




Quality of Ventilations during Infant Resuscitation: A Simulation Study Comparing Endotracheal Tube with Face Mask
 , , ,
, , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
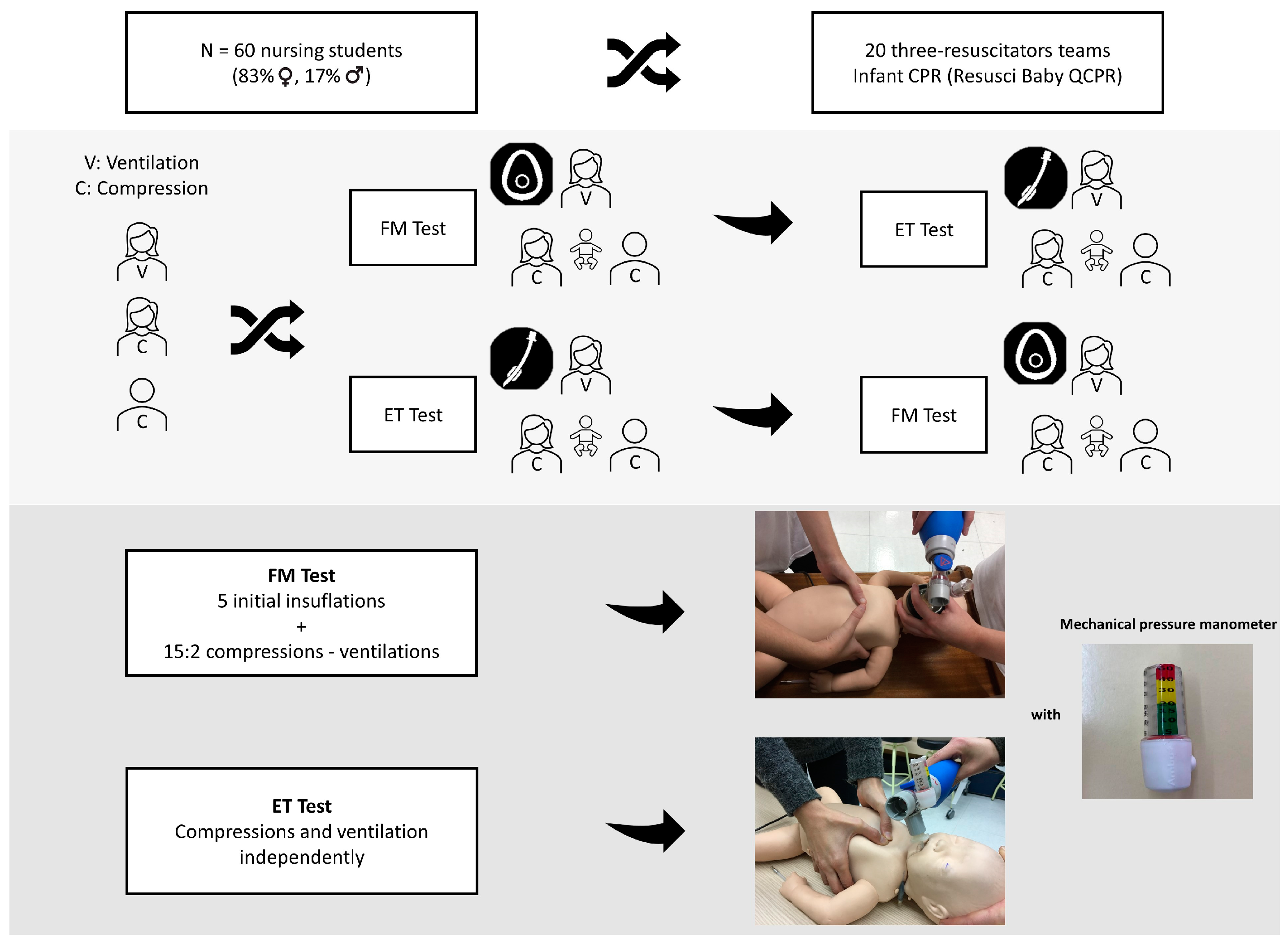
2.1. Study Design
2.2. Sample
2.3. Ethics
2.4. Development of the Test and Data Collection
- (a)
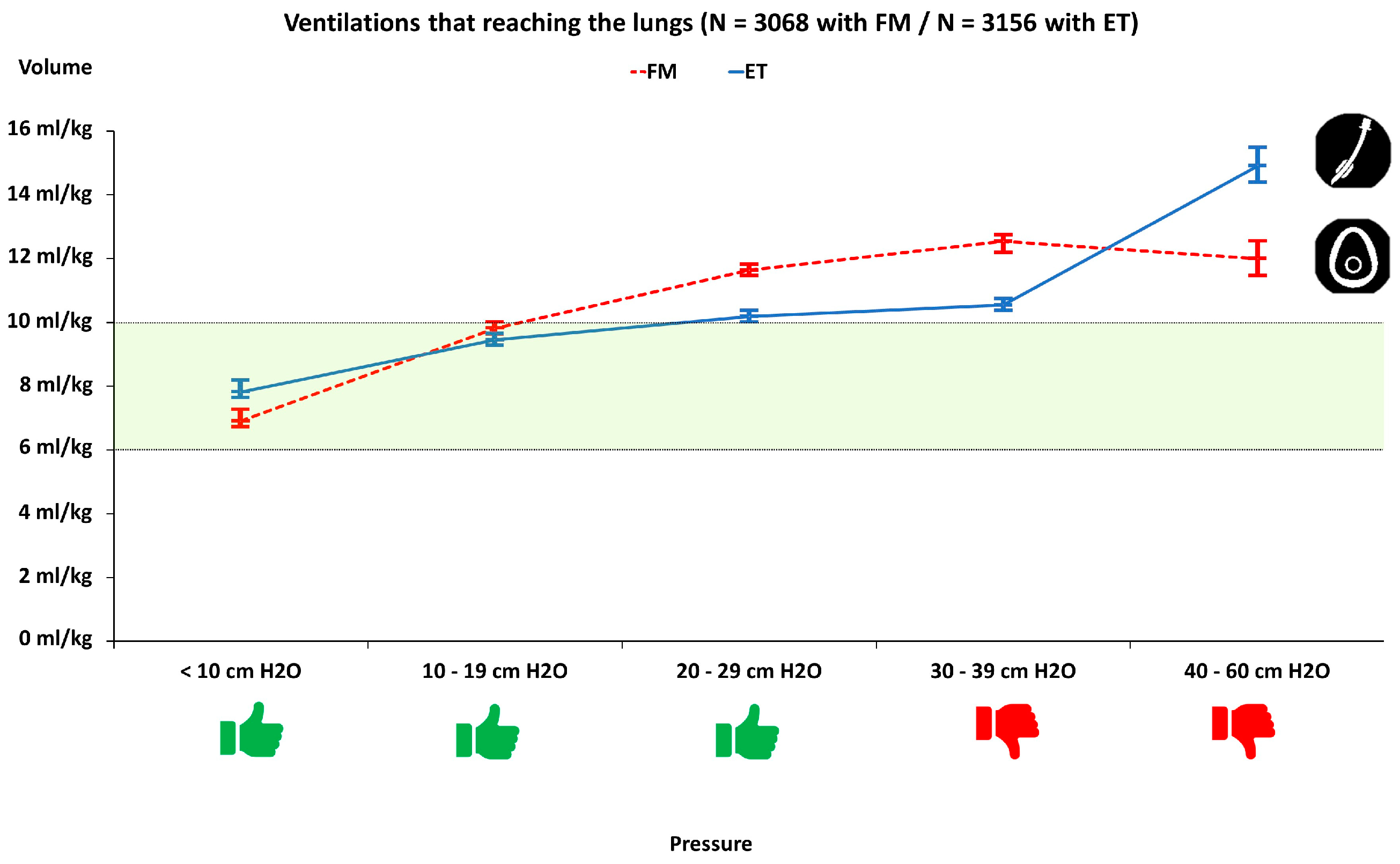
- Ventilation: Frequency (breaths per minute), mean ventilation volume (in mL and mL/kg), percentage of ventilations that reached the lungs, the percentage of ventilations with achieved volume labelled as insufficient (less than 35 mL or 6 mL/kg), optimal and excessive (greater than 55 mL or 10 mL/kg) and the percentage of ventilations in which peak pressure generated was greater than 30 cm H2O. The volume of each ventilation was recorded continuously, while the pressure was grouped into five ranges: <10 cm H2O, (10–19) cm H2O, (20–29) cm H2O, (30–39) cm H2O and (40–60) cm H2O.
- (b)
- Chest compressions: Mean compression rate (compressions per minute), mean compression depth (mm), percentage of CC with correct hand position and percentage of CC with adequate release.
2.5. Simulation Material and Measuring Instruments
2.6. Statistical Analysis
3. Results
3.1. Pre-Test Ventilation Pressure-Volume
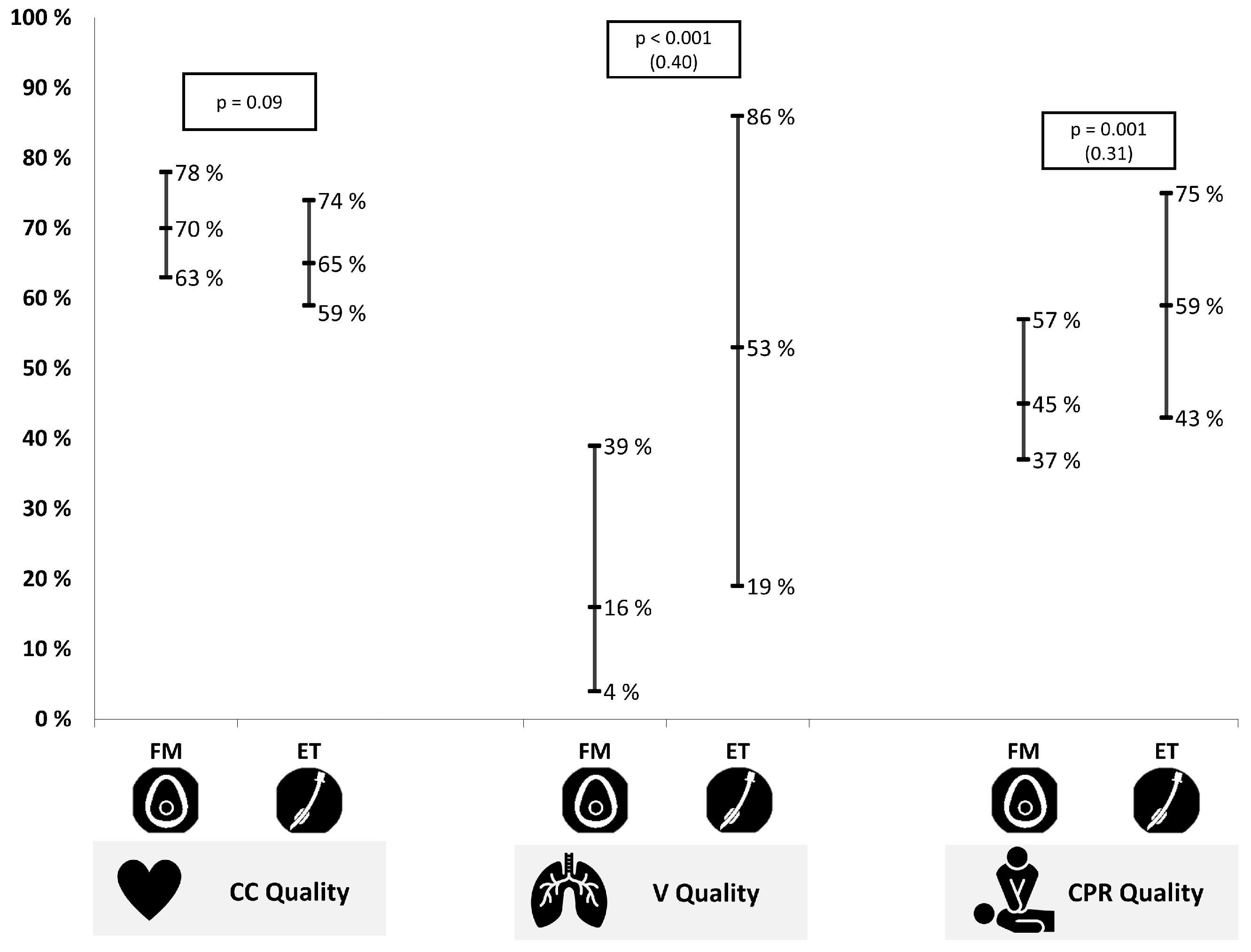
3.2. CPR Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van de Voorde, P.; Turner, N.M.; Djakow, J.; de Lucas, N.; Martinez-Mejias, A.; Biarent, D.; Bingham, R.; Brissaud, O.; Hoffmann, F.; Johannesdottir, G.B.; et al. European resuscitation council guidelines 2021: Paediatric life support. Resuscitation 2021, 161, 327–387. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo, J.; López-Herce, J.; Matamoros, M.; Cañadas, S.; Rodriguez-Calvo, A.; Cechetti, C.; Rodriguez-Núñez, A.; Álvarez, A.C.; The Iberoamerican Pediatric Cardiac Arrest Study Network RIBEPCI. Hyperoxia, hypocapnia and hypercapnia as outcome factors after cardiac arrest in children. Resuscitation 2012, 83, 1456–1461. [Google Scholar] [CrossRef] [PubMed]
- Guerra-Wallace, M.M.; Casey III, F.L.; Bell, M.J.; Fink, E.L.; Hickey, R.W. Hyperoxia and hypoxia in children resuscitated from cardiac arrest. Pediatr. Crit. Care Med. 2013, 14, e143–e148. [Google Scholar] [CrossRef] [PubMed]
- Kilgannon, J.H.; Jones, A.E.; Shapiro, N.I.; Angelos, M.G.; Milcarek, B.; Hunter, K.; Parrillo, J.E.; Trzeciak, S.; the Emergency Medicine Shock Research Network (EMShockNet) Investigators. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA 2010, 303, 2165–2171. [Google Scholar] [CrossRef]
- López-Herce, J.; Del Castillo, J.; Matamoros, M.; Canadas, S.; Rodriguez-Calvo, A.; Cecchetti, C.; Rodríguez-Núnez, A.; Carrillo, Á. Post return of spontaneous circulation factors associated with mortality in pediatric in-hospital cardiac arrest: A prospective multicenter multinational observational study. Crit. Care 2014, 18, 607. [Google Scholar] [CrossRef]
- González, R.; Pascual, L.; Sava, A.; Tolón, S.; Urbano, J.; López-Herce, J. Ventilation during cardiopulmonary resuscitation in children: A survey on clinical practice. World J. Pediatr. 2017, 13, 544–550. [Google Scholar] [CrossRef]
- Santos-Folgar, M.; Otero-Agra, M.; Fernández-Méndez, F.; Hermo-Gonzalo, M.T.; Barcala-Furelos, R.; Rodríguez-Núñez, A. Ventilation during cardiopulmonary resuscitation in the infant. Mouth to mouth and nose, or bag-valve-mask? A quasi-experimental study. Anoles Pediatr. 2018, 89, 272–278. [Google Scholar] [CrossRef]
- Otero-Agra, M.; Hermo-Gonzalo, M.T.; Santos-Folgar, M.; Fernández-Méndez, F.; Barcala-Furelos, R. Assessing Ventilation Skills by Nursing Students in Paediatric and Adult Basic Life Support: A Crossover Randomized Simulation Study Using Bag-Valve-Mask (BMV) vs Mouth-to-Mouth Ventilation (MMV). Signa Vitae 2020, 16, 44–51. [Google Scholar]
- Gonzalez-Salvado, V.; Fernández-Méndez, F.; Barcala-Furelos, R.; Pena-Gil, C.; González-Juanatey, J.R.; Rodriguez-Nunez, A. Very brief training for laypeople in hands-only cardiopulmonary resuscitation. Effect of real-time feedback. Am. J. Emerg. Med. 2016, 34, 993–998. [Google Scholar] [CrossRef]
- Méndez, F.F.; Barcala-Furelos, R.; Fungueiriño-Suárez, R.; Mecías-Calvo, M.; Abelairas-Gómez, C.; Rodríguez-Núñez, A. Cardiopulmonary resuscitation quality during navigation in inshore fishing boats: A pilot study with fishermen. Am. J. Emerg. Med. 2015, 33, 1705–1707. [Google Scholar] [CrossRef]
- Barcala-Furelos, R.; Abelairas-Gomez, C.; Palacios-Aguilar, J.; Rey, E.; Costas-Veiga, J.; Lopez-Garcia, S.; Rodriguez-Nunez, A. Can surf-lifeguards perform a quality cardiopulmonary resuscitation sailing on a lifeboat? A quasi-experimental study. Emerg. Med. J. 2017, 34, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Sutton, R.M.; Niles, D.; French, B.; Maltese, M.R.; Leffelman, J.; EilevstjØnn, J.; Wolfe, H.; Nishisaki, A.; Meaney, P.A.; Berg, R.A. First quantitative analysis of cardiopulmonary resuscitation quality during in-hospital cardiac arrests of young children. Resuscitation 2014, 85, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Augré, C.; Rogers, H.; Allan, M.; Thickett, D.R. CPREzy: An evaluation during simulated cardiac arrest on a hospital bed. Resuscitation 2005, 64, 103–108. [Google Scholar] [CrossRef]
- Cortegiani, A.; Russotto, V.; Montalto, F.; Iozzo, P.; Meschis, R.; Pugliesi, M.; Mariano, D.; Benenati, V.; Raineri, S.M.; Gregoretti, C.; et al. Use of a real-Time training software (Laerdal QCPR®) compared to instructor-based feedback for high-quality chest compressions acquisition in secondary school students: A randomized trial. PLoS ONE 2017, 12, e0169591. [Google Scholar] [CrossRef]
- Wagner, M.; Bibl, K.; Hrdliczka, E.; Steinbauer, P.; Stiller, M.; Gröpel, P.; Goeral, K.; Salzer-Muhar, U.; Berger, A.; Schmölzer, G.M.; et al. Effects of Feedback on Chest Compression Quality: A Randomized Simulation Study. Pediatrics 2019, 143, e20182441. [Google Scholar] [CrossRef]
- Lin, Y.; Cheng, A.; Grant, V.J.; Currie, G.R.; Hecker, K.G. Improving CPR quality with distributed practice and real-time feedback in pediatric healthcare providers—A randomized controlled trial. Resuscitation 2018, 130, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Huang, Z.; Li, H.; Zheng, G.; Ling, Q.; Tang, W.; Yang, Z. CPR feedback/prompt device improves the quality of hands-only CPR performed in manikin by laypersons following the 2015 AHA guidelines. Am. J. Emerg. Med. 2018, 36, 1980–1985. [Google Scholar] [CrossRef]
- Resusci Baby QCPR [Internet]. Laerdal Medical. Available online: https://laerdal.com/es/products/simulation-training/resuscitation-training/resusci-baby-qcpr/ (accessed on 25 October 2022).
- World Health Organization. WHO Child Growth Standards: Length/Heightfor-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Núñez, A.R. Ventilation During Pediatric CPR. Curr. Pediatr. Rev. 2013, 9, 109–114. [Google Scholar] [CrossRef]
- Wilkins, L.W. Part 7.1: Adjuncts for Airway Control and Ventilation. Circulation 2005, 112 (Suppl. 24), IV-51–IV-57. [Google Scholar]
- Ambu® Mark IV Adulto y Baby Resucitador Reutilizable [Internet]. Available online: https://www.ambu.es/emergencias/resucitadores/producto/ambu-mark-iv (accessed on 25 October 2022).
- Daigle, C.H.; Fiadjoe, J.E.; Laverriere, E.K.; Bruins, B.B.; Lockman, J.L.; Shults, J.; Krawiec, C.; Harwayne-Gidansky, I.; Page-Goertz, C.; Furlong-Dillard, J.; et al. Difficult Bag-Mask Ventilation in Critically Ill Children Is Independently Associated with Adverse Events. Crit. Care Med. 2020, 48, e744–e752. [Google Scholar] [CrossRef]
- Bassani, M.A.; Mezzacappa Filho, F.; de Carvalho Coppo, M.R.; Marba, S.T.M. An evaluation of peak inspiratory pressure, tidal volume, and ventilatory frequency during ventilation with a neonatal self-inflating bag resuscitator. Respir. Care 2012, 57, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Lacerda, R.S.; de Lima, F.C.A.; Bastos, L.P.; Vinco, A.F.; Schneider, F.B.A.; Coelho, Y.L.; Fernandes, H.G.C.; Bacalhau, J.M.R.; Bermudes, I.M.S.; da Silva, C.F.; et al. Benefits of Manometer in Non-Invasive Ventilatory Support. Prehosp. Disaster Med. 2017, 32, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, B.; Catlin, E.; Vetere, J.; Arguin, L. The role of in-line manometers in minimizing peak and mean airway pressure during the hand-regulated ventilation of newborn infants. Respir. Care 1989, 34, 23–27. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | Endotracheal Tube (ET) | Face Mask (FM) | p-Value | ||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | ||
| Ventilations (V) | |||||
| Frequency (breaths/min) | 10 | (9–13) | 10 | (10–11) | NS |
| Mean tidal volume (mL) | 50 | (46–56) | 57 | (51–69) | p = 0.02 |
| Mean tidal volume (mL/kg) | 9 | (8–10) | 10 | (9–12) | p = 0.02 |
| V that reached the lungs (%) | 100 | (100–100) | 98 | (81–100) | p < 0.001 |
| V with insufficient volume (%) | 0 | (0–1) | 5 | (2–10) | p < 0.001 |
| V with adequate volume (%) | 68 | (35–88) | 22 | (8–41) | p < 0.001 |
| V with excessive volume (%) | 29 | (11–62) | 53 | (29–73) | p = 0.04 |
| V with peak pressure > 30 cm H2O (%) | 0 | (0–41) | 18 | (0–56) | p = 0.03 |
| Chest compressions (CC) | |||||
| Mean depth (mm) | 40 | (38–41) | 41 | (39–42) | NS |
| Mean rate (CC/min) | 111 | (103–119) | 115 | (108–119) | NS |
| CC with correct hand position (%) | 100 | (95–100) | 100 | (99–100) | NS |
| CC with adequate release (%) | 81 | (57–96) | 93 | (74–99) | p = 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos-Folgar, M.; Lafuente-Filgueira, P.; Otero-Agra, M.; Fernández-Méndez, F.; Barcala-Furelos, R.; Trastoy-Quintela, J.; Aranda-García, S.; Fernández-Méndez, M.; Rodríguez-Núñez, A. Quality of Ventilations during Infant Resuscitation: A Simulation Study Comparing Endotracheal Tube with Face Mask. Children 2022, 9, 1757. https://doi.org/10.3390/children9111757
Santos-Folgar M, Lafuente-Filgueira P, Otero-Agra M, Fernández-Méndez F, Barcala-Furelos R, Trastoy-Quintela J, Aranda-García S, Fernández-Méndez M, Rodríguez-Núñez A. Quality of Ventilations during Infant Resuscitation: A Simulation Study Comparing Endotracheal Tube with Face Mask. Children. 2022; 9(11):1757. https://doi.org/10.3390/children9111757
Chicago/Turabian StyleSantos-Folgar, Myriam, Paula Lafuente-Filgueira, Martín Otero-Agra, Felipe Fernández-Méndez, Roberto Barcala-Furelos, Javier Trastoy-Quintela, Silvia Aranda-García, María Fernández-Méndez, and Antonio Rodríguez-Núñez. 2022. "Quality of Ventilations during Infant Resuscitation: A Simulation Study Comparing Endotracheal Tube with Face Mask" Children 9, no. 11: 1757. https://doi.org/10.3390/children9111757
APA StyleSantos-Folgar, M., Lafuente-Filgueira, P., Otero-Agra, M., Fernández-Méndez, F., Barcala-Furelos, R., Trastoy-Quintela, J., Aranda-García, S., Fernández-Méndez, M., & Rodríguez-Núñez, A. (2022). Quality of Ventilations during Infant Resuscitation: A Simulation Study Comparing Endotracheal Tube with Face Mask. Children, 9(11), 1757. https://doi.org/10.3390/children9111757