
Histopathological Records of Oral and Maxillofacial Lesions among Pediatric and Adolescent Patients in Sulaimani Governorate


Abstract
1. Introduction
2. Materials and Methods
2.1. Sample of the Study
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mouchrek, M.M.M.; Gonçalves, L.M.; Bezerra-Júnior, J.R.S.; Maia, E.D.C.S.; Da Silva, R.A.; Da Cruz, M.C.F.N. Oral and maxillofacial biopsied lesions in Brazilian pediatric patients: A 16-year retrospective study. Rev. Odonto. Cienc. 2011, 26, 222–226. [Google Scholar] [CrossRef][Green Version]
- Khiavi, M.M.; Haghi-Ashtiani, M.T.; Kharazi-Fard, M.J.; Kalantar, R. Frequency of head and neck masses in iranian children during a 21-year period. Iran. J. Pediatr. 2018, 28, e64087. [Google Scholar] [CrossRef]
- De Carvalho, G.M.; De Lavor, M.S.; Rickli, J.C.K.; Takara, T.F.M.; Guimarães, A.C.; Crespo, A.N. Pediatric neck mass. Int. J. Pediatr. 2015, 3, 1005–1014. [Google Scholar] [CrossRef]
- Tracy, T.F.; Muratore, C.S. Management of common head and neck masses. Semin. Pediatr. Surg. 2007, 16, 3–13. [Google Scholar] [CrossRef]
- Telander, R.L.; Filston, H.C. Review of head and neck lesions in infancy and childhood. Surg. Clin. N. Am. 1992, 72, 1429–1447. [Google Scholar] [CrossRef]
- Erikci, V.S. Clinics in Surgery Pediatric Congenital Neck Masses: A Review Article. Clin. Surg. 2017, 2, 1791. [Google Scholar]
- Brigger, M.T.; Cunningham, M.J. Malignant cervical masses in children. Otolaryngol. Clin. N. Am. 2015, 48, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Acierno, S.P.; Waldhausen, J.H.T. Congenital cervical cysts, sinuses and fistulae. Otolaryngol. Clin. N. Am. 2007, 40, 161–176. [Google Scholar] [CrossRef]
- Eşki, E.; Akdoğan, V.; Türkoğlu, S.B.; Sökmen, M.F.; Çaylaklı, F.; Özer, C.; Canpolat, E.T.; Yılmaz, I. Pediatric mass lesions of the head and neck region and fine-needle aspiration biopsy results. Turk. Arch. Otorhinolaryngol. 2016, 54, 29–34. [Google Scholar] [CrossRef]
- Erikci, V.S. Postoperative complications in children with congenital neck masses: A review article. J. Clinal. Res. Rep. 2020, 4, 01–03. [Google Scholar] [CrossRef]
- Lang, S.; Benjamin, K. Cervical lymph node diseases in children. GMS. Curr. Top. Otorhinolaryngol. Head. Neck. Surg. 2014, 13, 1–27. [Google Scholar]
- Deosthali, A.; Donches, K.; Delvecchio, M.; Aronoff, S. Etiologies of pediatric cervical lymphadenopathy: A systematic review of 2687 Subjects. Glob. Pediatr. Health 2019, 6, 1–7. [Google Scholar] [CrossRef]
- Chadha, N.K.; Forte, V. Pediatric head and neck malignancies. Curr. Opin. Otolaryngol. Head. Neck. Surg. 2009, 17, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Ragesh, K.P.; Chana, R.S.; Varshney, P.K.; Naim, M. Head and neck masses in children: A clinicopathological study. Indian J. Otolaryngol. Head. Neck. Surg. 2002, 54, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Sousa, F.B.; Etges, A.; Correa, L.; Mesquita, R.A.; de Araújo, N.S. Pediatric oral lesions: A 15-year review from São Paulo, Brazil. J. Clin. Pediatr. Dent. 2002, 26, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Gultelkin, S.E.; Tokman, B.; Turkseven, M.R. A review of paediatric oral biopsies in Turkey. Int. Dent. J. 2003, 53, 26–32. [Google Scholar] [CrossRef]
- Skiavounou-Andrikopoulou, A.; Piperi, E.; Papanikolaou, V.; Karakoulakis, I. Retrospective analysis over a 32-year period. J. Clin. Pediatr. Dent. 2005, 29, 175–178. [Google Scholar]
- Jones, A.V.; Franklin, C.D. An analysis of oral and maxillofacial pathology found in children over a 30-year period. Int. J. Paediatr. Dent. 2006, 16, 19–30. [Google Scholar] [CrossRef]
- Al Yamani, A.O.; Al Sebaei, M.O.; Bassyoni, L.J.; Badghaish, A.J.; Shawly, H.H. Variation of pediatric and adolescents head and neck pathology in the city of Jeddah: A retrospective analysis over 10 years. Saudi. Dent. J. 2011, 23, 197–200. [Google Scholar] [CrossRef]
- Abdullah, B.H.; Abdul Qader, O.A.; Mussedi, O.S. Retrospective analysis of 1286 oral and maxillofacial biopsied lesions of Iraqi children over a 30 years period. Pediatr. Dent. J. 2015, 5–9. [Google Scholar] [CrossRef]
- Al-Mayoof, A.F. Neck masses in paediatric population: An experience with children attended the Central Teaching Hospital of Pediatrics in Baghdad 2008-2009. Afr. J. Paediatr. Surg. 2015, 12, 136–139. [Google Scholar] [CrossRef]
- Yakin, M.; Jalal, J.A.; Al-khurri, L.E.; Rich, A.M. Oral and maxillofacial pathology submitted to Rizgary Teaching Hospital: A 6-year retrospective study. Int. Dent. J. 2016, 66, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Aljazaeri, S.A.W.; Al Qudsi, G.H.; Jaber, H.K.; Al Elwi, W.M.; Haddad, S.S. Biopsy records to the oral lesions in Basrah between 2012–2017. Oral. Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 6, 74–80. [Google Scholar] [CrossRef]
- Fahad, A.H.; Musa, S.Q. Prevalence of oral lesions in Al-Muthannagovernorate, Iraq: ( Clinicopathological study). Int. J. Enhanc. Res. Sci. Technol. Eng. 2018, 7, 2319–7463. [Google Scholar]
- Laurenti, R. Analysis of information on health data: 1893-1993, a hundred years of the International Classification of Diseases. Rev. Saude. Publica. S Paulo. 1991, 25, 407–417. [Google Scholar] [CrossRef]
- World Health Organization. 2015. International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Fifth edition. 2016. Available online: https://apps.who.int/iris/handle/10665/246208 (accessed on 1 October 2021).
- Mahmoudi, P.; Razavi, S.M.; Tahani, B. Orofacial pathological lesions in children and adolescents: A 25-year survey in Iran. J. Dent. Shiraz. Univ. Med. Sci. 2018, 19, 265–272. [Google Scholar]
- Khudeda, M.M.; Mudhir, M.A. The prevalence of dental careis among 6–12 years-old school children in Sharia camp. Duhok Med. J. 2018, 12, 55–62. [Google Scholar] [CrossRef][Green Version]
- Nibras, A.M.; Ahmed, N.A.M.; Anne N Åstrøm, A.N.; Skaug, N.; Petersen, P.E. Dental caries prevalence and risk factors among 12-year old schoolchildren from Baghdad, Iraq: A post-war survey. Int. Dent. J. 2007, 57, 36–44. [Google Scholar] [CrossRef]
- Khamrco, T.Y.; AL-Ajrab, M.G.H. Prevalence of dental caries (DMFT) in Iraqi children and adolescents living in areas with low and high level of natural fluoride. RDENTJ. 2001, 1, 385–400. [Google Scholar] [CrossRef]
- Maaita, J.K. Oral tumors in children: A review. J. Clin. Pediatr. Dent. 2000, 24, 133–135. [Google Scholar]
- Dhanuthai, K.; Banrai, M.; Limpanaputtajak, S. A retrospective study of paediatric oral lesions from Thailand. Int. J. Paediatr. Dent. 2007, 17, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Parra Sanabria, E.A.; Peña Vega, C.P. Frequency of oral and maxillofacial pathologies in patients from 0 to 18 years in the fundación hospital de la misericordia bogotá (Colombia), during the period 2006-2014. Univ. Med. 2018, 59. [Google Scholar] [CrossRef]
- Wang, Y.L.; Chang, H.H.; Chang, J.Y.; Huang, G.F.; Guo, M.K. Retrospective survey of biopsied oral lesions in pediatric patients. J. Formos. Med. Assoc. 2009, 108, 862–871. [Google Scholar] [CrossRef]
- Lima, G.D.S.; Fontes, S.T.; Aver de Araujo, L.M.; Etges, A.; Tarquinio, S.B.C.; Gomez, A.P.N. A survey of oral and maxillofacial biopsies in children. A single-center retrospective study of 20 years in Pelotas-Brazil. J. Appl. Oral. Sci. 2008, 16, 397–402. [Google Scholar] [CrossRef] [PubMed]
- De Paula, D.S.; Nóbrega Malta, C.E.; De Brito, W.H.; Mota Lemos, J.V.; Cetira Fillho, E.L.; Gurgel Costa, F.W.; Nunes Alves, A.P.N.; De Barros Silva, P.G. Prevalence of malignant neoplastic oral lesions among children and adolescents: A systematic review and meta-analysis. Int. J. Paediatr. Dent. 2021, 31, 504–519. [Google Scholar] [CrossRef] [PubMed]
- Rwakatema, D.S.; Chindia, M.L. An audit of Paediatric Orofacial Lesions at the Kilimanjaro Christian Medical Centre in Moshi, Tanzania. Surg. Sci. 2011, 2, 476–480. [Google Scholar] [CrossRef][Green Version]
- Zuniga, M.D.; Mendez, C.R.; Kauterich, R.R.; Paniagua, D.C. Paediatric oral pathology in a Chilean population: A 15-year review. Int. J. Paediatr. Dent. 2013, 23, 346–351. [Google Scholar] [CrossRef]
- Shah, S.K.; Le, M.C.; Carpenter, W.M. Retrospective review of pediatric oral lesions from a dental school biopsy service. Pediatr. Dent. 2009, 31, 14–19. [Google Scholar]
- Lapthanasupkul, P.; Juengsomjit, R.; Klanrit, P.; Taweechaisupapong, S.; Poomsawat, S. Oral and maxillofacial lesions in a Thai pediatric population: A retrospective review from two dental schools. J. Med. Assoc. Thai. 2015, 98, 291–297. [Google Scholar]
- Lei, F.; Chen, J.Y.; Lin, L.M.; Wang, W.C.; Huang, H.C.; Chen, C.H.; Ho, K.Y.; Chen, Y.K. Retrospective study of biopsied oral and maxillofacial lesions in pediatric patients from Southern Taiwan. J. Dent. Sci. 2014, 9, 351–358. [Google Scholar] [CrossRef]
- Maia, D.M.; Merly, F.; Castro, W.H.; Gomez, R.S. A survey of oral biopsies in Brazilian pediatric patients. ASDC J. Dent. Child. 2000, 67, 128–131, 83. [Google Scholar] [PubMed]
- Trobs, R.B.; Mader, E.; Friedrich, T.; Bennek, J. Oral tumors and tumor-like lesions in infants and children. Pediatr. Surg. Int. 2003, 19, 639–645. [Google Scholar] [CrossRef] [PubMed]



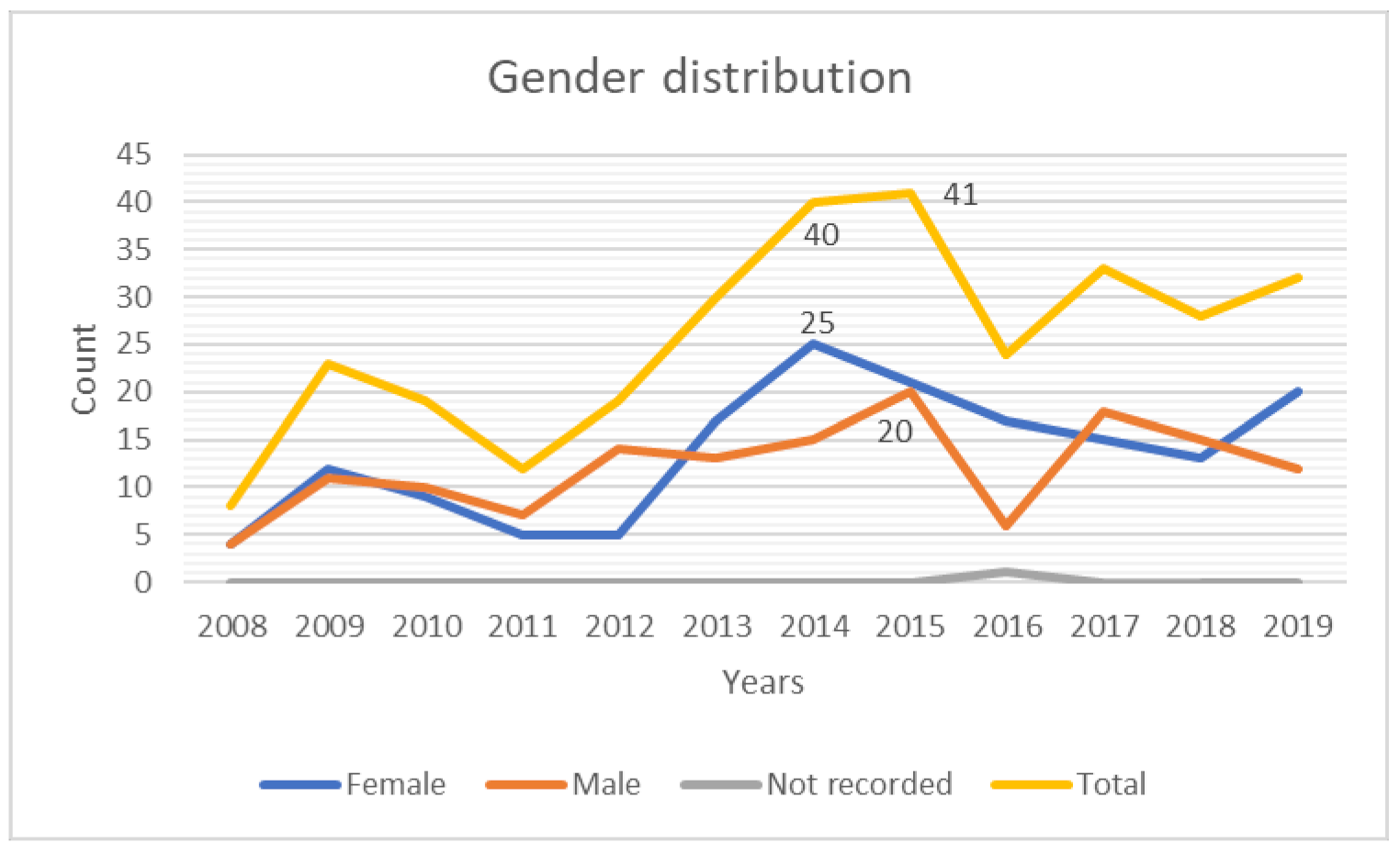{kind=link}
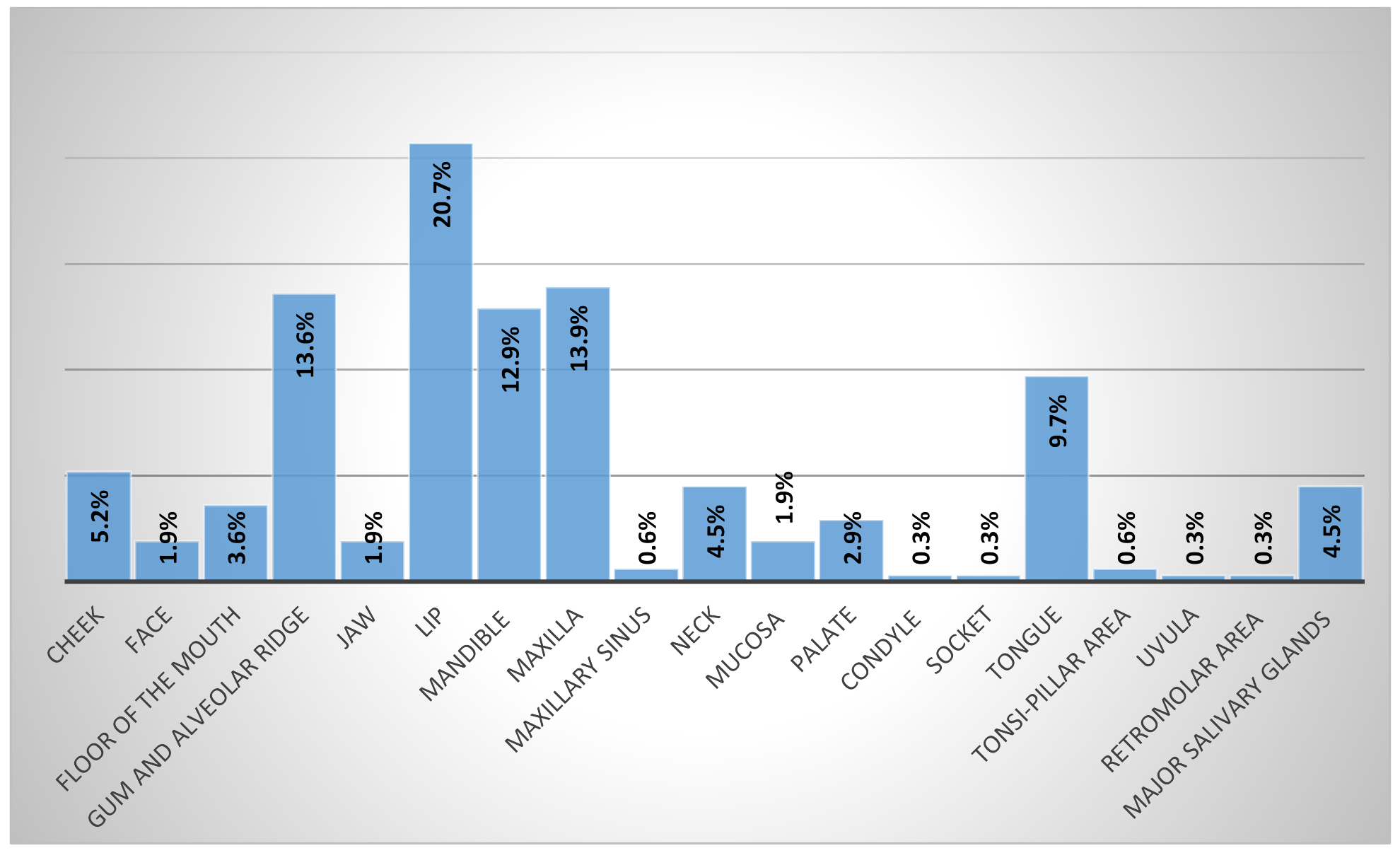{kind=link}
| Diagnosis Group | Age Group | Sex * | Type of Biopsy ≠ | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0–5 | 6–10 | 11–15 | 16–18 | Female | Male | Total | Incision | Excision | Inc/Excision | |
| Bone lesions | 1 | 5 | 7 | 0 | 3 | 10 | 13 (4.2%) | 2 | 9 | 2 |
| Bone tumors | 1 | 1 | 1 | 3 | 4 | 2 | 6 (1.9%) | 2 | 3 | 0 |
| Connective tissue tumors | 9 | 10 | 10 | 7 | 20 | 16 | 36 (11.6%) | 2 | 32 | 2 |
| Cystic lesions | 5 | 9 | 17 | 7 | 18 | 20 | 38 (12.4%) | 8 | 30 | 0 |
| Epithelial lesions | 2 | 1 | 0 | 3 | 3 | 3 | 6 (1.9%) | 0 | 6 | 0 |
| Hematologic neoplasm | 2 | 0 | 2 | 0 | 2 | 2 | 4 (1.4%) | 0 | 3 | 1 |
| Hematoma | 0 | 1 | 3 | 0 | 1 | 3 | 4 (1.4%) | 0 | 4 | 0 |
| Infection | 0 | 0 | 2 | 2 | 3 | 1 | 4 (1.3%) | 2 | 2 | 0 |
| Developmental anomaly | 2 | 1 | 1 | 0 | 4 | 0 | 4 (1.3%) | 0 | 4 | 0 |
| Mucocutaneous diseases | 0 | 1 | 0 | 3 | 3 | 1 | 4 (1.3%) | 2 | 2 | 0 |
| Mucositis/ulceration | 2 | 1 | 2 | 1 | 4 | 2 | 6 (1.9%) | 1 | 5 | 0 |
| Normal | 1 | 0 | 5 | 1 | 1 | 6 | 7 (2.3%) | 5 | 2 | 0 |
| Odontogenic tumors | 7 | 0 | 1 | 1 | 2 | 7 | 9 (2.9%) | 5 | 0 | 4 |
| Periapical lesions | 2 | 1 | 14 | 12 | 18 | 10 | 29 *(9.3%) | 4 | 25 | 0 |
| Periodontal diseases | 1 | 0 | 0 | 1 | 2 | 0 | 2 (0.6%) | 0 | 2 | 0 |
| Reactive hyperplasia of Lymph node | 1 | 0 | 1 | 0 | 1 | 1 | 2 (0.6%) | 0 | 2 | 0 |
| Salivary gland diseases | 7 | 21 | 33 | 3 | 36 | 28 | 64 (20.7%) | 1 | 63 | 0 |
| Salivary gland tumors | 0 | 0 | 6 | 1 | 2 | 5 | 7 (2.3%) | 0 | 7 | 0 |
| Inflammation | 1 | 1 | 0 | 0 | 1 | 1 | 2 (0.6%) | 0 | 2 | 0 |
| Reactive hyperplasia of connective tissue | 5 | 14 | 28 | 10 | 34 | 23 | 57 (18.4%) | 2 | 55 | 0 |
| epithelial tumors | 1 | 0 | 2 | 1 | 1 | 3 | 4 (1.3%) | 0 | 4 | 0 |
| Physical and chemical injury | 1 | 0 | 0 | 0 | 1 | 0 | 1 (0.3%) | 0 | 1 | 0 |
| Total | 51 (16.5%) | 67 (21.7%) | 135 (43.7%) | 56 (18.1%) | 164 (53.1%) | 144 (46.9%) | 309 (100%) | 36 (11.8%) | 263 (86%) | 9 (2.2%) |
| Sex | Age Group | |||||||
|---|---|---|---|---|---|---|---|---|
| Diagnosis Group | Lesions | No. and % | Female | Male | 0–5 | 6–10 | 11–15 | 16–18 |
| Infection | Verrucous vulgaris | 1 (0.3%) | 1 | 0 | 0 | 0 | 1 | 0 |
| Toxoplasmosis | 1 (0.3%) | 1 | 0 | 0 | 0 | 1 | 0 | |
| Actinomycosis | 1 (0.3%) | 0 | 1 | 0 | 0 | 0 | 1 | |
| Granulomatosis | 1 (0.3%) | 1 | 0 | 0 | 0 | 0 | 1 | |
| Inflammation | Chronic sinusitis | 2 (0.6%) | 1 | 1 | 1 | 1 | 0 | 0 |
| Bone lesions | Cherubism | 1 (0.3%) | 1 | 0 | 1 | 0 | 0 | 0 |
| Central giant cell granuloma | 7 (2.2%) | 1 | 6 | 0 | 2 | 5 | 0 | |
| Osteomyelitis | 3 (0.9%) | 1 | 2 | 0 | 2 | 1 | 0 | |
| Fibrous dysplasia | 2 (0.6%) | 0 | 2 | 0 | 1 | 1 | 0 | |
| Developmental anomaly | Macroglossia | 1 (0.3%) | 1 | 0 | 1 | 0 | 0 | 0 |
| Congenital epulis | 3 (0.9%) | 3 | 0 | 1 | 1 | 1 | 0 | |
| Mucositis | Non-specific ulcer | 6 (1.9%) | 4 | 2 | 2 | 1 | 2 | 1 |
| Normal tissue | Normal | 7 (2.3%) | 1 | 6 | 1 | 0 | 5 | 1 |
| Mucocutaneous diseases | Pemphigus vulgaris | 2 (0.6%) | 2 | 0 | 0 | 0 | 0 | 2 |
| Lichen planus | 1 (0.3%) | 1 | 0 | 0 | 0 | 0 | 1 | |
| Lichenoid reaction | 1 (0.3%) | 0 | 1 | 0 | 1 | 0 | 0 | |
| Cystic lesions | Kerato-odontogenic cyst | 11 (3.5%) | 3 | 8 | 0 | 1 | 7 | 3 |
| Aneurysmal bone cysts | 4 (1.3%) | 4 | 0 | 2 | 0 | 0 | 2 | |
| Dentigerous cysts | 10 (3.2%) | 1 | 9 | 0 | 5 | 5 | 0 | |
| Developmental cysts * | 7 (2.2%) | 5 | 2 | 1 | 2 | 4 | 0 | |
| Dermoid-Epidermoid cysts | 4 (1.2%) | 3 | 1 | 2 | 1 | 0 | 1 | |
| Eruption cysts | 1 (0.3%) | 1 | 0 | 0 | 0 | 1 | 0 | |
| Calcifying odontogenic cyst | 1 (0.3% | 1 | 0 | 0 | 0 | 0 | 1 | |
| Periapical lesions | Granuloma | 6 (1.9%) | 4 | 2 | 0 | 0 | 4 | 2 |
| Abscess | 2 (0.6%) | 2 | 0 | 1 | 1 | 0 | 0 | |
| Periapical cyst | 21 (6.8%) ≠ | 12 | 8 | 1 | 0 | 10 | 10 | |
| Reactive hyperplasia of LN | Reactive hyperplasia of Lymph nodes | 2 (0.6%) | 1 | 1 | 1 | 0 | 1 | 0 |
| Periodontal diseases | Chronic gingivitis | 1 (0.3%) | 1 | 0 | 1 | 0 | 0 | 0 |
| Gingival fibromatosis | 1 (0.3%) | 1 | 0 | 0 | 0 | 0 | 1 | |
| Salivary gland diseases | Mucocele | 60 (19.4%) | 35 | 25 | 7 | 20 | 30 | 3 |
| Chronic sialadenitis | 2 (0.6%) | 0 | 2 | 0 | 0 | 2 | 0 | |
| Benign lymphoepithelial lesions | 1 (0.3%) | 1 | 0 | 0 | 0 | 1 | 0 | |
| Acute sialadenitis | 1 (0.3%) | 0 | 1 | 0 | 1 | 0 | 0 | |
| Reactive hyperplasia of connective tissue | Pyogenic granuloma | 27 (8.7%) | 18 | 9 | 2 | 7 | 13 | 5 |
| Peripheral giant cell granuloma | 16 (5.2%) | 8 | 8 | 2 | 4 | 8 | 2 | |
| Fibro-epithelial polyp | 14 (4.6%) | 8 | 6 | 1 | 3 | 7 | 3 | |
| Physical and chemical injuries | Eosinophilic granuloma | 1 (0.3%) | 1 | 0 | 1 | 0 | 0 | 0 |
| Hematoma | Hematoma | 4 (1.3%) | 1 | 3 | 0 | 1 | 3 | 0 |
| Epithelial lesions | Hyperkeratosis | 2 (0.6%) | 1 | 1 | 0 | 1 | 0 | 1 |
| Hyperplasia | 2 (0.6%) | 0 | 2 | 2 | 0 | 0 | 0 | |
| Intradermal nevus | 1 (0.3%) | 1 | 0 | 0 | 0 | 0 | 1 | |
| Dysplasia | 1 (0.3%) | 1 | 0 | 0 | 0 | 0 | 1 | |
| Total = 243 (78.6%) | ||||||||
| Sex | Age Group | |||||||
|---|---|---|---|---|---|---|---|---|
| Diagnosis Group | Lesions | No. and % | Female | Male | 0–5 | 6–10 | 11–15 | 16–18 |
| Bone tumor | Ossifying fibroma | 2 (0.6%) | 1 | 1 | 1 | 0 | 0 | 1 |
| Osteochondroma | 1 (0.3%) | 1 | 0 | 0 | 0 | 0 | 1 | |
| Osteoma | 1 (0.3%) | 1 | 0 | 0 | 0 | 0 | 1 | |
| Osteosarcoma | 1 (0.3%) | 1 | 0 | 0 | 1 | 0 | 0 | |
| Ewing’s sarcoma | 1 (0.3%) | 0 | 1 | 0 | 0 | 1 | 0 | |
| Hematologic neoplasms | Burkitt’s lymphoma | 1 (0.3%) | 1 | 0 | 1 | 0 | 0 | 0 |
| Lymphoma | 1 (0.3%) | 0 | 1 | 0 | 0 | 1 | 0 | |
| Langerhans cell histiocytosis X | 2 (0.6%) | 1 | 1 | 1 | 0 | 1 | 0 | |
| Connective tissue tumors | Hemangiopericytoma | 3 (0.9%) | 1 | 2 | 1 | 1 | 1 | 0 |
| Nodular fasciitis | 3 (0.9%) | 2 | 1 | 3 | 0 | 0 | 0 | |
| Hemangioma | 10 (3.2%) | 5 | 5 | 2 | 2 | 3 | 3 | |
| Cystic hygroma | 2 (0.6%) | 2 | 0 | 1 | 0 | 1 | 0 | |
| Neural tumor | 3 (0.9%) | 0 | 3 | 1 | 0 | 2 | 0 | |
| Lymphangioma | 3 (0.9%) | 2 | 1 | 0 | 2 | 0 | 1 | |
| Lipoma | 1 (0.3%) | 1 | 0 | 0 | 1 | 0 | 0 | |
| Fibroma | 1 (0.3%) | 1 | 0 | 0 | 1 | 0 | 0 | |
| Peripheral ossifying fibroma | 6 (1.9%) | 6 | 0 | 0 | 1 | 3 | 2 | |
| Lymphangioma-hemangioma | 2 (0.6%) | 0 | 2 | 0 | 2 | 0 | 0 | |
| Rhabdomyosarcoma | 2 (0.6%) | 0 | 2 | 1 | 0 | 0 | 1 | |
| Salivary gland tumors | Pleomorphic adenoma | 4 (1.3%) | 2 | 2 | 0 | 0 | 3 | 1 |
| Mucoepidermoid carcinoma | 3 (1%) | 0 | 3 | 0 | 0 | 3 | 0 | |
| Epithelial tumors | Squamous papilloma | 3 (1%) | 1 | 2 | 1 | 0 | 1 | 1 |
| Melanoma | 1 (0.3%) | 0 | 1 | 0 | 0 | 1 | 0 | |
| Odontogenic tumors | Ameloblastic fibroma | 3 (1%) | 0 | 3 | 3 | 0 | 0 | 0 |
| Ameloblastoma | 1 (0.3%) | 1 | 0 | 1 | 0 | 0 | 0 | |
| Odontoma | 2 (0.6%) | 0 | 2 | 1 | 0 | 0 | 1 | |
| Odontogenic fibroma | 1 (0.3%) | 0 | 1 | 0 | 0 | 1 | 0 | |
| Melanotic neuroectodermal tumor | 2 (0.6%) | 1 | 1 | 2 | 0 | 0 | 0 | |
| Total = 66 (21.4%) | ||||||||
| Malignancies | Age Group | Sex | ||||
|---|---|---|---|---|---|---|
| 0–5 | 6–10 | 11–15 | 16–18 | Female | Male | |
| Osteosarcoma | 0 | 1 | 0 | 0 | 1 | 0 |
| Ewing’s sarcoma | 0 | 0 | 1 | 0 | 0 | 1 |
| Burkitt’s lymphoma | 1 | 0 | 0 | 0 | 1 | 0 |
| Lymphoma | 0 | 0 | 1 | 0 | 0 | 1 |
| Melanoma | 0 | 0 | 1 | 0 | 0 | 1 |
| Mucoepidermoid | 0 | 0 | 3 | 0 | 0 | 3 |
| Rhabdomyosarcoma | 1 | 0 | 0 | 1 | 0 | 2 |
| Total 10 (3%) | 2 (0.6%) | 1 (0.3%) | 6 (1.8%) | 1 (0.3%) | 2 (0.6%) | 8 (2.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohammad, D.N.; Ibraheem, B.F.; Garib, B.T.; Hamied, M.A.-S. Histopathological Records of Oral and Maxillofacial Lesions among Pediatric and Adolescent Patients in Sulaimani Governorate. Children 2022, 9, 156. https://doi.org/10.3390/children9020156
Mohammad DN, Ibraheem BF, Garib BT, Hamied MA-S. Histopathological Records of Oral and Maxillofacial Lesions among Pediatric and Adolescent Patients in Sulaimani Governorate. Children. 2022; 9(2):156. https://doi.org/10.3390/children9020156
Chicago/Turabian StyleMohammad, Dena Nadhim, Ban Falih Ibraheem, Balkees Taha Garib, and Marwa Abdul-Salam Hamied. 2022. "Histopathological Records of Oral and Maxillofacial Lesions among Pediatric and Adolescent Patients in Sulaimani Governorate" Children 9, no. 2: 156. https://doi.org/10.3390/children9020156
APA StyleMohammad, D. N., Ibraheem, B. F., Garib, B. T., & Hamied, M. A.-S. (2022). Histopathological Records of Oral and Maxillofacial Lesions among Pediatric and Adolescent Patients in Sulaimani Governorate. Children, 9(2), 156. https://doi.org/10.3390/children9020156