vaugoyeau, M.; Fontan, A.; Joverd, M.; Livete, M.-O.; Hugonenq, C.; Audic, F.; Chabrol, B.; Assaiante, C. Feedforward motor control in developmental dyslexia and developmental coordination disorder: Does comorbidity matter? Res. Dev. Disabil. 2018, 76, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, R.; Vaugoyeau, M.; Colé, P.; Assaiante, C. Effet de la comorbidité sensorimotrice dans la dyslexie développementale: Entre déficit phonologique et atteinte des représentations internes de l’action. ANAE 2021, 33, 689–699. [Google Scholar]
- Galli, M.; Vimercati, S.L.; Giacomo, S.; Caiazzo, G.; Norveti, F.; Onnis, F.; Rigoldi, C.; Albertini, G. A new approach for the quantitative evaluation of drawings in children with learning disabilities. Res. Dev. Disabil. 2011, 32, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Cignetti, F.; Nemmi, F.; Vaugoyeau, M.; Girard, N.; Albaret, J.-M.; Chaix, Y.; Péran, P.; Assaiante, C. Intrinsic Cortico-Subcortical Functional Connectivity in Developmental Dyslexia and Developmental Coordination Disorder. Cereb. Cortex 2020, 1, tgaa011. [Google Scholar] [CrossRef]
- Rae, C.; Harasty, J.A.; Dzendrowskyj, T.E.; Talcott, J.B.; Simpson, J.M.; Blamire, A.; Dixon, R.M.; Lee, M.A.; Thompson, C.H.; Styles, P.; et al. Cerebellar morphology in developmental dyslexia. Neuropsychologia 2002, 40, 1285–1292. [Google Scholar] [CrossRef]
- Eckert, M.A.; Leonard, C.M.; Richards, T.L.; Aylward, E.H.; Thomson, J.; Berninger, V.W. Anatomical correlates of dyslexia: Frontal and cerebellar findings. Brain 2003, 126, 482–1144. [Google Scholar] [CrossRef]
- Ibrahim, S.; Harun, D.; Kadar, M.; Mohd Rasdi, H.F.; Baharudin, N.S.; Jong Tze Hui, E. Motor performance and functional mobility in children with specific learning disabilities. Med. J. Malaysia 2019, 74, 34–39. [Google Scholar]
- Barnett, L.M.; Lai, S.K.; Veldman, S.L.C.; Hardy, L.L.; Cliff, D.P.; Morgan, P.J.; Zask, A.; Lubans, D.R.; Shultz, N.S.P. Correlates of Gross Motor Competence in Children and Adolescents: A Systematic Review and Meta Analysis. Sports Med. 2016, 46, 1663–1688. [Google Scholar] [CrossRef]
- Johnston, M.V. Plasticity in the developing brain: Implications for rehabilitation. Dev. Disabil. Res. Rev. 2009, 15, 94–101. [Google Scholar] [CrossRef]
- Ismail, F.Y.; Fatemi, A.; Johnston, M.V. Cerebral plasticity: Windows of opportunity in the developing brain. Eur. J. Paediatr. Neurol. 2017, 21, 23–48. [Google Scholar] [CrossRef]
- Blanchet, M.; Prince, F. Development of mediolateral postural control mechanisms and proprioception were accelerated by kicking sports training in adolescents. J. Pediatr. Exerc. Sci. 2022; sous presse. [Google Scholar]
- Sommeijer, J.P.; Ahmadlou, M.; Saiepour, M.H. Thalamic inhibition regulates critical-period plasticity in visual cortex and thalamus. Nat. Neurosci. 2017, 20, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Kalogeraki, E.; Pielecka-Fortuna, J.; Löwel, S. Environmental enrichment accelerates ocular dominance plasticity in mouse visual cortex whereas transfer to standard cages resulted in a rapid loss of increased plasticity. PLoS ONE 2017, 26, e0186999. [Google Scholar] [CrossRef] [PubMed]
- Paillard, T. Plasticity of the postural function to sport and/or motor experience. Neurosci. Biobehav. Rev. 2017, 72, 129–152. [Google Scholar] [CrossRef] [PubMed]
- Fontan, A.; Cignetti, F.; Nazarian, B.; Anton, J.L.; Vaugoyeau, M.; Assaiante, C. How does the body representation system develop in the human brain? Dev. Cogn. Neurosci. 2017, 24, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Goodway, J.; Langendorfer, S.J.; Roberton, M.A. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. NAKHE 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Lopes, L.; Santos, R.; Pereira, B.; Lopes, V.P. Associations between gross motor coordination and academic achievement in elementary school children. Hum. Mov. Sci. 2013, 32, 9–20. [Google Scholar] [CrossRef]
- Son, S.H.; Meisels, S.J. The relationship of young children’s motor skills to later reading and math achievement. Merrill-Palmer Q. 2006, 52, 755–778. [Google Scholar] [CrossRef]
- Soares, D.B.; Porto, E.; Marco, A.; Azoni, C.A.; Capelatto, I.V. Influence of the physical activity on motor performance of children with learning difficulties. Rev. CEFAC 2015, 17, 1132–1142. [Google Scholar] [CrossRef]
- Suggate, S.; Pufke, E.; Stoeger, H. Do fine motor skills contribute to early reading development? J. Res. Read. 2018, 41, 1–19. [Google Scholar] [CrossRef]
- Rivilis, I.; Hay, J.; Cairney, J.; Klentrou, P.; Liu, J.; Faught, B.E. Physical activity and fitness in children with developmental coordination disorder: A systematic review. Res. Dev. Disabil. 2011, 32, 894–910. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/fr (accessed on 27 May 2022).
- Grigorenko, E.L.; Donald, C.; Fuchs, L.; Wagner, R.; Willcutt, E.; Fletcher, J.M. Understanding, Educating, and Supporting Children with Specific Learning Disabilities: 50 Years of Science and Practice. Am. Psychol. 2020, 75, 37–51. [Google Scholar] [CrossRef] [PubMed]
- Zoia, S.; Barnett, A.; Wilson, P.; Hill, E. Special Issue: Developmental Coordination Disorder: Current Issues. Child Care Health Dev. 2006, 32, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, B.J.; Wilson, B.N.; Dewey, D.M.; Crawford, S.G. DCD may not be a discrete disorder. Hum. Mov. Sci. 1998, 17, 471–490. [Google Scholar] [CrossRef]
- Hussein, Z.A.; Abdel-Aty, S.A.-R.; Elmeniawy, G.H.; Mahgoub, E.A.-M. Defects of motor performance in children with different types of specific learning disability. Drug Invent. Today 2020, 14, 303–307. [Google Scholar]
- Vuijk, P.J.; Hartman, E.; Mombarg, R.; Scherder, E.; Visscher, C. Associations between academic and motor performance in a heterogeneous sample of children with Learning Disabilities. J. Learn. Disabil. 2011, 44, 276–282. [Google Scholar] [CrossRef]
- Poblano, A.; Ishiwara, K.; de Lourdes Arias, M.; García-Pedroza, F.; Marín, H.; Trujillo, M. Motor control alteration in posturography in learning-disabled children. Arch. Med. Res. 2002, 33, 485–488. [Google Scholar] [CrossRef]
- Blanchet, M.; Guetiti, S.; Cadoret, G. Limits of stability and postural control stability in children with learning disorders. ISEK, 2022; in review. [Google Scholar]
- Okuda, P.M.M.; Pinheiro, F.H. Motor Performance of Students with Learning Difficulties Procedia. Soc. Behav. Sci. 2015, 174, 1330–1338. [Google Scholar] [CrossRef][Green Version]
- Jongmans, M.J.; Bouwien, C.; Smits-Engelsman, M.; Schoemaker, M.M. Consequences of Comorbidity of Developmental Coordination Disorders and Learning Disabilities for Severity and Pattern of Perceptual–Motor Dysfunction. J. Learn. Disabil. 2003, 36, 528–537. [Google Scholar] [CrossRef]
- Getchell, N.; Pabreja, P.; Neeld, K.; Carrio, V. Comparing children with and without dyslexia on the Movement Assessment Battery for Children and the Test of Gross Motor Development. Percept. Mot. Ski. 2007, 105, 207–214. [Google Scholar] [CrossRef]
- Marchand-Krynski, M.-È.; Morin-Moncet, O.; Bélanger, A.-M.; Beauchamp, M.-H.; Leonard, G. Shared and differentiated motor skill impairments in children with dyslexia and/or attention deficit disorder: From simple to complex sequential coordination. PLoS ONE 2017, 19, e0177490. [Google Scholar] [CrossRef]
- Moe-Nilssen, R.; Helbostad, J.L.; Talcott, J.B.; Toennessen, F.E. Balance and gait in children with dyslexia. Exp. Brain Res. 2003, 150, 237–244. [Google Scholar] [CrossRef] [PubMed]
- McPhillips, M.; Sheehy, N. Prevalence of persistent primary reflexes and motor problems in children with reading difficulties. Dyslexia 2004, 10, 316–338. [Google Scholar] [CrossRef] [PubMed]
- Iversen, S.; Berg, K.; Ellertsen, B.; Tønnessen, F.-E. Motor coordination difficulties in a municipality group and in a clinical sample of poor readers. Dyslexia 2005, 11, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Barela, J.A.; Tesima, N.; Amaral, V.D.S.; Figueiredo, G.A.; Barela, A.M.F. Visually guided eye movements reduce postural sway in dyslexic children. Neurosci. Lett. 2020, 725, 134890. [Google Scholar] [CrossRef] [PubMed]
- Brookes, R.L.; Tinkler, S.; Nicolson, R.I.; Fawcett, A.J. Striking the right balance: Motor difficulties in children and adults with dyslexia. Dyslexia 2010, 16, 358–373. [Google Scholar] [CrossRef]
- Viana, A.R.; Razuk, M.; de Freitas, P.B.; Barela, J.A. Sensorimotor Integration in Dyslexic Children under Different Sensory Stimulations. PLoS ONE 2013, 8, e72719. [Google Scholar] [CrossRef]
- Barela, J.A.; Dias, J.L.; Godoi, D.; Viana, A.R.; de Freitas, P.B. Postural control and automaticity in dyslexic children: The relationship between visual information and body sway. Res. Dev. Disabil. 2011, 32, 1814–1821. [Google Scholar] [CrossRef]
- Razuk, M.; Barela, J.A. Dyslexic Children Suffer from Less Informative Visual Cues to Control Posture. Res. Dev. Disabil. 2014, 35, 1988–1994. [Google Scholar] [CrossRef]
- Razuk, M.; Lukasova, K.; Bucci, M.P.; Barela, J.A. Dyslexic children need more robust information to resolve conflicting sensory situations. Dyslexia 2020, 26, 52–66. [Google Scholar] [CrossRef]
- Goulème, N.; Gerard, C.L.; Bui-Quoc, E.; Bucci, M.P. Spatial and temporal analysis of postural control in dyslexic children. Clin. Neurophysiol. 2015, 126, 1370–1377. [Google Scholar] [CrossRef]
- Okuda, P.M.M.; Ramos, F.G.; Santos, L.C.A.; Padula, N.; Kirby, A.; Capellini, S.A. Motor profiles of students with dyslexia. Psychol. Res. 2014, 4, 31–39. [Google Scholar]
- Razuk, M.; Barela, J.A.; Peyre, H.; Gerard, C.L.; Bucci, M.P. Eye movements and postural control in dyslexic children performing different visual tasks. PLoS ONE 2018, 24, e0198001. [Google Scholar] [CrossRef] [PubMed]
- Bucci, M.P.; Goulème, N.; Stordeur, C.; Acquaviva, E.; Scheid, I.; Lefebvre, A.; Gerard, C.-L.; Peyre, H.; Delorme, R. Discriminant validity of spatial and temporal postural index in children with neurodevelopmental disorders. Int. J. Dev. Neurosci. 2017, 61, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Goulème, N.; Villeneuve, P.; Gérard, C.L.; Bucci, M.P. Influence of both cutaneous input from the foot soles and visual information on the control of postural stability in dyslexic children. Gait Posture 2017, 56, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Ramus, F.; Pidgeon, E.; Frith, U. The relationship between motor control and phonology in dyslexic children. J. Child Psychol. Psychiatry 2003, 44, 712–722. [Google Scholar] [CrossRef]
- Legrand, A.; Bui-Quoc, E.; Doré-Mazars, K.; Lemoine, C.; Gérard, C.-L.; Bucci, M.P. Effect of a dual task on postural control in dyslexic children. PLoS ONE 2012, 7, e35301. [Google Scholar] [CrossRef]
- Kapoula, Z.; Bucci, M.P. Postural control in dyslexic and non-dyslexic children. J. Neurol. 2007, 254, 1174–1183. [Google Scholar] [CrossRef]
- Lam, S.S.T.; Au, R.K.C.; Leung, H.W.H.; Li-Tsang, C.W.P. Chinese handwriting performance of primary school children with dyslexia. Res. Dev. Disabil. 2011, 32, 1745–1756. [Google Scholar] [CrossRef]
- Niechwiej-Szwedo, E.; Alramis, F.; Christian, L.W. Association between fine motor skills and binocular visual function in children with reading difficulties. Hum. Mov. Sci. 2017, 56, 1–10. [Google Scholar] [CrossRef]
- Wolff, P.H.; George, F.M.; Marsha, O.; Drake, C. Rate and Timing Precision of Motor Coordination in Developmental Dyslexia. Dev. Psychol. 1990, 26, 82–89. [Google Scholar] [CrossRef]
- Naz, S.; Najam, N. Neurological deficits and comorbidity in children with reading disorder. Psychiatr. Clin. Psychopharmacol. 2019, 29, 674–681. [Google Scholar] [CrossRef]
- Haouès, M.M.M.; Rahmab, A.; Walidc, O. Study on postural control of dyslexic versus normal-reading children. Rev. Podol. 2021, 17, 18–22. [Google Scholar] [CrossRef]
- Pieters, S.; Desoete, A.; Roeyers, H. Behind mathematical learning disabilities: What about visual perception and motor skills? Learn. Individ. Differ. 2012, 22, 498–504. [Google Scholar] [CrossRef]
- Kulkarni, S.K.; Naidu, P.S. Tardive dyskinesia: An update. Drugs Today 2001, 37, 97–119. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, D.A. Test of Gross Motor Development; Pro-Edinc: Austin, TX, USA, 1985. [Google Scholar]
- Ulrich, D.A. Test of Gross Motor Development, 2nd ed.; Pro-Edinc: Austin, TX, USA, 2000. [Google Scholar]
- Bluechardt, M.; Shephard Roy, J. Motor performance impairment in students with learning disability: Influence of gender and body build. BMC Sports Sci. Med. Rehabil. 1996, 7, 133–140. [Google Scholar] [CrossRef]
- Okuda, P.M.; Pinheiro, F.H.; Germano, G.D.; Padula, N.A.; Lourencetti, M.D.; Santos, L.C.; Capellini, S.A. Screening for Motor Dysgraphia in Public Schools. J. Soc. Bras. Fonoaudiol. 2011, 23, 351–357. [Google Scholar] [CrossRef]
- Capellini, S.A.; Coppede, A.C.; Valle, T.R. Fine motor function of school-aged children with dyslexia, learning disability and learning difficulties. Pró-Fono Rev. Atual. Cient. 2010, 22, 201–208. [Google Scholar] [CrossRef]
- Fawcett, A.J.; Nicolson, R.I.; Dean, P. Impaired performance of children with dyslexia on a range of cerebellar tasks. Ann. Dyslexia 1996, 46, 259–283. [Google Scholar] [CrossRef]
- Laprevotte, J.; Papaxanthis, C.; Saltarelli, S.; Quercia, P.; Gaveau, J. Movement detection thresholds reveal proprioceptive impairments in developmental dyslexia. Sci. Rep. 2021, 11, 299. [Google Scholar] [CrossRef]
- Van Hecke, R.; Danneels, M.; Dhooge, I.; Van Waelvelde, H.; Wiersema, J.R.; Deconinck, F.J.A.; Maes, L. Vestibular Function in Children with Neurodevelopmental Disorders: A Systematic Review. J. Autism Dev. Disord. 2019, 49, 3328–3350. [Google Scholar] [CrossRef]
- Craity, B.J. Physical Expressions of Intelligence; Prentice-Hall: Englewood Cliffs, NJ, USA, 1972. [Google Scholar]
- Maloyc, F.; Sattlerj, M. Motor and cognitive proficiency of learning disabled and normal children. J. Sch. Psychol. 1979, 17, 213–218. [Google Scholar] [CrossRef]
- Lipowska, M.; Czaplewska, E.; Wysocka, A. Visuospatial deficits of dyslexic children. Med. Sci. Monit. 2011, 17, CR216–CR221. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pozzo, T.; Vernet, P.; Creuzot-Garcher, C.; Robichon, F.; Bron, A.; Quercia, P. Static postural control in children with developmental dyslexia. Neurosci. Lett. 2006, 7, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Gashaj, V.; Oberer, N.; Mast, F.W.; Roebers, C.M. Individual differences in basic numerical skills: The role of executive functions and motor skills. J. Exp. Child Psychol. 2019, 182, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Luo, Z.; Jose, P.E.; Huntsinger, C.S.; Pigott, T.D. Fine motor skills and mathematics achievement in East Asian American and European American kindergartners and first graders. Br. J. Dev. Psychol. 2007, 25, 595–614. [Google Scholar] [CrossRef]
- Magistro, D.; Bardaglio, G.; Rabaglietti, E. Gross motor skills and academic achievement in typically developing children: The mediating effect of ADHD related behaviours. Cogn. Brain Behav. Interdiscip. J. 2015, 19, 149–163. [Google Scholar]
- Robinson, L.E.; Wadsworth, D.D.; Peoples, C.M. Correlates of School-Day Physical Activity in Preschool Students. Res. Q. Exerc. Sport 2012, 83, 20–26. [Google Scholar] [CrossRef]
- Kumari, P.; Raj, P. Role of Physical Activity in Learning Disability—A Review. Clin. Exp. Psychol. 2016, 2, 1–3. [Google Scholar] [CrossRef]
- Barnett, L.M.; van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Childhood motor skill proficiency as a predictor of adolescent physical activity. J. Adolesc. Health 2009, 44, 252–259. [Google Scholar] [CrossRef]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sports Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef]
- Burton, N. How can we help people with learning disabilities engage more in meaningful activities? Learn. Disabil. Elf 2016. Available online: https://www.nationalelfservice.net/populations-and-settings/quality-of-life/how-can-we-help-people-with-learning-disabilities-engage-more-in-meaningful-activities/ (accessed on 20 January 2022).
- Emerson, E.; Baines, S. Health Inequalities & People with Learning Disabilities in the UK. Tizard Learn. Disabil. Rev. 2011, 16, 42–48. [Google Scholar]
- Cook, B.G.; Li, D.; Heinrich, K.M. Obesity, physical activity, and sedentary behavior of youth with learning disabilities and ADHD. J. Learn. Disabil. 2015, 48, 563–576. [Google Scholar] [CrossRef]
- Cairney, J.; Hay, J.A.; Faught, B.E.; Flouris, A.; Klentrou, P. Developmental coordination disorder and cardiorespiratory fitness in children. Pediatr. Exerc. Sci. 2007, 19, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Cairney, J.; Veldhuizen, S.; King-Dowling, S.; Faught, B.E.; Hay, J. Tracking cardiorespiratory fitness and physical activity in children with and without motor coordination problems. J. Sci. Med. Sport 2017, 20, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Hollins, S. Meeting the needs of patients with learning disabilities. BMJ 2013, 346, f3421. [Google Scholar] [CrossRef]
- McGuigan, M.S.; Hollins, S.; Attard, M. Age-specific standardized mortality rates in people with learning disability. JIDR 1995, 39, 527–531. [Google Scholar] [CrossRef]
- Cantell, M.; Crawford, S.G.; Doyle-Baker, P.K. Physical fitness and health indices in children, adolescents and adults with high or low motor competence. Hum. Mov. Sci. 2008, 27, 344–362. [Google Scholar] [CrossRef]
- Humphrey, N.; Mullins, P.M. Self-concept and self-esteem in developmental dyslexia. J. Res. Spéc. Educ. Needs 2002, 2. [Google Scholar] [CrossRef]
- Zadina, J.N.; Corey, D.M.; Casbergue, R.M.; Lemen, L.C.; Rouse, J.C.; Knaus, T.A.; Foundas, A.L. Lobar Asymmetries in Subtypes of Dyslexic and Control Subjects. J. Child Neurol. 2006, 21, 917–922. [Google Scholar] [CrossRef]
- Rintala, P.; Linjala, J. Scores on test of gross motor development of children with dysphasia: A pilot study. Percept. Mot. Ski. 2003, 97, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, K.; Milne, N.; Orr, R.; Pope, R. Relationships between motor proficiency and academic performance in mathematics and reading in school-aged children and adolescents: A systematic review. Int. J. Environ. Res. 2018, 15, 1603. [Google Scholar] [CrossRef] [PubMed]
- Hynd, G.W.; Semrud-Clikeman, M. Dyslexia and brain morphology. Psychol. Bull. 1989, 106, 447–482. [Google Scholar] [CrossRef]
- Filipek, P.A. Neurobiologic correlates of developmental dyslexia: How do dyslexics’ brains differ from those of normal readers? J. Child Neurol. 1995, 10, S62–S68. [Google Scholar] [CrossRef]
- Leonard, C.M.; Lombardino, L.J.; Walsh, K.; A Eckert, M.; Mockler, J.L.; A Rowe, L.; Williams, S.; DeBose, C.B. Anatomical risk factors that distinguish dyslexia from SLI predict reading skill in normal children. J. Commun. Disord. 2002, 35, 501–531. [Google Scholar] [CrossRef]
- Hazzaa, N.; Shalaby, A.; Hassanein, S.; Naeem, F.; Khattab, A.; Metwally, N. Assesment of balance functions and primitive reflexes in children with learning disability. Ain Shams Med. J. 2021, 72, 97–103. [Google Scholar] [CrossRef]
- Morasso, P.G.; Schieppati, M. Can Muscle Stiffness Alone Stabilize Upright Standing? J. Neurophysiol. 1999, 82, 1622–1626. [Google Scholar] [CrossRef]
- Jover, M.; Ducrot, S.; Huau, A.; Bellocchi, S.; Brun-Hénin, F.; Mancini, J. Les troubles moteurs chez les enfants dyslexiques: Revue de travaux et perspectives. Enfance 2013, 4, 323–347. [Google Scholar]
- Lukasova, K.; Silva, I.P.; Macedo, E. Impaired Oculomotor Behavior of Children with Developmental Dyslexia in Antisaccades and Predictive Saccades Tasks. Front. Psychol. 2016, 7, 987. [Google Scholar] [CrossRef]
- Stoodley, C.J.; Talcott, J.B.; Carter, E.L.; Witton, C.; Stein, J.F. Selective deficits of vibrotactile sensitivity in dyslexic readers. Neurosci. Lett. 2000, 295, 13–16. [Google Scholar] [CrossRef]
- Wright, B.A.; Bowen, R.W.; Zecker, S.G. Nonlinguistic perceptual deficits associated with reading and language disorders. Curr. Opin. Neurobiol. 2000, 10, 482–486. [Google Scholar] [CrossRef]
- Stein, J. The magnocellular theory of developmental dyslexia. Dyslexia 2001, 7, 12–36. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, R.I.; Fawcett, A.J.; Dean, P. Developmental dyslexia: The cerebellar deficit hypothesis. Trends Neurosci. 2001, 24, 508–511. [Google Scholar] [CrossRef]
- Reiter, A.; Tucha, O.; Lange, K.W. Executive functions in children with dyslexia. Dyslexia 2005, 11, 116–131. [Google Scholar] [CrossRef]
- Nicolson, R.I.; Fawcett, A.J. Automaticity: A new framework for dyslexia research? Cognition 1990, 35, 159–182. [Google Scholar] [CrossRef]
- Nicolson, R.I.; Fawcett, A.J.; Berry, E.L.; Jenkins, H.I.; Dean, P.; Brooks, D.J. Association of abnormal cerebellum activation with motor learning difficulties in dyslexic adults. Lancet 1999, 15, 1662–1667. [Google Scholar] [CrossRef]
- Assaiante, C.; Barlaam, F.; Cignetti, F.; Vaugoyeau, M. Building of body schema during childhood and adolescence: A neurosensory approach. Neurophysiol. Clin. 2014, 44, 3–12. [Google Scholar] [CrossRef]
- Assaiante, C. Faire avec son corps qui change: Construction du schéma corporel chez l’enfant et l’adolescent. “Corps, espaces et apprentissages chez l’enfant et l’adolescent” Numéro spécial. ANAE 2020, 168, 535–542. [Google Scholar]
- Vaivre-Douret, L.; Mazeau, M.; Jolly, C.; Huron, C.; Arnaudi, C.; Gonzalez-Monge, S.; Assaiante, C. L’expertise collective de l’Inserm sur le trouble développemental de la coordination ou dyspraxie: État des principaux travaux et recommandations. Neuropsychiatr. L’enfance L’adolescence 2021, 69, 311–330. [Google Scholar] [CrossRef]
- Beaton, A.A. Dyslexia and the cerebellar deficit hypothesis. Cortex 2002, 38, 479–490. [Google Scholar] [CrossRef]
- Pope, D.H.; Whiteley, H. The lost boys? A case-history view of very able children with dyslexia. In Psychology, Proceedings of the British Psychological Society (BPS) Education Section Conference, Liverpool, UK, 23–24 October 2003; British Psychological Society: London, UK, 2003. [Google Scholar]
- Margari, L.; Buttiglione, M.; Craig, F.; Cristella, A.; de Giambattista, C.; Matera, E.; Operto, F.; Simone, M. Neuropsychopathological comorbidities in learning disorders. BMC Neurol. 2013, 13, 113–198. [Google Scholar] [CrossRef] [PubMed]
- Kirby, A.; Sugden, D.; Beveridge, S.; Edwards, L. Developmental co-ordination disorder (DCD) in adolescents and adults in further and higher education. J. Res. Spec. Educ. 2008, 8, 120–131. [Google Scholar] [CrossRef]
- Gooch, D.; Hulme, C.; Nash, H.M.; Snowling, M.J. Comorbidities in preschool children at family risk of dyslexia. J. Child Psychol. Psychiatry 2014, 55, 237–246. [Google Scholar] [CrossRef]
- Meltzoff, A.N.; Moore, M.K. Imitation of facial and manual gestures by human neonates. Science 1977, 7, 75–78. [Google Scholar] [CrossRef]
- Adolph, K.E.; Eppler, M.A.; Gibson, E.J. Crawling versus walking infants’ perception of affordances for locomotion over sloping surfaces. Child Dev. 1993, 64, 1158–1174. [Google Scholar] [CrossRef]
- Rizzolatti, G.; Fogassi, L.; Gallese, V. Neurophysiological mechanisms underlying the understanding and imitation of action. Nat. Rev. Neurosci. 2001, 2, 661–670. [Google Scholar] [CrossRef]
- Wolpert, D.M.; Miall, R.C. Forward Models for Physiological Motor Control. Neural. Netw. 1996, 9, 1265–1279. [Google Scholar]
- Kawato, M.; Wolpert, D. Internal models for motor control. Sens. Guid. Mov. 1998, 218, 291–304. [Google Scholar]
- Wolpert, D.M.; Miall, R.C.; Kawato, M. Internal models in the cerebellum. Trends Cogn. Sci. 1998, 1, 338–347. [Google Scholar] [CrossRef]
- Wilson, M.; Knoblich, G. The case for motor involvement in perceiving conspecifics. Psychol. Bull. 2005, 131, 460–473. [Google Scholar] [CrossRef]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental movement skills in children and adolescents: Review of associated health benefits. Sports Med. 2010, 1, 1019–1035. [Google Scholar] [CrossRef] [PubMed]
- Ensrud-Skraastad, O.K.; Haga, M. Associations between Motor Competence, Physical Self-Perception and Autonomous Motivation for Physical Activity in Children. Sports 2020, 8, 120. [Google Scholar] [CrossRef] [PubMed]
- Katartzi, E.S.; Vlachopoulos, S.P. Motivating children with developmental coordination disorder in school physical education: The self-determination theory approach. Res. Dev. Disabil. 2011, 32, 2674–2682. [Google Scholar] [CrossRef] [PubMed]
- Boutros, G.H.; Giroux, C.; Sonjak, V.; Blanchet, M. Exercise interventions and evaluation tool of the cardiovascular capacity in children with developmental coordination disorder. Pediatr. Neonatol. 2020, 9, 1–5. [Google Scholar]
- Livonen, K.S.; Sääkslahti, A.K.; Mehtälä, A.; Villberg, J.J.; Tammelin, T.H.; Kulmala, J.S.; Poskiparta, M. Relationship between Fundamental Motor Skills and Physical Activity in 4-Year-Old Preschool Children. Percept. Mot. Ski. 2013, 117, 627–646. [Google Scholar] [CrossRef]
- Foweather, L.; Knowles, Z.; Ridgers, N.D.; O’Dwyer, M.V.; Foulkes, J.D.; Stratton, G. Fundamental movement skills in relation to weekday and weekend physical activity in preschool children. J. Sci. Med. Sport 2015, 18, 691–696. [Google Scholar] [CrossRef]
- LeGear, M.; Greyling, L.; Sloan, E.; Bell, R.I.; Williams, B.-L.; Naylor, P.-J.; Temple, V.A. A window of opportunity? Motor skills and perceptions of competence of children in kindergarten. Int. J. Behav. Nutr. Phys. Act. 2012, 15, 9–29. [Google Scholar] [CrossRef]
- Mancini, V.O.; Rigoli, D.; Roberts, L.D.; Heritage, B.; Piek, J.P. The relationship between motor skills and psychosocial factors in young children: A test of the elaborated environmental stress hypothesis. Br. J. Educ. Psychol. 2018, 88, 363–379. [Google Scholar] [CrossRef]
- Taube, W.; Gruber, M.; Gollhofer, A. Spinal and supraspinal adaptations associated with balance training and their functional relevance. Acta Physiol. 2008, 193, 101–116. [Google Scholar] [CrossRef]
- Steenbergen-Hu, S.; Olszewski-Kubilius, P.; Calvert, E. The Effectiveness of Current Interventions to Reverse the Underachievement of Gifted Students: Findings of a Meta-Analysis and Systematic Review. Gift. Child Q. 2020, 64, 132–165. [Google Scholar] [CrossRef]
- Renshaw, I.; Chow, J.-Y. A constraint-led approach to sport and physical education pedagogy. Phys. Educ. Sport Pedagog. 2019, 24, 103–116. [Google Scholar] [CrossRef]
- Brymer, E.; Renshaw, I. An introduction to the constraints-led approach to learning in outdoor education. Outdoor Environ. Educ. 2010, 14, 33–41. [Google Scholar] [CrossRef]


{kind=link}
| Study | Participants | Motor Tests | Comorbidity Exclusions |
|---|---|---|---|
| SLD | |||
| Hussein et al., 2020 [38] | 100 students with SLD (dyslexia, dyscalculia, or mixed) 100 typical children
| Bruininks–Oseretsky test of motor proficiency, second edition (BOT-2). |
|
| Westendorp et al., 2011 [11] | 104 students with SLD
| Test of Gross Motor Development-2 |
|
| Westendorp et al., 2014 [12] | 91 students with SLD 46 control students
| Test of Gross Motor Development-2 |
|
| Vuijk et al., 2011 [39] | 137 students with SLD, included ADHD (16.8%) and PDD-NOS (13.9%),
| M-ABC |
|
| ** Ibrahim et al., 2019 [19] | 148 students with SLD (dyslexia, dyscalculia, dysgraphia and/or slow learner based on Dyslexia Association Malaysian criteria)
|
|
|
| ** Poblano et al., 2001 [40] | 27 students with SLD 27 control students
|
|
|
| ** Blanchet et al., 2022 [41] | 74 students with SLD but only 10 without comorbidities were included 20 control students
| Forward, backward, leftward and rightward stability limits with eyes open or eyes closed, standing on foam conditions. |
|
| Galli et al., 2011 [15] | 18 students with SLD 24 control students
| Upwards and downwards spring test |
|
| ** Okuda and Pinheiroa 2015 [42] | 10 students with learning difficulties, 10 control students
| Bruininks–Oseretsky Test of Motor Proficiency |
|
| Jongmans 2003 [43] | 94 SLD students without DCD, 57 students with DCD but without SLD, 53 students with both DCD and SLD, 545 control students (without DCD and without SLD)
| M-ABC |
|
| DYSLEXIA | |||
| Getchell et al., 2007 [44] | 26 students with dyslexia
|
|
|
| ** Marchand-Krynski et al., 2017 [45] | 27 students with dyslexia 27 students with attention deficit disorder with or without hyperactivity disorder (AD) student group 27 students with Dylexia + AD 27 control students
| The Leonard Tapping Task |
|
| Moe-Nilssen et al., 2003 [46] | 18 students with dyslexia 21 control students
| Standing on firm, compliant mat (0.00-m-thick) and compliant pillow (0.10-m-thick) during quiet standing (eyes open (EO), with eyes closed (EC), and walking. |
|
| McPhillips and Sheehy, 2004 [47] | 41 poor readers students (bottom 10% based on WORD percentile scores with ties resolved by reference to NARA percentile scores) 41 middle reader students (middle 10%) 41 good reader students (top 10%)
|
|
|
| ** Iversen et al., 2005 [48] | 20 students with dyslexia (severe dyslexia referred to specialist evaluation) 17 poor readers (teacher selected municipality sample comprising the 5% poorest readers) 22 good readers (control group) (teacher selected municipality sample comprising the 5% best readers)
| M-ABC |
|
| ** Barela et al., 2020 [49] | 12 students with dyslexia 12 control students
| Quiet upright stance in both fixation and guided conditions (fixate on a target that appeared and disappeared on the left and right sides of the monitor). Body sway was measured with OPTOTRAK. Eye movements were tracked using eye-tracking glasses (ETG 2.0-SMI). |
|
| * Kaplan et al., 1998 [37] | 224 students with learning reading disorders/attention disorders. 155 control students
|
|
|
| ** Brookes 2010 [50] | 16 students with dyslexia 24 control students 17 adults with dyslexia 30 control adults,
|
|
|
| Viana et al., 2013 [51] | 30 students with dyslexia 30 control students
| Quiet standing balance inside a moving room under five conditions:
|
|
| Barela 2011 [52] | 10 students with dyslexia 10 control students
| Quiet upright standing balance inside a moving room that remained stationary or oscillated back and forward at frequencies of 0.2 or 0.5 Hz. |
|
| Razuk et Barela, 2014 [53] | 18 students with dyslexia 18 control students
| Quiet upright standing balance inside a moving room; looked at a target at different distances between the participant and a moving room frontal wall (25–150 cm) and with different vision (full and central). |
|
| ** Razuk et al., 2020 [54] | 20 students with dyslexia 19 control students
| Quiet upright standing balance inside a moving room and another balance test with OR during lightly touching a moving bar with three different stimulus characteristics: low (pre-transition), high (transition), and low-amplitude (post-transition). |
|
| ** Goulème et al., 2015 [55] | 30 students with dyslexia 30 control students
| Quiet upright standing balance was evaluated using Multitest Equilibre from Framiral®. Posture with eyes open and eyes closed under stable and unstable platform conditions. |
|
| Okuda et al., 2014 [56] | 19 students with dyslexia 60 control students
| Bruininks–Oseretsky Test of Motor Proficiency (second edition) |
|
| ** Razuk et al., 2018 [57] | 15 students with dyslexia 15 control students
| Quiet upright standing balance during text reading and Landolt reading. Eye movements (Mobile T2®, SuriCog) and center of pressure excursions (Multitest Equilibre) |
|
| ** Bucci et al., 2017 [58] | 23 students with dyslexia 23 students with Autism Spectrum Disorder (ASD) 23 students with Attention deficit/hyperactive disorder (ADHD) 23 control students
| Quiet upright standing balance (Multitest Equilibre) on both a stable and an unstable platform, under two different visual conditions: eyes open and eyes closed. |
|
| ** Goulème et al., 2017 [59] | 24 students with dyslexia 24 control students
| Quiet upright standing balance (TechnoConcept® platform) on both a firm and foam support surface under two different visual conditions: eyes open and eyes closed |
|
| * Ramus et al., 2003 [60] | 22 students with dyslexia (included 7 with ADHD, 1 with DCD, and 2 both ADHD and DCD) 22 control students
| Cerebellar tests |
|
| ** Legrand et al., 2012 [61] | 18 students with dyslexia 18 control students
| Quiet upright standing balance (TechnoConcept® platform) during visually guided saccade task and silent reading of a text. |
|
| ** Kapoula et Bucci, 2007 [62] | 13 students with dyslexia 13 control students
| Quiet upright standing balance during fixing LED placed near to (25 cm) or far from (150 cm) participants with fixation alternated between the far and the near LED targets. |
|
| ** Lam et al., 2011 [63] | 137 students with dyslexia 756 control students
| Chinese Handwriting Assessment Tool (CHAT) |
|
| Niechwiej-Szwedo et al., 2017 [64] | 19 poor readers (who were reading below expected grades and age-level) 19 typically developing children.
| Bead-threading and pegboard |
|
| ** Wolff et al., 1990 [65] | 50 students with dyslexia 50 control students 40 dyslexic adults
| Tap in time to an entraining metronome at 3 prescribed rates by moving the index fingers of both hands in unison, in rhythmical alternation, or in more complex bimanual patterns. |
|
| ** Naz and Najam 2019 [66] | 24 reading disorder students (pure), 24 reading disorder + ADHD students 24 control students
|
|
|
| Haouès et al., 2021 [67] | 30 students with dyslexia (28.9% had ADHD) 30 control students
| Quiet upright standing balance (RunTime®) bipedal and unipedal (eyes open and eyes closed). |
|
| Dyscalculia | |||
| Pieters et al., 2012 [68] | 39 students with mathematical learning disabilities, 106 control students.
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanchet, M.; Assaiante, C. Specific Learning Disorder in Children and Adolescents, a Scoping Review on Motor Impairments and Their Potential Impacts. Children 2022, 9, 892. https://doi.org/10.3390/children9060892
Blanchet M, Assaiante C. Specific Learning Disorder in Children and Adolescents, a Scoping Review on Motor Impairments and Their Potential Impacts. Children. 2022; 9(6):892. https://doi.org/10.3390/children9060892
Chicago/Turabian StyleBlanchet, Mariève, and Christine Assaiante. 2022. "Specific Learning Disorder in Children and Adolescents, a Scoping Review on Motor Impairments and Their Potential Impacts" Children 9, no. 6: 892. https://doi.org/10.3390/children9060892
APA StyleBlanchet, M., & Assaiante, C. (2022). Specific Learning Disorder in Children and Adolescents, a Scoping Review on Motor Impairments and Their Potential Impacts. Children, 9(6), 892. https://doi.org/10.3390/children9060892