

Central Venous Catheter Cannulation in Pediatric Anesthesia and Intensive Care: A Prospective Observational Trial

 , ,
, ,
Abstract
:1. Introduction
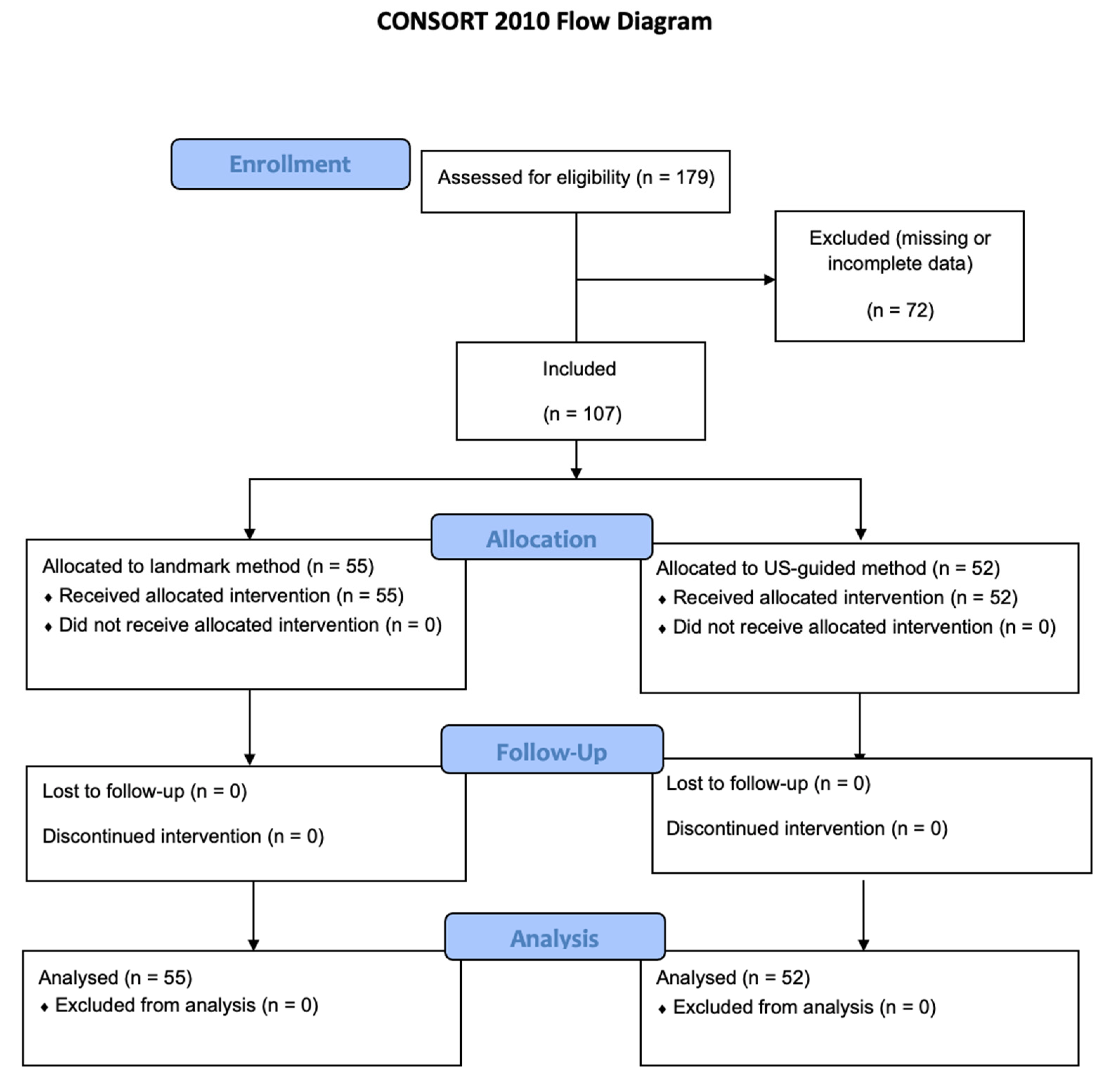
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Souza, T.H.; Brandão, M.B.; Nadal, J.; Nogueira, R. Ultrasound Guidance for Pediatric Central Venous Catheterization: A Meta-analysis. Pediatrics 2018, 142, e20181719. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.Y.; Ling, Q.; Cao, L.H.; Wang, J.; Xu, M.X.; Zeng, W.A. Real-time Two-dimensional Ultrasound Guidance for Central Venous Cannulation: A Meta-analysis. Anesthesiology 2013, 118, 361–375. [Google Scholar] [CrossRef]
- Lamperti, M.; Biasucci, D.G.; Disma, N.; Pittiruti, M.; Breschan, C.; Vailati, D.; Subert, M.; Traškaitė, V.; Macas, A.; Estebe, J.P.; et al. European Society of Anaesthesiology guidelines on peri-operative use of ultrasound-guided for vascular access (PERSEUS vascular access). Eur. J. Anaesthesiol. 2020, 37, 344–376. [Google Scholar] [CrossRef]
- Dassinger, M.S.; Renaud, E.J.; Goldin, A.; Huang, E.Y.; Russell, R.T.; Streck, C.J.; Tang, X.; Blakely, M.L. Use of real-time ultrasound during central venous catheter placement: Results of an APSA survey. J. Pediatr. Surg. 2015, 50, 1162–1167. [Google Scholar] [CrossRef]
- Lau, C.S.; Chamberlain, R.S. Ultrasound-guided central venous catheter placement increases success rates in pediatric patients: A meta-analysis. Pediatr. Res. 2016, 80, 178–184. [Google Scholar] [CrossRef]
- Shime, N.; Hosokawa, K.; MacLaren, G. Ultrasound Imaging Reduces Failure Rates of Percutaneous Central Venous Catheterization in Children. Pediatr. Crit. Care Med. 2015, 16, 718–725. [Google Scholar] [CrossRef]
- Froehlich, C.D.; Rigby, M.R.; Rosenberg, E.S.; Li, R.; Roerig, P.L.; Easley, K.A.; Stockwell, J.A. Ultrasound-guided central venous catheter placement decreases complications and decreases placement attempts compared with the landmark technique in patients in a pediatric intensive care unit. Crit. Care Med. 2009, 37, 1090–1096. [Google Scholar] [CrossRef]
- Guilbert, A.S.; Xavier, L.; Ammouche, C.; Desprez, P.; Astruc, D.; Diemunsch, P.; Bientz, J. Supraclavicular ultrasound-guided catheterization of the subclavian vein in pediatric and neonatal ICUs: A feasibility study. Pediatr. Crit. Care Med. 2013, 14, 351–355. [Google Scholar] [CrossRef]
- Oulego-Erroz, I.; González-Cortes, R.; García-Soler, P.; Balaguer-Gargallo, M.; Frías-Pérez, M.; Mayordomo-Colunga, J.; Llorente-de-la-Fuente, A.; Santos-Herraiz, P.; Menéndez-Suso, J.J.; Sánchez-Porras, M.; et al. Ultrasound-guided or landmark techniques for central venous catheter placement in critically ill children. Intensive Care Med. 2018, 44, 61–72. [Google Scholar] [CrossRef]
- Safety Committee of Japanese Society of Anesthesiologists. Practical guide for safe central venous catheterization and management 2017. J. Anesth. 2020, 34, 167–186. [Google Scholar] [CrossRef]
- Eisen, L.A.; Narasimhan, M.; Berger, J.S.; Mayo, P.H.; Rosen, M.J.; Schneider, R.F. Mechanical complications of central venous catheters. J. Intensive Care Med. 2006, 21, 40–46. [Google Scholar] [CrossRef]
- Rhondali, O.; Attof, R.; Combet, S.; Chassard, D.; de Queiroz Siqueira, M. Ultrasound-guided subclavian vein cannulation in infants: Supraclavicular approach. Pediatr. Anaesth. 2011, 21, 1136–1141. [Google Scholar] [CrossRef]
- Byon, H.J.; Lee, G.W.; Lee, J.H.; Park, Y.H.; Kim, H.S.; Kim, C.S.; Kim, J.T. Comparison between ultrasound-guided supraclavicular and infraclavicular approaches for subclavian venous catheterization in children—A randomized trial. Br. J. Anaesth. 2013, 111, 788–792. [Google Scholar] [CrossRef] [Green Version]
- Merchaoui, Z.; Lausten-Thomsen, U.; Pierre, F.; Ben Laiba, M.; Le Saché, N.; Tissieres, P. Supraclavicular Approach to Ultrasound-Guided Brachiocephalic Vein Cannulation in Children and Neonates. Front. Pediatr. 2017, 5, 211. [Google Scholar] [CrossRef] [Green Version]
- McGee, D.C.; Gould, M.K. Preventing complications of central venous catheterization. N. Engl. J. Med. 2003, 348, 1123–1133. [Google Scholar] [CrossRef]
- Calvache, J.-A.; Rodríguez, M.-V.; Trochez, A.; Klimek, M.; Stolker, R.-J.; Lesaffre, E. Incidence of Mechanical Complications of Central Venous Catheterization Using Landmark Technique: Do Not Try More Than 3 Times. J. Intensive Care Med. 2016, 31, 397–402. [Google Scholar] [CrossRef]
- Lausten-Thomsen, U.; Merchaoui, Z.; Dubois, C.; Eleni Dit Trolli, S.; Le Saché, N.; Mokhtari, M.; Tissières, P. Ultrasound-guided subclavian vein cannulation in low birth weight neonates. Pediatr. Crit. Care Med. 2017, 18, 172–175. [Google Scholar] [CrossRef]
- Oulego-Erroz, I.; Alonso-Quintela, P.; Terroba-Seara, S.; Jiménez-González, A.; Rodríguez-Blanco, S.; Vázquez-Martínez, J.L. Ultrasound-guided cannulation of the brachiocephalic vein in neonates and preterm infants: A prospective observational study. Am. J. Perinatol. 2018, 35, 503–508. [Google Scholar]
- Nardi, N.; Wodey, E.; Laviolle, B.; De La Brière, F.; Delahaye, S.; Engrand, C.; Gauvrit, C.; Dessard, S.; Defontaine, A.; Ecoffey, C. Effectiveness and complications of ultrasound-guided subclavian vein cannulation in children and neonates. Anaesth. Crit. Care Pain Med. 2016, 35, 209–213. [Google Scholar] [CrossRef]
- Di Nardo, M.; Tomasello, C.; Pittiruti, M.; Perrotta, D.; Marano, M.; Cecchetti, C.; Pasotti, E.; Pirozzi, N.; Stoppa, F. Ultrasound-guided central venous cannulation in infants weighing less than 5 kilograms. J. Vasc. Access 2011, 12, 321–324. [Google Scholar] [CrossRef]
- Tsuboi, N.; Abe, M.; Matsumoto, S.; Nishimura, N.; Nakagawa, S. The effect of clinical experience on the learning curve of pediatric intensive care unit residents for the central venous catheter placement procedure. J. Pediatr. Intensive Care 2018, 7, 39–42. [Google Scholar]
- Altun, D.; Nuraç, S.H.; Toprak, V.; Eti, E.Z. The success rate and safety of internal jugular vein catheterization under ultrasound guidance in infants undergoing congenital heart surgery. Turk. J. Thorac. Cardiovasc. Surg. 2019, 27, 23–28. [Google Scholar] [CrossRef]


{kind=link}
| US-Guided (n = 52) | Landmark (n = 55) | |||
|---|---|---|---|---|
| Mean (SD) | Median (Min–Max) | Mean (SD) | Median (Min–Max) | |
| Age (years) | 6.6 | 7.1 | 4.1 | 0.3 |
| (5.9) | (0.0–17.7) | (5.9) | (0.0–17.5) | |
| Height (cm) | 108 | 121 | 86 | 60 |
| (48) | (34–186) | (48) | (33–180) | |
| Weight (kg) | 26 | 22 | 18 | 5 |
| (22) | (1–82) | (22) | (1–71) | |
| Category | US-Guided (n = 52) | Landmark (n = 55) | p-Value | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Indication | Long-term I.V. access Parenteral nutrition Catecholamine’s Infusion therapy Antibiotics | 28 (53.8%) 20 (38.5%) 2 (3.8%) 2 (3.8%) 0 (0.0%) | 27 (49.1%) 24 (43.6%) 2 (3.6%) 1 (1.8%) 1 (1.8%) | 0.909 |
| Planned insertion site | Vena subclavia l. sin. Vena subclavia l. dx. Vena brachiocephalica l. sin. Vena brachiocephalica l. dx. Vena jugularis interna l. sin. Vena jugularis interna l. dx. Vena femoralis l. sin. Vena femoralis l. dx. | 2 (3.8%) 0 (0.0%) 29 (55.8%) 7 (13.5%) 2 (3.8%) 10 (19.2%) 1 (1.9%) 1 (1.9%) | 50 (90.9%) 5 (9.1%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) | <0.001 |
| Type of anesthesia | General anesthesia | 51 (98.1%) | 53 (96.4%) | 1.000 |
| Sedation | 1 (1.9%) | 2 (3.6%) |
| Category | US-Guided (n = 52) | Landmark (n = 55) | p-Value | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Success cannulation | Yes No | 52 (100%) 0 (0.00%) | 53 (96.4%) 2 (3.6%) | 0.496 |
| Number of necessary attempts (necessary skin puncture) | 1 2 3 4 More than 5 | 30 (57.7%) 11 (21.2%) 4 (7.7%) 2 (3.8%) 0 (0.0%) | 25 (45.5%) 12 (21.8%) 3 (5.5%) 6 (10.9%) 9 (16.4%) | 0.460 |
| Final insertion site | Vena subclavia l. sin. Vena subclavia l. dx. Vena brachiocephalica l. sin. Vena brachiocephalica l. dx. Vena jugularis interna l. sin. Vena jugularis interna l. dx. Vena femoralis l. sin. Vena femoralis l. dx. | 9 (17.3%) 2 (3.8%) 26 (50.0%) 3 (5.8%) 1 (1.9%) 8 (15.4%) 1 (1.9%) 1 (1.9%) | 49 (89.1%) 5 (9.1%) 1 (1.8%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) | <0.001 |
| Catheter size (Fr) | 1.0 3.0 4.0 5.0 5.5 7.0 9.0 12.0 | 1 (1.9%) 4 (7.7%) 11 (21.2%) 9 (17.3%) 4 (7.7%) 21 (40.4%) 1 (1.9%) 1 (1.9%) | 0 (0.0%) 15 (27.3%) 16 (29.1%) 8 (14.5%) 4 (7.3%) 12 (21.8%) 0 (0.0%) 0 (0.0%) | 0.042 |
| No of lumens | 2 | 32 (61.5%) | 43 (78.2%) | 0.090 |
| 3 or more | 20 (38.5%) | 12 (21.8%) | ||
| No of operators | 1 2 | 28 (53.8%) 24 (46.2%) | 40 (72.7%) 15 (27.3%) | 0.047 |
| Years of practice | 0–5 5–10 10 and more | 28 (53.8%) 12 (23.1%) 12 (23.1%) | 31 (56.4%) 4 (7.3%) 20 (36.3%) | 0.048 |
| US-Guided (n = 52) | Landmark (n = 55) | p-value | |||
|---|---|---|---|---|---|
| Mean (SD) | Median (Min-Max) | Mean (SD) | Median (Min-Max) | ||
| Depth of insertion (cm) | 10.6 | 10.5 | 9.2 | 8.0 | 0.031 |
| (3.6) | (5.0–18.0) | (3.6) | (5.0–17.0) | ||
| Time of insertion (min) | 19.3 (11.9) | 15,1 (2.0–50.0) | 14.5 (7.9) | 15.0 (2.7–42.0) | 0.085 |
| Category | US-Guided (n = 52) | Landmark (n = 55) | p-Value | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Artificial punction of artery | No Yes | 48 (92.3%) 4 (7.7%) | 53 (96.4%) 2 (3.6%) | 0.429 |
| Insertion of guidewire (No. of attempts) | 1st 2nd 3rd or more | 36 (69.2%) 11 (21.2%) 5 (9.6%) | 48 (87.3%) 5 (9.1%) 2 (3.6%) | 0.075 |
| Periprocedural X-ray control | No | 3 (5.8%) | 3 (5.5%) | 1.000 |
| Yes | 49 (94.2%) | 52 (94.5%) | ||
| X-ray control and possible malposition | No Yes–no malposition Yes–malposition | 7 (13.5%) 37 (71.2%) 8 (15.4%) | 3 (5.5%) 47 (85.5%) 5 (9.1%) | 0.222 |
| Pneumothorax | No control Control–PNO Control–no PNO | 7 (13.5%) 44 (84.6%) 1 (1.9%) | 2 (3.6%) 52 (94.5%) 1 (1.8%) | 0.125 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vafek, V.; Skříšovská, T.; Kosinová, M.; Klabusayová, E.; Musilová, T.; Kramplová, T.; Djakow, J.; Klučka, J.; Kalina, J.; Štourač, P. Central Venous Catheter Cannulation in Pediatric Anesthesia and Intensive Care: A Prospective Observational Trial. Children 2022, 9, 1611. https://doi.org/10.3390/children9111611
Vafek V, Skříšovská T, Kosinová M, Klabusayová E, Musilová T, Kramplová T, Djakow J, Klučka J, Kalina J, Štourač P. Central Venous Catheter Cannulation in Pediatric Anesthesia and Intensive Care: A Prospective Observational Trial. Children. 2022; 9(11):1611. https://doi.org/10.3390/children9111611
Chicago/Turabian StyleVafek, Václav, Tamara Skříšovská, Martina Kosinová, Eva Klabusayová, Tereza Musilová, Tereza Kramplová, Jana Djakow, Jozef Klučka, Jiří Kalina, and Petr Štourač. 2022. "Central Venous Catheter Cannulation in Pediatric Anesthesia and Intensive Care: A Prospective Observational Trial" Children 9, no. 11: 1611. https://doi.org/10.3390/children9111611
APA StyleVafek, V., Skříšovská, T., Kosinová, M., Klabusayová, E., Musilová, T., Kramplová, T., Djakow, J., Klučka, J., Kalina, J., & Štourač, P. (2022). Central Venous Catheter Cannulation in Pediatric Anesthesia and Intensive Care: A Prospective Observational Trial. Children, 9(11), 1611. https://doi.org/10.3390/children9111611