
Impact of the Free-Pelvis Innovation in Very Rigid Braces for Adolescents with Idiopathic Scoliosis: Short-Term Results of a Matched Case-Control Study

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
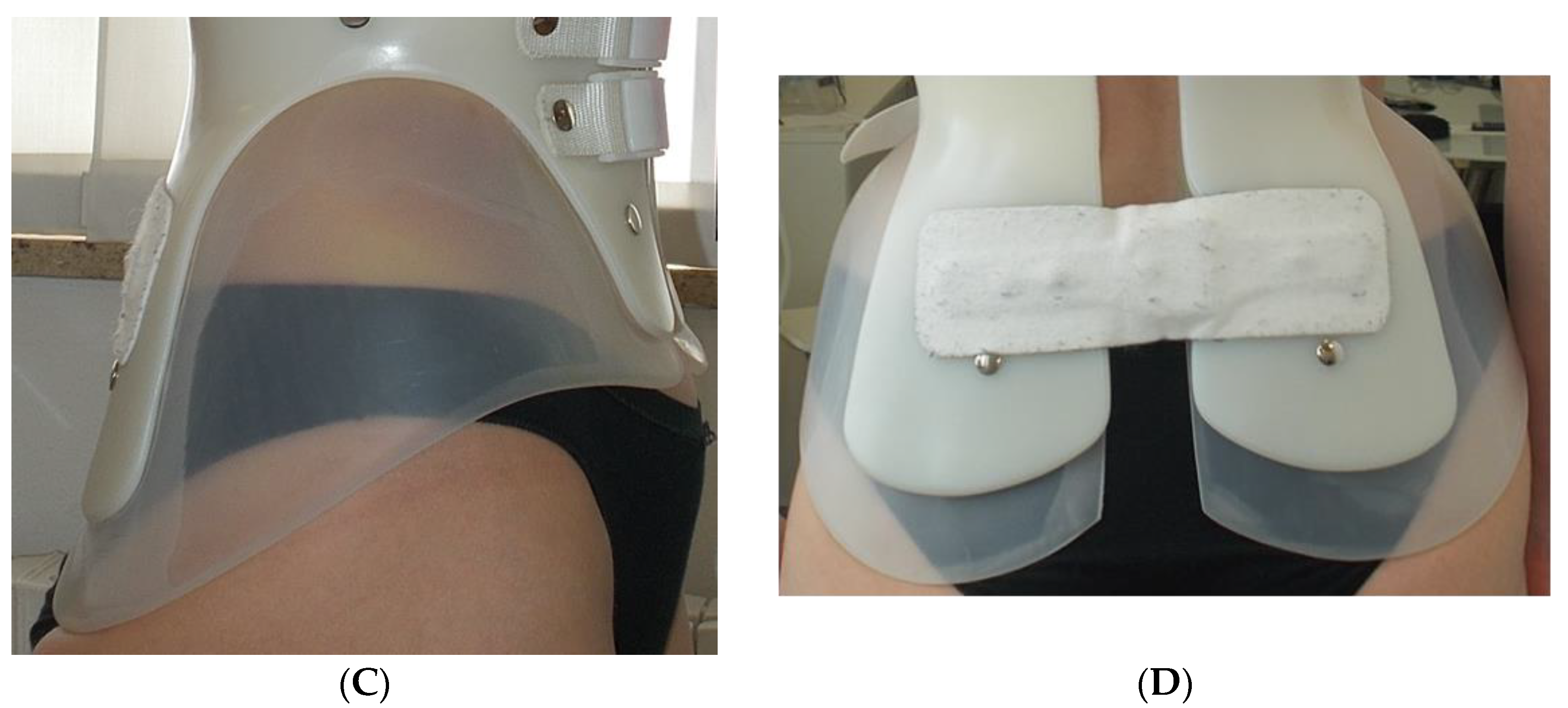
2.3. Treatments
2.4. Outcome
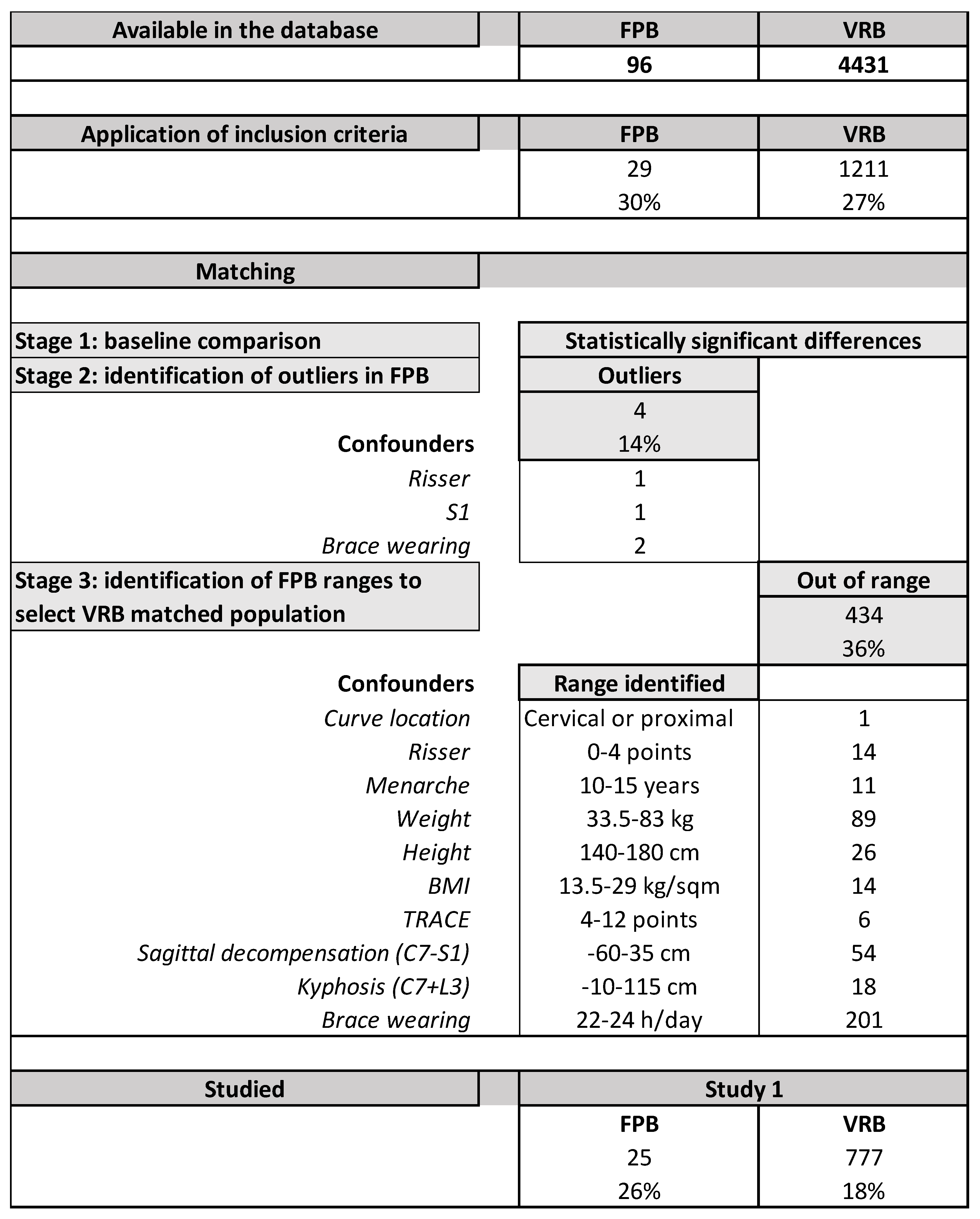
2.5. Matching
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT Guidelines: Orthopaedic and Rehabilitation Treatment of Idiopathic Scoliosis during Growth. Scoliosis Spinal Disord 2018, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of Bracing in Adolescents with Idiopathic Scoliosis. N. Eng. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef] [PubMed]
- Nachemson, A.L.; Peterson, L.E. Effectiveness of Treatment with a Brace in Girls Who Have Adolescent Idiopathic Scoliosis. A Prospective, Controlled Study Based on Data from the Brace Study of the Scoliosis Research Society. J. Bone Jt. Surg Am. 1995, 77, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Minozzi, S.; Bettany-Saltikov, J.; Chockalingam, N.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Romano, M.; Zaina, F. Braces for Idiopathic Scoliosis in Adolescents. Cochrane Database Syst Rev. 2015, 6, CD006850. [Google Scholar] [CrossRef]
- Negrini, S.; Aulisa, A.G.; Cerny, P.; de Mauroy, J.C.; McAviney, J.; Mills, A.; Donzelli, S.; Grivas, T.B.; Hresko, M.T.; Kotwicki, T.; et al. The Classification of Scoliosis Braces Developed by SOSORT with SRS, ISPO, and POSNA and Approved by ESPRM. Eur. Spine J. 2022, 31, 980–989. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Donzelli, S.; Negrini, F.; Arienti, C.; Zaina, F.; Peers, K. A Pragmatic Benchmarking Study of an Evidence-Based Personalised Approach in 1938 Adolescents with High-Risk Idiopathic Scoliosis. J. Clin. Med. 2021, 10, 5020. [Google Scholar] [CrossRef]
- Negrini, S.; Marchini, G.; Tessadri, F. Brace Technology Thematic Series—The Sforzesco and Sibilla Braces, and the SPoRT (Symmetric, Patient Oriented, Rigid, Three-Dimensional, Active) Concept. Scoliosis 2011, 6, 8. [Google Scholar] [CrossRef]
- Lusini, M.; Donzelli, S.; Minnella, S.; Zaina, F.; Negrini, S. Brace Treatment Is Effective in Idiopathic Scoliosis over 45°: An Observational Prospective Cohort Controlled Study. Spine J. 2014, 14, 1951–1956. [Google Scholar] [CrossRef]
- Zaina, F.; de Mauroy, J.C.; Donzelli, S.; Negrini, S. SOSORT Award Winner 2015: A Multicentre Study Comparing the SPoRT and ART Braces Effectiveness According to the SOSORT-SRS Recommendations. Scoliosis 2015, 10, 23. [Google Scholar] [CrossRef]
- Tessadri, F.; Negrini, S. Orthopaedic Brace and Method for Customizing an Orthopaedic Brace. Patent No. 102019000003045, 4 February 2021. [Google Scholar]
- Negrini, S.; Hresko, T.M.; O’Brien, J.P.; Price, N.; SOSORT Boards. SRS Non-Operative Committee Recommendations for Research Studies on Treatment of Idiopathic Scoliosis: Consensus 2014 between SOSORT and SRS Non-Operative Management Committee. Scoliosis 2015, 10, 8. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Negrini, S.; Atanasio, S.; Negrini, F.; Zaina, F.; Marchini, G. The Sforzesco Brace Can Replace Cast in the Correction of Adolescent Idiopathic Scoliosis: A Controlled Prospective Cohort Study. Scoliosis 2008, 3, 15. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Marchini, G. Efficacy of the Symmetric, Patient-Oriented, Rigid, Three-Dimensional, Active (SPoRT) Concept of Bracing for Scoliosis: A Prospective Study of the Sforzesco versus Lyon Brace. Eura Med. 2007, 43, 171–181; discussion 183–184. [Google Scholar]
- Donzelli, S.; Zaina, F.; Negrini, S. In Defense of Adolescents: They Really Do Use Braces for the Hours Prescribed, If Good Help Is Provided. Results from a Prospective Everyday Clinic Cohort Using Thermobrace. Scoliosis 2012, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.; Negrini, A.; Parzini, S.; Tavernaro, M.; Zaina, F.; Donzelli, S.; Negrini, S. SEAS (Scientific Exercises Approach to Scoliosis): A Modern and Effective Evidence Based Approach to Physiotherapic Specific Scoliosis Exercises. Scoliosis 2015, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Grivas, T.B.; Kotwicki, T.; Rigo, M.; Zaina, F. The international Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) Guidelines on “Standards of Management of Idiopathic Scoliosis with Corrective Braces in Everyday Clinics and in Clinical Research”: SOSORT Consensus 2008. Scoliosis 2009, 4, 2. [Google Scholar] [CrossRef]
- Dolan, L.A.; Donzelli, S.; Zaina, F.; Weinstein, S.L.; Negrini, S. Adolescent Idiopathic Scoliosis Bracing Success Is Influenced by Time in Brace: Comparative Effectiveness Analysis of BrAIST and ISICO Cohorts. Spine (Phila Pa 1976) 2020, 45, 1193–1199. [Google Scholar] [CrossRef]
- Bunnell, W.P. Outcome of Spinal Screening. Spine 1993, 18, 1572–1580. [Google Scholar] [CrossRef]
- Zaina, F.; Negrini, S.; Atanasio, S. TRACE (Trunk Aesthetic Clinical Evaluation), a Routine Clinical Tool to Evaluate Aesthetics in Scoliosis Patients: Development from the Aesthetic Index (AI) and Repeatability. Scoliosis 2009, 4, 3. [Google Scholar] [CrossRef]
- Negrini, A.; Vanossi, M.; Donzelli, S.; Zaina, F.; Romano, M.; Negrini, S. Spinal Coronal and Sagittal Balance in 584 Healthy Individuals During Growth: Normal Plumb Line Values and Their Correlation With Radiographic Measurements. Phys. Ther. 2019, 99, 1712–1718. [Google Scholar] [CrossRef]
- Negrini, S.; Donzelli, S.; Jurenaite, G.; Negrini, F.; Zaina, F. Efficacy of Bracing in Early Infantile Scoliosis: A 5-Year Prospective Cohort Shows That Idiopathic Respond Better than Secondary-2021 SOSORT Award Winner. Eur. Spine J. 2021, 30, 3498–3508. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M.; Negrini, S.; Weiss, H.R.; Grivas, T.B.; Maruyama, T.; Kotwicki, T. SOSORT “SOSORT Consensus Paper on Brace Action: TLSO Biomechanics of Correction (Investigating the Rationale for Force Vector Selection)”. Scoliosis 2006, 1, 11. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.E.; Durrani, A.A. Factors That Influence Outcome in Bracing Large Curves in Patients with Adolescent Idiopathic Scoliosis. Spine (Phila Pa 1976) 2001, 26, 2354–2361. [Google Scholar] [CrossRef]
- Negrini, N.; Di Felice, F.; Negrini, F.; Rebagliati, G.; Zaina, F.; Donzelli, S. Predicting Final Results of Brace Treatment of Adolescents with Idiopathic Scoliosis: First out-of-Brace Radiograph Is Better than in-Brace Radiograph-SOSORT 2020 Award Winner. Eur. Spine J. 2022. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FPB | VRB | |||||
|---|---|---|---|---|---|---|
| Average | SD | Average | SD | p | ||
| Number | 25 | 777 | ||||
| Males | 16% | 11% | NS | |||
| Age | years | 13.3 | 1.5 | 13.1 | 1.5 | NS |
| Risser | score | 1.4 | 1.4 | 1.7 | 1.4 | NS |
| Age at menarche | years | 11.6 | 1.3 | 11.8 | 1.1 | NS |
| Menarche | 64% | 66% | NS | |||
| Weight | kg | 49.4 | 11.3 | 49.9 | 8.8 | NS |
| Height | cm | 159.8 | 8.7 | 158.7 | 7.3 | NS |
| BMI | kg/sqm | 19.3 | 3.6 | 19.8 | 2.9 | NS |
| Previous brace | 20% | 46% | 0.009 | |||
| Main curve | Cobb degrees | 48.3 | 10.0 | 46.7 | 7.4 | NS |
| Thoracic proximal | 4% | 1% | NS | |||
| Thoracic | 64% | 71% | ||||
| Thoracolumbar | 20% | 14% | ||||
| Lumbar | 8% | 13% | ||||
| Main prominence | ATR degrees | 13.0 | 3.9 | 12.8 | 3.4 | NS |
| Aesthetics | TRACE index | 8.5 | 1.9 | 8.3 | 1.9 | NS |
| Plumbline C7 + L3 | mm | 46.4 | 30.3 | 46.5 | 25.6 | NS |
| Plumbline C7 − S1 | mm | 0.2 | 20.6 | −0.9 | 17.7 | NS |
| Declared brace use | 23.1 | 0.5 | 22.9 | 0.4 | 0.027 | |
| Recorded brace use | 0.9 | 0.0 | 0.9 | 0.1 | 0.000 | |
| FPB (N = 25) | VRB (N = 777) | p | ||||||
|---|---|---|---|---|---|---|---|---|
| Improved | Unchanged | Progressed | Improved | Unchanged | Progressed | |||
| Main curve | Cobb degrees | 68% | 32% | 0% | 77% | 23% | 1% | NS |
| Main prominence | ATR degrees | 60% | 40% | 0% | 60% | 40% | 2% | NS |
| Aesthetics | TRACE index | 68% | 32% | 0% | 70% | 30% | 0% | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Negrini, S.; Tessadri, F.; Negrini, F.; Tavernaro, M.; Zonta, A.; Zaina, F.; Donzelli, S. Impact of the Free-Pelvis Innovation in Very Rigid Braces for Adolescents with Idiopathic Scoliosis: Short-Term Results of a Matched Case-Control Study. Children 2022, 9, 871. https://doi.org/10.3390/children9060871
Negrini S, Tessadri F, Negrini F, Tavernaro M, Zonta A, Zaina F, Donzelli S. Impact of the Free-Pelvis Innovation in Very Rigid Braces for Adolescents with Idiopathic Scoliosis: Short-Term Results of a Matched Case-Control Study. Children. 2022; 9(6):871. https://doi.org/10.3390/children9060871
Chicago/Turabian StyleNegrini, Stefano, Fabrizio Tessadri, Francesco Negrini, Marta Tavernaro, Andrea Zonta, Fabio Zaina, and Sabrina Donzelli. 2022. "Impact of the Free-Pelvis Innovation in Very Rigid Braces for Adolescents with Idiopathic Scoliosis: Short-Term Results of a Matched Case-Control Study" Children 9, no. 6: 871. https://doi.org/10.3390/children9060871
APA StyleNegrini, S., Tessadri, F., Negrini, F., Tavernaro, M., Zonta, A., Zaina, F., & Donzelli, S. (2022). Impact of the Free-Pelvis Innovation in Very Rigid Braces for Adolescents with Idiopathic Scoliosis: Short-Term Results of a Matched Case-Control Study. Children, 9(6), 871. https://doi.org/10.3390/children9060871