
Sensory Processing Impairments in Children with Developmental Coordination Disorder





Abstract
1. Introduction
2. Materials and Methods
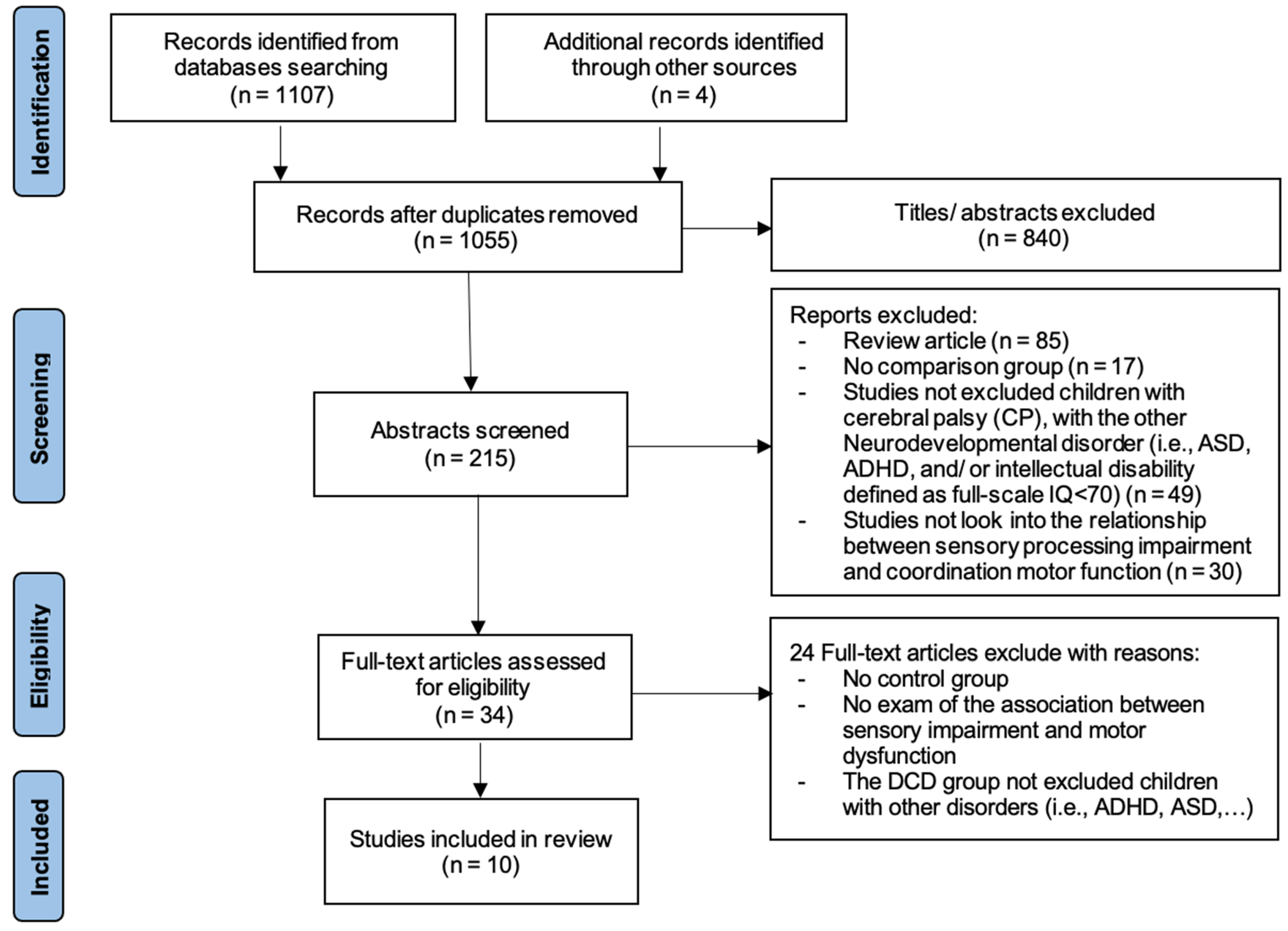
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Outcome Targets
2.5. Data Extraction and Analysis
3. Results
4. Discussion
4.1. Evidence Synthesis for Sensory Impairment in DCD Compared with Non-DCD
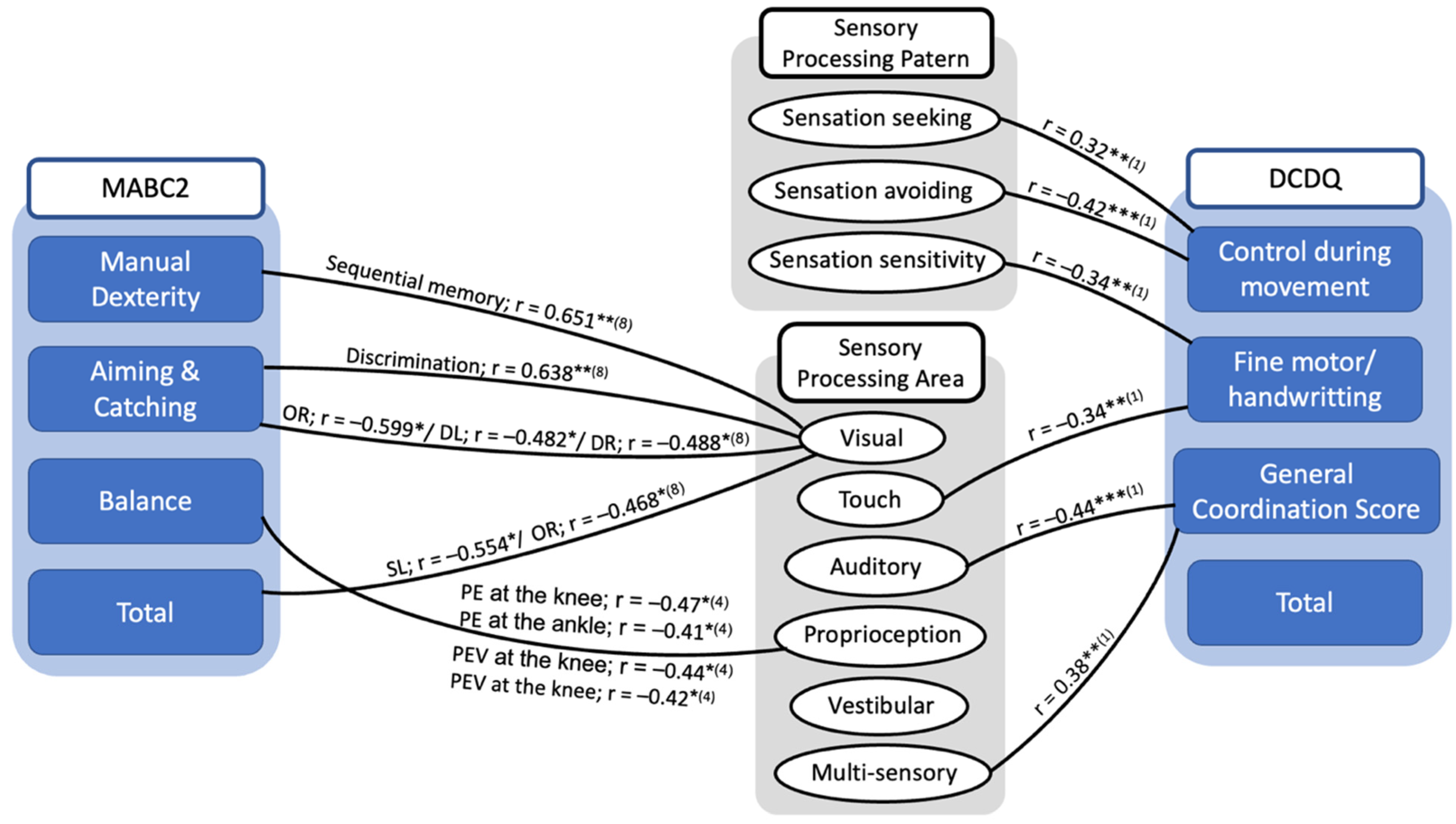
4.2. Evidence Synthesis for the Relationship between Motor Performance and Sensory Processing in DCD
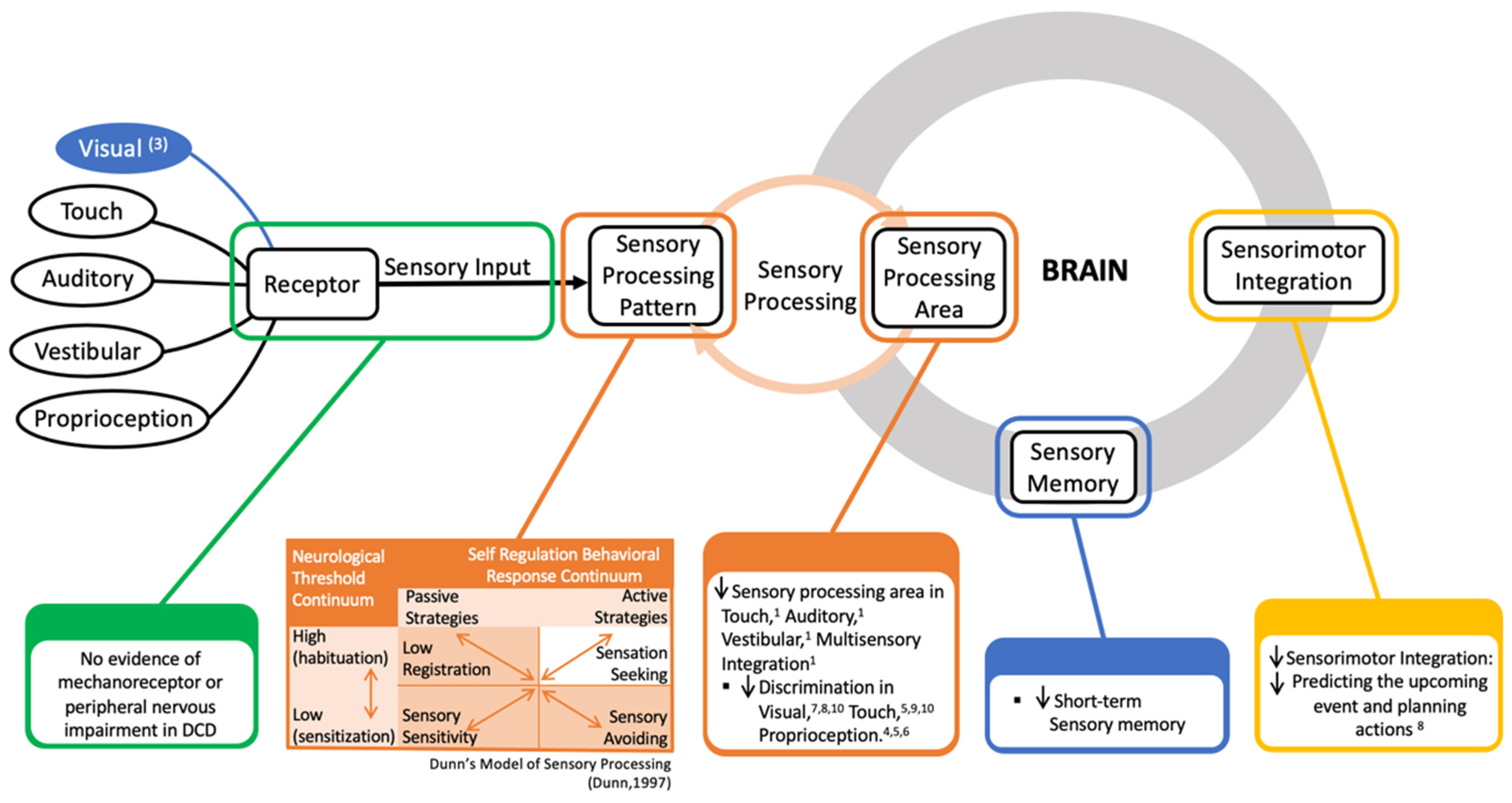
4.3. Explain the Underlying Mechanism of the Sensory Impairment
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Missiuna, C.; Gaines, R.; McLean, J.; Delaat, D.; Egan, M.; Soucie, H. Description of children identified by physicians as having developmental coordination disorder. Dev. Med. Child Neurol. 2008, 50, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Blank, R.; Barnett, A.L.; Cairney, J.; Green, D.; Kirby, A.; Polatajko, H.; Rosenblum, S.; Smits-Engelsman, B.; Sugden, D.; Wilson, P.; et al. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev. Med. Child Neurol. 2019, 61, 242–285. [Google Scholar] [CrossRef]
- Tsai, C.L.; Wilson, P.H.; Wu, S.K. Role of visual-perceptual skills (non-motor) in children with developmental coordination disorder. Hum. Mov. Sci. 2008, 27, 649–664. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.J.; Miller, L.J.; Hanft, B.E. Toward a consensus in terminology in sensory integration theory and practice: Part 2: Sensory integration patterns of function and dysfunction. Sens. Integr. Spec. Interest Sect. Q. 2000, 23, 1–3. [Google Scholar]
- Dunn, W.; Little, L.; Dean, E.; Robertson, S.; Evans, B. The State of the Science on Sensory Factors and Their Impact on Daily Life for Children: A Scoping Review. OTJR (Thorofare N. J.) 2016, 36, 3s–26s. [Google Scholar] [CrossRef] [PubMed]
- Bonifacci, P. Children with low motor ability have lowe.r visual-motor integration ability but unaffected perceptual skills. Hum. Mov. Sci. 2004, 23, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Van Waelvelde, H.; De Weerdt, W.; De Cock, P.; Smits-Engelsman, B.C. Aspects of the validity of the Movement Assessment Battery for Children. Hum. Mov. Sci. 2004, 23, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.H.; McKenzie, B.E. Information processing deficits associated with developmental coordination disorder: A meta-analysis of research findings. J. Child Psychol. Psychiatry 1998, 39, 829–840. [Google Scholar]
- Sigmundsson, H.; Hansen, P.C.; Talcott, J.B. Do ‘clumsy’ children have visual deficits. Behav. Brain Res. 2003, 139, 123–129. [Google Scholar] [CrossRef]
- Law, S.H.; Lo, S.K.; Chow, S.; Cheing, G.L. Grip force control is dependent on task constraints in children with and without developmental coordination disorder. Int. J. Rehabil. Res. 2011, 34, 93–99. [Google Scholar] [CrossRef]
- Elbasan, B.; Kayihan, H.; Duzgun, I. Sensory integration and activities of daily living in children with developmental coordination disorder. Ital. J. Pediatr. 2012, 38, 14. [Google Scholar] [CrossRef] [PubMed]
- Malloy-Miller, T.; Polatajko, H.; Anstett, B. Handwriting Error Patterns of Children with Mild Motor Difficulties. Can. J. Occup. Ther. 1995, 62, 258–267. [Google Scholar] [CrossRef]
- Carey, L.M.; Oke, L.E.; Matyas, T.A. Impaired Touch Discrimination After Stroke: A Quantiative Test. J. Neurol. Rehabil. 1997, 11, 219–232. [Google Scholar] [CrossRef]
- Xu, D.; Hong, Y.; Li, J.; Chan, K. Effect of tai chi exercise on proprioception of ankle and knee joints in old people. Br. J. Sports Med. 2004, 38, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Bairstow, P.J.; Laszlo, J.I. Kinaesthetic sensitivity to passive movements and its relationship to motor development and motor control. Dev. Med. Child Neurol. 1981, 23, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R.; Piek, J.P.; Livesey, D.J. A longitudinal study of motor ability and kinaesthetic acuity in young children at risk of developmental coordination disorder. Hum. Mov. Sci. 2001, 20, 95–110. [Google Scholar] [CrossRef]
- Li, K.Y.; Su, W.J.; Fu, H.W.; Pickett, K.A. Kinesthetic deficit in children with developmental coordination disorder. Res. Dev. Disabil. 2015, 38, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Piek, J.P.; Coleman-Carman, R. Kinaesthetic sensitivity and motor performance of children with developmental co-ordination disorder. Dev. Med. Child Neurol. 1995, 37, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Adams, I.L.; Ferguson, G.D.; Lust, J.M.; Steenbergen, B.; Smits-Engelsman, B.C. Action planning and position sense in children with Developmental Coordination Disorder. Hum. Mov. Sci. 2016, 46, 196–208. [Google Scholar] [CrossRef]
- Smyth, M.M.; Mason, U.C. Planning and execution of action in children with and without developmental coordination disorder. J. Child Psychol. Psychiatry 1997, 38, 1023–1037. [Google Scholar] [CrossRef] [PubMed]
- Hoare, D.; Larkin, D. Kinaesthetic abilities of clumsy children. Dev. Med. Child Neurol. 1991, 33, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Lord, R.; Hulme, C. Kinaesthetic sensitivity of normal and clumsy children. Dev. Med. Child Neurol. 1987, 29, 720–725. [Google Scholar] [CrossRef] [PubMed]
- Mikami, M.; Hirota, T.; Takahashi, M.; Adachi, M.; Saito, M.; Koeda, S.; Yoshida, K.; Sakamoto, Y.; Kato, S.; Nakamura, K.; et al. Atypical Sensory Processing Profiles and Their Associations With Motor Problems In Preschoolers With Developmental Coordination Disorder. Child Psychiatry Hum. Dev. 2021, 52, 311–320. [Google Scholar] [CrossRef]
- Allen, S.; Casey, J. Developmental coordination disorders and sensory processing and integration: Incidence, associations and co-morbidities. Br. J. Occup. Ther. 2017, 80, 549–557. [Google Scholar] [CrossRef]
- Wilson, P.H.; Smits-Engelsman, B.; Caeyenberghs, K.; Steenbergen, B.; Sugden, D.; Clark, J.; Mumford, N.; Blank, R. Cognitive and neuroimaging findings in developmental coordination disorder: New insights from a systematic review of recent research. Dev. Med. Child Neurol. 2017, 59, 1117–1129. [Google Scholar] [CrossRef] [PubMed]
- Zwicker, J.G.; Missiuna, C.; Harris, S.R.; Boyd, L.A. Developmental coordination disorder: A pilot diffusion tensor imaging study. Pediatr. Neurol. 2012, 46, 162–167. [Google Scholar] [CrossRef]
- Kashiwagi, M.; Iwaki, S.; Narumi, Y.; Tamai, H.; Suzuki, S. Parietal dysfunction in developmental coordination disorder: A functional MRI study. Neuroreport 2009, 20, 1319–1324. [Google Scholar] [CrossRef]
- Julian, P.T.H.; Sally, G. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK; Hoboken, NJ, USA, 2008. [Google Scholar]
- Sanderson, S.; Tatt, L.D.; Higgins, J.P.T. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef]
- Dunn, W. The impact of sensory processing abilities on the daily lives of young children and their families: A conceptual model. Infants Young Child. 1997, 9, 23–35. [Google Scholar] [CrossRef]
- Jebsen, R.H.; Taylor, N.; Trieschmann, R.B.; Trotter, M.J.; Howard, L.A. An objective and standardized test of hand function. Arch. Phys. Med. Rehabil. 1969, 50, 311–319. [Google Scholar]
- Amundson, S.J. Evaluation Tool of Children’s Handwriting: ETCH Examiner’s Manual; O.T. KIDS: Homer, AK, USA, 1995. [Google Scholar]
- Auld, M.L.; Boyd, R.N.; Moseley, G.L.; Johnston, L.M. Tactile assessment in children with cerebral palsy: A clinimetric review. Phys. Occup. Ther. Pediatr. 2011, 31, 413–439. [Google Scholar] [CrossRef] [PubMed]
- Auld, M.L.; Boyd, R.N.; Moseley, G.L.; Ware, R.S.; Johnston, L.M. Impact of tactile dysfunction on upper-limb motor performance in children with unilateral cerebral palsy. Arch. Phys. Med. Rehabil. 2012, 93, 696–702. [Google Scholar] [CrossRef]
- Auld, M.L.; Ware, R.S.; Boyd, R.N.; Moseley, G.L.; Johnston, L.M. Reproducibility of tactile assessments for children with unilateral cerebral palsy. Phys. Occup. Ther. Pediatr. 2012, 32, 151–166. [Google Scholar] [CrossRef]
- Bair, W.N.; Kiemel, T.; Jeka, J.J.; Clark, J.E. Development of multisensory reweighting for posture control in children. Exp. Brain Res. 2007, 183, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.C.; Li, L.L.; Chu, C.H.; Pan, C.Y.; Tsai, C.L. Finger soaking enhances effects of light touch on reducing body sway in children with developmental coordination disorder. J. Rehabil. Med. 2019, 51, 217–224. [Google Scholar] [CrossRef]
- Lincoln, N.B.; Jackson, J.; Adams, S.A. Reliability and Revision of the Nottingham Sensory Assessment for Stroke Patients. Physiotherapy 1998, 84, 358–365. [Google Scholar] [CrossRef]
- Stolk-Hornsveld, F.; Crow, J.L.; Hendriks, E.P.; van der Baan, R.; Harmeling-van der Wel, B.C. The Erasmus MC modifications to the (revised) Nottingham Sensory Assessment: A reliable somatosensory assessment measure for patients with intracranial disorders. Clin. Rehabil. 2006, 20, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Lobete, L.; Pértega-Díaz, S.; Santos-Del-Riego, S.; Montes-Montes, R. Sensory processing patterns in developmental coordination disorder, attention deficit hyperactivity disorder and typical development. Res. Dev. Disabil. 2020, 100, 103608. [Google Scholar] [CrossRef]
- Mon-Williams, M.A.; Mackie, R.T.; McCulloch, D.L.; Pascal, E. Visual evoked potentials in children with developmental coordination disorder. Ophthalmic Physiol. Opt. 1996, 16, 178–183. [Google Scholar] [CrossRef]
- Hill, E.L. Non-specific nature of specific language impairment: A review of the literature with regard to concomitant motor impairments. Int. J. Lang. Commun. Disord. 2001, 36, 149–171. [Google Scholar] [CrossRef]
- Gaines, R.; Missiuna, C. Early identification: Are speech/language-impaired toddlers at increased risk for Developmental Coordination Disorder? Child Care Health Dev. 2007, 33, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Summers, J.; Larkin, D.; Dewey, D. Activities of daily living in children with developmental coordination disorder: Dressing, personal hygiene, and eating skills. Hum. Mov. Sci. 2008, 27, 215–229. [Google Scholar] [CrossRef] [PubMed]
- Gomez, A.; Sirigu, A. Developmental coordination disorder: Core sensori-motor deficits, neurobiology and etiology. Neuropsychologia 2015, 79, 272–287. [Google Scholar] [CrossRef] [PubMed]
- Mimouni-Bloch, A.; Offek, H.; Rosenblum, S.; Posener, I.; Silman, Z.; Engel-Yeger, B. Association between sensory modulation and daily activity function of children with attention deficit/hyperactivity disorder and children with typical development. Res. Dev. Disabil. 2018, 83, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.E.; Harris, E.C.; Auld, M.L.; Johnston, L.M. Impact of tactile function on upper limb motor function in children with Developmental Coordination Disorder. Res. Dev. Disabil. 2015, 46, 373–383. [Google Scholar] [CrossRef]
- Chen, F.C.; Pan, C.Y.; Chu, C.H.; Tsai, C.L.; Tseng, Y.T. Joint position sense of lower extremities is impaired and correlated with balance function in children with developmental coordination disorder. J. Rehabil. Med. 2020, 52, jrm00088. [Google Scholar] [CrossRef]
- Tseng, Y.T.; Tsai, C.L.; Chen, F.C.; Konczak, J. Wrist position sense acuity and its relation to motor dysfunction in children with developmental coordination disorder. Neurosci. Lett. 2018, 674, 106–111. [Google Scholar] [CrossRef]
- Biotteau, M.; Chaix, Y.; Blais, M.; Tallet, J.; Péran, P.; Albaret, J.M. Neural Signature of DCD: A Critical Review of MRI Neuroimaging Studies. Front. Neurol. 2016, 7, 227. [Google Scholar] [CrossRef]
- Peters, L.H.; Maathuis, C.G.; Hadders-Algra, M. Neural correlates of developmental coordination disorder. Dev. Med. Child Neurol. 2013, 55 (Suppl. 4), 59–64. [Google Scholar] [CrossRef]
- Hadders-Algra, M. Developmental coordination disorder: Is clumsy motor behavior caused by a lesion of the brain at early age? Neural Plast. 2003, 10, 39–50. [Google Scholar] [CrossRef]
- Vaivre-Douret, L.; Lalanne, C.; Ingster-Moati, I.; Boddaert, N.; Cabrol, D.; Dufier, J.L.; Golse, B.; Falissard, B. Subtypes of developmental coordination disorder: Research on their nature and etiology. Dev. Neuropsychol. 2011, 36, 614–643. [Google Scholar] [CrossRef] [PubMed]
- Romeo, D.M.; Venezia, I.; De Biase, M.; Ascione, F.; Lala, M.R.; Arcangeli, V.; Mercuri, E.; Brogna, C. Developmental Coordination Disorder and Joint Hypermobility in Childhood: A Narrative Review. Children 2022, 9, 1011. [Google Scholar] [CrossRef]
- Fatoye, F.; Palmer, S.; Macmillan, F.; Rowe, P.; van der Linden, M. Proprioception and muscle torque deficits in children with hypermobility syndrome. Rheumatology 2009, 48, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Mallik, A.K.; Ferrell, W.R.; McDonald, A.G.; Sturrock, R.D. Impaired proprioceptive acuity at the proximal interphalangeal joint in patients with the hypermobility syndrome. Br. J. Rheumatol. 1994, 33, 631–637. [Google Scholar] [CrossRef]
- Konczak, J.; Corcos, D.M.; Horak, F.; Poizner, H.; Shapiro, M.; Tuite, P.; Volkmann, J.; Maschke, M. Proprioception and motor control in Parkinson’s disease. J. Mot. Behav. 2009, 41, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Chu, V.W.T. Assessing Proprioception in Children: A Review. J. Mot. Behav. 2017, 49, 458–466. [Google Scholar] [CrossRef]
- Wilson, P.H.; Maruff, P.; Butson, M.; Williams, J.; Lum, J.; Thomas, P.R. Internal representation of movement in children with developmental coordination disorder: A mental rotation task. Dev. Med. Child Neurol. 2004, 46, 754–759. [Google Scholar] [CrossRef]
- Zoia, S.; Castiello, U.; Blason, L.; Scabar, A. Reaching in children with and without developmental coordination disorder under normal and perturbed vision. Dev. Neuropsychol. 2005, 27, 257–273. [Google Scholar] [CrossRef]
- Zwicker, J.G.; Missiuna, C.; Harris, S.R.; Boyd, L.A. Brain activation of children with developmental coordination disorder is different than peers. Pediatrics 2010, 126, e678–e686. [Google Scholar] [CrossRef]
- Fuelscher, I.; Caeyenberghs, K.; Enticott, P.G.; Williams, J.; Lum, J.; Hyde, C. Differential activation of brain areas in children with developmental coordination disorder during tasks of manual dexterity: An ALE meta-analysis. Neurosci. Biobehav. Rev. 2018, 86, 77–84. [Google Scholar] [CrossRef]
- Gentile, G.; Petkova, V.I.; Ehrsson, H.H. Integration of visual and tactile signals from the hand in the human brain: An FMRI study. J. Neurophysiol. 2011, 105, 910–922. [Google Scholar] [CrossRef] [PubMed]
- Zwicker, J.G.; Missiuna, C.; Harris, S.R.; Boyd, L.A. Brain activation associated with motor skill practice in children with developmental coordination disorder: An fMRI study. Int. J. Dev. Neurosci. 2011, 29, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Baumann, O.; Borra, R.J.; Bower, J.M.; Cullen, K.E.; Habas, C.; Ivry, R.B.; Leggio, M.; Mattingley, J.B.; Molinari, M.; Moulton, E.A.; et al. Consensus paper: The role of the cerebellum in perceptual processes. Cerebellum 2015, 14, 197–220. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| STUDY | Selection | Comparability | Exposure | Score/Stars | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1a | 1b | 1 | 2 | 3 | ||
| 1. Mikami et al., 2021 [23] |  | | - | | | - | | | - | 6/9 |
| 2. Delgado-Lobete et al., 2020 [30] | | | | | | - | | | - | 7/9 |
| 3. Nobusako et al., 2021 [31] | | | | | | - | | | - | 7/9 |
| 4. Chen et al., 2020 [32] | | | | | | - | | | - | 7/9 |
| 5. Tseng et al., 2019 [33] | | | | | | - | | | - | 7/9 |
| 6. Tseng et al., 2018 [34] | | | | | | - | | | - | 7/9 |
| 7. Prunty et al., 2016 [35] | | | | | | - | | | - | 7/9 |
| 8. Cheng et al., 2014 [36] | | | | | | - | | | - | 7/9 |
| 9. Cox et al., 2015 [37] | | | - | | | - | | | - | 6/9 |
| 10. Elbasan et al., 2012 [11] | | | - | | | - | | | - | 6/9 |
| Study Design (Author, year) Population (Age: M ± SD) | Measures | Sensory Processing Impairment: DCD Group vs. TD or Other Disability Group | |||||
|---|---|---|---|---|---|---|---|
| Touch | Proprioceptive | Visual | Auditory | Vestibular | Appendixes | ||
| 1. CS (Mikami et al., 2021) [23] 63 DCD (64 ± 2 months) 106 TD (64 ± 2 months) |
| ↓—DCD is poorer | - | - | ↓—DCD is poorer | ↓—DCD is poorer | ↓—DCD is poorer - oral sensory (↑ DCD significant higher in the score of ** oral sensory) ↑ DCD significant higher in the score of ** low registration, ** sensory sensitivity, ** sensation avoiding |
| 2. CS (Delgado-Lobete et al., 2020) [30] 46 DCD (10 ± 2 years) 369 TD (9 ± 2 years) |
| - | - | - | - | - | ↑ DCD significant higher in the score of * low registration, * sensory sensitivity, * sensation avoiding, * seeking |
| 3. CS (Nobusako et al., 2021) [31] 19 DCD (9.3 ± 1.4 years) 19 TD (9.3 ± 1.4 years) |
| ↓—DCD is poorer (↑* DCD significant higher in the score of PSE) | - | - | - | - | - |
| 4. CS (Chen et al., 2020) [32] 28 DCD (10.86 ± 1.07 years) 28 TD (10.96 ± 1.18 years) |
| - | ↓—DCD is poorer (↑* DCD significant higher in the score of PE at knee; ↑** DCD significant higher in the score of PE at ankle; ↑** DCD significant higher in the score of PEV at ankle) | - | - | - | - |
| 5. CS (Tseng et al., 2019) [33] 20 DCD (10.55 ± 0.72 years) 20 TD (10.65 ± 0.45 years) |
| ↓—DCD is poorer (↑*** DCD significant higher in the score of DT) | ↓—DCD is poorer (↑*** DCD significant higher in the score of DT) | - | - | - | - |
| 6. CS (Tseng et al., 2018) [34] 20 DCD (10 years 4 months ± 3 months) 30 TD (10 years 5 months ± 3 months) |
| - | ↓—DCD is poorer (↑* DCD significant higher in the score of SDPE at the wrist; ↑*** DCD significant higher in the score of JND at the wrist) | - | - | - | - |
| 7. CS (Prunty et al., 2016) [35] 28 DCD (10.61 ± 2.23 years) 28 TD (10.95 ± 2.12 years) |
| - | - | ↓—DCD is poorer (↓DCD significant lower in the score of *** TVPS; *** VD; * VM; * SR; ** SM; *** VF; ** VC) | - | - | - |
| 8. CS (Cheng et al., 2014) [36] 17 DCD (7.25 ± 0.28 years) 17 TD (7.09 ± 0.34 years) |
| - | - | ↓—DCD is poorer (↓ DCD significant lower in the score of * VD; * FC; *** TVPS; * SM; ** VF) | - | - | - |
| 9. CS (Cox et al., 2015) [37] 20 DCD (8.35 ± 1.63 years) 16 TD (8.69 ± 2.24 years) |
| ↓—DCD is poorer (↓ DCD significant lower in the score of * SPL—nondominant) | - | - | - | - | - |
| 10. CS (Elbasan et al., 2012) [11] 37 DCD (boys: 10 ± 1.5 years; girls: 10 ± 2 years) 35 TD (boys: 10 ± 0.8 years; girls: 9 ± 1 years) |
| ↓—DCD is poorer (↓ DCD significant lower in the score of * MFP; * FI; * Graphesthesia; * LTS; * DTSP; * Kinesthesia) | - | ↓—DCD is poorer (↓ DCD significant lower in the score of * SV; *** Position in space; ** Design copying) | - | - | - |
| Scheme. | Sensory Process | Developmental Coordination Disorder Questionnaire (DCDQ) | Movement Assessment Battery for Children-2nd Edition (M-ABC2) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CDM | FM&M | GC | Total Score | MD | A&C | Bal | Total Score | |||
| 1. Mikami et al., 2021 [23] | Auditory | DCD | - | - | −0.44 *** | - | ||||
| TD | - | - | - | - | ||||||
| Touch | DCD | - | −0.34 ** | - | - | |||||
| TD | - | - | - | - | ||||||
| Multi-sensory | DCD | - | - | 0.38 ** | - | |||||
| TD | - | - | −0.19 * | |||||||
| Sensation avoiding score | DCD | −0.42 *** | - | - | - | |||||
| TD | - | - | - | - | ||||||
| Sensory sensitivity score | DCD | - | −0.34 ** | - | - | |||||
| TD | - | - | - | - | ||||||
| Sensation seeking score | DCD | 0.32 ** | - | - | - | |||||
| TD | - | - | - | - | ||||||
| Low registration score | DCD | - | - | - | - | |||||
| TD | - | - | −0.23 * | - | ||||||
| 2. Delgado-Lobete et al., 2020 [30] | Low registration score | DCD | - | - | - | - | ||||
| TD | - | - | - | - | ||||||
| Both | −0.28 *** | - | −0.17 *** | −0.47 *** | ||||||
| Sensory sensitivity score | DCD | - | - | - | - | |||||
| TD | - | - | - | - | ||||||
| Both | - | −0.14 *** | −0.16 *** | −0.29 ** | ||||||
| 3. Nobusako et al., 2021 [31] | Visual (PSE) | DCD | NS | NS | NS | NS | NS | NS | NS | NS |
| TD | - | - | - | - | - | - | - | - | ||
| Both | - | - | - | - | 0.43 ** | - | - | - | ||
| 4. Chen et al., 2020 [32] | Proprioceptive (PE) at the knee | DCD | NS | NS | –0.47 * | - | ||||
| TD | NS | NS | NS | - | ||||||
| Proprioceptive (PE) at the ankle | DCD | NS | NS | –0.41 * | - | |||||
| TD | NS | NS | NS | - | ||||||
| Proprioceptive (PEV) at the knee | DCD | NS | NS | –0.44 * | - | |||||
| TD | NS | NS | NS | - | ||||||
| Proprioceptive (PEV) at the ankle | DCD | NS | NS | –0.42 * | - | |||||
| TD | NS | NS | NS | - | ||||||
| 5. Tseng et al., 2019 [33] | Touch (discrimination thresholds) | DCD | - | - | - | - | ||||
| TD | - | - | - | - | ||||||
| Both | −0.43 ** | −0.40 ** | −0.49 ** | - | ||||||
| 6. Tseng et al., 2018 [34] | Proprioceptive (SDPE) | DCD | - | - | - | - | ||||
| TD | - | - | - | - | ||||||
| Both | NS | −0.29 * | −0.30 * | - | ||||||
| Proprioceptive (JND thresholds) | DCD | - | - | - | - | |||||
| TD | - | - | –0.40 * | - | ||||||
| Both | −0.40 ** | NS | −0.50 *** | - | ||||||
| Proprioceptive (PE) | DCD | - | - | - | - | |||||
| TD | - | - | - | - | ||||||
| Both | NS | −0.08 | NS | - | ||||||
| 7. Prunty et al., 2016 [35] | Found no association between sensory and motor | |||||||||
| 8. Cheng et al., 2014 [36] | Visual (discrimination) | DCD | NS | 0.64 ** | NS | NS | ||||
| TD | NS | NS | NS | NS | ||||||
| Visual (Form constancy) | DCD | NS | NS | NS | NS | |||||
| TD | NS | NS | NS | NS | ||||||
| Visual (Sequential memory) | DCD | 0.65 ** | NS | NS | NS | |||||
| TD | NS | NS | NS | NS | ||||||
| Visual (Figure ground) | DCD | NS | NS | NS | NS | |||||
| TD | NS | NS | NS | NS | ||||||
| Visual (Single in left—SL) | DCD | NS | NS | NS | –0.55 * | |||||
| TD | NS | NS | NS | NS | ||||||
| Visual (Single in right—SR) | DCD | NS | NS | NS | NS | |||||
| TD | NS | NS | NS | NS | ||||||
| Visual (double off in the left—OL) | DCD | NS | NS | NS | NS | |||||
| TD | NS | NS | NS | NS | ||||||
| Visual (double off in the right—OR) | DCD | NS | −0.60 * | NS | –0.47 * | |||||
| TD | NS | NS | NS | NS | ||||||
| Visual (double left—DL) | DCD | NS | −0.48 * | NS | NS | |||||
| TD | NS | NS | NS | NS | ||||||
| Visual (double right—DR) | DCD | NS | –0.49 * | NS | NS | |||||
| TD | NS | NS | NS | NS | ||||||
| 9. Cox et al., 2015 [37] | Touch (spatial tactile perception—SPL) in both hands | DCD | - | - | - | - | ||||
| TD | - | - | - | - | ||||||
| Both | −0.04 ** | 1.44 ** | 1.39 ** | |||||||
| 10. Elbasan et al., 2012 [11] | Found no association between sensory and motor | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, H.-T.; Li, Y.-C.; Lin, H.-Y.; Lee, S.-D.; Wang, P.-J. Sensory Processing Impairments in Children with Developmental Coordination Disorder. Children 2022, 9, 1443. https://doi.org/10.3390/children9101443
Tran H-T, Li Y-C, Lin H-Y, Lee S-D, Wang P-J. Sensory Processing Impairments in Children with Developmental Coordination Disorder. Children. 2022; 9(10):1443. https://doi.org/10.3390/children9101443
Chicago/Turabian StyleTran, Huynh-Truc, Yao-Chuen Li, Hung-Yu Lin, Shin-Da Lee, and Pei-Jung Wang. 2022. "Sensory Processing Impairments in Children with Developmental Coordination Disorder" Children 9, no. 10: 1443. https://doi.org/10.3390/children9101443
APA StyleTran, H.-T., Li, Y.-C., Lin, H.-Y., Lee, S.-D., & Wang, P.-J. (2022). Sensory Processing Impairments in Children with Developmental Coordination Disorder. Children, 9(10), 1443. https://doi.org/10.3390/children9101443