
Urinary Biomarkers of Renal Injury KIM-1 and NGAL: Reference Intervals for Healthy Pediatric Population in Sri Lanka

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- Aged between 10 and 18 years at the time of enrollment.
- Expressed consent of the children and the parents for participation, medical examination, donation of samples and long-term storage, and to produce records on medical history and current medications.
- Willingness to be contacted for future updates on medical status.
- Within normal BMI range (18.5–22.9 kg/m2) [18].
- Known genetic disorders.
- Family history of chronic kidney disease.
- History or persistence of renal injury or disease kidney injury or disease, including renal stones, IGA Nephropathy, abnormal bladder, urinary infections, urinary reflux, and ureteral reimplantation.
- History or persistence of metabolic disorders, gastroesophageal reflux disease, gastrointestinal disorders.
- History or persistence of respiratory diseases including asthma, wheezing, and allergies.
- Hepatic diseases or impaired hepatic function detected in medical reports or a medical examination.
- BMI in underweight (<18.5 kg/m2), overweight (23–24.9 kg/m2) and obese (>25 kg/m2) ranges [18].
- Elevated ACR (>30 mg/g) in the urine samples collected within the present study.
2.2. Sample and Data Management
2.3. Assessment of Renal Biomarkers
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
Reference Intervals
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saran, R.; Hedgeman, E.; Huseini, M.; Stack, A.; Shahinian, V. Surveillance of Chronic Kidney Disease around the World: Tracking and Reining in a Global Problem. Adv. Chronic Kidney Dis. 2010, 17, 271–281. [Google Scholar] [CrossRef]
- Nugent, R.A.; Fathima, S.F.; Feigl, A.B.; Chyung, D. The Burden of Chronic Kidney Disease on Developing Nations: A 21st Century Challenge in Global Health. Nephron. Clin. Pract. 2011, 118, c269–c277. [Google Scholar] [CrossRef]
- Campese, V.M. The Unresolved Epidemic of Chronic Kidney Disease of Uncertain Origin (CKDu) around the World: A Review and New Insights. Clin. Nephrol. 2021, 95, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Gunasekara, T.D.K.S.C.; De Silva, P.M.C.S.; Herath, C.; Siribaddana, S.; Siribaddana, N.; Jayasumana, C.; Jayasinghe, S.; Cardenas-Gonzalez, M.; Jayasundara, N. The Utility of Novel Renal Biomarkers in Assessment of Chronic Kidney Disease of Unknown Etiology (CKDu): A Review. Int. J. Environ. Res. Public Health 2020, 17, 9522. [Google Scholar] [CrossRef] [PubMed]
- Babich, R.; Ulrich, J.C.; Ekanayake, E.M.D.V.; Massarsky, A.; De Silva, P.M.C.S.; Manage, P.M.; Jackson, B.P.; Ferguson, P.L.; Di Giulio, R.T.; Drummond, I.A.; et al. Kidney Developmental Effects of Metal-Herbicide Mixtures: Implications for Chronic Kidney Disease of Unknown Etiology. Environ. Int. 2020, 144, 106019. [Google Scholar] [CrossRef]
- Agampodi, S.B.; Amarasinghe, G.S.; Naotunna, P.G.C.R.; Jayasumana, C.S.; Siribaddana, S.H. Early Renal Damage among Children Living in the Region of Highest Burden of Chronic Kidney Disease of Unknown Etiology (CKDu) in Sri Lanka. BMC Nephrol. 2018, 19, 115. [Google Scholar] [CrossRef] [Green Version]
- Moranne, O.; Froissart, M.; Rossert, J.; Gauci, C.; Boffa, J.-J.; Haymann, J.P.; M’rad, M.B.; Jacquot, C.; Houillier, P.; Stengel, B.; et al. Timing of Onset of CKD-Related Metabolic Complications. J. Am. Soc. Nephrol. 2009, 20, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Lameire, N.H.; Bagga, A.; Cruz, D.; De Maeseneer, J.; Endre, Z.; Kellum, J.A.; Liu, K.D.; Mehta, R.L.; Pannu, N.; Van Biesen, W.; et al. Acute Kidney Injury: An Increasing Global Concern. Lancet 2013, 382, 170–179. [Google Scholar] [CrossRef]
- Mehta, R.L.; Cerdá, J.; Burdmann, E.A.; Tonelli, M.; García-García, G.; Jha, V.; Susantitaphong, P.; Rocco, M.; Vanholder, R.; Sever, M.S.; et al. International Society of Nephrology’s 0by25 Initiative for Acute Kidney Injury (Zero Preventable Deaths by 2025): A Human Rights Case for Nephrology. Lancet 2015, 385, 2616–2643. [Google Scholar] [CrossRef]
- Goyal, A.; Daneshpajouhnejad, P.; Hashmi, M.F.; Bashir, K. Acute Kidney Injury. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Isakova, T.; Nickolas, T.L.; Denburg, M.; Yarlagadda, S.; Weiner, D.E.; Gutiérrez, O.M.; Bansal, V.; Rosas, S.E.; Nigwekar, S.; Yee, J.; et al. KDOQI US Commentary on the 2017 KDIGO Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Am. J. Kidney Dis. 2017, 70, 737–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Askenazi, D.J.; Ambalavanan, N.; Goldstein, S.L. Acute Kidney Injury in Critically Ill Newborns: What Do We Know? What Do We Need to Learn? Pediatr. Nephrol. 2009, 24, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Waikar, S.S.; Bonventre, J.V. Creatinine Kinetics and the Definition of Acute Kidney Injury. J. Am. Soc. Nephrol. 2009, 20, 672–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Letellier, G.; Desjarlais, F. Analytical Interference of Drugs in Clinical Chemistry: II--The Interference of Three Cephalosporins with the Determination of Serum Creatinine Concentration by the Jaffé Reaction. Clin. Biochem. 1985, 18, 352–356. [Google Scholar] [CrossRef]
- Weber, J.A.; van Zanten, A.P. Interferences in Current Methods for Measurements of Creatinine. Clin. Chem. 1991, 37, 695–700. [Google Scholar] [CrossRef]
- Kashani, K.; Cheungpasitporn, W.; Ronco, C. Biomarkers of Acute Kidney Injury: The Pathway from Discovery to Clinical Adoption. Clin. Chem. Lab. Med. 2017, 55, 1074–1089. [Google Scholar] [CrossRef]
- List of Qualified Biomarkers|FDA. Available online: https://www.fda.gov/drugs/biomarker-qualification-program/list-qualified-biomarkers (accessed on 23 June 2021).
- Lim, J.U.; Lee, J.H.; Kim, J.S.; Hwang, Y.I.; Kim, T.-H.; Lim, S.Y.; Yoo, K.H.; Jung, K.-S.; Kim, Y.K.; Rhee, C.K. Comparison of World Health Organization and Asia-Pacific Body Mass Index Classifications in COPD Patients. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 2465–2475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, M.R.; Nehus, E.; Haffner, C.; Ma, Q.; Devarajan, P. Pediatric Reference Ranges for Acute Kidney Injury Biomarkers. Pediatr. Nephrol. 2015, 30, 677–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamianowska, M.; Szczepański, M.; Kulikowska, E.E.; Bebko, B.; Wasilewska, A. Do Serum and Urinary Concentrations of Kidney Injury Molecule-1 in Healthy Newborns Depend on Birth Weight, Gestational Age or Gender? J. Perinatol. 2017, 37, 73–76. [Google Scholar] [CrossRef]
- McWilliam, S.J.; Antoine, D.J.; Sabbisetti, V.; Pearce, R.E.; Jorgensen, A.L.; Lin, Y.; Leeder, J.S.; Bonventre, J.V.; Smyth, R.L.; Pirmohamed, M. Reference Intervals for Urinary Renal Injury Biomarkers KIM-1 and NGAL in Healthy Children. Biomark. Med. 2014, 8, 1189–1197. [Google Scholar] [CrossRef] [Green Version]
- Hyltoft Petersen, P.; Rustad, P. Prerequisites for Establishing Common Reference Intervals. Scand. J. Clin. Lab. Invest. 2004, 64, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Leibler, J.H.; Ramirez-Rubio, O.; Velázquez, J.J.A.; Pilarte, D.L.; Obeid, W.; Parikh, C.R.; Gadupudi, S.; Scammell, M.K.; Friedman, D.J.; Brooks, D.R. Biomarkers of Kidney Injury among Children in a High-Risk Region for Chronic Kidney Disease of Uncertain Etiology. Pediatr. Nephrol. 2021, 36, 387–396. [Google Scholar] [CrossRef]
- Ramírez-Rubio, O.; Amador, J.J.; Kaufman, J.S.; Weiner, D.E.; Parikh, C.R.; Khan, U.; McClean, M.D.; Laws, R.L.; López-Pilarte, D.; Friedman, D.J.; et al. Urine Biomarkers of Kidney Injury among Adolescents in Nicaragua, a Region Affected by an Epidemic of Chronic Kidney Disease of Unknown Aetiology. Nephrol. Dial. Transplant. 2016, 31, 424–432. [Google Scholar] [CrossRef] [Green Version]
- De Silva, P.M.C.S.; Mohammed Abdul, K.S.; Eakanayake, E.M.D.V.; Jayasinghe, S.S.; Jayasumana, C.; Asanthi, H.B.; Perera, H.S.D.; Chaminda, G.G.T.; Chandana, E.P.S.; Siribaddana, S.H. Urinary Biomarkers KIM-1 and NGAL for Detection of Chronic Kidney Disease of Uncertain Etiology (CKDu) among Agricultural Communities in Sri Lanka. PLoS Negl. Trop. Dis. 2016, 10, e0004979. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
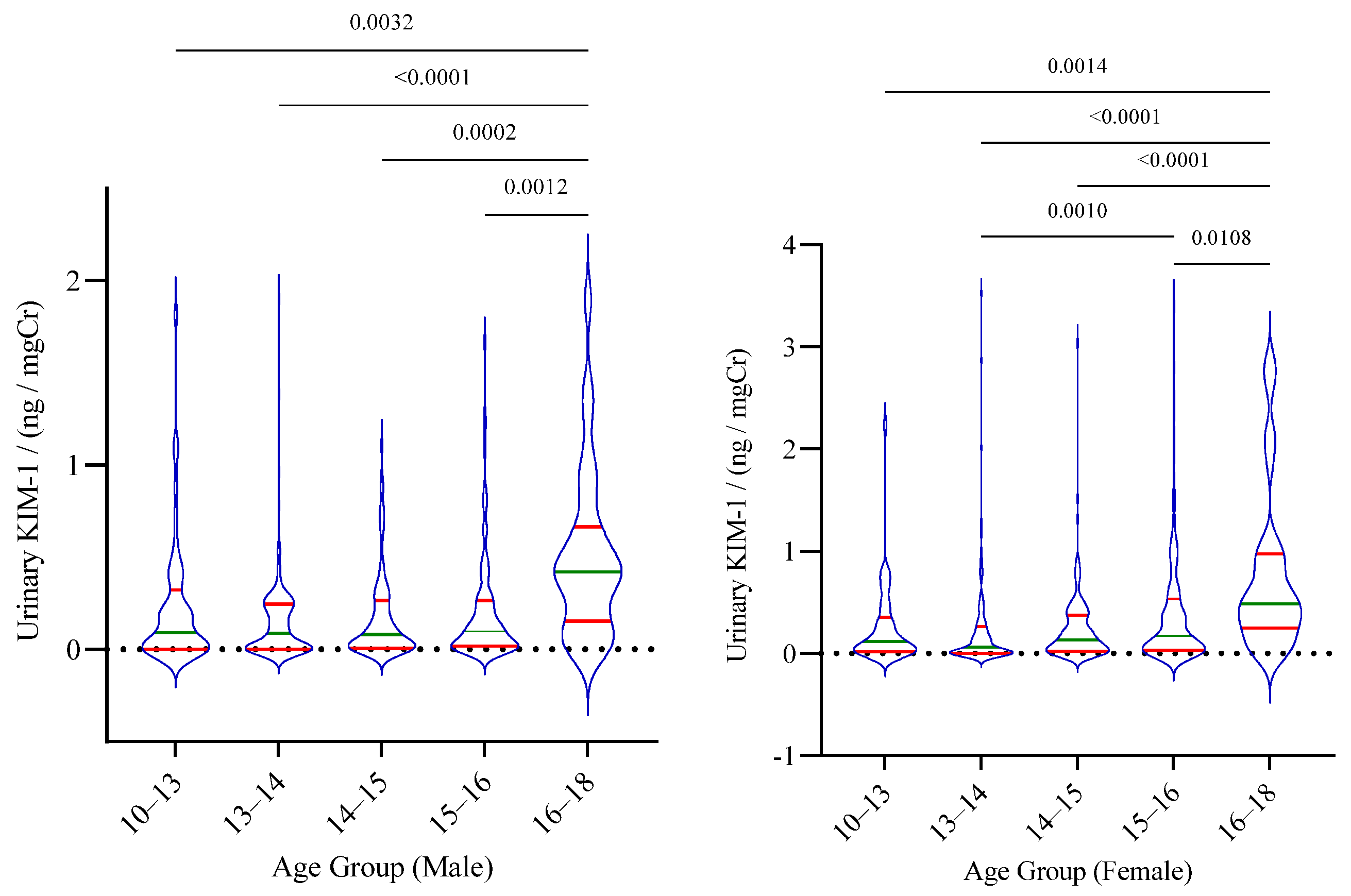
| Age Group/Years | Urinary KIM-1 Concentration/(ng/mg Cr) | CI:RI Ratio | ||
|---|---|---|---|---|
| 2.5th Quantile (90% CI) | 50th Quantile (90% CI) | 97.5th Quantile (90% CI) | ||
| Male (N = 425) | ||||
| 10–13 (N = 50) | 0.0008 (0.0003–0.0012) | 0.0966 (0–0.1999) | 1.1220 (0.3204–1.9236) | 1.4289 |
| 13–14 (N = 123) | 0.0005 0.0003–0.0007) | 0.0939 (0.0290–0.1589) | 0.7818 (0.3021–1.2616) | 1.2272 |
| 14–15 (N = 112) | 0.0005 (0.0003–0.0006) | 0.0800 (0.0343–0.1258) | 0.8813 (0.7267–1.0359) | 0.3500 |
| 15–16 (N = 109) | 0.0005 (0.0002–0.0007) | 0.0984 (0.0558–0.1411) | 1.1915 (0.8019–1.5811) | 0.6539 |
| 16–18 (N = 31) | 0.0009 (0–0.0367) | 0.4262 (0.3534–0.4991) | 1.8930 (1.3911–2.3949) | 0.5303 |
| Female (N =484) | ||||
| 10–13 (N = 44) | 0.0010 (0.0001–0.0019) | 0.1188 (0–0.2625) | 0.8253 (0–2.2014) | 1.9990 |
| 13–14 (N = 127) | 0.0006 (0.0005–0.0007) | 0.0781 (0.0244–0.1319) | 1.2904 (0.5197–2.0611) | 1.1945 |
| 14–15 (N = 142) | 0.0005 (0.0003–0.0006) | 0.1395 (0.0868–0.1921) | 0.9105 (0–1.9010) | 2.0000 |
| 15–16 (N = 131) | 0.0009 (0.0006–0.0013) | 0.1737 (0.1188–0.2286) | 2.3671 (1.4606–3.2735) | 0.7659 |
| 16–18 (N = 40) | 0.0008 (0–0.0792) | 0.5076 (0.3751–0.6401) | 2.8650 (2.6851–3.0450) | 0.1256 |
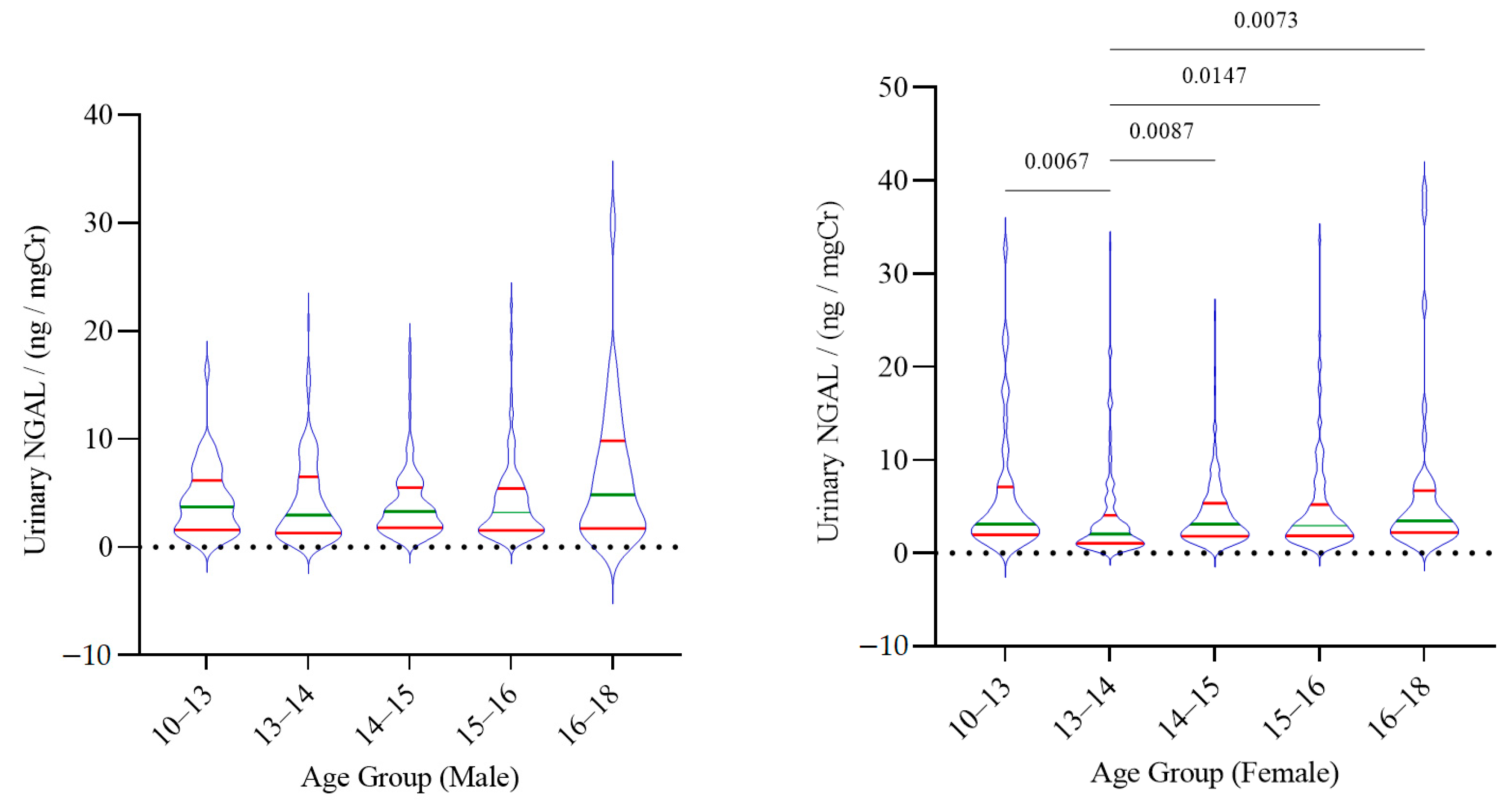
| Age Group/Years | Urinary NGAL Concentration/(ng/mg Cr) | CI:RI Ratio | ||
|---|---|---|---|---|
| 2.5th Quantile (90% CI) | 50th Quantile (90% CI) | 97.5th Quantile (90% CI) | ||
| Male (N = 425) | ||||
| 10–13 (N = 50) | 0.4420 (0.0758–0.8082) | 3.7475 (2.8171–4.6779) | 9.6458 (5.3693–13.9223) | 1.4433 |
| 13–14 (N = 123) | 0.4240 (0.2728–0.5752) | 2.9659 (2.1162–3.8155) | 15.3648 (10.3116–20.4180) | 1.3289 |
| 14–15 (N = 112) | 0.6478 (0.4573–0.8383) | 3.2992 (2.6910–3.9074) | 15.9261 (10.0773–21.7750) | 1.3672 |
| 15–16 (N = 109) | 0.6895 (0.5671–0.8118) | 3.2780 (2.5590–3.9970) | 17.9484 (10.8294–25.0673) | 1.3966 |
| 16–18 (N = 31) | 0.4393 (0–1.0586) | 4.8512 (1.9920–7.7104) | 30.0482 (17.1954–42.9010) | 1.4278 |
| Female (N = 484) | ||||
| 10–13 (N = 44) | 0.8702 (0.2860–1.4544) | 3.1455 (2.0366–4.2544) | 23.4905 (11.1470–35.8340) | 1.0509 |
| 13–14 (N = 127) | 0.4189 (0.3221–0.5158) | 2.0849 (1.5707–2.5992) | 17.2057 (8.81067–25.6007) | 0.9758 |
| 14–15 (N = 142) | 0.7530 (0.4495–1.0566) | 3.1281 (2.6457–3.6104) | 13.5191 (6.8249–20.2134) | 0.9903 |
| 15–16 (N = 131) | 0.5727 (0.1730–0.9723) | 2.9841 (2.6099–3.3584) | 20.0642 (15.1797–24.9487) | 0.4869 |
| 16–18 (N = 40) | 1.1261 (1.0624–1.1898) | 3.4958 (2.8220–4.1696) | 38.9910 (33.3216–44.6603) | 0.2908 |
| Variable | KIM-1 | NGAL | ||
|---|---|---|---|---|
| rs | p | rs | p | |
| Unpartitioned (Male and Female) | ||||
| Age (years) | 0.185 | <0.0001 | 0.067 | 0.0004 |
| Gender | 0.109 | 0.001 | −0.034 | 0.308 |
| BMI (kg/m2) | 0.01 | 0.782 | 0.043 | 0.222 |
| ACR (mg/g) | 0.044 | 0.193 | 0.094 | 0.005 |
| KIM-1 (ng/mg Cr) | 0.119 | 0.0004 | ||
| Partitioned—Male | ||||
| Age (years) | 0.137 | 0.005 | 0.019 | 0.705 |
| BMI (kg/m2) | −0.09 | 0.081 | 0.004 | 0.94 |
| ACR (mg/g) | 0.034 | 0.484 | 0.091 | 0.062 |
| KIM-1 (ng/mg Cr) | 0.048 | 0.323 | ||
| Partitioned—Female | ||||
| Age (Years) | 0.215 | <0.0001 | 0.116 | 0.012 |
| BMI (kg/m2) | 0.053 | 0.272 | 0.098 | 0.042 |
| ACR (mg/g) | 0.028 | 0.543 | 0.104 | 0.024 |
| KIM-1 (ng/mg Cr) | 0.192 | <0.0001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Silva, P.M.C.S.; Gunasekara, T.D.K.S.C.; Gunarathna, S.D.; Sandamini, P.M.M.A.; Pinipa, R.A.I.; Ekanayake, E.M.D.V.; Thakshila, W.A.K.G.; Jayasinghe, S.S.; Chandana, E.P.S.; Jayasundara, N. Urinary Biomarkers of Renal Injury KIM-1 and NGAL: Reference Intervals for Healthy Pediatric Population in Sri Lanka. Children 2021, 8, 684. https://doi.org/10.3390/children8080684
De Silva PMCS, Gunasekara TDKSC, Gunarathna SD, Sandamini PMMA, Pinipa RAI, Ekanayake EMDV, Thakshila WAKG, Jayasinghe SS, Chandana EPS, Jayasundara N. Urinary Biomarkers of Renal Injury KIM-1 and NGAL: Reference Intervals for Healthy Pediatric Population in Sri Lanka. Children. 2021; 8(8):684. https://doi.org/10.3390/children8080684
Chicago/Turabian StyleDe Silva, P. Mangala C. S., T. D. K. S. C. Gunasekara, S. D. Gunarathna, P. M. M. A. Sandamini, R. A. I. Pinipa, E. M. D. V. Ekanayake, W. A. K. G. Thakshila, S. S. Jayasinghe, E. P. S. Chandana, and Nishad Jayasundara. 2021. "Urinary Biomarkers of Renal Injury KIM-1 and NGAL: Reference Intervals for Healthy Pediatric Population in Sri Lanka" Children 8, no. 8: 684. https://doi.org/10.3390/children8080684
APA StyleDe Silva, P. M. C. S., Gunasekara, T. D. K. S. C., Gunarathna, S. D., Sandamini, P. M. M. A., Pinipa, R. A. I., Ekanayake, E. M. D. V., Thakshila, W. A. K. G., Jayasinghe, S. S., Chandana, E. P. S., & Jayasundara, N. (2021). Urinary Biomarkers of Renal Injury KIM-1 and NGAL: Reference Intervals for Healthy Pediatric Population in Sri Lanka. Children, 8(8), 684. https://doi.org/10.3390/children8080684