
The Effect of Timing of Mandibular Distraction Osteogenesis on Weight Velocity in Infants Affected by Severe Robin Sequence


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Study Variables
2.3. Statistical Analysis
3. Results
3.1. Sample Distribution
3.2. Weight Outcomes at Different Timing Points
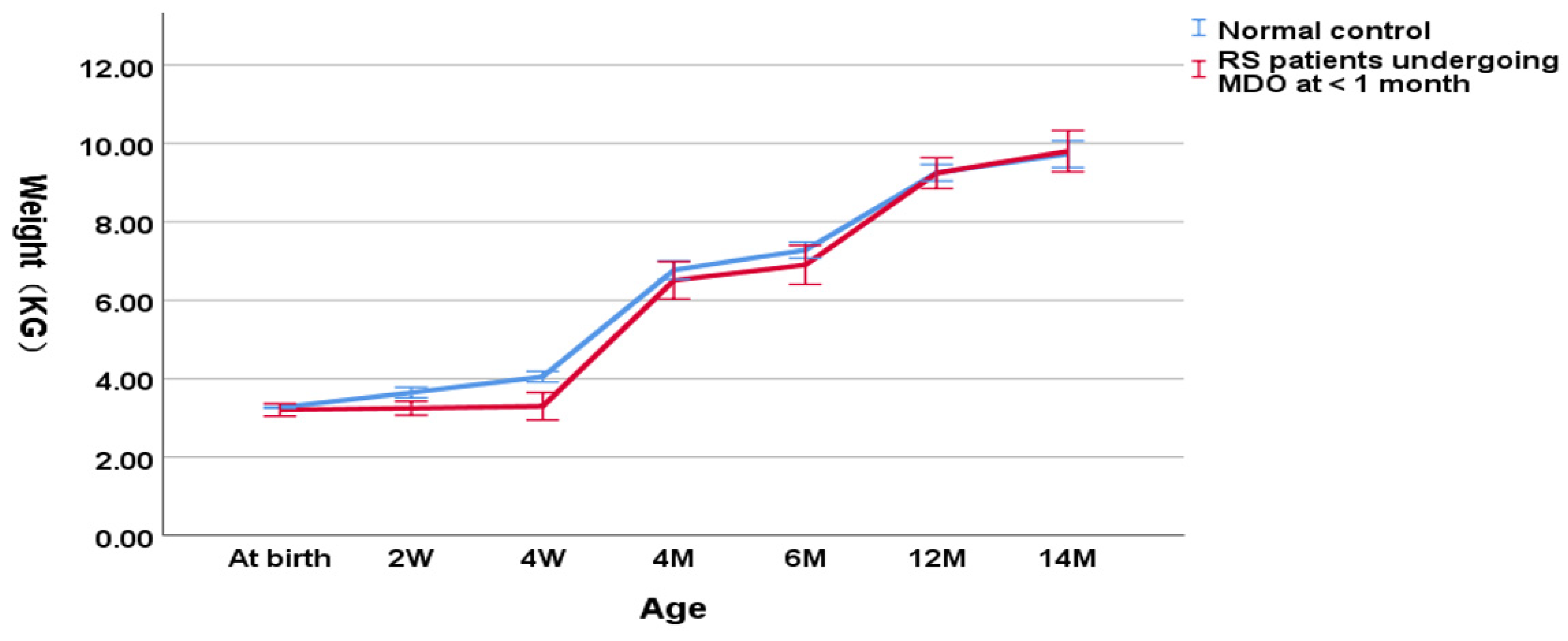
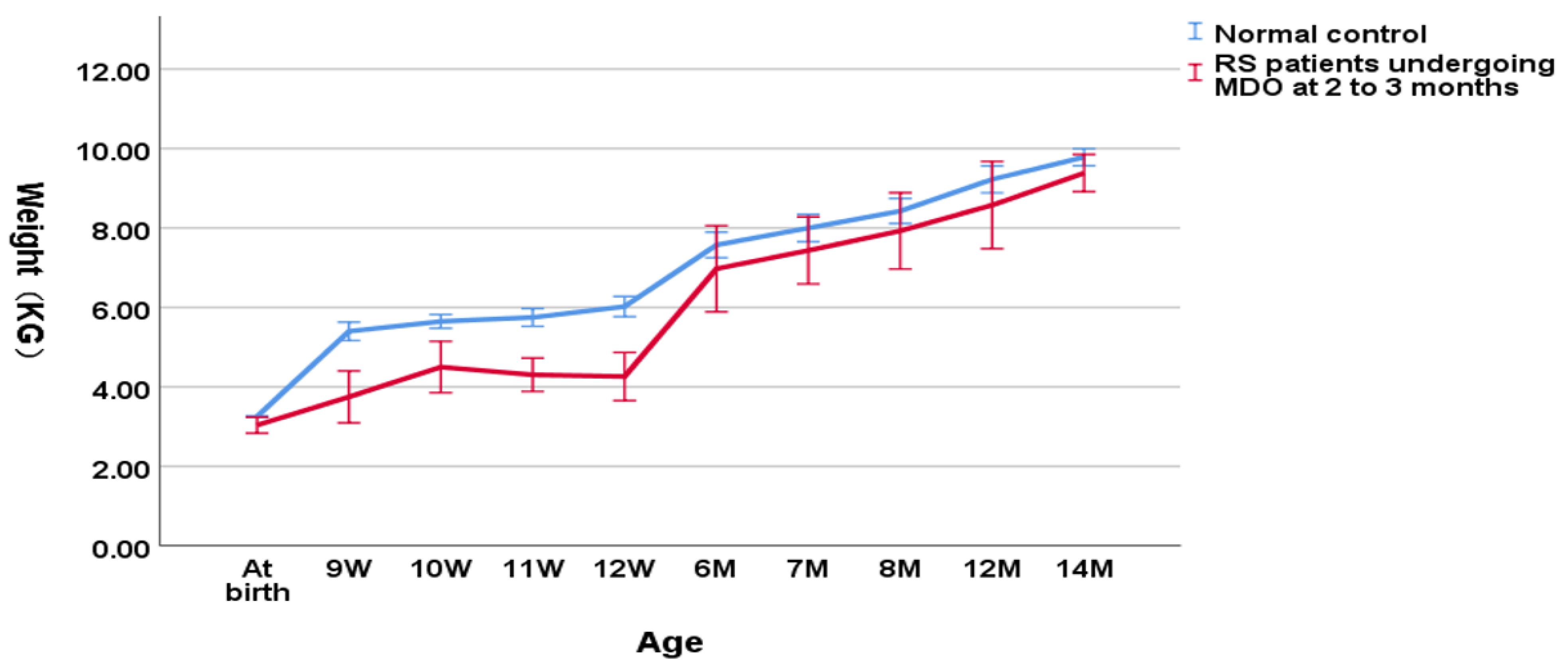
3.3. Weight Outcomes Intervened by MDO Surgical Age
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Izumi, K.; Konczal, L.L.; Mitchell, A.L.; Jones, M.C. Underlying Genetic Diagnosis of Pierre Robin Sequence: Retrospective Chart Review at Two Children’s Hospitals and a Systematic Literature Review. J. Pediatr. 2012, 160, 645–650.e2. [Google Scholar] [CrossRef] [PubMed]
- Vatlach, S.; Maas, C.; Poets, C.F. Birth prevalence and initial treatment of Robin sequence in Germany: A prospective epidemiologic study. Orphanet J. Rare Dis. 2014, 9, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakobsen, L.P.; Knudsen, M.A.; Lespinasse, J.; García Ayuso, C.; Ramos, C.; Fryns, J.P.; Bugge, M.; Tommerup, N. The genetic basis of the Pierre Robin sequence. Cleft Palate-Craniofac. J. 2006, 43, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, L.P.; Ullmann, R.; Christensen, S.B.; Jensen, K.E.; Mølsted, K.; Henriksen, K.F.; Hansen, C.; Knudsen, M.A.; Larsen, L.A.; Tommerup, N.; et al. Pierre Robin sequence may be caused by dysregulation of SOX9 and KCNJ2. J. Med. Genet. 2007, 44, 381–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, S.T.; Woo, A.S. Pierre Robin sequence. Clin. Plast. Surg. 2019, 46, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Gangopadhyay, N.; Mendonca, D.A.; Woo, A.S. Pierre robin sequence. Semin. Plast. Surg. 2012, 26, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Tomic, J.; Metzler, P.; Alcon, A.; Jakse, N.; Zemann, W.; Schanbacher, M.; Zrnc, T.A. Weight gain in infants with Pierre Robin sequence. J. Cranio-Maxillofac. Surg. 2020, 48, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Gary, C.S.; Marczewski, S.; Vitagliano, P.M.; Sawh-Martinez, R.; Wu, R.; Steinbacher, D.M. A Quantitative Analysis of Weight Gain Following Mandibular Distraction Osteogenesis in Robin Sequence. J. Craniofac. Surg. 2018, 29, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Breik, O.; Umapathysivam, K.; Tivey, D.; Anderson, P. Feeding and reflux in children after mandibular distraction osteogenesis for mi-crognathia: A systematic review. Int. J. Pediatric Otorhinolaryngol. 2016, 85, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Breik, O.; Tivey, D.; Umapathysivam, K.; Anderson, P. Mandibular distraction osteogenesis for the management of upper airway obstruction in children with micrognathia: A systematic review. Int. J. Oral Maxillofac. Surg. 2016, 45, 769–782. [Google Scholar] [CrossRef]
- Adhikari, A.N.; Heggie, A.A.; Shand, J.M.; Bordbar, P.; Pellicano, A.; Kilpatrick, N. Infant mandibular distraction for upper airway obstruction: A clinical audit. Plast. Reconstr. Surg. Glob. Open 2016, 4, e812. [Google Scholar] [CrossRef] [PubMed]
- Mudd, P.A.; Perkins, J.N.; Harwood, J.E.; Valdez, S.; Allen, G.C. Early intervention: Distraction osteogenesis of the mandible for severe airway obstruction. Otolaryngol. Head Neck Surg. 2012, 146, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Spring, M.A.; Mount, D.L. Pediatric Feeding Disorder and Growth Decline following Mandibular Distraction Osteogenesis. Plast. Reconstr. Surg. 2006, 118, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Khansa, I.; Hall, C.; Madhoun, L.L.; Splaingard, M.; Baylis, A.; Kirschner, R.E.; Pearson, G.D. Airway and feeding outcomes of mandibular distraction, tongue-lip adhesion, and Conservative management in Pierre robin sequence: A prospective study. Plast. Reconstr. Surg. 2017, 139, 975e–983e. [Google Scholar] [CrossRef] [PubMed]
- Breugem, C.C.; Evans, K.N.; Poets, C.F.; Suri, S.; Picard, A.; Filip, C.; Paes, E.C.; Mehendale, F.V.; Saal, H.M.; Basart, H.; et al. Best practices for the diagnosis and evaluation of infants with robin sequence: A clinical consensus report. JAMA Pediatr. 2016, 170, 894–902. [Google Scholar] [CrossRef] [Green Version]
- Mao, Z.; Zhang, N.; Shu, L.; Cui, Y. Imaging characteristics of the mandible and upper airway in children with Robin sequence and relationship to the treatment strategy. Int. J. Oral Maxillofac. Surg. 2020, 49, 1122–1127. [Google Scholar] [CrossRef]
- Mao, Z.; Ye, L. Effects of Mandibular Distraction Osteogenesis on Three-Dimensional Upper Airway Anatomy in Newborns Affected by Isolated Pierre Robin Sequence. J. Craniofac. Surg. 2021, 32, 1459–1463. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chen, Y.; Li, F.; Wu, W.; Hao, J.; Luo, D.; Wang, H. Condylar positions before and after bilateral mandibular distraction osteogenesis in children with Pierre Robin sequence. Int. J. Oral Maxillofac. Surg. 2018, 47, 57–63. [Google Scholar] [CrossRef]
- Cole, S.Z.; Lanham, J.S. Failure to thrive: An update. Am. Fam. Phys. 2011, 83, 21. [Google Scholar]
- Collins, C.E.; MacDonald-Wicks, L.; Rowe, S.; O’Loughlin, E.V.; Henry, R.L. Normal growth in cystic fibrosis associated with a specialized centre. Arch. Dis. Child. 1999, 81, 241–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zemel, B.S.; Pipan, M.; Stallings, V.A.; Hall, W.; Schadt, K.; Freedman, D.S.; Thorpe, P. Growth Charts for Children with Down Syndrome in the United States. Pediatrics 2015, 136, e1204–e1211. [Google Scholar] [CrossRef] [Green Version]
- Shprintzen, R.J. The Implications of the Diagnosis of Robin Sequence. Cleft Palate-Craniofac. J. 1992, 29, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Jensen, B.L.; Kreiborg, S.; Dahl, E.; Fogh-Andersen, P. Cleft lip and palate in Denmark, 1976–1981: Epidemiology, variability, and early somatic development. Cleft Palate J. 1988, 25, 25. [Google Scholar]
- Luo, D.; Chen, Y.; Wang, H.; Li, T.; Fan, L.; Wenli, W.; Jiayu, L.; Jiansuo, H. The Effect of Mandibular Distraction Osteogenesis on Weight Velocity in Infants with Severe Pierre Robin Syndrome. J. Craniofac. Surg. 2018, 29, 1851–1854. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.B.; Pashayan, H.M. Management of infants with Robin anomaly. Clin. Pediatr. 1980, 19, 519–521. [Google Scholar] [CrossRef]
- Monasterio, F.O.; Molina, F.; Berlanga, F.; López, M.E.; Ahumada, H.; Takenaga, R.H.; Ysunza, A. Swallowing Disorders in Pierre Robin Sequence: Its Correction by Distraction. J. Craniofac. Surg. 2004, 15, 934–941. [Google Scholar] [CrossRef]
- da Silva Freitas, R.; Lopes-Grego, A.B.; Dietrich, H.L.D.; de Moraes Cerchiari, N.R.; Nakakogue, T.; Tonocchi, R.; Gabardo, J.; da Silva, E.D.B.; Forte, A.J. Weight gain in children with cleft lip and palate without use of palatal plates. Plast. Surg. Int. 2012, 2012, 973240. [Google Scholar] [CrossRef] [Green Version]
- Al-Samkari, H.T.; Kane, A.A.; Molter, D.W.; Vachharajani, A. Neonatal outcomes of Pierre Robin sequence: An institutional expe-rience. Clin. Pediatr. 2010, 49, 1117–1122. [Google Scholar] [CrossRef] [PubMed]
- Skillman, J.; Cole, A.; Slator, R. Sodium Supplementation in Neonates with Pierre Robin Sequence Significantly Improves Weight Gain if Urinary Sodium is Low. Cleft Palate-Craniofac. J. 2012, 49, 39–43. [Google Scholar] [CrossRef]
- Anderson, K.D.; Cole, A.; Chuo, C.B.; Slator, R. Home Management of Upper Airway Obstruction in Pierre Robin Sequence Using a Nasopharyngeal Airway. Cleft Palate-Craniofac. J. 2007, 44, 269–273. [Google Scholar] [CrossRef]
- Almajed, A.; Viezel-Mathieu, A.; Gilardino, M.S.; Flores, R.L.; Tholpady, S.; Côté, A. Outcome following Surgical Interventions for Micrognathia in Infants with Pierre Robin Sequence: A Systematic Review of the Literature. Cleft Palate-Craniofac. J. 2017, 54, 32–42. [Google Scholar] [CrossRef]
- Resnick, C.M.; Calabrese, C.E.; Sahdev, R.; Padwa, B.L. Is Tongue-Lip Adhesion or Mandibular Distraction More Effective in Relieving Obstructive Apnea in Infants with Robin Sequence? J. Oral Maxillofac. Surg. 2019, 77, 591–600. [Google Scholar] [CrossRef]
- Hong, P.; Bezuhly, M.; Taylor, S.M.; Hart, R.D.; Kearns, D.B.; Corsten, G. Tracheostomy versus mandibular distraction osteogenesis in Canadian children with Pierre Robin sequence: A comparative cost analysis. J. Otolaryngol. Head Neck Surg. 2012, 41, 207–214. [Google Scholar]
- Li, L.; Scott, A.R. Weight Gain in Infants with Pierre Robin Sequence in the First Year of Life. Otolaryngol. Head Neck Surg. 2020, 163, 1032–1037. [Google Scholar] [CrossRef]
- Dauria, D.; Marsh, J.L. Mandibular distraction osteogenesis for Pierre Robin sequence: What percentage of neonates need it? J. Craniofac. Surg. 2008, 19, 1237–1243. [Google Scholar] [CrossRef]
- Daniel, M.; Bailey, S.; Walker, K.; Hensley, R.; Kol-Castro, C.; Badawi, N.; Cheng, A.; Waters, K. Airway, feeding and growth in infants with Robin sequence and sleep apnoea. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 499–503. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| <1 Month for MDO | 1 to 2 Months for MDO | 2 to 3 Months for MDO | 3 to 4 Months for MDO | |
|---|---|---|---|---|
| Gender (Male/Female) | 18/10 | 19/21 | 14/3 | 7/8 |
| Classification (Isolated RS/Syndromic RS) | 21/7 | 31/9 | 15/2 | 14/1 |
| Cleft Palate (No/Yes) | 0/28 | 2/38 | 2/15 | 1/14 |
| Average Age of Patients Undergoing MDO | 2 weeks | 6 weeks | 11 weeks | 14 weeks |
| Timing Point | Number | Weight (kg) | t | p | ||
|---|---|---|---|---|---|---|
| PRS Patient | Normal Control | PRS Patient | Normal Control | |||
| At birth | 100 | 100 | 3.06 ± 0.48 | 3.26 ± 0.05 | −4.166 | p = 0.000066 p < 0.01 |
| MDO | 100 | 100 | 3.58 ± 0.67 | 4.97 ± 0.91 | −16.148 | p = 0.0000 p < 0.01 |
| Post-discharge Weight | 100 | 100 | 4.05 ± 0.66 | 5.57 ± 0.76 | −17.497 | p = 0.0000 p < 0.01 |
| Distractor Removal | 100 | 100 | 7.03 ± 0.11 | 7.60 ± 0.83 | −6.407 | p = 0.0000 p < 0.01 |
| Cleft Palate Surgery | 100 | 100 | 9.12 ± 0.12 | 9.56 ± 0.09 | −3.450 | p = 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mao, Z.; Battaglino, R.; Zhou, J.; Cui, Y.; Shrivastava, M.; Tian, G.; Sahebdel, F.; Ye, L. The Effect of Timing of Mandibular Distraction Osteogenesis on Weight Velocity in Infants Affected by Severe Robin Sequence. Children 2022, 9, 319. https://doi.org/10.3390/children9030319
Mao Z, Battaglino R, Zhou J, Cui Y, Shrivastava M, Tian G, Sahebdel F, Ye L. The Effect of Timing of Mandibular Distraction Osteogenesis on Weight Velocity in Infants Affected by Severe Robin Sequence. Children. 2022; 9(3):319. https://doi.org/10.3390/children9030319
Chicago/Turabian StyleMao, Zhe, Ricardo Battaglino, Jiawei Zhou, Yingqiu Cui, Mayank Shrivastava, Gabriel Tian, Faezeh Sahebdel, and Liang Ye. 2022. "The Effect of Timing of Mandibular Distraction Osteogenesis on Weight Velocity in Infants Affected by Severe Robin Sequence" Children 9, no. 3: 319. https://doi.org/10.3390/children9030319
APA StyleMao, Z., Battaglino, R., Zhou, J., Cui, Y., Shrivastava, M., Tian, G., Sahebdel, F., & Ye, L. (2022). The Effect of Timing of Mandibular Distraction Osteogenesis on Weight Velocity in Infants Affected by Severe Robin Sequence. Children, 9(3), 319. https://doi.org/10.3390/children9030319