
Meditation Effects on Anxiety and Resilience of Preadolescents and Adolescents: A Randomized Controlled Study




Abstract
:1. Introduction
1.1. Anxiety
1.2. Resilience
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.2.1. Multidimensional Anxiety Scale for Children (MASC)
2.2.2. Strengths and Difficulties Questionnaire (SDQ)
2.2.3. Health Kids Resilience Assessment Module (HKRA)
2.3. Intervention
2.4. Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomas, J.; Cohen, M. A methodological review of meditation research. Front. Psychiatry 2014, 5, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, M.M.; Penman, S.; Pirotta, M.; Da Costa, C. The integration of complementary therapies in Australian general practice: Results of a national survey. J. Altern. Complement. Med. 2005, 11, 995–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matko, K.; Sedlmeier, P. What is meditation? Proposing an empirically derived classification system. Front. Psychol. 2019, 10, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bond, K.; Ospina, M.B.; Hooton, N.; Bialy, L.; Dryden, D.M.; Buscemi, N.; Shannahoff-Khalsa, D.; Dusek, J.; Carlson, L.E. Defining a complex intervention: The development of demarcation criteria for “meditation”. Psychol. Relig. Spiritual. 2009, 1, 129–137. [Google Scholar] [CrossRef]
- Ganguly, A.; Hulke, S.; Bharshanakar, R.; Parashar, R.; Wakode, S. Effect of meditation on autonomic function in healthy individuals: A longitudinal study. J. Fam. Med. Prim. Care 2020, 9, 3944–3948. [Google Scholar] [CrossRef]
- Mosini, A.C.; Saad, M.; Braghetta, C.C.; De Medeiros, R.; Peres, M.F.P.; Leão, F.C. Neurophysiological, cognitive-behavioral and neurochemical effects in practitioners of transcendental meditation—A literature review. Rev. Assoc. Med. Bras. 2019, 65, 706–713. [Google Scholar] [CrossRef]
- Waters, L.; Barsky, A.; Ridd, A.; Allen, K. Contemplative education: A systematic, evidence-based review of the effect of meditation interventions in schools. Educ. Psychol. Rev. 2015, 27, 103–134. [Google Scholar] [CrossRef] [Green Version]
- Elder, C.; Nidich, S.; Colbert, R.; Hagelin, J.; Grayshield, L.; Oviedo-Lim, D.; Nidich, R.; Rainforth, M.; Jones, C.; Gerace, D. Reduced Psychological Distress in Racial and Ethnic Minority Students Practicing the Transcendental Meditation Program. J. Instr. Psychol. 2011, 38, 109–116. [Google Scholar]
- Colbert, R. Effect of the Transcendental Meditation program on graduation, college acceptance and dropout rates for students attending an urban public high school. Education 2013, 133, 495–501. Available online: https://www.ingentaconnect.com/content/prin/ed/2013/00000133/00000004/art00012 (accessed on 5 May 2021).
- Wendt, S.; Hipps, J.; Abrams, A.; Grant, J.; Valosek, L.; Nidich, S. Practicing transcendental meditation in high schools: Relationship to well-being and academic achievement among students. Contemp. School Psychol. 2015, 19, 312–319. [Google Scholar] [CrossRef]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child. Psychol. Psychiatry Allied Discip. 2015, 56, 345–365. [Google Scholar] [CrossRef] [PubMed]
- Voltas, N.; Hernández-Martínez, C.; Arija, V.; Canals, J. The natural course of anxiety symptoms in early adolescence: Factors related to persistence. Anxiety Stress Coping 2017, 30, 671–686. [Google Scholar] [CrossRef]
- Pinto, J.C.; Martins, P.; Pinheiro, T.B.; Oliveira, A.C. Ansiedade, Depressão e Stresse: Um Estudo com Jovens Adultos e Adultos Portugueses. Psicol. Saúde Doenças 2015, 16, 148–163. [Google Scholar] [CrossRef] [Green Version]
- Grolli, V.; Wagner, M.F.; Dalbosco, S.N.P. Sintomas Depressivos e de Ansiedade em Adolescentes do Ensino Médio. Rev. Psicol. IMED 2017, 9, 87. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, P.M. Anxiety. In Magill’S Medical Guide (Online Edition); Salem Press: Pasadena, CA, USA, 2017. [Google Scholar]
- Keeley, M.L.; Storch, E.A. Anxiety Disorders in Youth. J. Pediatr. Nurs. 2009, 24, 26–40. [Google Scholar] [CrossRef]
- Rosen, R.H. Embracing uncertainty and anxiety. Lead. Lead. 2008, 2008, 34–38. [Google Scholar] [CrossRef]
- Grissom, C. Resilience in Students. Educ. Forum 2015, 79, 206–207. [Google Scholar] [CrossRef]
- Masten, A.S. Ordinary magic: Resilience processes in development. Am. Psychol. 2001, 56, 227–238. [Google Scholar] [CrossRef]
- Wu, Y.; Sang, Z.Q.; Zhang, X.C.; Margraf, J. The relationship between resilience and mental health in Chinese college students: A longitudinal cross-lagged analysis. Front. Psychol. 2020, 11, 1–11. [Google Scholar] [CrossRef]
- Abiola, T.; Udofia, O. Psychometric assessment of the Wagnild and Young’s resilience scale in Kano, Nigeria. BMC Res. Notes 2011, 4, 509. [Google Scholar] [CrossRef] [Green Version]
- Valosek, L.; Wendt, S.; Link, J.; Abrams, A.; Hipps, J.; Grant, J.; Nidich, R.; Loiselle, M.; Nidich, S. Meditation Effective in Reducing Teacher Burnout and Improving Resilience: A Randomized Controlled Study. Front. Educ. 2021, 6, 1–6. [Google Scholar] [CrossRef]
- Arrogante, Ó. Mediator effect of resilience between burnout and health in nursing staff. Enferm. Clin. 2014, 24, 283–289. [Google Scholar] [CrossRef]
- March, J.; Parker, J.; Sullivan, K.; Stallings, P.; Conners, K. The Multidimensional Anxiety Scale for Children (MASC): Factor Structure, Reliability, and Validity. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 554–565. [Google Scholar] [CrossRef]
- Goodman, R.; Meltzer, H.; Bailey, V. The Strengths and Difficulties Questionnaire: A pilot study on the validity of the self-report version. Eur. Child Adolesc. Psychiatry 1998, 7, 125–130. [Google Scholar] [CrossRef]
- Constantine, N.A.; Bernard, B. California Healthy Kids Survey Resilience Assessment Module: Technical Report; Public Health Institute: Berkeley, CA, USA, 2001. [Google Scholar]
- Salvador, M.C.; Matos, A.P.; Oliveira, S.; March, J.; Arnarson, E.; Carey, S.; Craighead, E. The Multidimensional Anxiety Scale for Children (MASC): Psychometric Properties and Confirmatory Factor Analysis in a Sample of Portuguese Adolescents. Rev. Iberoam. Diagn. Eval. Aval. Psicol. 2017, 45, 33–46. [Google Scholar] [CrossRef]
- March, J.S.; Sullivan, K.; Parker, J. Test-retest reliability of the Multidimensional Anxiety Scale for Children. J. Anxiety Disord. 1999, 13, 349–358. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Pechorro, P.; Poiares, C.; Vieira, R. Psychometric properties of the Portuguese self-report version of the Strenghts and Difficulties Questionnaire. Rev. Psiquiatr. Cons. Ligação 2011, 16–19, 99–109. [Google Scholar]
- Constantine, N.; Benard, B.; Diaz, M. Measuring protective factors and resilience traits in youth: The healthy kids resilience assessment. In Proceedings of the Seventh Annual Meeting of the Society for Prevention Research, New Orleans, LA, USA, 24–26 June 1999; pp. 3–15. [Google Scholar]
- Martins, M.H. Contributions to the Analysis of Children and Youth at Risk/Resilience and Development. Unpublished. Doctoral Thesis, Universidade do Algarve, Faro, Portugal, 2005. Available online: http://hdl.handle.net/10400.1/8497 (accessed on 20 January 2017).
- Nidich, S.I.; Rainforth, M.V.; Haaga, D.A.; Hagelin, J.; Salerno, J.W.; Travis, F.; Tanner, M.; Gaylord-King, C.; Grosswald, S.; Schneider, R.H. A randomized controlled trial on effects of the Transcendental Meditation program on blood pressure, psychological distress, and coping in young adults. Am. J. Hypertens. 2009, 22, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Nidich, S.; Mjasiri, S.; Nidich, R.; Rainforth, M.; Grant, J.; Valosek, L.; Chang, W.; Zigler, R.L. Academic Achievement and Transcendental Meditation: A Study with At-Risk Urban Middle School Students. Education 2011, 131, 556–564. [Google Scholar]
- Orme-Johnson, D.W. Transcendental Meditation in the Treatment of Mental and Physical Conditions. In The Oxford Handbook of Meditation; Farias, M., Braziera, D., Lalljee, M., Eds.; Oxford University Press: Oxford, UK, 2020; pp. 1–37. [Google Scholar]
- So, K.-T.; Orme-Johnson, D.W. Three randomized experiments on the longitudinal effects of the Transcendental Meditation technique on cognition. Intelligence 2001, 29, 419–440. [Google Scholar] [CrossRef]
- Woolfolk, R.L.; Rooney, A.J. The effect of explicit expectations on initial meditation experiences. Biofeedback Self-Regul. 1981, 6, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.; Gauntlett-Gilbert, J. Mindfulness with Children and Adolescents: Effective Clinical Application. Clin. Child Psychol. Psychiatry 2008, 13, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Orme-Johnson, D.W.; Barnes, V.A. Effects of the transcendental meditation technique on trait anxiety: A meta-analysis of randomized controlled trials. J. Altern. Complement. Med. 2014, 20, 330–341. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Before | After | ||||
|---|---|---|---|---|---|---|
| Experimental | Control | Mean | Experimental | Control | Mean | |
| (Mean ± SD) | Differences (p) | (Mean ± SD) | Differences (p) | |||
| Anxiety | ||||||
| Humiliation | 5.88 ± 3.580 | 4.82 ± 3.358 | 0.057 | 3.92 ± 3.373 | 3.60 ± 2.775 | 0.521 |
| Public performance fears | 4.89 ± 2.334 | 4.68 ± 2.376 | 0.573 | 3.30 ± 2.170 | 3.22 ± 2.211 | 0.832 |
| Separation anxiety | 6.99 ± 2.882 | 7.23 ± 3.561 | 0.640 | 5.02 ± 2.793 | 5.57 ± 3.283 | 0.435 |
| Perfectionism | 6.98 ± 1.763 | 7.01 ± 2.098 | 0.934 | 7.25 ± 0.121 | 6.90 ± 1.996 | 0.287 |
| Anxious coping | 7.83 ± 2.559 | 7.82 ± 2.465 | 0.999 | 6.78 ± 2.743 | 6.44 ± 3.001 | 0.451 |
| Tense/Restless | 4.18 ± 2.931 | 3.91 ± 2.650 | 0.532 | 3.14 ± 2.588 | 3.05 ± 2.184 | 0.814 |
| Somatic/Autonomic | 3.16 ± 2.623 | 3.23 ± 2.852 | 0.879 | 2.02 ± 1.960 | 2.08 ± 2.442 | 0.856 |
| Strengths and Difficulties | ||||||
| Internalizing problems | 9.03 ± 2.079 | 9.17 ± 1.896 | 0.661 | 8.89 ± 1.977 | 8.51 ± 1.916 | 0.211 |
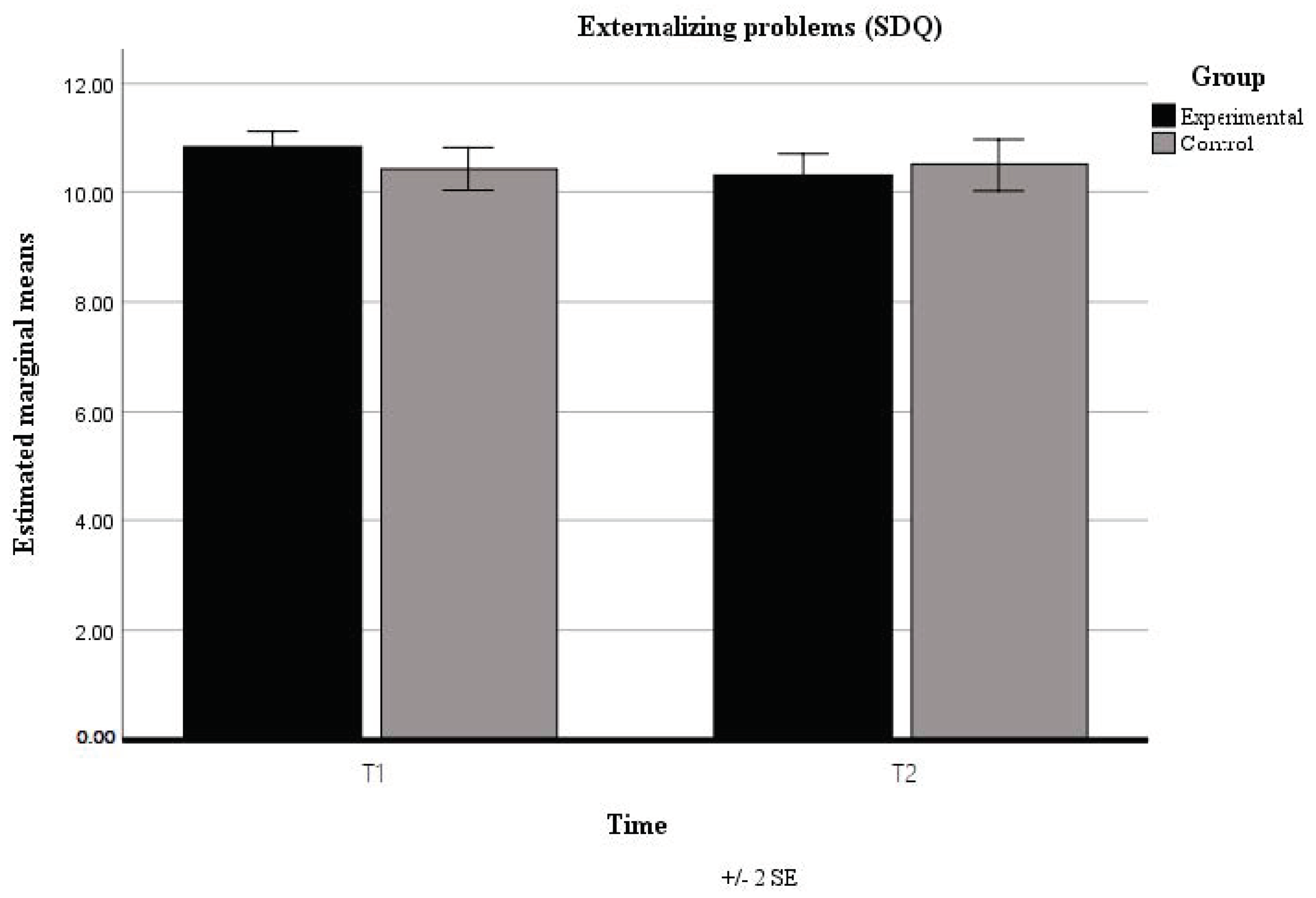
| Externalizing problems | 10.82 ± 1.572 | 10.42 ± 1.579 | 0.107 | 10.30 ± 2.059 | 10.50 ± 1.818 | 0.523 |
| Prosocial behavior | 8.40 ± 1.081 | 8.45 ± 1.180 | 0.786 | 7.88 ± 1.481 | 7.99 ± 1.359 | 0.638 |
| Resilience | ||||||
| External resources | 3.09 ± 0.416 | 3.06 ± 0.487 | 0.613 | 3.13 ± 0.503 | 3.12 ± 0.499 | 0.954 |
| Internal resources | 3.19 ± 0.459 | 3.13 ± 0.567 | 0.429 | 3.22 ± 0.606 | 3.15 ± 0.653 | 0.497 |
| Response set breakers | 2.96 ± 0.359 | 2.94 ± 0.475 | 0.782 | 3.02 ± 0.474 | 2.98 ± 0.514 | 0.585 |
| Time | Group | Time * Group | |||||||
|---|---|---|---|---|---|---|---|---|---|
| F | p | η2p | F | p | η2p | F | p | η2p | |
| Anxiety | |||||||||
| Humiliation | 49.299 | <0.001 * | 0.229 | 2.113 | 0.148 | 0.016 | 2.624 | 0.107 | 0.013 |
| Public performance fears | 72.773 | <0.001 * | 0.305 | 0.208 | 0.649 | 0.001 | 0.145 | 0.704 | 0.0008 |
| Separation anxiety | 50.371 | <0.001 * | 0.233 | 0.515 | 0.474 | 0.003 | 0.075 | 0.784 | 0.0004 |
| Perfectionism | 0.216 | 0.643 | 0.001 | 0.353 | 0.553 | 0.002 | 1.393 | 0.240 | 0.008 |
| Anxious coping | 29.106 | <0.001 * | 0.149 | 0.224 | 0.637 | 0.001 | 0.565 | 0.453 | 0.003 |
| Tense/Restless | 17.998 | <0.001 * | 0.098 | 0.277 | 0.599 | 0.002 | 0.179 | 0.673 | 0.001 |
| Somatic/Autonomic | 51.096 | <0.001 * | 0.235 | 0.001 | 0.992 | 0.0001 | 0.033 | 0.857 | 0.0006 |
| Strengths and Difficulties | |||||||||
| Internalizing problems | 7.046 | 0.009 * | 0.041 | 0.204 | 0.652 | 0.001 | 3.069 | 0.082 | 0.018 |
| Externalizing problems | 2.177 | 0.142 | 0.013 | 0.181 | 0.671 | 0.001 | 4.237 | 0.041 * | 0.025 |
| Prosocial behavior | 20.988 | <0.001 * | 0.112 | 0.202 | 0.654 | 0.001 | 0.074 | 0.786 | 0.0004 |
| Resilience | |||||||||
| External resources | 2.245 | 0.136 | 0.013 | 0.091 | 0.764 | 0.0005 | 0.209 | 0.648 | 0.001 |
| Internal resources | 0.250 | 0.618 | 0.002 | 0.700 | 0.404 | 0.004 | 0.002 | 0.963 | 0.0001 |
| Response set breakers | 2.115 | 0.148 | 0.013 | 0.243 | 0.622 | 0.001 | 0.112 | 0.738 | 0.0007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomes, A.; Vieira dos Santos, J.; Vieira, L.S. Meditation Effects on Anxiety and Resilience of Preadolescents and Adolescents: A Randomized Controlled Study. Children 2021, 8, 689. https://doi.org/10.3390/children8080689
Gomes A, Vieira dos Santos J, Vieira LS. Meditation Effects on Anxiety and Resilience of Preadolescents and Adolescents: A Randomized Controlled Study. Children. 2021; 8(8):689. https://doi.org/10.3390/children8080689
Chicago/Turabian StyleGomes, Alexandra, Joana Vieira dos Santos, and Luís Sérgio Vieira. 2021. "Meditation Effects on Anxiety and Resilience of Preadolescents and Adolescents: A Randomized Controlled Study" Children 8, no. 8: 689. https://doi.org/10.3390/children8080689
APA StyleGomes, A., Vieira dos Santos, J., & Vieira, L. S. (2021). Meditation Effects on Anxiety and Resilience of Preadolescents and Adolescents: A Randomized Controlled Study. Children, 8(8), 689. https://doi.org/10.3390/children8080689