
Vitamin D Levels in Pregnant Women Do Not Affect Neonatal Bone Strength

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Uday, S.; Högler, W. Nutritional Rickets and Osteomalacia in the Twenty-first Century: Revised Concepts, Public Health, and Prevention Strategies. Curr. Osteoporos. Rep. 2017, 15, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Marshall, I.; Mehta, R.; Petrova, A. Vitamin D in the maternal–fetal–neonatal interface: Clinical implications and requirements for supplementation. J. Matern. Fetal Neonatal Med. 2013, 26, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, C.S. Maternal Mineral and Bone Metabolism During Pregnancy, Lactation, and Post-Weaning Recovery. Physiol. Rev. 2016, 96, 449–547. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, C.S. Bone Development and Mineral Homeostasis in the Fetus and Neonate: Roles of the Calciotropic and Phosphotropic Hormones. Physiol. Rev. 2014, 94, 1143–1218. [Google Scholar] [CrossRef]
- Verhaeghe, J.; Bouillon, R. Calciotropic hormones during reproduction. J. Steroid Biochem. Mol. Biol. 1992, 41, 469–477. [Google Scholar] [CrossRef]
- Fudge, N.J.; Kovacs, C.S. Pregnancy Up-Regulates Intestinal Calcium Absorption and Skeletal Mineralization Independently of the Vitamin D Receptor. Endocrinology 2010, 151, 886–895. [Google Scholar] [CrossRef]
- Gillies, B.R.; Ryan, B.A.; Tonkin, B.A.; Poulton, I.J.; Ma, Y.; Kirby, B.J.; St-Arnaud, R.; Sims, N.A.; Kovacs, C.S. Absence of calcitriol causes increased lactational bone loss and lower milk calcium but does not impair post-lactation bone recovery in Cyp27b1 null mice: Effects of calcitriol during pregnancy and lactation. J. Bone Miner. Res. 2018, 33, 16–26. [Google Scholar] [CrossRef]
- Halloran, B.P.; DeLuca, H.F. Calcium transport in small intestine during pregnancy and lactation. Am. J. Physiol. Endocrinol. Metab. 1980, 239, E64–E68. [Google Scholar] [CrossRef]
- Brommage, R.; Baxter, D.C.; Gierke, L.W. Vitamin D-independent intestinal calcium and phosphorus absorption during reproduction. Am. J. Physiol. Gastrointest. Liver Physiol. 1990, 259, G631–G638. [Google Scholar] [CrossRef]
- Ward, L.M.; Gaboury, I.; Ladhani, M.; Zlotkin, S. Vitamin D-deficiency rickets among children in Canada. Can. Med. Assoc. J. 2007, 177, 161–166. [Google Scholar] [CrossRef]
- Cooper, C.; Harvey, N.C.; Bishop, N.J.; Kennedy, S.; Papageorghiou, A.T.; Schoenmakers, I.; Fraser, R.; Gandhi, S.V.; Carr, A.; D’Angelo, S.; et al. Maternal gestational vitamin D supplementation and offspring bone health (MAVIDOS): A multicentre, double-blind, randomised placebo-controlled trial. Lancet Diabetes Endocrinol. 2016, 4, 393–402. [Google Scholar] [CrossRef]
- Viljakainen, H.T.; Saarnio, E.; Hytinantti, T.; Miettinen, M.; Surcel, H.; Mäkitie, O.; Andersson, S.; Laitinen, K.; Lamberg-Allardt, C. Maternal Vitamin D Status Determines Bone Variables in the Newborn. J. Clin. Endocrinol. Metab. 2010, 95, 1749–1757. [Google Scholar] [CrossRef]
- Mahon, P.; Harvey, N.; Crozier, S.; Inskip, H.; Robinson, S.; Arden, N.; Swaminathan, R.; Cooper, C.; Godfrey, K. Low maternal vitamin D status and fetal bone development: Cohort study. J. Bone Miner. Res. 2010, 25, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, C.; Javaid, M.K.; Mahon, P.; Yaqub, M.K.; Harvey, N.C.; Godfrey, K.M.; Noble, J.A.; Cooper, C.; Papageorghiou, A.T. The Effect of Maternal Vitamin D Concentration on Fetal Bone. J. Clin. Endocrinol. Metab. 2012, 97, E2070–E2077. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N.C.; Sheppard, A.; Godfrey, K.M.; McLean, C.; Garratt, E.; Ntani, G.; Davies, L.; Murray, R.; Inskip, H.M.; Gluckman, P.D.; et al. Childhood Bone Mineral Content Is Associated with Methylation Status of the RXRA Promoter at Birth. J. Bone Miner. Res. 2014, 29, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Nemet, D.; Dolfin, T.; Wolach, B.; Eliakim, A. Quantitative ultrasound measurements of bone speed of sound in premature infants. Eur. J. Pediatr. 2001, 160, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Wright, L.L.; Glade, M.J.; Gopal, J. The Use of Transmission Ultrasonics to Assess Bone Status in the Human Newborn. Pediatr. Res. 1987, 22, 541–544. [Google Scholar] [CrossRef]
- Gursoy, T.; Yurdakok, M.; Hayran, M.; Korkmaz, A.; Yigit, S.; Tekinalp, G. Bone Speed of Sound Curves of Twin and Singleton Neonates. J. Pediatric Endocrinol. Metab. 2008, 21, 1065–1071. [Google Scholar] [CrossRef]
- Regev, R.H.; Dolfin, T.; Eliakim, A.; Arnon, S.; Bauer, S.; Nemet, D.; Litmanovitz, I. Bone Speed of Sound in Infants of Mothers with Gestational Diabetes Mellitus. J. Pediatric Endocrinol. Metab. 2004, 17, 1083–1088. [Google Scholar] [CrossRef]
- Litmanovitz, I.; Dolfin, T.; Friedland, O.; Arnon, S.; Regev, R.; Shainkin-Kestenbaum, R.; Lis, M.; Eliakim, A. Early Physical Activity Intervention Prevents Decrease of Bone Strength in Very Low Birth Weight Infants. Pediatrics 2003, 112, 15–19. [Google Scholar] [CrossRef]
- Mukamel, M.N.; Weisman, Y.; Somech, R.; Eisenberg, Z.; Landman, J.; Shapira, I.; Spirer, Z.; Jurgenson, U. Vitamin D deficiency and insufficiency in Orthodox and non-Orthodox Jewish mothers in Israel. Isr. Med. Assoc. J. 2001, 3, 419–421. [Google Scholar] [PubMed]
- Fouda, M.A.; Turkestani, I.Z.; Almusharraf, S.; Al-Ajlan, A.; Angkaya-Bagayawa, F.F.; Sabico, S.; Mohammed, A.G.; Hassanato, R.; Al-Serehi, A.; Alshingetti, N.M.; et al. Extremely High Prevalence of Maternal and Neonatal Vitamin D Deficiency in the Arab Population. Neonatology 2017, 112, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Simhan, H.N.; Powers, R.W.; Frank, M.P.; Cooperstein, E.; Roberts, J.M. High Prevalence of Vitamin D Insufficiency in Black and White Pregnant Women Residing in the Northern United States and Their Neonates. J. Nutr. 2007, 137, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, A.; Sharifi, F.; Jafari, N.; Mousavinasab, N. High Prevalence of Vitamin D Deficiency among Pregnant Women and their Newborns in an Iranian Population. J. Women’s Health 2009, 18, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Shany, S.; Biale, Y.; Zuili, I.; Yankowitz, N.; Berry, J.L.; Mawer, E.B. Feto-maternal relationships between vitamin D metabolites in Israeli Bedouins and Jews. Am. J. Clin. Nutr. 1984, 40, 1290–1294. [Google Scholar] [CrossRef]
- Karras, S.; Bili, H.; Goulis, D.; Papadopoulou, F.; Harizopoulou, V.; Kintiraki, E.; Gkastaris, K.; Badis, K.; Tarlatzis, B. High prevalence of vitamin d deficiency among pregnant women at term and their neonates in Thessaloniki, Northern Greece. Bone 2012, 50 (Suppl. S1), S104. [Google Scholar] [CrossRef]
- Esmeraldo, C.U.P.; Martins, M.E.P.; Maia, E.R.; Leite, J.L.A.; Ramos, J.L.S.; Goncalves, J., Jr.; Neta, C.M.; Suano-Souza, F.I.; Sarni, R.O.S. Vitamin D in Term Newborns: Relation with Maternal Concentrations and Birth Weight. Ann. Nutr. Metab. 2019, 75, 39–46. [Google Scholar] [CrossRef]
- Olmos-Ortiz, A.; Avila, E.; Durand-Carbajal, M.; Díaz, L. Regulation of Calcitriol Biosynthesis and Activity: Focus on Gestational Vitamin D Deficiency and Adverse Pregnancy Outcomes. Nutrients 2015, 7, 443–480. [Google Scholar] [CrossRef]
- Karras, S.N.; Wagner, C.L.; Castracane, V.D. Understanding vitamin D metabolism in pregnancy: From physiology to pathophysiology and clinical outcomes. Metabolism 2018, 86, 112–123. [Google Scholar] [CrossRef]
- Evans, K.N.; Bulmer, J.N.; Kilby, M.D.; Hewison, M. Vitamin D and Placental-Decidual Function. J. Soc. Gynecol. Investig. 2004, 11, 263–271. [Google Scholar] [CrossRef]
- Velkavrh, M.; Paro-Panjan, D.; Benedik, E.; Mis, N.F.; Godnov, U.; Salamon, A.S. The Influence of Maternal Levels of Vitamin D and Adiponectin on Anthropometrical Measures and Bone Health in Offspring. PRILOZI 2019, 40, 91–98. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Liao, X.P.; Zhang, W.L.; Yan, C.H.; Zhou, X.J.; Wang, P.; Sun, J.H.; Yu, X.D.; Wu, M.Q. Reduced tibial speed of sound in Chinese infants at birth compared with Caucasian peers: The effects of race, gender, and vitamin D on fetal bone development. Osteoporos. Int. 2010, 21, 2003–2011. [Google Scholar] [CrossRef]
- Masztalerz-Kozubek, D.; Zielinska-Pukos, M.A.; Hamulka, J. Maternal Diet, Nutritional Status, and Birth-Related Factors Influencing Offspring’s Bone Mineral Density: A Narrative Review of Observational, Cohort, and Randomized Controlled Trials. Nutrients 2021, 13, 2302. [Google Scholar] [CrossRef] [PubMed]
- Hyde, N.K.; Brennan-Olsen, S.L.; Wark, J.D.; Hosking, S.M.; Pasco, J.A. Gestational Vitamin D and Offspring Bone Measures: Is the Association Independent of Maternal Bone Quality? Calcif. Tissue Int. 2021, 108, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.K.; Crozier, S.R.; Harvey, N.C.; Gale, C.R.; Dennison, E.M.; Boucher, B.J.; Arden, N.K.; Godfrey, K.M.; Cooper, C. Maternal Vitamin D Status During Pregnancy and Childhood Bone Mass at Age 9 Years: A Longitudinal Study. Obstet. Gynecol. Surv. 2006, 61, 305–307. [Google Scholar] [CrossRef]
- Sayers, A.; Tobias, J.H. Estimated maternal ultraviolet B exposure levels in pregnancy influence skeletal development of the child. J. Clin. Endocrinol. Metab. 2009, 94, 765–771. [Google Scholar] [CrossRef]
- Cole, Z.A.; Gale, C.R.; Javaid, M.K.; Robinson, S.M.; Law, C.; Boucher, B.J.; Crozier, S.R.; Godfrey, K.M.; Dennison, E.M.; Cooper, C. Maternal dietary patterns during pregnancy and childhood bone mass: A longitudinal study. J. Bone Miner. Res. 2009, 24, 663–668. [Google Scholar] [CrossRef]
- Ryan, B.A.; Kovacs, C.S. Maternal and fetal vitamin D and their roles in mineral homeostasis and fetal bone development. J. Endocrinol. Investig. 2021, 44, 643–659. [Google Scholar] [CrossRef]
- Wierzejska, R.; Jarosz, M.; Klemińska-Nowak, M.; Tomaszewska, M.; Sawicki, W.; Bechanek, M.; Siuba-Strzelinska, M. Maternal and Cord Blood Vitamin D Status and Anthropometric Measurements in Term Newborns at Birth. Front. Endocrinol. 2018, 9, 9. [Google Scholar] [CrossRef]
- Miliku, K.; Vinkhuyzen, A.; Blanken, L.M.; McGrath, J.J.; Eyles, D.W.; Burne, T.H.; Hofman, A.; Tiemeier, H.; Steegers, E.A.; Gaillard, R.; et al. Maternal vitamin D concentrations during pregnancy, fetal growth patterns, and risks of adverse birth outcomes. Am. J. Clin. Nutr. 2016, 103, 1514–1522. [Google Scholar] [CrossRef]
- Leffelaar, E.R.; Vrijkotte, T.G.M.; van Eijsden, M. Maternal early pregnancy vitamin D status in relation to fetal and neonatal growth: Results of the multi-ethnic Amsterdam Born Children and their Development cohort. Br. J. Nutr. 2010, 104, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Bowyer, L.; Catling-Paull, C.; Diamond, T.; Homer, C.; Davis, G.; Craig, M.E. Vitamin D, PTH and calcium levels in pregnant women and their neonates. Clin. Endocrinol. 2009, 70, 372–377. [Google Scholar] [CrossRef] [PubMed]
- De-Regil, L.M.; Palacios, C.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2016, CD008873. [Google Scholar] [CrossRef]
- Harvey, N.C.; Holroyd, C.; Ntani, G.; Javaid, K.; Cooper, P.; Moor, R.; Cole, Z.; Tinati, T.; Godfrey, K.; Dennison, E.; et al. Vitamin D supplementation in pregnancy: A systematic review. Health Technol. Assess. 2014, 18, 1–190. [Google Scholar] [CrossRef]
- Theodoratou, E.; Tzoulaki, I.; Zgaga, L.; Ioannidis, J.P.A. Vitamin D and multiple health outcomes: Umbrella review of systematic reviews and meta-analyses of observational studies and randomised trials. BMJ 2014, 348, g2035. [Google Scholar] [CrossRef]
- Aghajafari, F.; Nagulesapillai, T.; Ronksley, P.E.; Tough, S.C.; O’Beirne, M.; Rabi, D.M. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: Systematic review and meta-analysis of observational studies. BMJ 2013, 346, f1169. [Google Scholar] [CrossRef]
- Thorne-Lyman, A.; Fawzi, W.W. Vitamin D During Pregnancy and Maternal, Neonatal and Infant Health Outcomes: A Systematic Review and Meta-analysis: Vitamin D and health outcomes. Paediatr. Perinat. Epidemiol. 2012, 26, 75–90. [Google Scholar] [CrossRef]
- Al-Faris, N. High Prevalence of Vitamin D Deficiency among Pregnant Saudi Women. Nutrients 2016, 8, 77. [Google Scholar] [CrossRef]
- Hajizadeh, S.; Rankin Shary, J.; Gayle Reed, S.; Lynn Wagner, C. The prevalence of hypovitaminosis D and its risk factors in pregnant women and their newborns in the Middle East: A systematic review. Int. J. Reprod. Biomed. (IJRM) 2019, 17, 685–708. [Google Scholar] [CrossRef]
- Buyukuslu, N.; Esin, K.; Hizli, H.; Sunal, N.; Yigit, P.; Garipagaoglu, M. Clothing preference affects vitamin D status of young women. Nutr. Res. 2014, 34, 688–693. [Google Scholar] [CrossRef]
- Kasirer, Y.; Reichman, B.; Zaslavsky-Paltiel, I.; Bin-Nun, A.; Lerner-Geva, L.; Mimouni, F.B.; in collaboration with the Israel Neonatal Network. Short-term outcomes of Jewish and Arab preterms: A population-based comparison. J. Perinatol. 2021, 41, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Hajhashemi, M.; Khorsandi, A.; Haghollahi, F. Comparison of sun exposure versus vitamin D supplementation for pregnant women with vitamin D deficiency. J. Matern. Fetal Neonatal Med. 2019, 32, 1347–1352. [Google Scholar] [CrossRef] [PubMed]
- Shalof, H.; Dimitri, P.; Shuweihdi, F.; Offiah, A.C. Which skeletal imaging modality is best for assessing bone health in children and young adults compared to DXA? A systematic review and meta-analysis. Bone 2021, 150, 116013. [Google Scholar] [CrossRef] [PubMed]
- Pezzuti, I.L.; Kakehasi, A.M.; Filgueiras, M.T.; de Guimarães, J.A.; de Lacerda, I.A.C.; Silva, I.N. Imaging methods for bone mass evaluation during childhood and adolescence: An update. J. Pediatr. Endocrinol. Metab. 2017, 30, 485–497. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.C.; Wang, K.C.; Amirabadi, A.; Cheung, E.; Uleryk, E.; Moineddin, R.; Doria, A.S. Evidence-based outcomes on diagnostic accuracy of quantitative ultrasound for assessment of pediatric osteoporosis—A systematic review. Pediatr. Radiol. 2014, 44, 1573–1587. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Maternal | Value |
|---|---|
| Age (years) | 30.7 ± 5.1 |
| Education (years) | 15.6 ± 2.2 |
| Origin: Jewish | 69 (86%) |
| Nulliparous | 47 (59%) |
| Singleton | 75 (94%) |
| Daily sun exposure | |
| Less than 15 min | 31 (40%) |
| More than 30 min | 47 (60%) |
| Sun skin protection | 29 (37%) |
| Vitamin D supplementation | 36 (45%) |
| Vitamin D supplementation dose (IU) | 1127 ± 894 |
| Vitamin D from nutrition (IU) | 239.3 ± 140.6 |
| Total Vitamin D consumption (IU) | 748 ± 824 |
| Infant | |
| Gestational age (weeks) | 39.5 ± 1.26 |
| Birth weight (grams) | 3223 ± 476 |
| Length (centimeters) | 50.7 ± 2.9 |
| Head circumference (cm) | 34.3 ± 1.3 |
| Male sex | 35 (44%) |
| Speed of sound (m/s) | 3042 ± 130 |
| 25(OH)D (nmol/L) | N | SOS (m/s) (Mean ± SD) | p-Value |
|---|---|---|---|
| Cord blood | |||
| <25 | 6 | 3040 ± 161 | 0.97 |
| 25–50 | 29 | 3049 ± 137 | |
| >50 | 38 | 3042 ± 123 | |
| Maternal | |||
| <25 | 13 | 3053 ± 119 | 0.15 |
| 25–50 | 29 | 3076 ± 143 | |
| >50 | 31 | 3011 ± 118 | |
| Continuous Variables | Pearson Correlation | Significance |
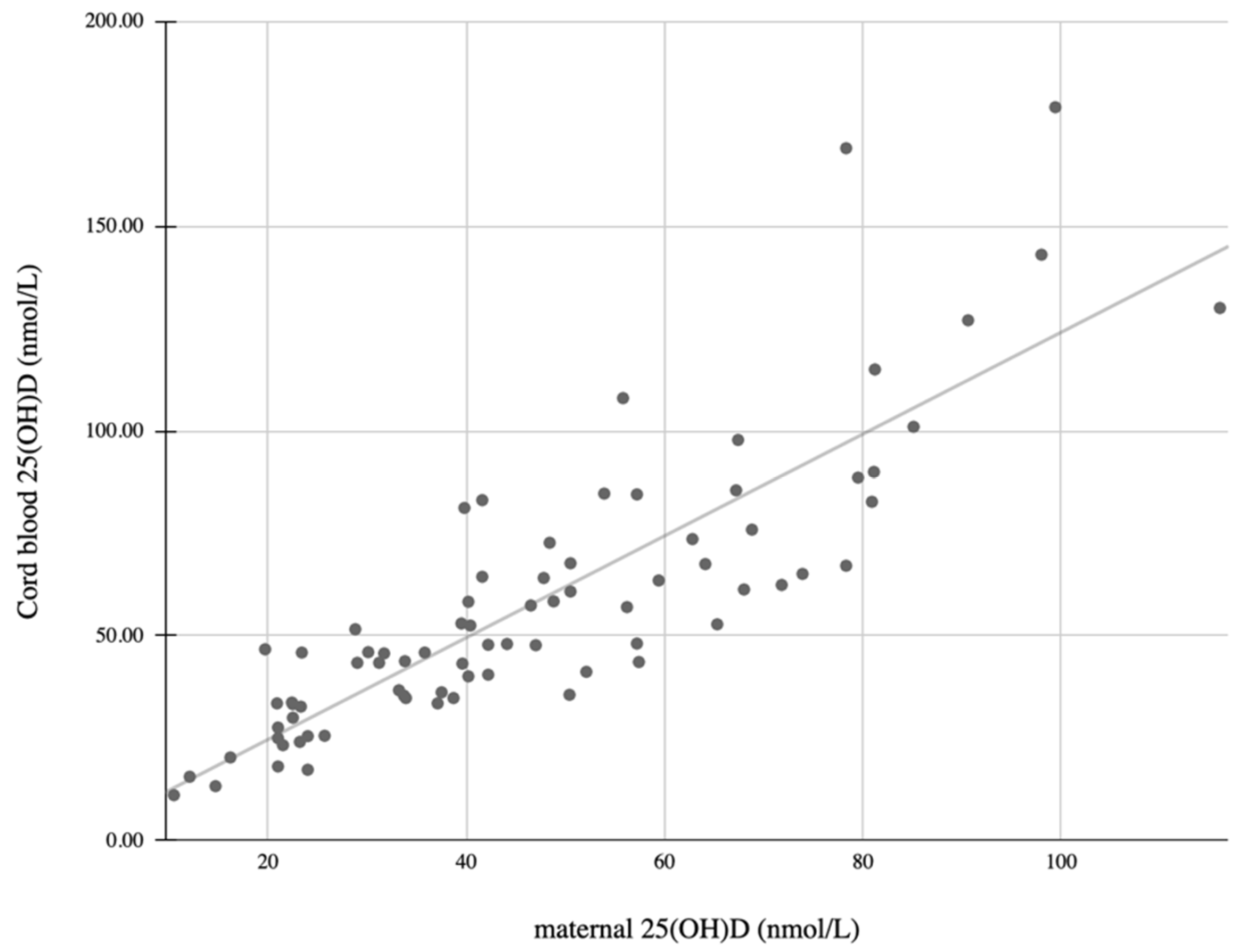
| Infant 25(OH)D levels | 0.85 | <0.001 |
| Infant SOS | −0.1 | 0.4 |
| Vitamin D intake–total | 0.36 | 0.001 |
| Vitamin D intake from food only | 0.026 | 0.82 |
| Vitamin D intake from supplements | 0.21 | 0.002 |
| Infant length at birth | 0.009 | 0.94 |
| Infant weight at birth | 0.082 | 0.47 |
| Infant head circumference | 0.212 | 0.063 |
| Maternal age | 0.11 | 0.32 |
| Non-continuous variables (MW test) | Significance | |
| Maternal ethnicity | <0.0001 | |
| Maternal sunlight exposure | 0.62 | |
| Maternal skin exposure | 0.12 | |
| Maternal use of sunscreen | 0.08 | |
| Season of the year | 0.76 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levkovitz, O.; Lagerev, E.; Bauer-Rusak, S.; Litmanovitz, I.; Grinblatt, E.; Sirota, G.L.; Shalit, S.; Arnon, S. Vitamin D Levels in Pregnant Women Do Not Affect Neonatal Bone Strength. Children 2022, 9, 883. https://doi.org/10.3390/children9060883
Levkovitz O, Lagerev E, Bauer-Rusak S, Litmanovitz I, Grinblatt E, Sirota GL, Shalit S, Arnon S. Vitamin D Levels in Pregnant Women Do Not Affect Neonatal Bone Strength. Children. 2022; 9(6):883. https://doi.org/10.3390/children9060883
Chicago/Turabian StyleLevkovitz, Orly, Elena Lagerev, Sofia Bauer-Rusak, Ita Litmanovitz, Eynit Grinblatt, Gisela Laura Sirota, Shachar Shalit, and Shmuel Arnon. 2022. "Vitamin D Levels in Pregnant Women Do Not Affect Neonatal Bone Strength" Children 9, no. 6: 883. https://doi.org/10.3390/children9060883
APA StyleLevkovitz, O., Lagerev, E., Bauer-Rusak, S., Litmanovitz, I., Grinblatt, E., Sirota, G. L., Shalit, S., & Arnon, S. (2022). Vitamin D Levels in Pregnant Women Do Not Affect Neonatal Bone Strength. Children, 9(6), 883. https://doi.org/10.3390/children9060883