
Active Video Games Performance and Heart Rate on the Wii or Kinect in Children with and without Developmental Coordination Disorder

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Instruments
2.4. Randomization
2.5. Training and Procedure
2.6. Data Analysis
3. Results
3.1. Group Comparability
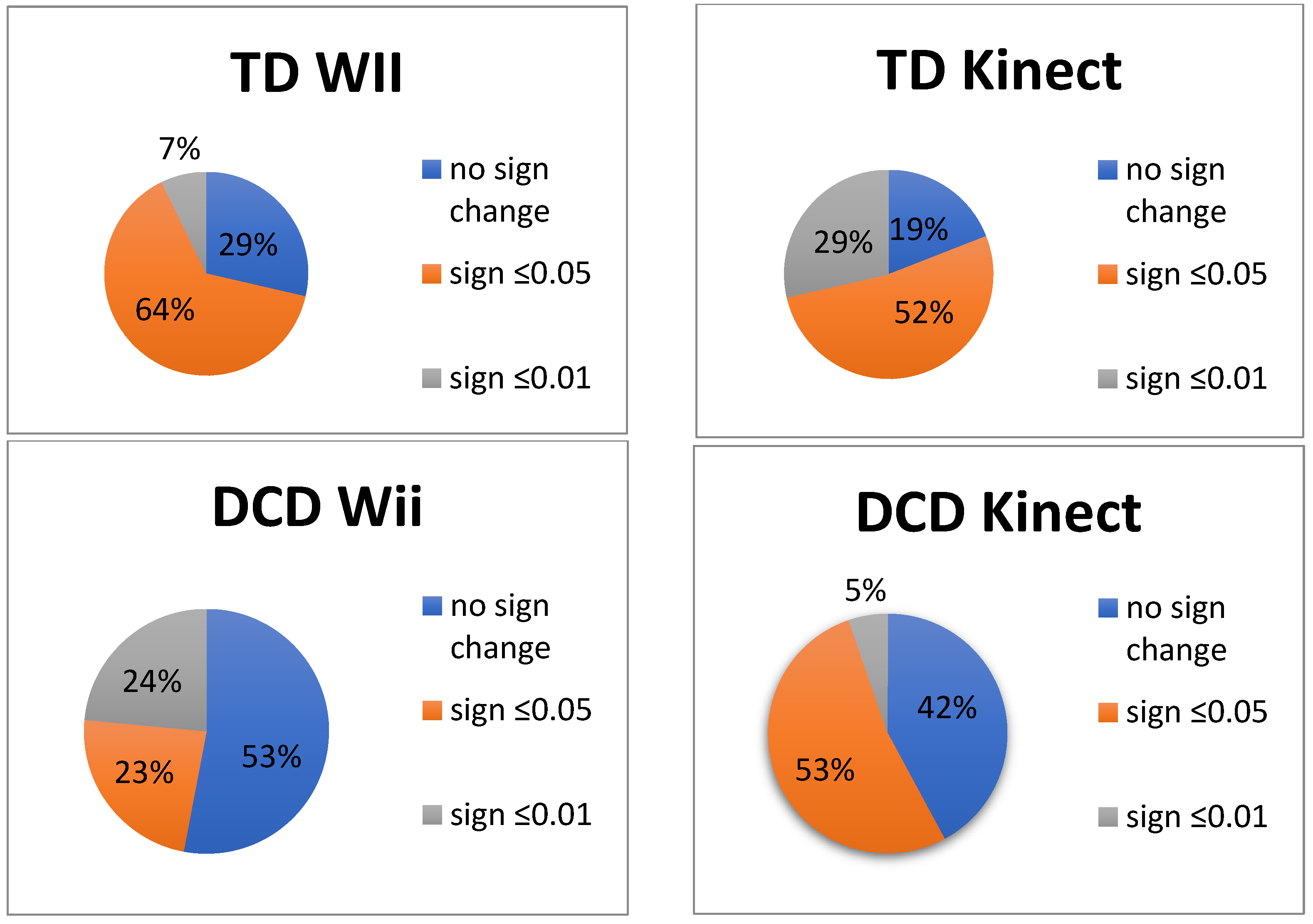
3.2. Performance in Percentage of Normalized Game Scores during the 5 Weeks of Training
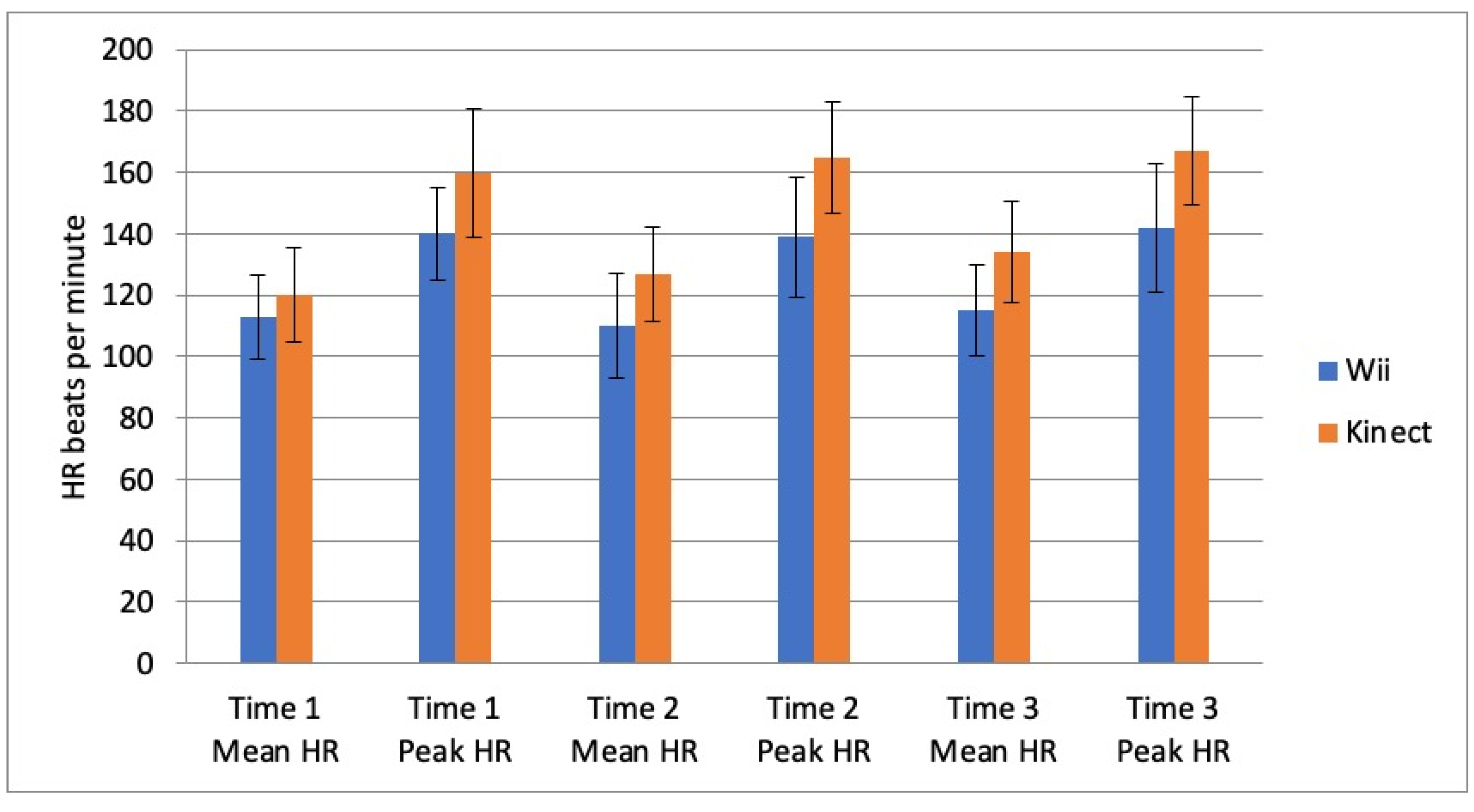
3.3. Intensity of Training
3.4. Perceived Exertion
3.5. Enjoyment
4. Discussion
Kinect and Wii
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic Stat. Man. Ment. Disord. DSM-5. 2013. Available online: Dsm.psychiatryonline.org (accessed on 5 August 2022).
- Blank, R.; Barnett, A.L.; Cairney, J.; Green, D.; Kirby, A.; Polatajko, H.; Rosenblum, S.; Smits-Engelsman, B.; Sugden, D.; Wilson, P.; et al. International Clinical Practice Recommendations on the Definition, Diagnosis, Assessment, Intervention, and Psychosocial Aspects of Developmental Coordination Disorder. Dev. Med. Child Neurol. 2019, 61, 242–285. [Google Scholar] [CrossRef] [PubMed]
- Burdea, G.C. Virtual Rehabilitation–Benefits and Challenges. Methods Inf. Med. 2003, 42, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Lin, J.H.; Pfeiffer, K.A.; Winn, B. Need Satisfaction Supportive Game Features as Motivational Determinants: An Experimental Study of a Self-Determination Theory Guided Exergame. Media Psychol. 2012, 15, 175–196. [Google Scholar] [CrossRef]
- Straker, L.M.; Fenner, A.A.; Howie, E.K.; Feltz, D.L.; Gray, C.M.; Lu, A.S.; Mueller, F.F.; Simons, M.; Barnett, L.M. Efficient and Effective Change Principles in Active Videogames. Games Health J. 2015, 1, 43–52. [Google Scholar] [CrossRef]
- Choi, E.; Shin, S.H.; Ryu, J.K.; Jung, K.I.; Kim, S.Y.; Park, M.H. Commercial Video Games and Cognitive Functions: Video Game Genres and Modulating Factors of Cognitive Enhancement. Behav. Brain Funct. 2020, 16, 2. [Google Scholar] [CrossRef] [PubMed]
- Nintendo Inc. Nintendo Wii Sports Resort. 2018. Available online: http://www.nintendo.ca/cgibin/usersite/display_info.cgi?pageNum=5&lang=en&id=5352161&from=wii (accessed on 1 March 2022).
- Chang, Y.-J.; Chen, S.-F.; Huang, J.-D. A Kinect-Based System for Physical Rehabilitation: A Pilot Study for Young Adults with Motor Disabilities. Res. Dev. Disabil. 2011, 32, 2566–2570. [Google Scholar] [CrossRef]
- Vojciechowski, A.S.; Natal, J.Z.; Gomes, A.R.S.; Rodrigues, E.V.; Villegas, I.L.P.; Korelo, R.I.G. Effects of Exergame Training on the Health Promotion of Young Adults. Fisioter. Mov. 2017, 30, 59–67. [Google Scholar] [CrossRef]
- Tatla, S.K.; Radomski, A.; Cheung, J.; Maron, M.; Jarus, T. Wii-Habilitation as Balance Therapy for Children with Acquired Brain Injury. Dev. Neurorehabil. 2012, 17, 740508. [Google Scholar] [CrossRef]
- Luna-Oliva, L.; Ortiz-Gutiérrez, R.M.; Cano-de la Cuerda, R.; Piédrola, R.M.; Alguacil-Diego, I.M.; Sánchez-Camarero, C.; Martínez Culebras, M.D.C. Kinect Xbox 360 as a Therapeutic Modality for Children with Cerebral Palsy in a School Environment: A Preliminary Study. NeuroRehabilitation 2013, 33, 513–521. [Google Scholar] [CrossRef]
- Snider, L.; Majnemer, A.; Darsaklis, V. Virtual Reality as a Therapeutic Modality for Children with Cerebral Palsy. Dev. Neurorehabil. 2010, 13, 120–128. [Google Scholar] [CrossRef]
- Sveistrup, H. Motor Rehabilitation Using Virtual Reality. J. Neuroeng. Rehabil. 2004, 1, 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Reid, D. Virtual Reality in Pediatric Neurorehabilitation: Attention Deficit Hyperactivity Disorder, Autism and Cerebral Palsy. Neuroepidemiology 2011, 36, 2–18. [Google Scholar] [CrossRef]
- Hickman, R.; Popescu, L.; Manzanares, R.; Morris, B.; Lee, S.-P.; Dufek, J.S. Use of Active Video Gaming in Children with Neuromotor Dysfunction: A Systematic Review. Dev. Med. Child Neurol. 2017, 59, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Jelsma, D.; Geuze, R.H.; Mombarg, R.; Smits-Engelsman, B.C.M. The Impact of Wii Fit Intervention on Dynamic Balance Control in Children with Probable Developmental Coordination Disorder and Balance Problems. Hum. Mov. Sci. 2014, 33, 404–418. [Google Scholar] [CrossRef]
- Cavalcante Neto, J.L.; Steenbergen, B.; Wilson, P.; Zamunér, A.R.; Tudella, E. Is Wii-Based Motor Training Better than Task-Specific Matched Training for Children with Developmental Coordination Disorder? A Randomized Controlled Trial. Disabil. Rehabil. 2019, 42, 2611–2620. [Google Scholar] [CrossRef]
- Bonney, E.; Jelsma, L.D.; Ferguson, G.D.; Smits-Engelsman, B.C.M. Learning Better by Repetition or Variation? Is Transfer at Odds with Task Specific Training? PLoS ONE 2017, 12, e0174214. [Google Scholar] [CrossRef]
- Bonney, E.; Jelsma, D.; Ferguson, G.; Smits-Engelsman, B. Variable Training Does Not Lead to Better Motor Learning Compared to Repetitive Training in Children with and without DCD When Exposed to Active Video Games. Res. Dev. Disabil. 2017, 62, 124–136. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.C.M.; Jelsma, L.D.; Ferguson, G.D.; Geuze, R.H. Motor Learning: An Analysis of 100 Trials of a Ski Slalom Game in Children with and without Developmental Coordination Disorder. PLoS ONE 2015, 10, e0140470. [Google Scholar] [CrossRef]
- Jelsma, D.; Ferguson, G.D.; Smits-Engelsman, B.C.M.; Geuze, R.H. Short-Term Motor Learning of Dynamic Balance Control in Children with Probable Developmental Coordination Disorder. Res. Dev. Disabil. 2015, 38, 213–222. [Google Scholar] [CrossRef]
- Hocking, D.R.; Farhat, H.; Gavrila, R.; Caeyenberghs, K.; Shields, N. Do Active Video Games Improve Motor Function in People with Developmental Disabilities? A Meta-Analysis of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2019, 100, 769–781. [Google Scholar] [CrossRef]
- Prado, M.; Magalhães, L.; Wilson, B. Cross-Cultural Adaptation of the Developmental Coordination Disorder Questionnaire for Brazilian Children. Brazilian J. Phys. Ther. 2009, 13, 236–243. [Google Scholar] [CrossRef]
- Bonney, E.; Ferguson, G.; Smits-Engelsman, B. The Efficacy of Two Activity-Based Interventions in Adolescents with Developmental Coordination Disorder. Res. Dev. Disabil. 2017, 71, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Venetsanou, F.; Kambas, A.; Ellinoudis, T.; Fatouros, I.; Giannakidou, D.; Kourtessis, T. Can the Movement Assessment Battery for Children-Test Be the “Gold Standard” for the Motor Assessment of Children with Developmental Coordination Disorder? Res. Dev. Disabil. 2011, 32, 1–10. [Google Scholar] [CrossRef]
- Henderson, S.E.; Sugden, D.A.; Barnett, A. Movement Assessment Battery for Children, 2nd ed.; Psychological Corporation: London, UK, 2007; Available online: https://www.pearsonclinical.com/therapy/products/100000433/movement-assessment-battery-for-children-second-edition-movement-abc-2.html (accessed on 10 September 2022).
- Jelsma, L.D.; Bergen-Verhoef, L.L.J.; Niemeijer, A.; Smits-Engelsman, B. Agreement between the Movement Assessment Battery for Children Second Edition and the Bruininks-Oseretsky Test of Motor Proficiency Second Edition for Children of 7–11 Years Old. Dutch J. Pediatr. Phys. Ther. 2010, 64, 16–17. [Google Scholar]
- Van Beek, I.; Booij, J.C.; Niemeijer, A.S.; Smits-Engelsman, B.C.M. The Movement Assessment Battery for Children Second Edition and the Körperkoordinations Test Für Kinder Compared for Children of 11–16 Years Old. Dutch J. Pediatr. Phys. Ther. 2010, 64, 18–19. [Google Scholar]
- Smits-Engelsman, B.C.M. Movement ABC-2-NL Dutch Manual, 2nd ed.; Pearson: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Robertson, R.J.; Goss, F.L.; Dubé, J.; Rutkowski, J.; Dupain, M.; Brennan, C.; Andreacci, J. Validation of the Adult OMNI Scale of Perceived Exertion for Cycle Ergometer Exercise. Med. Sci. Sports Exerc. 2004, 36, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Sanders, G.J.; Peacock, C.A.; Barkley, J.E.; Gish, B.; Brock, S.; Volpenhein, J. Heart Rate and Liking during “Kinect Boxing” Versus “Wii Boxing”: The Potential for Enjoyable Vigorous Physical Activity Videogames. Games Health J. 2015, 4, 265–270. [Google Scholar] [CrossRef]
- Scheer, K.S.; Siebrant, S.M.; Brown, G.A.; Shaw, B.S.; Shaw, I. Wii, Kinect, and Move. Heart Rate, Oxygen Consumption, Energy Expenditure, and Ventilation Due to Different Physically Active Video Game Systems in College Students. Int. J. Exerc. Sci. 2014, 7, 22–32. Available online: http://www.ncbi.nlm.nih.gov/pubmed/27182399 (accessed on 15 April 2022).
- Canabrava, K.L.R.; Faria, F.R.; Lima, J.R.P.D.; Guedes, D.P.; Amorim, P.R.S. Energy Expenditure and Intensity of Active Video Games in Children and Adolescents. Res. Q. Exerc. Sport 2018, 89, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Smallwood, S.R.; Morris, M.M.; Fallows, S.J.; Buckley, J.P. Physiologic Responses and Energy Expenditure of Kinect Active Video Game Play in Schoolchildren. Arch. Pediatr. Adolesc. Med. 2012, 166, 1005–1009. [Google Scholar] [CrossRef]
- Lisón, J.F.; Cebolla, A.; Guixeres, J.; Álvarez-Pitti, J.; Escobar, P.; Bruñó, A.; Lurbe, E.; Alcañiz, M.; Baños, R. Competitive Active Video Games: Physiological and Psychological Responses in Children and Adolescents. Paediatr. Child Health 2015, 20, 373–376. [Google Scholar] [CrossRef] [PubMed][Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Wii Group (n = 36) DCD (n = 16) TD (n = 20) | Kinect Group (n = 40) DCD (n = 19) TD (n = 21) | p Value |
|---|---|---|---|
| Age (years) | 9.8 (SD 1.3) | 9.7 (SD 1.0) | 0.726 |
| Weight (kg) | 33.12 (SD 9.04) | 35.65 (SD 12.15) | 0.953 |
| Height (cm) | 140.22 (SD 7.60) | 137.96 (SD 10.24) | 0.806 |
| BMI | 17.21 (SD 1.93) | 20.40 (SD 4.72) | 0.936 |
| MABC-2 | 7.31 (SD 2.9) | 7.43 (SD 3.1) | 0.863 |
| Gender | |||
| Boys Girls | n = 20 (55.6%) n = 16 (44.4%) | n = 22 (55.0%) n = 18 (45.0%) | 0.358 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavalcante-Neto, J.L.; Jelsma, D.; Draghi, T.T.G.; Tudella, E.; Smits-Engelsman, B. Active Video Games Performance and Heart Rate on the Wii or Kinect in Children with and without Developmental Coordination Disorder. Children 2022, 9, 1823. https://doi.org/10.3390/children9121823
Cavalcante-Neto JL, Jelsma D, Draghi TTG, Tudella E, Smits-Engelsman B. Active Video Games Performance and Heart Rate on the Wii or Kinect in Children with and without Developmental Coordination Disorder. Children. 2022; 9(12):1823. https://doi.org/10.3390/children9121823
Chicago/Turabian StyleCavalcante-Neto, Jorge Lopes, Dorothee Jelsma, Tatiane Targino Gomes Draghi, Eloisa Tudella, and Bouwien Smits-Engelsman. 2022. "Active Video Games Performance and Heart Rate on the Wii or Kinect in Children with and without Developmental Coordination Disorder" Children 9, no. 12: 1823. https://doi.org/10.3390/children9121823
APA StyleCavalcante-Neto, J. L., Jelsma, D., Draghi, T. T. G., Tudella, E., & Smits-Engelsman, B. (2022). Active Video Games Performance and Heart Rate on the Wii or Kinect in Children with and without Developmental Coordination Disorder. Children, 9(12), 1823. https://doi.org/10.3390/children9121823