Abstract
Background: This study investigated the effect of different components of screen time (mobile phone use, TV/video viewing, and video gaming) on cardiorespiratory fitness (CRF) development in children aged 9–12 years. Methods: This was a two-year longitudinal study conducted with 175 children (49.7% girls, mean age = 9.5) in Japan. CRF was assessed using a 20 m shuttle run test conducted at baseline and again at follow-up. Children were categorized as “Good” or “Poor” based on the change in CRF scores for each gender. Screen time was assessed using a self-reported questionnaire at baseline and termed as “high” if children reported ≥ 2 h/day. Univariate and multivariate logistic regression analyses were performed after adjusting for gender, physical activity, and time of data collection. Results: Children scoring “high” on mobile phone use had lower odds of being categorized as “Good” in CRF change (crude odds ratio (OR): 0.34; 95% confidence interval (CI): 0.15–0.90 (adjusted OR: 0.33; 95% CI: 0.12–0.91)). There were no significant effects of TV/video viewing (crude OR: 1.54; 95% CI: 0.84–2.81) and video gaming (crude OR: 0.98; 95% CI: 0.48–1.97) on changes in CRF. Conclusions: Limiting excessive mobile phone usage might be important for ensuring healthy development of CRF in children.
1. Introduction
There has been a substantial decline in cardiorespiratory fitness (CRF) among children in developed countries since the 1980s [1,2,3]. In children, lower CRF is associated with poor academic achievement, adiposity, and onset of depression and anxiety [4,5,6,7]. On the other hand, CRF is associated with preventing the negative health effects of stress in youth and improving social health [8,9]. Thus, it is important to understand the cause behind the substantial decline in CRF.
The increasing amount of time spent in front of screens has been identified as one cause for this [10]. Previous studies have reported that the total screen time, including watching TV/videos, playing video games, and using a computer, was negatively associated with changes in CRF in children between the ages of 11 to 13 [11,12]. In addition to this, the percentage of children aged 8–11 years who own a mobile phone has been increasing over the years (from 13% in 2010 to 35% in 2017), along with an increase in mobile phone use for watching videos and playing games and a decrease in time spent watching TV [13]. Consequently, a study in 2015 reported that mobile phones had been added to the total screen time, and this total screen time was also negatively associated with CRF [14]. Therefore, it is necessary to investigate the effect of mobile phone use, in addition to TV/video viewing and video gaming, on CRF development.
However, to the best of our knowledge, there have been only a few studies that have investigated the longitudinal association between mobile phone use and CRF development. Similarly, there have been a few studies that have investigated the difference in the effect of the various components of screen time (TV/video viewing, video gaming, and mobile phone use) on CRF development. Furthermore, it is important to investigate the relationships between screen time and CRF during the age when maximum development of CRF takes place (for boys, at 11.4 years; for girls, at 10.5 years) [15].
In line with this, the purpose of this study was to investigate the effect of each type of screen time (including mobile phone use, TV/video viewing, and video gaming) on CRF development in children between the ages of 9–10 to 11–12 years.
2. Methods
2.1. Participants
This was a 2-year longitudinal study. We recruited fourth-grade children from two public elementary schools in Kobe, Japan, as participants from May to October 2016 and from May to October 2017. The inclusion criteria were those who gave consent to participate in our study. The exclusion criteria were as follows: (1) children who missed follow-up and (2) children whose data were missing. We explained the study protocol to the principals, teachers, and children and obtained informed consent from both the children and their guardians. This study protocol was approved by the Research Ethics Committee of Kobe University Graduate School of Health Science (Approval number: 545-3).
2.2. Procedure
A self-reported questionnaire, anthropometric measurements, and a 20 m shuttle run test were used to gather data at both baseline (2016 and 2017) and at the 2-year follow-up (2018 and 2019). The children answered the questionnaire with support from well-trained research assistants. Anthropometric measurements and 20 m shuttle run test were conducted by elementary school teachers and the school staff.
2.3. Measurements
- (1)
- Demographic data
The children’s age and gender were ascertained from the self-reported questionnaire. Their height (cm) and weight (kg) were obtained from the records of the routine health examinations conducted at the elementary schools. Body mass index (BMI) was calculated as weight in kilograms divided by height in meter squared (kg/m2).
- (2)
- Cardiorespiratory Fitness (CRF)
CRF was assessed using the 20 m shuttle run test, which is a valid and reliable way of assessing CRF in children [16]. The 20 m shuttle run test was conducted according to the guidelines for physical fitness measurement prescribed by the Ministry of Education, Culture, Sports, Science, and Technology of Japan [17]. Participants ran back and forth between lines set 20 m apart while keeping pace with audio signals emitted from a pre-recorded compact disc. The initial speed was 8.5 km/h, and the pace was increased by 0.5 km/h every minute. The test ended when the participants could no longer maintain the pace or could not complete two laps continuously within the time limit. The total number of laps was recorded at the end of the test.
- (3)
- Screen time
Information regarding screen time was obtained using a self-reported questionnaire. We assessed screen time spent on each electronic device, including mobile phone use, TV/video viewing, and video gaming, during the daytime. Participants indicated their daily screen time as “no time spent”, “30 min”, “1 h”, “2 h”, “3 h”, “4 h”, “5 h”, “6 h”, or “≥7 h” [18,19]. From 2017 to 2019, we assessed the average time spent daily during the daytime on each component. In 2016, we assessed the time spent on weekdays and weekends separately and calculated the daily average time as follows: {(weekday times) × 5 + (weekend time) × 2}/7. There is a moderate-to-high agreement between repeated responses to the screen time questions, with Kappa coefficients ranging from 0.68 to 0.82 [20]. We categorized the duration of each component of screen time into <2 h/day and ≥2 h/day [21,22].
- (4)
- Physical Activity (PA)
We assessed PA using the Japanese version of the Physical Activity Questionnaire for Older Children (PAQ-C), which has acceptable reliability and validity (Cronbach’s alpha = 0.81, intraclass correlation coefficients = 0.83) [23]. The PAQ-C is a self-reported 7-day recall questionnaire that measures general levels of moderate to vigorous PA in 8–14-year-olds, during the school year. The PAQ-C consists of nine computable items, and each item was scored on a 5-point scale, with higher scores indicating higher PA levels. The total PAQ-C score was calculated as the mean score of the nine items, ranged between 1.00 (lowest activity level) and 5.00 (highest activity level), and was used as a continuous variable [24].
2.4. Statistical Analysis
Within each gender group, children were divided into tertiles on the basis of their performance in the 20 m shuttle run test at baseline and follow-up. Children were categorized as “Poor” if they moved down a lower tertile during follow-up or if they maintained the lowest tertile. Alternately, children were categorized as “Good” if they moved up to a higher tertile or if they maintained the middle or the highest tertile. A univariate logistic regression analysis was used to assess the effects of different components of screen time at baseline on the changes observed in CRF over the two-year period. The analysis was performed using screen time as an independent variable and the change in CRF as the outcome variable (1: Good and 0: Poor). Multivariate logistic regression analysis was also performed while adjusting for gender, physical activity, and time of data collection (2016 or 2017), since screen time and CRF have been found to be associated with gender and PA [10,25]. The level of significance was set at p < 0.05. The data were analyzed using the free software EZR Version 1.40 (Jichi Medical University Saitama Medical Center, Saitama, Japan) [26].
3. Results
Figure 1 reveals the participant flow during the study. We recruited 203 children, and all 203 were initially included. However, we then excluded 14 children who had missed follow-up and another 14 whose data were missing (CRF, n = 14). Finally, 175 children were included in the analysis (mean age ± standard deviation: 9.5 ± 0.5; boys, n = 88 and girls, n = 87).
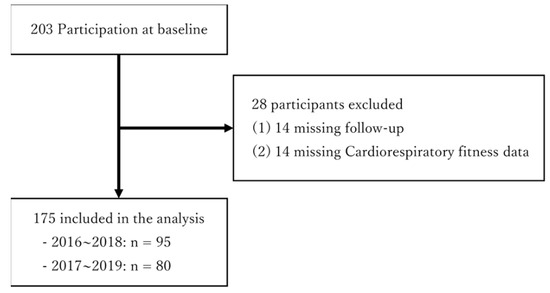
Figure 1.
Flow chart of participation, detailing loss to follow-up and final participant sample used in this study (n = 175).
Table 1 presents the study sample characteristics according to time point (baseline and follow-up) and gender. During the follow-up period, mean laps in the 20 m shuttle run test increased by 14.4 for boys and by 12.9 for girls. A total of 99 children were categorized as “Good” based on the changes in their scores for CRF. At the baseline, 23 (13%) children were using mobile phones, 98 (56%) were watching TV/videos, and 41 (23%) were playing video games for two hours or more a day. Further, among these children who spent 2 h or more a day on their screens, the number of children who were categorized as “Good”, with respect to their 2-year changes in CRF, was 8/23 (35%) for those using mobile phones, 60/98 (61%) for those watching TV/videos, and 23/41 (56%) for those playing video games.

Table 1.
Characteristic of the study sample (n = 175).
Table 2 shows the results of the logistic regression analysis. In the univariate logistic regression models, children who used their mobile phones for 2 h or more a day had significantly lower odds of being categorized as “Good” based on the changes in their CRF scores over the two years, as compared with those who used their phones for less than 2 h a day (odds ratio: 0.34; 95% confidence interval: 0.15–0.90). Similarly, in the multivariate logistic regression models, children who used their mobile phones for 2 h or more a day also had lower odds of being categorized as “Good” based on the changes in their CRF scores, as compared with those who used their phones for less than 2 h a day (odds ratio: 0.33; 95% confidence interval: 0.12–0.91). There were no significant effects found for TV/video viewing (odds ratio: 1.54; 95% confidence interval: 0.84–2.81) or video gaming (odds ratio: 0.98; 95% confidence interval: 0.48–1.97) on the change in CRF.
Table 2.
Univariate and multivariate logistic models assessing the effects of each screen time on 2 years change in CRF.
4. Discussion
This study investigated the longitudinal association between different components of screen time (mobile phone use, TV/video viewing, and video gaming) and changes in CRF over a period of 2 years among 9–12 year old children. We found that children who used mobile phones for ≥2 h/day had poor CRF development, independent of their gender, PA, and time at which the data were collected. However, TV/video viewing and video gaming were not associated with changes in CRF over the two-year period.
Previous studies have shown that an increase in total screen time negatively impacts CRF development in children [11,12]. Our results supported the findings from previous studies. Furthermore, the present study was the first to investigate the longitudinal association between different components of screen time and CRF.
Excessive sedentary behavior might be one explanation as to why mobile phone use changed CRF over a two-year period. Screen time accounts for an overall sedentary time among children and youth [27]. Additionally, excessive sedentary behavior influences lower CRF [28]. Elementary school children mainly use mobile phone for playing games [29]; online video viewing and playing video games time on mobile phones were increasing, while TV viewing time was decreasing [14]. Since mobile phones have become widespread and is replacing TV and video games [13], even children using mobile phone only, may present excessive sedentary behavior. Therefore, it was possible that ≥2 h/day mobile phone use negatively affected CRF development. However, future studies are needed to determine the difference in the effect of each device usage on CRF development since our samples who were ≥2 h/day for TV/videos and video games were larger than for mobile phones.
Another possible explanation for the negative effect of mobile phone use on CRF development could be unhealthy sleeping habits. Inadequate amounts of sleep and poor sleep quality have previously been associated with poorer CRF development [30,31]. There are several ways in which mobile phone use can cause difficulties in sleep. First, due to the pulse-modulated radiofrequency fields used in mobile phones, greater use of mobile phones has been associated with lower sleep duration [32]. Furthermore, prolonged use of wireless phones is associated with lower concentrations of β-trace protein (lipocalin-type prostaglandin D synthase), which is a key enzyme in the synthesis of prostaglandin D2, an endogenous sleep-promoting neurohormone [33]. Second, nocturnal awakening due to incoming text messages and calls leads to poorer sleep quality, including problems with falling asleep and disturbed sleep [34]. Third, due to the portability of mobile phones and ease of connectivity, the tendency to develop an addiction to them is stronger than that for a TV [35]. Greater mobile phone addiction has also been found to increase the risk of poor sleep quality [36]. In view of these reasons, it seems likely that excessive mobile phone use might lead to unhealthy sleeping habits, which in turn negatively affect CRF development; although, this study did not investigate the purpose of mobile phone use and sleep habits. Future studies need to include the purpose of screen time and sleep habits, clarifying the factor that influences CRF.
While our results were consistent with the findings from previous research [11,12], this study had several limitations. First, the sample size was small. Second, screen time and physical activity were assessed using self-reported questionnaires. Although these questionnaires were evaluated in terms of their reliability and validity [20,24], more objective measures of screen time and physical activity can be considered for use in future studies. Finally, this study lacked maturity status and parental economic status data, which could have influenced the findings. These variables should be considered in future longitudinal studies.
5. Conclusions
This study revealed that mobile phone use had a negative effect on CRF development over a period of two-year period, among 9–12 year old children. This suggests that, in today’s world, where several types of electronic devices exist, limiting excessive mobile phone use might be important for ensuring the healthy development of CRF in school children.
Author Contributions
Conceptualization, R.G. and T.I.; methodology, R.G. and T.I.; formal analysis, R.G.; investigation, R.G., T.I., R.K., K.H., Y.T., K.N., K.U., and K.S.; data curation, R.O.; writing—original draft preparation, R.G.; writing—review and editing, T.I., R.K., K.H., Y.T., K.N., K.U., K.S., and R.O.; visualization, R.G.; supervision, R.O.; project administration, R.O.; funding acquisition, T.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Sasakawa Sports Research Grant from Sasakawa Sports Foundation (grant number 180B3-042). The funding source had no involvement in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Kobe University Graduate School of Health Science (approval number: 545-3).
Informed Consent Statement
We explained the study protocol to the principals, teachers, and children and obtained informed consent from both the children and their guardians.
Data Availability Statement
The data are available upon request to the corresponding author.
Acknowledgments
The authors thank the teachers and children of the two schools that participated in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S. Temporal trends in the cardiorespiratory fitness of children and adolescents representing 19 high-income and upper middle-income countries between 1981 and 2014. Br. J. Sports Med. 2019, 53, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Education, Culture, Sports, Science and Technology. 2002 Central Education Council Report, Comprehensive Measures to Improve Physical Fitness of Children. Available online: http://www.mext.go.jp/b_menu/shingi/chukyo/chukyo0/gijiroku/attach/1344530.htm (accessed on 25 November 2019). (In Japanese).
- Japan Sports Agency. About Summary and Report of 2018 Physical Strength and Athletic Performance Survey Results. Available online: http://www.mext.go.jp/sports/b_menu/toukei/chousa04/tairyoku/kekka/k_detail/1421920.htm (accessed on 25 November 2019). (In Japanese).
- Sardinha, L.B.; Marques, A.; Minderico, C.; Palmeira, A.; Martins, S.; Santos, D.; Ekelund, U. Longitudinal Relationship between Cardiorespiratory Fitness and Academic Achievement. Med. Sci. Sports Exerc. 2016, 48, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, S.I.; Stolk, R.P.; Liem, E.T.; Lemmink, K.A.P.M.; Corpeleijn, E. The role of fitness in the association between fatness and cardiometabolic risk from childhood to adolescence. Pediatr. Diabetes 2013, 14, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.P.; Leitão, R.; Lopes, V.P. Physical fitness predicts adiposity longitudinal changes over childhood and adolescence. J. Sci. Med. Sport. 2013, 16, 118–123. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mücke, M.; Ludyga, S.; Brand, S.; Colledge, F.; Pühse, U.; Gerber, M. Associations between Cardiorespiratory Fitness and Endocrine, Autonomous and Psychological Stress Reactivity in Male Adolescents. J. Psychophysiol. 2021, 35, 23–34. [Google Scholar] [CrossRef]
- Fernández-Bustos, J.G.; Pastor-Vicedo, J.C.; González-Martí, I.; Cuevas-Campos, R. Physical Fitness and Peer Relationships in Spanish Preadolescents. Int. J. Environ. Res. Public Health 2020, 17, 1890. [Google Scholar] [CrossRef]
- Saunders, T.J.; Vallance, J.K. Screen Time and Health Indicators among Children and Youth: Current Evidence, Limitations and Future Directions. Appl. Health Econ. Health Policy 2017, 15, 323–331. [Google Scholar] [CrossRef]
- Aggio, D.; Ogunleye, A.A.; Voss, C.; Sandercock, G.R.H. Temporal relationships between screen-time and physical activity with cardiorespiratory fitness in English Schoolchildren: A 2-year longitudinal study. Prev. Med. 2012, 55, 37–39. [Google Scholar] [CrossRef]
- Mitchell, J.A.; Pate, R.R.; Blair, S.N. Screen-Based Sedentary Behavior and Cardiorespiratory Fitness from Age 11 to 13. Med. Sci. Sports Exerc. 2012, 44, 1302–1309. [Google Scholar] [CrossRef]
- Ofcom.org.uk. Children’s Media Use and Attitudes. Available online: https://www.ofcom.org.uk/research-and-data/media-literacy-research/childrens (accessed on 29 November 2019).
- Hardy, L.L.; Ding, D.; Peralta, L.R.; Mihrshahi, S.; Merom, D. Association between Sitting, Screen Time, Fitness Domains, and Fundamental Motor Skills in Children Aged 5–16 Years: Cross-Sectional Population Study. J. Phys. Act. Health 2018, 15, 933–940. [Google Scholar] [CrossRef] [PubMed]
- Ohsawa, S. Determining the optimal age to begin physical fitness training: Derived from an analysis of data from the MEXT new physical fitness test. Jpn. J. Hum. Growth Dev. Res. 2015, 2015, 25–35. [Google Scholar] [CrossRef][Green Version]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Japan Sports Agency. The Guidelines for Physical Fitness Measurement. Available online: http://www.mext.go.jp/sports/b_menu/sports/mcatetop03/list/detail/1408001.htm (accessed on 7 October 2019). (In Japanese).
- Sigmundová, D.; Sigmund, E.; Bucksch, J.; Baďura, P.; Kalman, M.; Hamřík, Z. Trends in Screen Time Behaviours in Czech Schoolchildren between 2002 and 2014: HBSC Study. Cent. Eur. J. Public Health 2017, 25 (Suppl. 1), S15–S20. [Google Scholar] [CrossRef]
- Janssen, I.; Roberts, K.C.; Thompson, W. Adherence to the 24-Hour Movement Guidelines among 10- to 17-year-old Canadians. Health Promot. Chronic Dis. Prev. Can. 2017, 37, 369–375. [Google Scholar] [CrossRef]
- Rey-López, J.P.; Vicente-Rodriguez, G.; Ortega, F.B.; Ruiz, J.R.; Martinez-Gómez, D.; De Henauw, S.; Manios, Y.; Molnar, D.; Polito, A.; Verloigne, M.; et al. Sedentary patterns and media availability in European adolescents: The HELENA study. Prev. Med. 2010, 51, 50–55. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41 (Suppl. 3), S311–S327. [Google Scholar] [CrossRef]
- Department of Health: Australia’s Physical Activity and Sedentary Behaviour Guidelines and the Australian 24-Hour Movement Guidelines. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/health-pubhlth-strateg-phys-act-guidelines (accessed on 14 October 2019).
- Isa, T.; Sawa, R.; Torizawa, K.; Murata, S.; Saito, T.; Ebina, A.; Kondo, Y.; Tsuboi, Y.; Fukuta, A.; Misu, S.; et al. Reliability and Validity of the Japanese Version of the Physical Activity Questionnaire for Older Children. Clin. Med. Insights Pediatr. 2019, 13, 1179556519835833. [Google Scholar] [CrossRef]
- Kowalski, K.C.; Crocker, P.R.E.; Donen, R.M. The Physical Activity Questionnaire for Older Children (PAQ-C) and Adolescents (PAQ-A) Manual; College of Kinesiology, University of Saskatchewan: Saskatoon, SK, Canada, 2004; pp. 1–38. [Google Scholar]
- Porter, A.K.; Matthews, K.J.; Salvo, D.; Kohl, H.W., 3rd. Associations of Physical Activity, Sedentary Time, and Screen Time with Cardiovascular Fitness in United States Adolescents: Results from the NHANES National Youth Fitness Survey. J. Phys. Act. Health 2017, 14, 506–512. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely-available easy-to-use software “EZR” (Easy R) for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Gopinath, B.; Hardy, L.L.; Baur, L.A.; Burlutsky, G.; Mitchell, P. Physical activity and sedentary behaviors and health-related quality of life in adolescents. Pediatrics 2012, 130, e167–e174. [Google Scholar] [CrossRef] [PubMed]
- Hjorth, M.F.; Chaput, J.; Michaelsen, K.; Astrup, A.; Tetens, I.; Sjödin, A. Seasonal variation in objectively measured physical activity, sedentary time, cardio-respiratory fitness and sleep duration among 8–11 year-old Danish children: A repeated-measures study. BMC Public Health 2013, 13, 808. [Google Scholar] [CrossRef] [PubMed]
- Cabinet Office. Survey on Internet Usage Environment for Young People. Available online: https://www8.cao.go.jp/youth/youth-harm/chousa/net-jittai_list.html (accessed on 25 November 2019). (In Japanese).
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Association of cardiorespiratory fitness levels with dietary habits and lifestyle factors in schoolchildren. Appl. Physiol. Nutr. Metab. 2019, 44, 539–545. [Google Scholar] [CrossRef]
- Mota, J.; Vale, S. Associations between sleep quality with cardiorespiratory fitness and BMI among adolescent girls. Am. J. Hum. Biol. 2010, 22, 473–475. [Google Scholar] [CrossRef] [PubMed]
- Huss, A.; van Eijsden, M.; Guxens, M.; Beekhuizen, J.; van Strien, R.; Kromhout, H.; Vrijkotte, T.; Vermeulen, R. Environmental Radiofrequency Electromagnetic Fields Exposure at Home, Mobile and Cordless Phone Use, and Sleep Problems in 7-Year-Old Children. PLoS ONE 2015, 10, e0139869. [Google Scholar] [CrossRef]
- Söderqvist, F.; Carlberg, M.; Zetterberg, H.; Hardell, L. Use of wireless phones and serum β-trace protein in randomly recruited persons aged 18–65 years: A cross-sectional study. Electromagn. Biol. Med. 2012, 31, 416–424. [Google Scholar] [CrossRef]
- Foerster, M.; Henneke, A.; Chetty-Mhlanga, S.; Röösli, M. Impact of Adolescents’ Screen Time and Nocturnal Mobile Phone-Related Awakenings on Sleep and General Health Symptoms: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 518. [Google Scholar] [CrossRef]
- Kwon, M.; Lee, J.Y.; Won, W.Y.; Park, J.W.; Min, J.A.; Hahn, C.; Gu, X.; Choi, J.; Kim, D. Development and validation of a smartphone addiction scale (SAS). PLoS ONE 2013, 8, e56936. [Google Scholar] [CrossRef]
- Lee, J.E.; Jang, S.I.; Ju, Y.J.; Kim, W.; Lee, H.J.; Park, E.C. Relationship between Mobile Phone Addiction and the Incidence of Poor and Short Sleep among Korean Adolescents: A Longitudinal Study of the Korean Children & Youth Panel Survey. J. Korean Med. Sci. 2017, 32, 1166–1172. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).