
Screening Questionnaire for Vitamin D Insufficiency in Children with Obesity

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.2.1. Auxological Evaluation
2.2.2. VitD Level Assessment
2.3. Questionnaire Design and Scoring
2.4. Statistical Analysis
3. Results
3.1. Demographic and Auxological Parameters and VitD
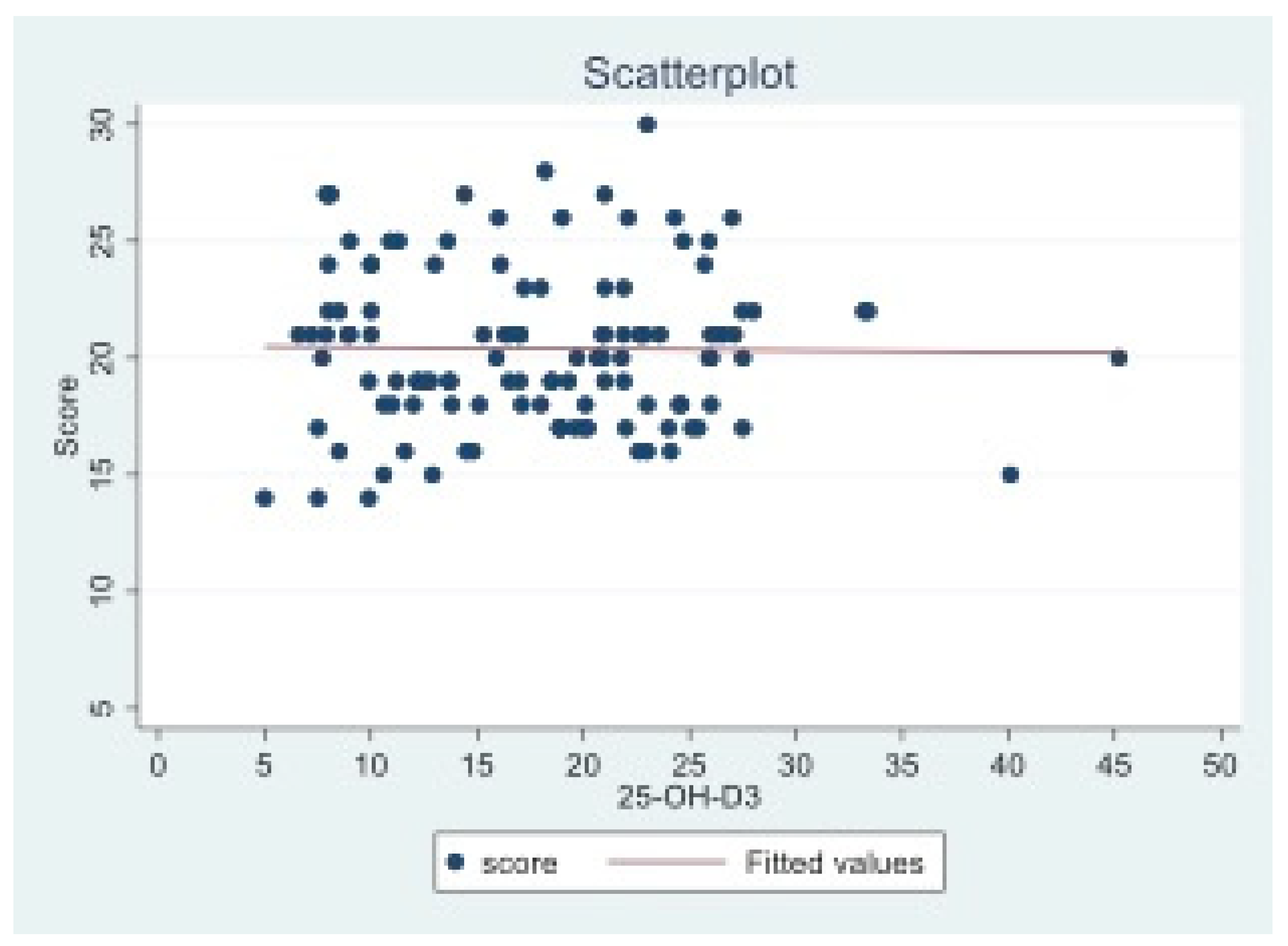
3.2. Questionnaire Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tagliaferri, S.; Porri, D.; De Giuseppe, R.; Manuelli, M.; Alessio, F.; Cena, H. The controversial role of vitamin D as an antioxidant: Results from randomised controlled trials. Nutr. Res. Rev. 2019, 32, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.P.; Alagiakrishnan, K.; Sadowski, C. The cure of ageing: Vitamin D—magic or myth? Postgrad. Med. J. 2010, 861020, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross, A.C.; Taylor, C.L.; Yaktine, A.L.; Valle, H.B.D. Overview of VitD. In Dietary Reference Intakes for Calcium and VitD; National Academies Press: Washington, DC, USA, 2011. Available online: https://www.ncbi.nlm.nih.gov/books/NBK56061/ (accessed on 1 September 2022).
- Davis, C.D.; Hartmuller, V.; Freedman, D.M.; Hartge, P.; Picciano, M.F.; Swanson, C.A.; Milner, J.A. Vitamin D and cancer: Current dilemmas and future needs. Nutr. Rev. 2007, 65, S71–S74. [Google Scholar] [CrossRef] [PubMed]
- VitD and Health in the 21st Century: An Update. Proceedings of a conference held September 2007 in Bethesda, Maryland, USA. Am. J. Clin. Nutr. 2008, 88, 483S–592S.
- Davis, C.D. Vitamin D and cancer: Current dilemmas and future research needs. Am. J. Clin. Nutr. 2008, 88, 565S–569S. [Google Scholar] [CrossRef]
- Chung, M.; Balk, E.M.; Brendel, M.; Ip, S.; Lau, J.; Lee, J.; Lichtenstein, A.; Patel, K.; Raman, G.; Tatsioni, A.; et al. Vitamin D and calcium: A systematic review of health outcomes. Evid. Rep./Technol. Assess. 2009, 183, 1–420. [Google Scholar]
- Saggese, G.; Vierucci, F.; Prodam, F.; Cardinale, F.; Cetin, I.; Chiappini, E.; De’Angelis, G.L.; Massari, M.; Miraglia Del Giudice, E.; Miraglia Del Giudice, M.; et al. Vitamin D in pediatric age: Consensus of the Italian Pediatric Society and the Italian Society of Preventive and Social Pediatrics, jointly with the Italian Federation of Pediatricians. Ital. J. Pediatr. 2018, 44, 51. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- National Diet and Nutrition Survey Results from Years 5 and 6 (combined) of the Rolling Programme (2012/2013–2013/2014). Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/551352/NDNS_Y5_6_UK_Main_Text.pdf (accessed on 1 September 2022).
- Aguiar, M.; Andronis, L.; Pallan, M.; Högler, W.; Frew, E. Micronutrient deficiencies and health-related quality of life: The case of children with vitamin D deficiency. Public Health Nutr. 2020, 23, 1165–1172. [Google Scholar] [CrossRef]
- Vierucci, F.; Del Pistoia, M.; Fanos, M.; Gori, M.; Carlone, G.; Erba, P.; Massimetti, G.; Federico, G.; Saggese, G. Vitamin D status and predictors of hypovitaminosis D in Italian children and adolescents: A cross-sectional study. Eur. J. Pediatr. 2013, 172, 1607–1617. [Google Scholar] [CrossRef]
- Blumberg, J.B.; Cena, H.; Barr, S.I.; Biesalski, H.K.; Dagach, R.U.; Delaney, B.; Frei, B.; Moreno González, M.I.; Hwalla, N.; Lategan-Potgieter, R.; et al. The Use of Multivitamin/Multimineral Supplements: A Modified Delphi Consensus Panel Report. Clin. Ther. 2018, 40, 640–657. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Zhu, L.; He, L.; Duan, Y.; Liang, W.; Nie, Z.; Jin, Y.; Wu, X.; Fang, Y. A meta-analysis of the relationship between vitamin D deficiency and obesity. Int. J. Clin. Exp. Med. 2015, 8, 14977–14984. [Google Scholar] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Golden, N.H.; Abrams, S.A.; Committee on Nutrition. Optimizing bone health in children and adolescents. Pediatrics 2014, 134, e1229–e1243. [Google Scholar] [CrossRef] [PubMed]
- Zakharova, I.; Klimov, L.; Kuryaninova, V.; Nikitina, I.; Malyavskaya, S.; Dolbnya, S.; Kasyanova, A.; Atanesyan, R.; Stoyan, M.; Todieva, A.; et al. Vitamin D Insufficiency in Overweight and Obese Children and Adolescents. Front. Endocrinol. 2019, 10, 103. [Google Scholar] [CrossRef] [PubMed]
- De Giuseppe, R.; Tomasinelli, C.E.; Cena, H.; Braschi, V.; Giampieri, F.; Preatoni, G.; Centofanti, D.; Princis, M.P.; Bartoletti, E.; Biino, G. Development of a Short Questionnaire for the Screening for Vitamin D Deficiency in Italian Adults: The Evidence-Q Project. Nutrients 2022, 14, 1772. [Google Scholar] [CrossRef]
- Nuti, R.; Brandi, M.L.; Checchia, G.; Di Munno, O.; Dominguez, L.; Falaschi, P.; Fiore, C.E.; Iolascon, G.; Maggi, S.; Michieli, R.; et al. Guidelines for the management of osteoporosis and fragility fractures. Intern. Emerg. Med. 2019, 14, 85–102. [Google Scholar] [CrossRef]
- Calcaterra, V.; Cena, H.; de Silvestri, A.; Albertini, R.; De Amici, M.; Valenza, M.; Pelizzo, G. Stress Measured by Allostatic Load in Neurologically Impaired Children: The Importance of Nutritional Status. Horm. Res. Paediatr. 2017, 88, 224–230. [Google Scholar] [CrossRef]
- Calcaterra, V.; Cena, H.; De Silvestri, A.; Girgenti, V.; Bommarito, D.; Pelizzo, G. Diabetes Type 2 in Neurologically Impaired Children and Adolescents Without Obesity: A New Emerging Entity? Front. Neurol. 2019, 10, 947. [Google Scholar] [CrossRef]
- Marshall, W.A.; Tanner, J.M. Variations in pattern of pubertal changes in girls. Arch. Dis. Child. 1969, 44, 291–303. [Google Scholar] [CrossRef]
- Marshall, W.A.; Tanner, J.M. Variations in the pattern of pubertal changes in boys. Arch. Dis. Child. 1970, 45, 13–23. [Google Scholar] [CrossRef] [PubMed]
- WHO. Child Growth Standards. World Health Organization. Available online: https://www.who.int/tools/child-growth-standards (accessed on 1 September 2022).
- Antonucci, R.; Locci, C.; Clemente, M.G.; Chicconi, E.; Antonucci, L. Vitamin D deficiency in childhood: Old lessons and current challenges. J. Pediatr. Endocrinol. Metab. 2018, 31, 247–260. [Google Scholar] [CrossRef] [PubMed]
- Saneifard, H.; Shakiba, M.; Sheikhy, A.; Baniadam, L.; Abdollah Gorji, F.; Fallahzadeh, A. Vitamin D Deficiency in Children and Adolescents: Role of Puberty and Obesity on Vitamin D Status. Nutr. Metab. Insights 2021, 14, 11786388211018726. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.; De Sanctis, V.; Elalaily, R.; Bedair, S. Advances in pubertal growth and factors influencing it: Can we increase pubertal growth? Indian J. Endocrinol. Metab. 2014, 18 (Suppl. 1), S53–S62. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferri, S.; De Giuseppe, R.; Cena, H. Comments about the Potential Relationship between VitD Status and Obesity or Body Fatness. In Responses by the Scientific Advisory Committee on Nutrition (SACN) to Comments Received during Public Consultation (22 July–23 September 2015) on the Draft VitD and Health Report. Available online: https://www.gov.uk/government/consultations/consultation-on-draft-sacn-vitamin-d-and-health-report (accessed on 21 July 2016).
- Drincic, A.T.; Armas, L.A.; Van Diest, E.E.; Heaney, R.P. Volumetric dilution, rather than sequestration best explains the low vitamin D status of obesity. Obesity 2012, 20, 1444–1448. [Google Scholar] [CrossRef]
- Wolden-Kirk, H.; Overbergh, L.; Gysemans, C.; Brusgaard, K.; Naamane, N.; Van Lommel, L.; Schuit, F.; Eizirik, D.L.; Christesen, H.; Mathieu, C. Unraveling the effects of 1,25OH2D3 on global gene expression in pancreatic islets. J. Steroid Biochem. Mol. Biol. 2013, 136, 68–79. [Google Scholar] [CrossRef]
- Obesity Impacts ncds and Communicable Disease too: Ace2 Receptor in Human Adipose Tissue. Available online: https://easo.org/obesity-impacts-ncds-and-communicable-disease-too-ace2-receptor-in-human-adipose-tissue/ (accessed on 1 September 2022).
- Calcaterra, V.; Regalbuto, C.; Porri, D.; Pelizzo, G.; Mazzon, E.; Vinci, F.; Zuccotti, G.; Fabiano, V.; Cena, H. Inflammation in Obesity-Related Complications in Children: The Protective Effect of Diet and Its Potential Role as a Therapeutic Agent. Biomolecules 2020, 10, 1324. [Google Scholar] [CrossRef]
- Hossein-nezhad, A.; Holick, M.F. Vitamin D for health: A global perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef]
- Cena, H.; Fiechtner, L.; Vincenti, A.; Magenes, V.C.; De Giuseppe, R.; Manuelli, M.; Zuccotti, G.V.; Calcaterra, V. COVID-19 Pandemic as Risk Factors for Excessive Weight Gain in Pediatrics: The Role of Changes in Nutrition Behavior. A Narrative Review. Nutrients 2021, 13, 4255. [Google Scholar] [CrossRef]
- Contreras-Bolívar, V.; García-Fontana, B.; García-Fontana, C.; Muñoz-Torres, M. Mechanisms Involved in the Relationship between Vitamin D and Insulin Resistance: Impact on Clinical Practice. Nutrients 2021, 13, 3491. [Google Scholar] [CrossRef]
- Cesareo, R.; Attanasio, R.; Caputo, M.; Castello, R.; Chiodini, I.; Falchetti, A.; Guglielmi, R.; Papini, E.; Santonati, A.; Scillitani, A.; et al. Italian Association of Clinical Endocrinologists (AME) and Italian Chapter of the American Association of Clinical Endocrinologists (AACE) Position Statement: Clinical Management of Vitamin D Deficiency in Adults. Nutrients 2018, 10, 546. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Gender | ||
|---|---|---|
| Males | Females | |
| Age, y | 10.2 (2.69) | 10.2 (3.35) |
| Weight, kg | 62.2 (16.2) | 53.7 (18.81) |
| Weight z-score | 10.2 (2.69) | 10.2 (3.35) |
| Height, m | 1.5 (0.14) | 1.4 (0.19) |
| Height z-score | 2.7 (1.09) | 2.6 (1.11) |
| BMI kg/m2 | 27.2 (3.18) | 26.9 (4.22) |
| BMI z-score | 2.75 (0.7) | 2.73 (0.6) |
| Waist, cm | 90.4 (10.67) | 85.6 (10.92) |
| Waist/Height | 3.1 (0.92) | 3 (1.08) |
| VitD | BMI | Waist | W/H | Weight | |
|---|---|---|---|---|---|
| VitD | 1 | ||||
| BMI | −0.2430 ** | 1 | |||
| Waist | −0.2390 * | 0.6889 ** | 1 | ||
| W/H | −0.0413 | 0.2962 ** | 0.3415 ** | 1 | |
| Weight | −0.3058 ** | 0.7987 ** | 0.8310 ** | −0.02 | 1 |
| VitD Cut-Off 30 ng/mL | Number of Patients | Questionnaire Score | ||
| Mean (SD) | Median | Min–Max | ||
| Severe deficiency (<10) | 19 | 20.7 (4.26) | 19.3 | 14–27 |
| Insufficiency (10–30) | 97 | 20.4 (3.24) | 17 | 15–30 |
| Sufficiency (>30) | 4 | 19.8 (3.3) | 0 | 15–22 |
| VitD Cut-Off 20 ng/mL | Number of Patients | Questionnaire Score | ||
| Mean (SD) | Median | Min–Max | ||
| Severe deficiency (<10) | 19 | 20.7 (4.26) | 21 | 14–27 |
| Insufficiency (10–20) | 50 | 20.2 (3.27) | 19 | 15–28 |
| Sufficiency (>20) | 51 | 20.5 (3.21) | 20 | 15–30 |
| Score Cut-Off | Sensitivity | 95% CI | Specificity | 95% CI | #Pos | #Neg |
|---|---|---|---|---|---|---|
| Severe Deficiency 25(OH)D < 10 mg/dL | ||||||
| 30 | 0.00% | (0–0.209) | 99.01% | (0.938–0.999) | 0 | 1 |
| 27 | 15.79% | (0.042–0.405) | 96.04% | (0.896–0.987) | 3 | 3 |
| 21 a | 63.16% | (0.386–0.828) | 55.45% | (0.452–0.652) | 9 | 41 |
| 14 | 100.00% | (0.791–1) | 0.00% | (0–0.046) | 7 | 56 |
| Severe deficiency prevalence (score ≥ 21) = 47.5%; ROC curve AUC = 0.615; SE = 0.082 | ||||||
| Deficiency 25(OH)D < 20 mg/dL | ||||||
| 14 | 4.35% | (0.011–0.13) | 100.00% | (0.913–1) | ||
| 15 | 7.25% | (0.027–0.168) | 98.04% | (0.882–0.999) | 5 | 1 |
| 19 a | 49.28% | (0.371–0.615) | 64.71% | (0.5–0.772) | 29 | 17 |
| 28 | 100.00% | (0.934–1) | 1.96% | (0.001–0.118) | 18 | 19 |
| 30 | 100.00% | (0.934–1) | 0.00% | (0–0.087) | 35 | 33 |
| Deficiency prevalence (score ≥ 19) = 69.2%; ROC curve AUC = 0.583; SE = 0.053 | ||||||
| Insufficiency 25(OH)D < 30 mg/dL | ||||||
| 23 a | 24.14% | (0.169–0.331) | 100.00% | (0.396–1) | 111 | 3 |
| 16 | 95.69% | (0.897–0.984) | 25.00% | (0.013–0.781) | 5 | 1 |
| 14 | 100.00% | (0.96–1) | 0.00% | (0–0.604) | 111 | 3 |
| Insufficiency prevalence (score ≥ 23) = 23.3%; ROC curve AUC = 0.694; SE = 0.147 | ||||||
| Sufficiency 25(OH)D ≥ 30 mg/dL | ||||||
| 14 | 0.00% | (0–0.604) | 97.41% | (0.921–0.993) | 0 | 3 |
| 15 | 25.00% | (0.013–0.781) | 95.69% | (0.897–0.984) | 1 | 2 |
| 22 a | 100.00% | (0.396–1) | 24.14% | (0.169–0.331) | 0 | 0 |
| 30 | 100.00% | (0.396–1) | 0.00% | (0–0.04) | 3 | 111 |
| Sufficiency prevalence (score ≥ 22) = 29.2%; ROC curve AUC = 0.691; SE = 0.147 | ||||||
| 25(OH)D < 10 mg/dL | 25(OH)D < 20 mg/dL | 25(OH)D < 30 mg/dL | 25(OH)D ≥ 30 mg/dL | |
|---|---|---|---|---|
| Optimal operating slope | 1 | 1 | 1 | 1 |
| Optimal cut-off | 21 | 19 | 23 | 22 |
| Optimal sensitivity | 0.632 | 0.493 | 0.241 | 1 |
| Optimal specificity | 0.554 | 0.647 | 1 | 0.241 |
| Clinical information statistic | 0.186 | 0.139 | 0.241 | 0.241 |
| Area under the ROC Curve | 0.615 | 0.583 | 0.694 | 0.691 |
| SE of Area (Hanley) | 0.082 | 0.053 | 0.147 | 0.147 |
| Sample size | 120 | 120 | 120 | 120 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calcaterra, V.; Cena, H.; Biino, G.; Grazi, R.; Bortoni, G.; Braschi, V.; Tomasinelli, C.E.; Schneider, L.; Zuccotti, G. Screening Questionnaire for Vitamin D Insufficiency in Children with Obesity. Children 2022, 9, 1685. https://doi.org/10.3390/children9111685
Calcaterra V, Cena H, Biino G, Grazi R, Bortoni G, Braschi V, Tomasinelli CE, Schneider L, Zuccotti G. Screening Questionnaire for Vitamin D Insufficiency in Children with Obesity. Children. 2022; 9(11):1685. https://doi.org/10.3390/children9111685
Chicago/Turabian StyleCalcaterra, Valeria, Hellas Cena, Ginevra Biino, Roberta Grazi, Giulio Bortoni, Valentina Braschi, Chiara Elena Tomasinelli, Laura Schneider, and Gianvincenzo Zuccotti. 2022. "Screening Questionnaire for Vitamin D Insufficiency in Children with Obesity" Children 9, no. 11: 1685. https://doi.org/10.3390/children9111685
APA StyleCalcaterra, V., Cena, H., Biino, G., Grazi, R., Bortoni, G., Braschi, V., Tomasinelli, C. E., Schneider, L., & Zuccotti, G. (2022). Screening Questionnaire for Vitamin D Insufficiency in Children with Obesity. Children, 9(11), 1685. https://doi.org/10.3390/children9111685