
Radial Club Hand Treated by Paley Ulnarization Generation 3: Is This the New Centralization?


Abstract
1. Introduction
2. Materials and Methods
Paley Ulnarization G3 Surgical Technique:
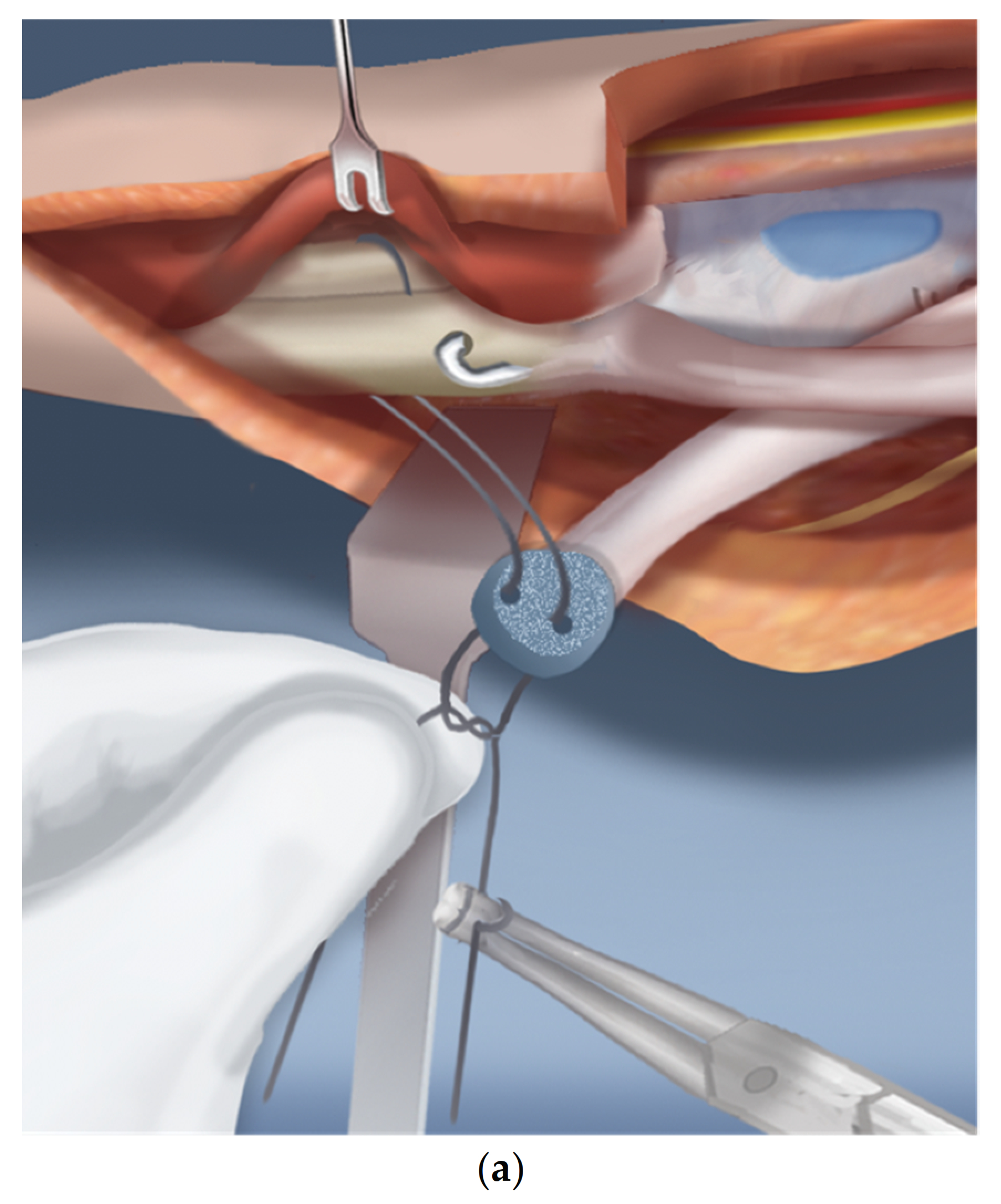
- Step 1.
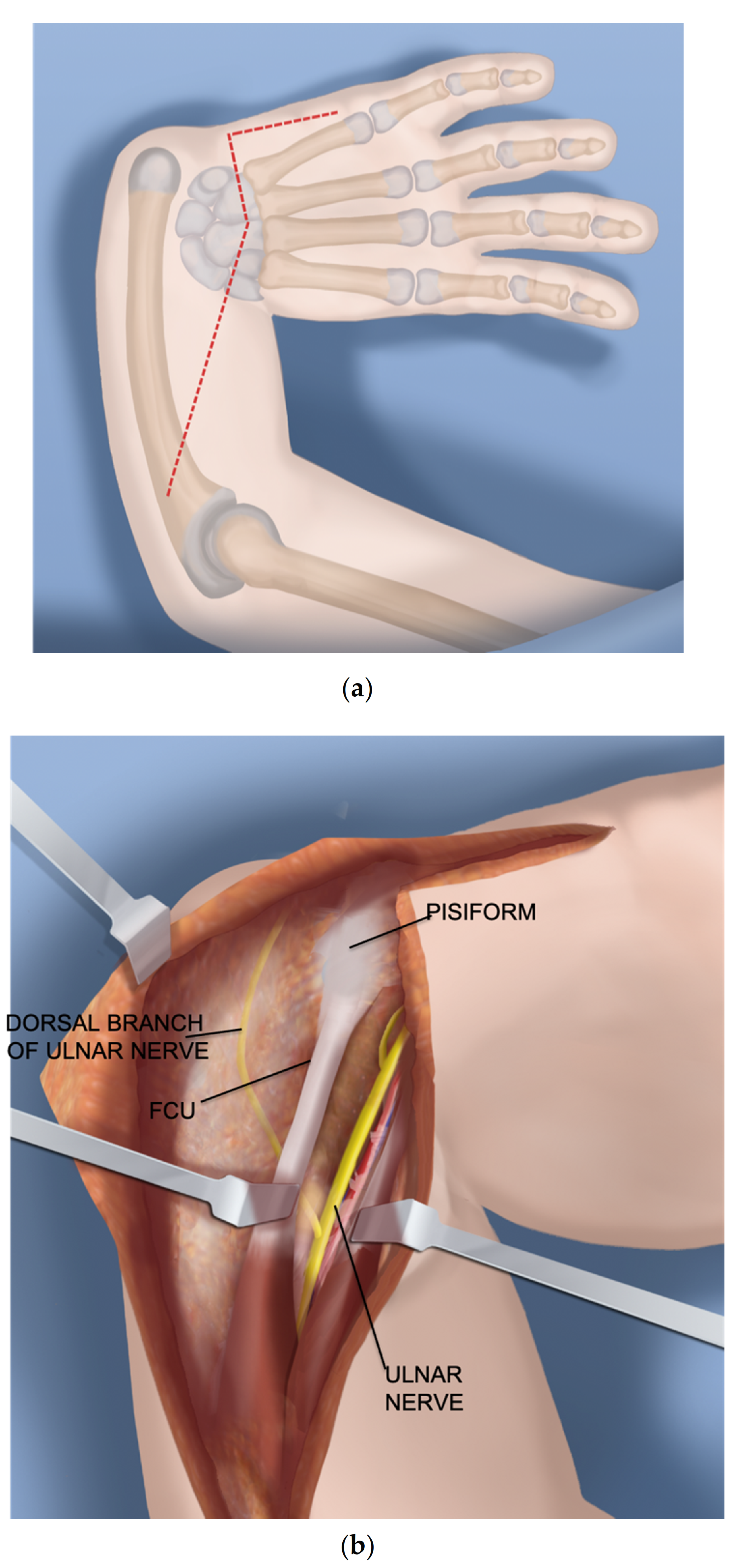
- After a tourniquet is applied to the arm, a volar Z-shaped incision is made. The middle line of the Z is along the wrist flexor crease. The proximal longitudinal incision runs from the midpoint of the wrist crease towards the ulnar border of the forearm. The distal limb is along the ulnar border of the hand (Figure 1a).
- Step 2.
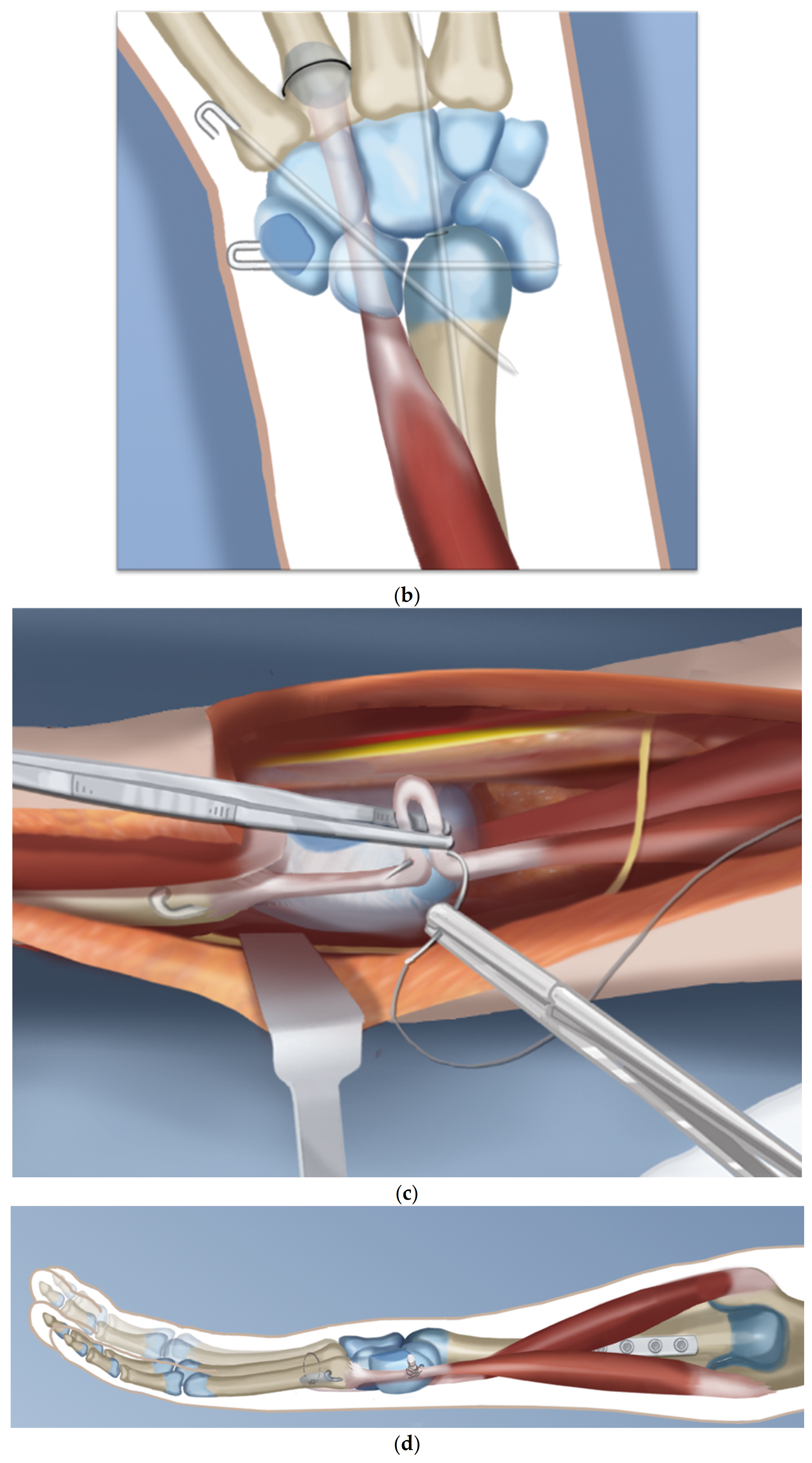
- A volar fasciotomy is performed. The ulnar neuro-vascular bundle is exposed together with the flexor carpi ulnaris (FCU) tendon. Care is taken not to injure the dorsal branch of the ulnar nerve which passes underneath the FCU (Figure 1b).
- Step 3.
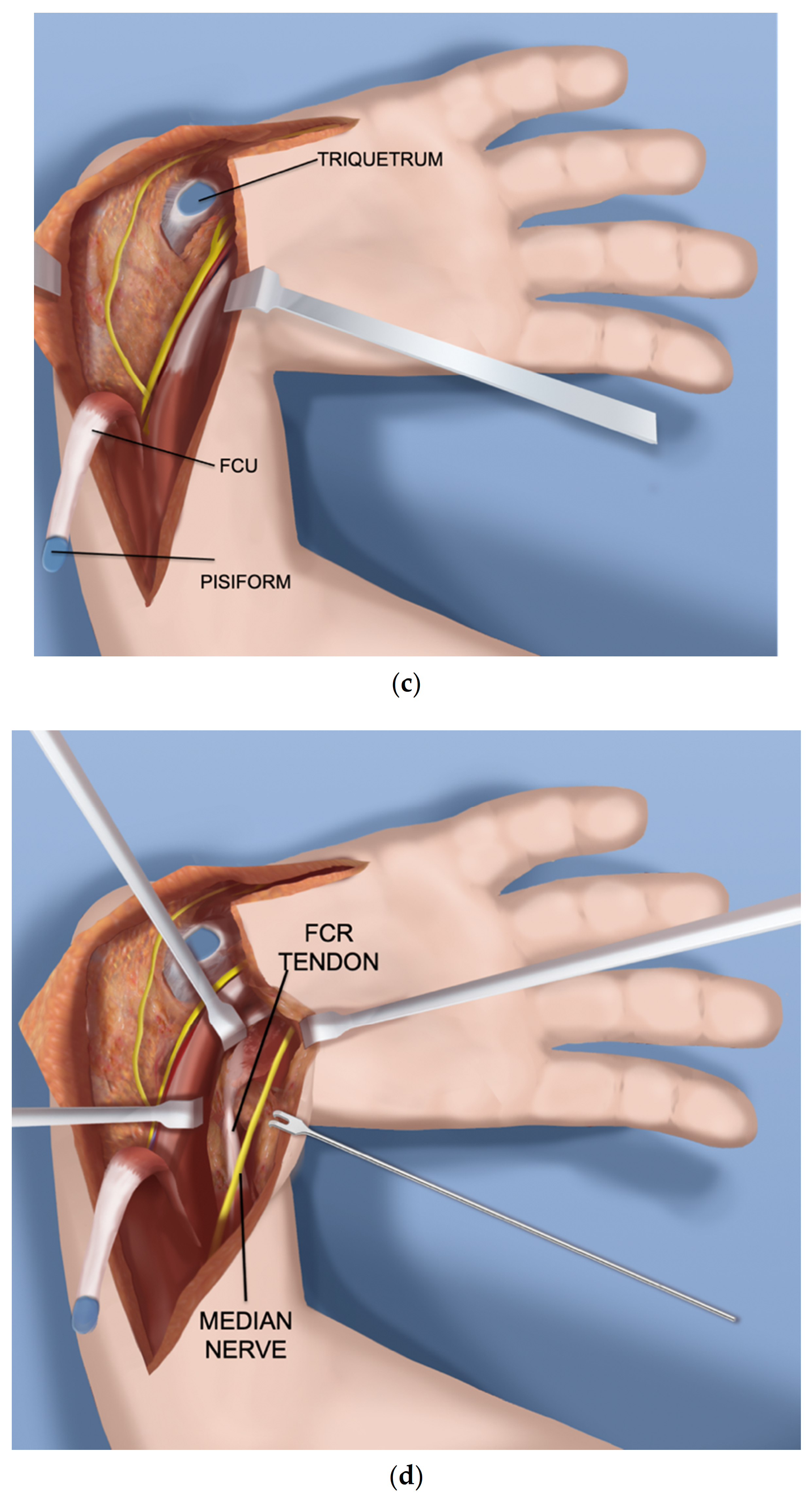
- Decompress the ulnar nerve and the dorsal branch of the ulnar nerve. Detach the pisiform bone from the triquetrum and reflect back the FCU with its muscle (Figure 1c).
- Step 4.
- Expose and decompress the median nerve into the carpal tunnel. Look for an FCR tendon (Figure 1d).
- Step 5.
- Detach the FCR from the carpus. In a TAR syndrome with weak thumb extension, transfer it to the EPL (extensor pollicis longus) or EPB (extensor pollicis brevis) (Figure 1e).
- Step 6.
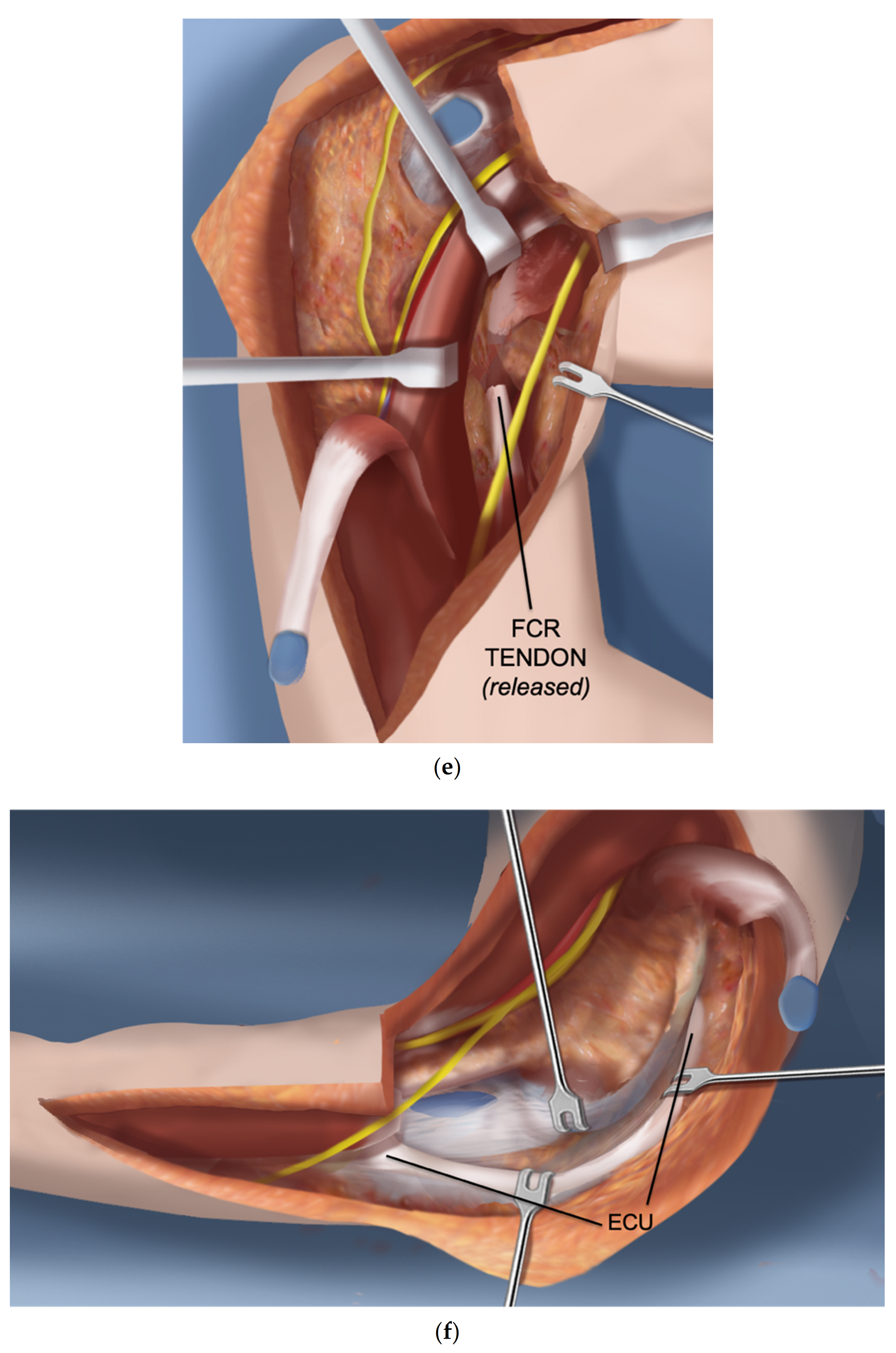
- On the ulnar side dissect the ECU (extensor carpi ulnaris) free of the ulna to its insertion (Figure 1f).
- Step 7.
- Find the EDM (extensor digiti minimi) on the dorsum of the ulna and free it up proximally and distally (Figure 1g).
- Step 8.
- The ulno-carpal capsule is cut laterally. The dissecting scissors are oriented from the distal to proximal end along the shaft of the ulna. The natural tendency is to dissect from the ulnar to the radial cutting across the lunate. The exposed triquetral side of the piso-triquetral joint helps to orient the anatomy (Figure 1h).
- Step 9.
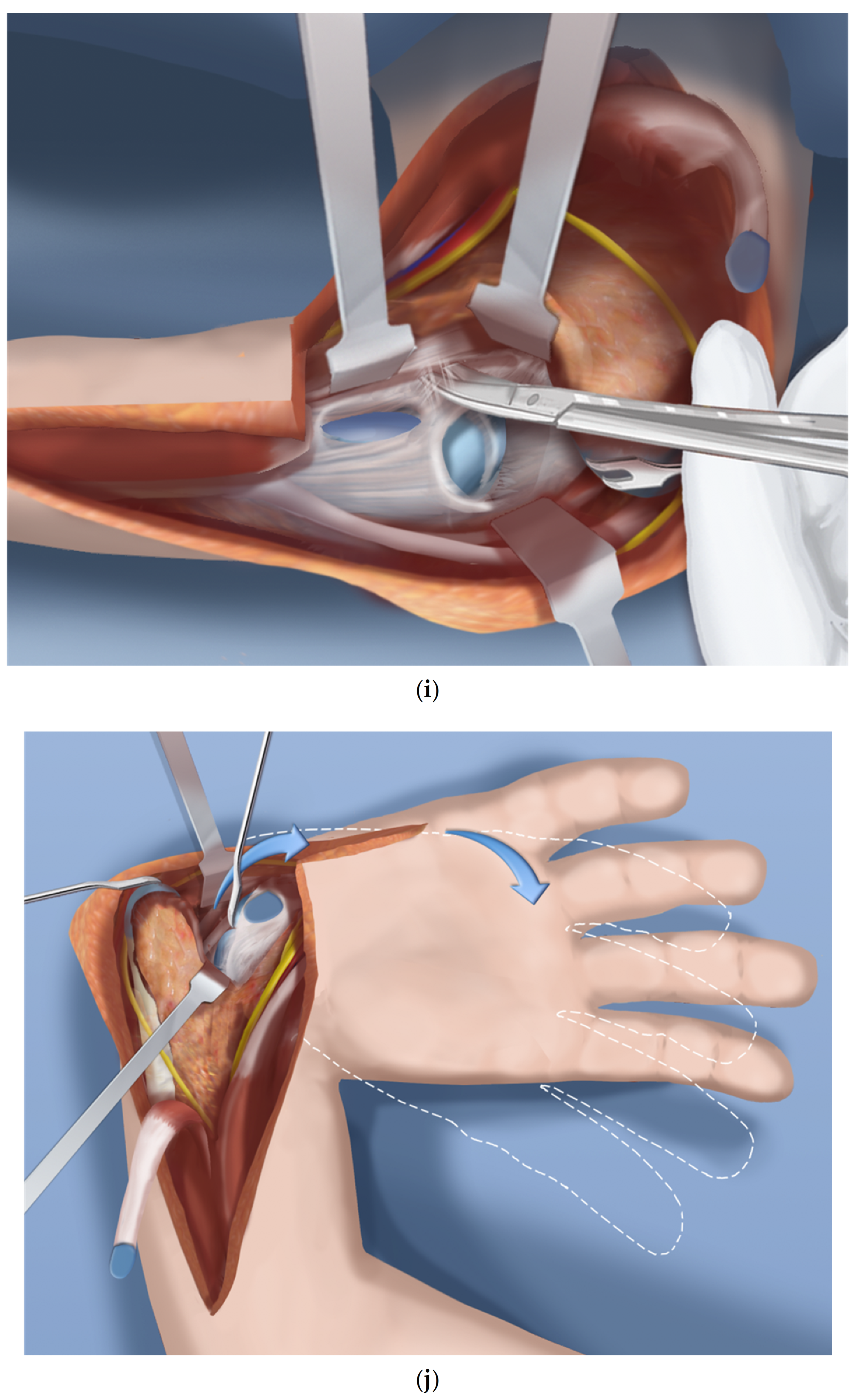
- It is important to preserve the volar soft tissues anterior and radial to the head of the ulna. A retractor is placed there to protect these tissues that contain the caput ulnar vessels. The capsulotomy is continued in a radial direction on the carpal side (Figure 1i).
- Step 10.
- The volar soft tissue pedicle must be protected at all times during the ulno-carpal capsulotomy (Figure 1j).
- Step 11.
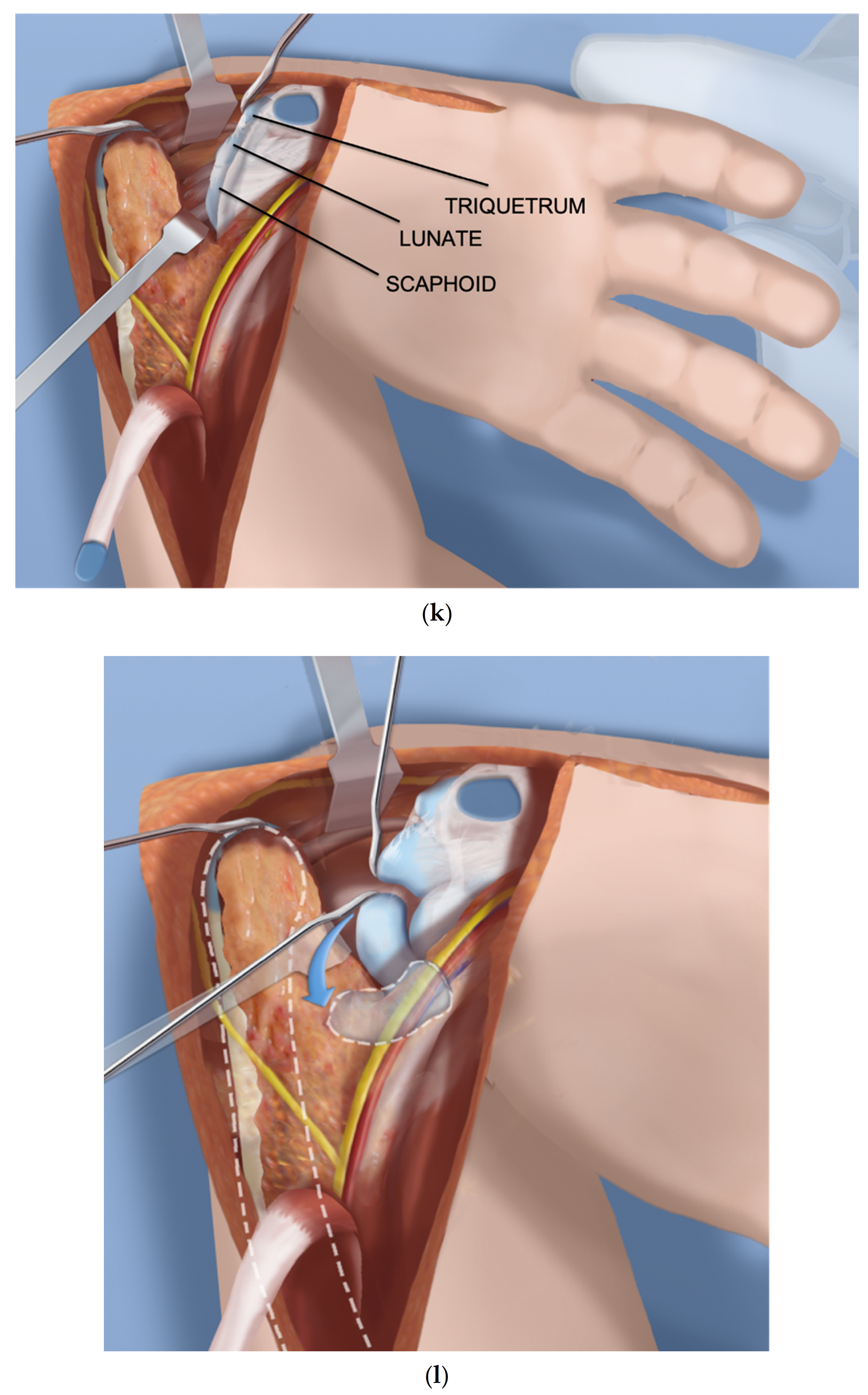
- The carpal bones are released from their capsular connections while preserving the volar flap (Figure 1k).
- Step 12.
- Once the scaphoid is reached, the scapholunate ligaments are released from and the scaphoid is flapped open (Figure 1l).
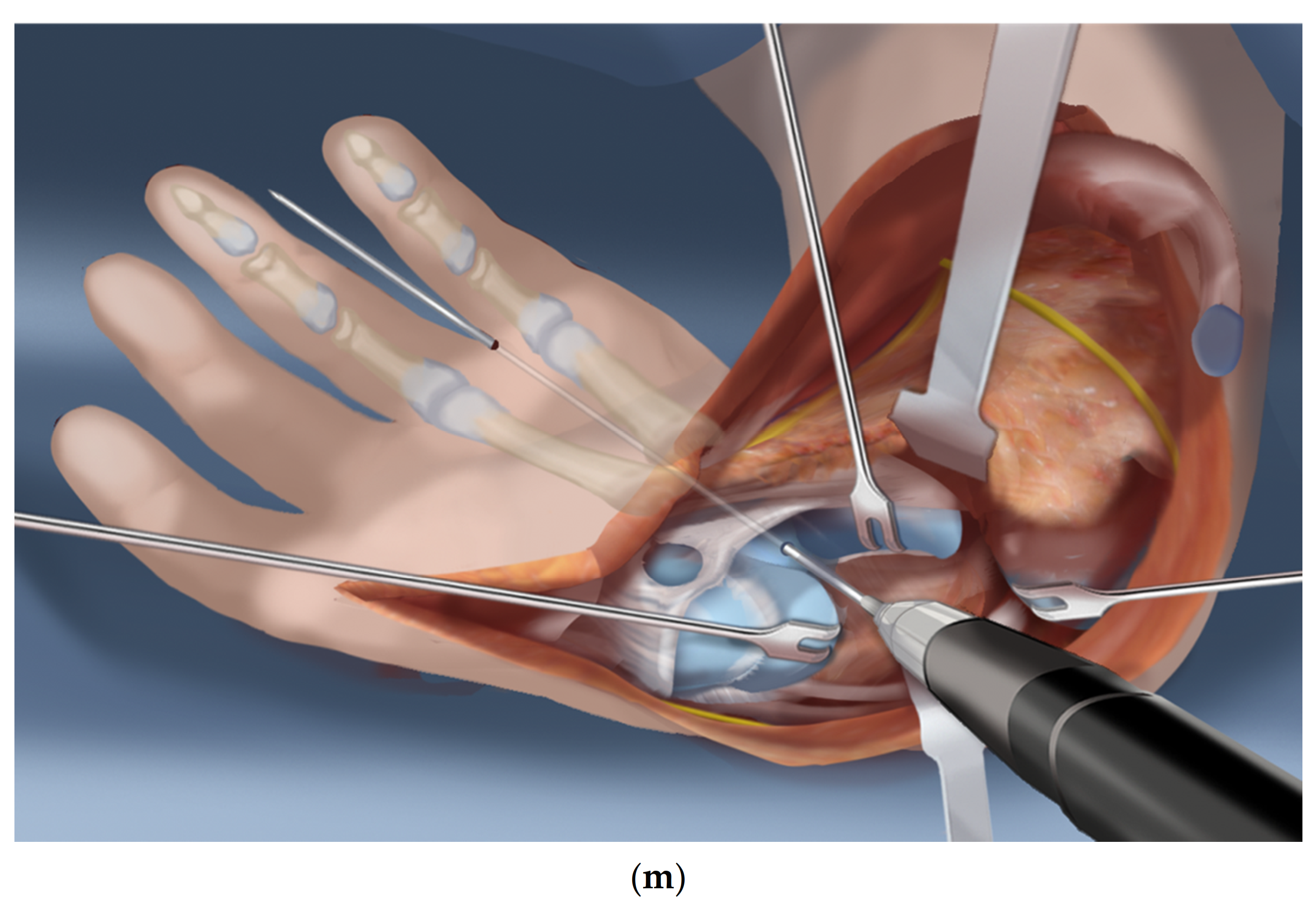
- Step 13.
- Insert a 1.5 mm wire through the distal row of the carpus after flapping back the scaphoid. This wire exits between the index and middle fingers (Figure 1m).
- Step 14.
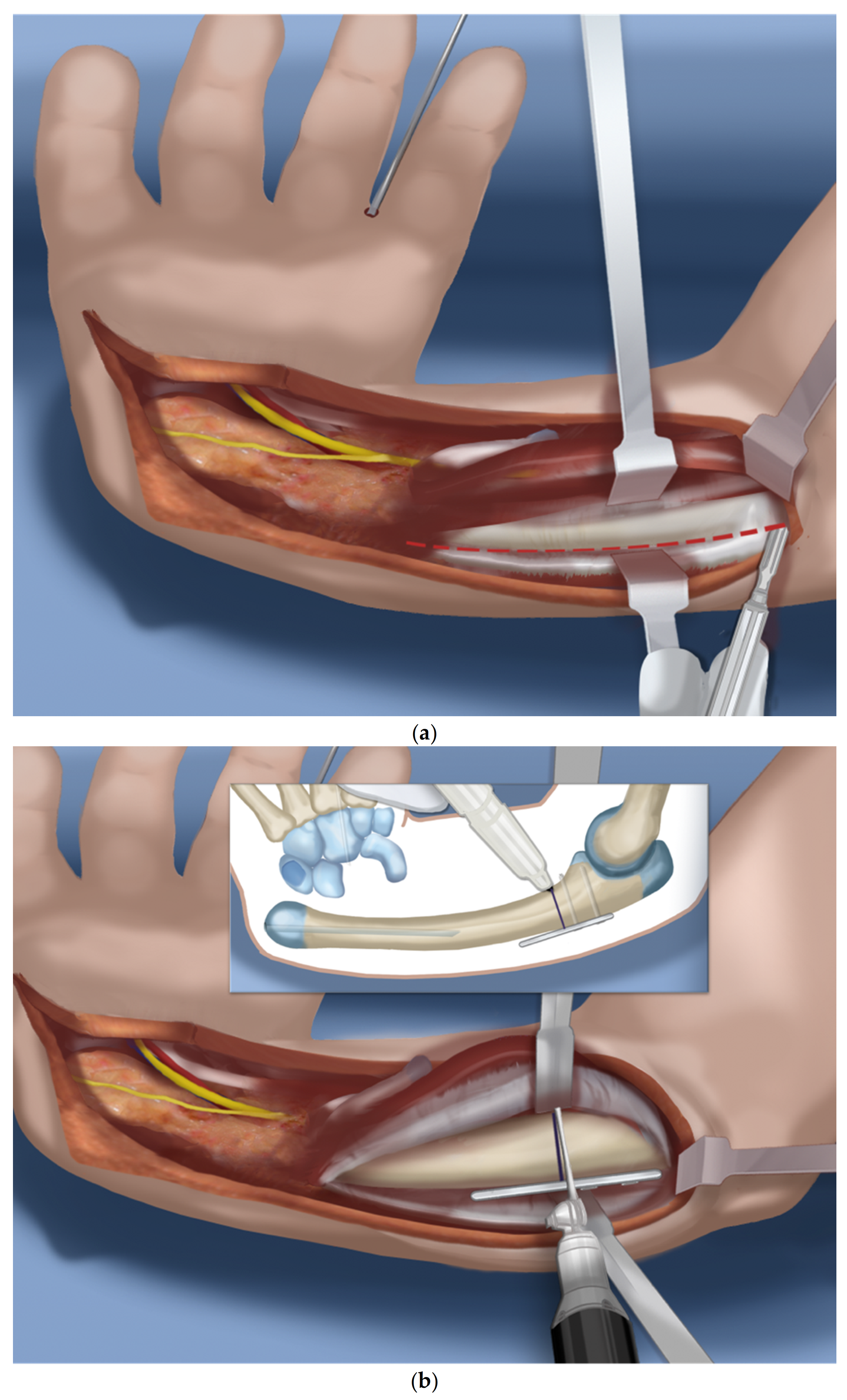
- Expose the proximal shaft of the ulna subperiosteally (Figure 2a).
- Step 15.
- Apply a 4-hole locking plate by affixing it with two locking screws to the ulna just proximal to the planned level of the osteotomy and mark the osteotomy level distal to the screws. Predrill the end of the ulna with a 1.8 mm wire to make it easier to pin the hand to the ulna in Step 17 (Figure 2b).
- Step 16.
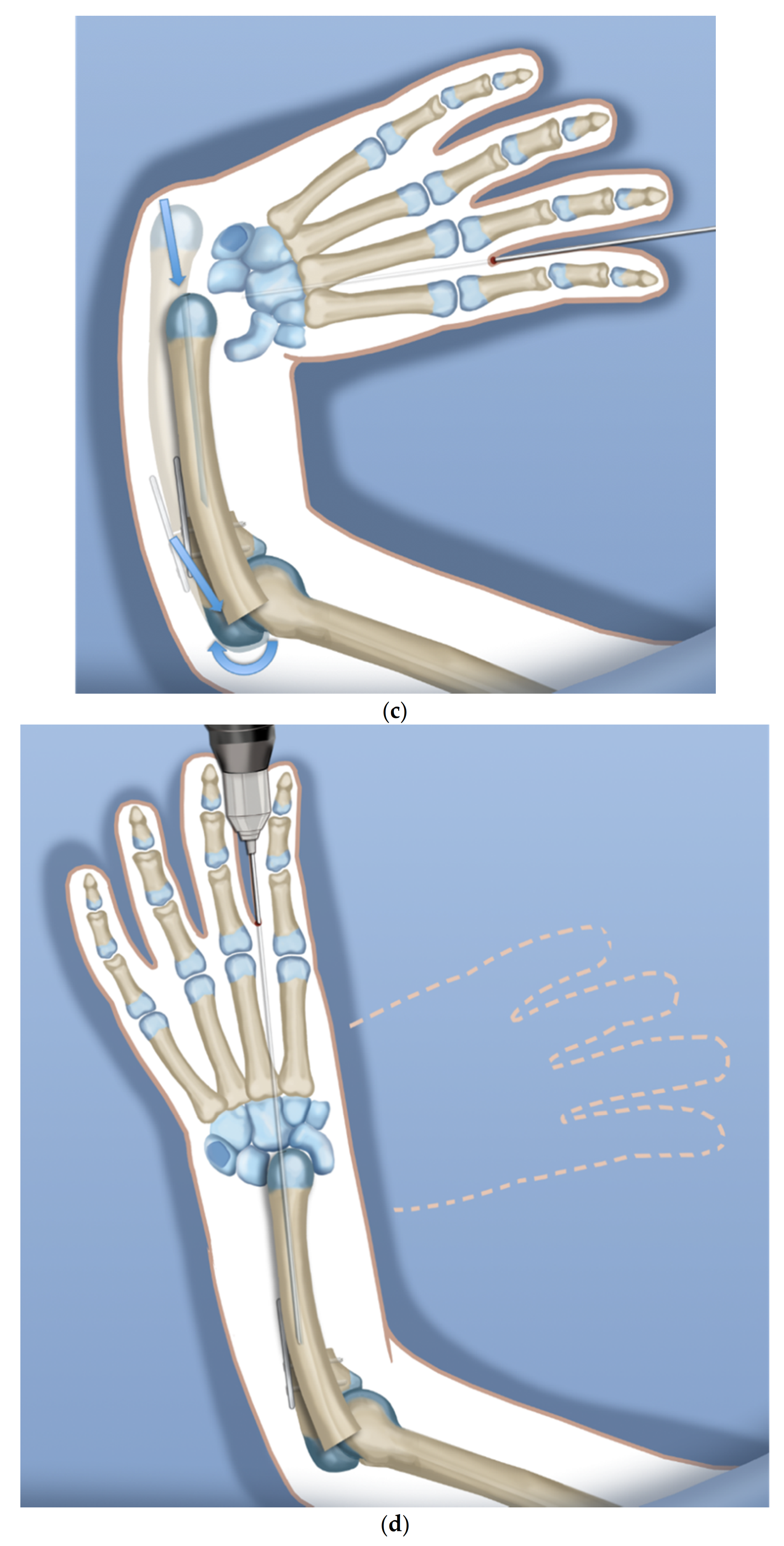
- After the osteotomy, shorten the ulna and overlap the bone ends. This brings the head of the ulna to the level of the diastasis created between the lunate and the scaphoid (Figure 2c).
- Step 17.
- Advance the wire in the hand into the hole created in the head of the ulna and part way down the shaft of the ulna (Figure 2d).
- Step 18.
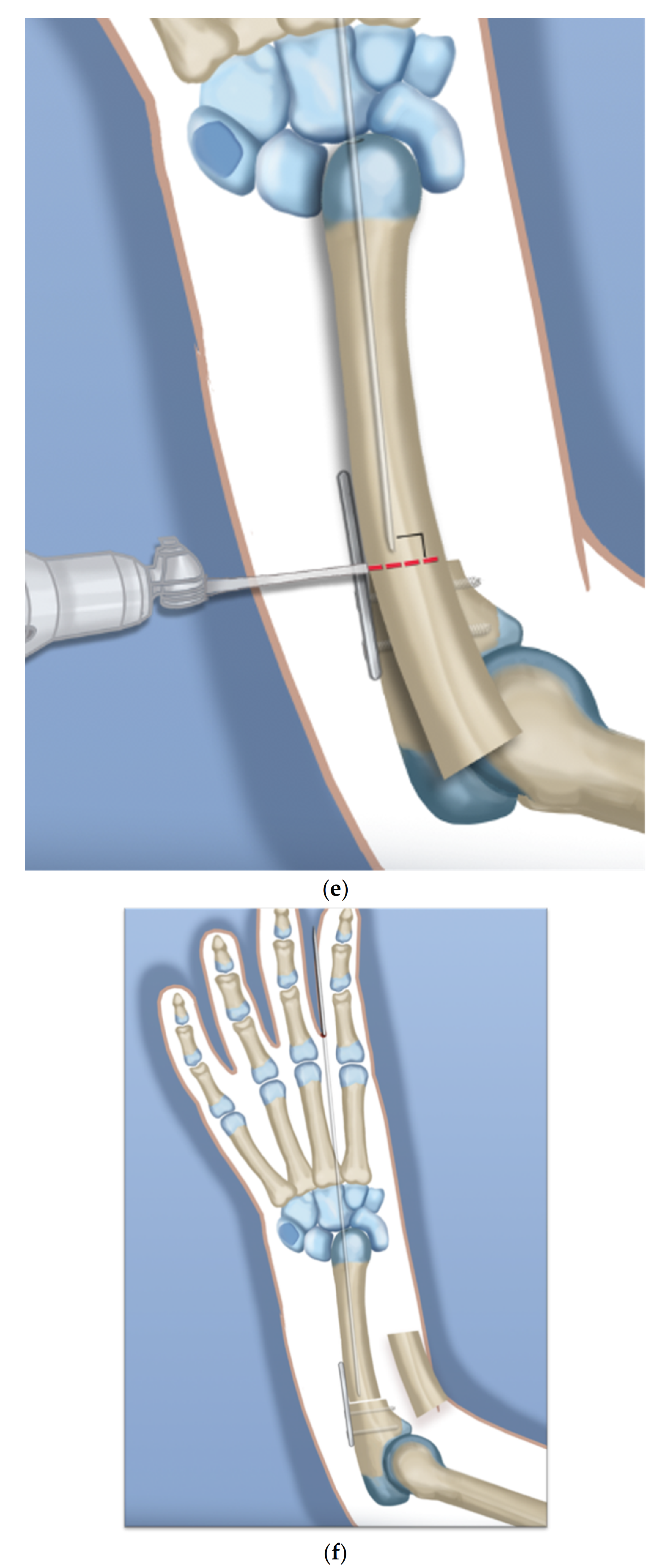
- Mark the level of overlap and perform an osteotomy for shortening of the ulna (Figure 2e,f).
- Step 19.
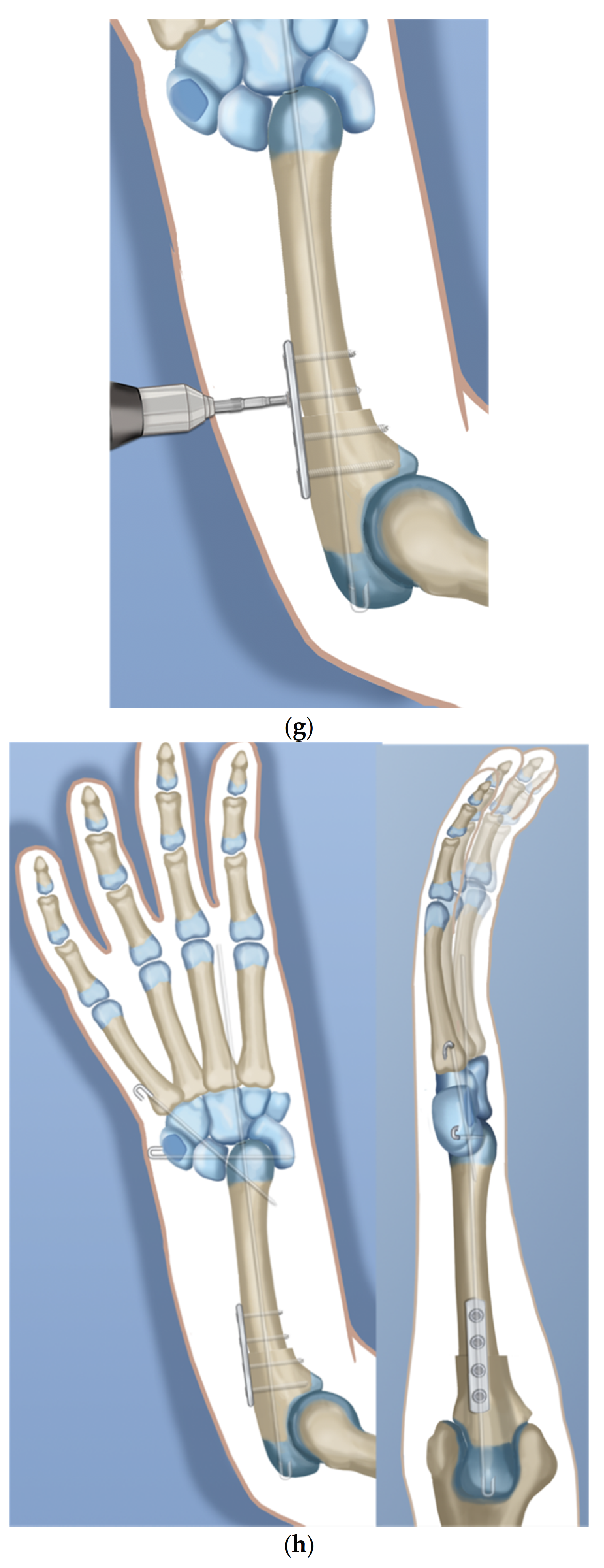
- Advance the ulnar wire across the osteotomy and out the olecranon. Adjust it at the wrist and then cut and bend this wire and bury under the skin. Complete the plate fixation by insertion of the two distal locking screws (Figure 2g).
- Step 20.
- Pin the carpus to the head of the ulna with the plane of the hand in mid pronation-supination using two additional 1.5 mm wires, one transverse and one oblique. Cut and curl the near end of the wires and bury under the skin (Figure 2h).
- Step 21.
- Use a 15 blade to remove the articular surface of the pisiform. Pass the FCU tendon deep to the ECU and EDM and the dorsal cutaneous branch of the ulnar nerve. Pass a 2-0 non-absorbable suture from dorsal to volar through the pisiform. Pass the needle through the interspace between the 3rd and 4th metacarpal bases from dorsal to volar. Then, re-pass the same needle from volar to dorsal between the 4th to 5th metacarpal bases. Pass the needle through the pisiform from volar to dorsal. Secure the pisiform down to the bone by tying the suture (Figure 3a,b).
- Step 22.
- Imbricate the ECU tendon with non-absorbable sutures (Figure 3c,d).
- Step 23.
- Extend the volar fasciotomy of the forearm proximally.
- Step 24.
- The tourniquet is let down. After achieving hemostasis, close the wound over a drain. Excess skin folds on the ulnar side should be resected.
- Step 25.
- A custom molded splint either from cast material or orthoplasty is made in the operating room. The above elbow splint should leave the fingers free to move.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goldfarb, C.A.; Wall, L.B.; Bohn, D.; Moen, P.; Van Heest, A. Epidemiology of Congenital Upper Limb Anomalies in a Midwest United States Population: An Assessment Using the Oberg, Manske, and Tonkin Classification. J. Hand Surg. 2015, 40, 127–132.e2. [Google Scholar] [CrossRef] [PubMed]
- Ekblom, A.G.; Laurell, T.; Arner, M. Epidemiology of Congenital Upper Limb Anomalies in Stockholm, Sweden, 1997 to 2007: Application of the Oberg, Manske, and Tonkin Classification. J. Hand Surg. 2014, 39, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.H.; Baek, G.H.; Kim, Y.-J.; Kim, M.-J.; Kim, J.K. Epidemiology of congenital upper limb anomalies in Korea: A nationwide population-based study. PLoS ONE 2021, 16, e0248105. [Google Scholar] [CrossRef] [PubMed]
- James, M.; McCarroll, H.; Manske, P.R. The spectrum of radial longitudinal deficiency: A modified classification. J. Hand Surg. 1999, 24, 1145–1155. [Google Scholar] [CrossRef]
- Khalid, S.; Faizan, M.; Alam, M.; Hassan, F.; Zaheer, S.; Khalid, M. Congenital Longitudinal Radial Deficiency in Infants: Spectrum of Isolated Cases to VACTERL Syndrome. J. Clin. Neonatol. 2013, 2, 193–195. [Google Scholar] [CrossRef]
- Koskimies, E.; Lindfors, N.; Gissler, M.; Peltonen, J.; Nietosvaara, Y. Congenital Upper Limb Deficiencies and Associated Malformations in Finland: A Population-Based Study. J. Hand Surg. 2011, 36, 1058–1065. [Google Scholar] [CrossRef]
- Giele, H.; Giele, C.; Bower, C.; Allison, M. The incidence and epidemiology of congenital upper limb anomalies: A total population study. J. Hand Surg. 2001, 26, 628–634. [Google Scholar] [CrossRef]
- Lourie, G.M.; Lins, R.E. Radial Longitudinal Deficiency. Hand Clin. 1998, 14, 85–99. [Google Scholar] [CrossRef]
- Heikel, H.V. Aplasia and Hypoplasa of the Radius: Studies on 64 Cases and on Epiphyseal Transplantation in Rabbits with the Imitated Defect. Acta Orthop. Scand Suppl. 1959, 39, 1–155. [Google Scholar]
- Wall, L.B.; Kim, D.J.; Cogsil, T.; Goldfarb, C.A. Treatment of Radial Longitudinal Deficiency: An International Survey. J. Hand Surg. 2021, 46, 241.e1–241.e11. [Google Scholar] [CrossRef]
- Murphy, G.R.F.; Logan, M.P.O.; Smith, G.; Sivakumar, B.; Smith, P. Correction of “Wrist” Deformity in Radial Dysplasia: A Systematic Review and Meta-Analysis. J. Bone Joint Surg. Am. 2017, 99, 2120–2126. [Google Scholar] [CrossRef]
- McCarthy, J.J.; Kozin, S.H.; Tuohy, C.; Cheung, E.; Davidson, R.S.; Noonan, K. External Fixation and Centralization Versus External Fixation and Ulnar Osteotomy: The Treatment of Radial Dysplasia Using the Resolved Total Angle of Deformity. J. Pediatr. Orthop. 2009, 29, 797–803. [Google Scholar] [CrossRef]
- Buck-Gramcko, D. Radialization as a new treatment for radial club hand. J. Hand Surg. 1985, 10, 964–968. [Google Scholar] [CrossRef]
- Buck-Gramcko, D. Radialization for Radial Club Hand. Tech. Hand Up. Extremity Surg. 1999, 3, 2–12. [Google Scholar] [CrossRef]
- Paley, D.; Belthur, M.; Standard, S. Ulnarization for the Treatment of Radial Clubhand. In Proceedings of the American Academy of Orthopedic Surgeons 75th Annual Meeting, San Francisco, CA, USA, 5–9 March 2008. [Google Scholar]
- Paley, D.; Robbins, C.A. Ulnarization as Treatment for Radial Clubhand (RCH). In Limb Lengthening and Reconstruction Surgery Case Atlas: Pediatric Deformities; Rozbruch, S.R., Hamdy, R., Eds.; Springer International Publishing: Cham, Switzerlands, 2015; pp. 1–11. [Google Scholar]
- Paley, D. The Paley ulnarization of the carpus with ulnar shortening osteotomy for treatment of radial club hand. SICOT-J 2017, 3, 5. [Google Scholar] [CrossRef]
- Paley, D.; Herzenberg, J. Distraction treatment of congenital and developmental deformities of the foot and hand. In Congenital Malformations of the Hand and Forearm; Buck-Gramcko, D., Ed.; Churchill Livingstone: London, UK, 1998; p. 73117. [Google Scholar]
- Manske, P.R.; McCarroll, H.R.; Swanson, K. Centralization of the radial club hand: An ulnar surgical approach. J. Hand Surg. 1981, 6, 423–433. [Google Scholar] [CrossRef]
- Goldfarb, C.A.; Murtha, Y.M.; Gordon, J.E.; Manske, P.R. Soft-Tissue Distraction With a Ring External Fixator Before Centralization for Radial Longitudinal Deficiency. J. Hand Surg. 2006, 31, 952–959. [Google Scholar] [CrossRef]
- Kanojia, R.K.; Sharma, N.; Kapoor, S.K. Preliminary Soft Tissue Distraction Using External Fixator in Radial Club Hand. J. Hand Surg. Eur. 2008, 33, 622–627. [Google Scholar] [CrossRef]
- Pfister, G.; Le Hanneur, M.; Bachy, M.; Fitoussi, F. Radial club hand treated with soft-tissue distraction and subsequent pin stabilization: Mid- to long-term results. J. Hand Surg. Eur. 2020, 45, 729–736. [Google Scholar] [CrossRef]
- Romaña, C.; Ciais, G.; Fitoussi, F. Treatment of severe radial club hand by distraction using an articulated mini-rail fixator and transfixing pins. Orthop. Traumatol. Surg. Res. 2015, 101, 495–500. [Google Scholar] [CrossRef][Green Version]
- Manske, M.C.; Wall, L.B.; Steffen, J.A.; Goldfarb, C.A. The Effect of Soft Tissue Distraction on Deformity Recurrence after Centralization for Radial Longitudinal Deficiency. J. Hand Surg. 2014, 39, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Paley, D. Shortening: The orthopedic theory of relativity. J. Limb Lengthening Reconstr. 2020, 6, 1. [Google Scholar] [CrossRef]
- Damore, E.; Kozin, S.H.; Thoder, J.J.; Porter, S. The recurrence of deformity after surgical centralization for radial clubhand. J. Hand Surg. 2000, 25, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Lahiji, F.A.; Asgari, F.; Mirzaee, F.; Zafarani, Z.; Aslani, H. Clinical and functional results of radial club hand with centralization and pollicization using the second metacarpus: A clinical case series. Int. J. Surg. Case Rep. 2019, 61, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Mazhar, F.N.; Shariatzadeh, H.; Balvardi, M.; Amroodi, M.N.; Mirzaei, A. Recurrence rate of radial deviation following the centralization surgery of radial club hand. Med. J. Islam. Repub. Iran 2018, 32, 100–104. [Google Scholar] [CrossRef]
- Mittal, S.; Garg, B.; Mehta, N.; Kumar, V.; Kotwal, P. Randomized Trial Comparing Preliminary Results of Radialization and Centralization Procedures in Bayne Types 3 and 4 Radial Longitudinal Deficiency. J. Pediatr. Orthop. 2020, 40, 509–514. [Google Scholar] [CrossRef]
- Das, S.P.; Ganesh, G.S. Outcome of Centralization and Ulnarization of the Carpus with Ulnar Shortening Osteotomy on Functioning in Children with Radial Club Hand. Indian J. Orthop. 2020, 54, 87–96. [Google Scholar] [CrossRef]
- Bhat, A.K.; Acharya, A.; Nahas, N. Radialization With Ulnar Cuff Osteotomy: A Technique for Deformity Correction in Radial Longitudinal Deficiency. J. Hand Surg. 2018, 43, 293.e1–293.e7. [Google Scholar] [CrossRef]
- Vilkki, S.K. Vascularized Metatarsophalangeal Joint Transfer for Radial Hypoplasia. Semin. Plast. Surg. 2008, 22, 195–212. [Google Scholar] [CrossRef]
- Yang, J.; Qin, B.; LiQiang, G.; Fu, G.; Xiang, J.; Gu, L. Vascularized Proximal Fibular Epiphyseal Transfer for Bayne and Klug Type III Radial Longitudinal Deficiency in Children. Plast. Reconstr. Surg. 2015, 135, 157e–166e. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Thumb | Syndrome | Sex | Involvement | Side | Age at Surgery (Months) | Follow-Up (Months) |
|---|---|---|---|---|---|---|---|
| 1 | Hypoplastic | Female | Unilateral | Right | 37 | 19 | |
| 2 | Absent | VACTRL | Female | Unilateral | Left | 28 | 19 |
| 3 | Absent | Female | Unilateral | Right | 29 | 19 | |
| 4 | Normal | TAR | Male | Bilateral | Left | 32 | 19 |
| 5 | Normal | TAR | Male | Bilateral | Right | 32 | 19 |
| 6 | Normal | Male | Unilateral | Right | 18 | 19 | |
| 7 | Normal | TAR | Female | Bilateral | Left | 19 | 15 |
| 8 | Normal | TAR | Female | Bilateral | Right | 19 | 15 |
| 9 | Normal | TAR | Male | Bilateral | Left | 25 | 15 |
| 10 | Normal | TAR | Male | Bilateral | Right | 25 | 15 |
| 11 | Normal | TAR | Female | Bilateral | Left | 17 | 15 |
| 12 | Normal | TAR | Female | Bilateral | Right | 17 | 15 |
| 13 | Absent | Female | Unilateral | Left | 26 | 12 | |
| 14 | Normal | TAR | Male | Unilateral | Right | 21 | 12 |
| 15 | Normal | TAR | Male | Bilateral | Left | 23 | 8 |
| 16 | Normal | TAR | Male | Bilateral | Right | 23 | 8 |
| 17 | Hypoplastic | Male | Unilateral | Right | 25 | 8 | |
| 18 | Normal | Male | Unilateral | Left | 18 | 7 | |
| 19 | Absent | Female | Unilateral | Right | 19 | 7 | |
| 20 | Normal | Male | Unilateral | Right | 21 | 3 | |
| 21 | Normal | Female | Unilateral | Left | 18 | 3 | |
| 22 | Absent | Male | Unilateral | Right | 52 | 3 |
| Case No. | Total ROM (Flex. + Ext.) | HFA Pre-Op | HFA Post-Op | HFA Follow-Up | HFA Correction |
|---|---|---|---|---|---|
| 1 | 83 | 76.2 | 12.8 | 14.4 | 63.5 |
| 2 | 44 | 88.4 | 8.9 | 12.4 | 79.5 |
| 3 | 76 | 85.1 | 10.9 | 11.3 | 74.1 |
| 4 | 69 | 95.8 | 9.4 | 12.4 | 86.4 |
| 5 | 56 | 82.2 | 6.3 | 9.1 | 75.9 |
| 6 | 98 | 76.3 | 10.7 | 13.4 | 65.7 |
| 7 | 64 | 96.2 | 7.4 | 9.2 | 88.7 |
| 8 | 78 | 95.2 | 9.7 | 12.2 | 85.5 |
| 9 | 86 | 67.4 | 9.1 | 10.2 | 58.3 |
| 10 | 90 | 81.0 | 7.5 | 13.2 | 73.5 |
| 11 | 78 | 68.1 | 9.9 | 12.4 | 58.2 |
| 12 | 92 | 74.7 | 8.1 | 9.4 | 66.6 |
| 13 | 84 | 92.4 | 9.2 | 12.9 | 83.2 |
| 14 | 75 | 74.3 | 4.2 | 7.3 | 70.1 |
| Case No. | Ulnar Bow Pre-Op | Ulnar Bow Post-Op | Ulnar Length Pre-Op (cm) | Ulnar Length Post-Op (cm) | Ulnar Length at Follow-Up (cm) | Shortening (cm) | Growth (cm/year) |
|---|---|---|---|---|---|---|---|
| 1 | 1.3 | 0.3 | 9.3 | 7.6 | 9.5 | 1.7 | 1.9 |
| 2 | 0.5 | 0.4 | 8.2 | 6.8 | 8.3 | 1.4 | 1.5 |
| 3 | 12.5 | 3.9 | 7.8 | 6.2 | 7.4 | 1.6 | 1.2 |
| 4 | 17.5 | 5.3 | 9.0 | 7.4 | 9.2 | 1.6 | 1.8 |
| 5 | 19.4 | 6.2 | 8.7 | 7.2 | 9.1 | 1.5 | 1.9 |
| 6 | 4.5 | 0.5 | 6.9 | 5,74 | 7.3 | 1.2 | 1.6 |
| 7 | 11.1 | 3.3 | 7.4 | 6.1 | 7.5 | 1.3 | 1.4 |
| 8 | 10.4 | 4.2 | 7.5 | 5.9 | 7.3 | 1.6 | 1.4 |
| 9 | 5.4 | 1.1 | 7.5 | 6.4 | 7.7 | 1.1 | 1.3 |
| 10 | 3.4 | 3.3 | 7.5 | 6.3 | 7.3 | 1.2 | 1.0 |
| 11 | 16.6 | 0.8 | 7.3 | 4.7 | 5.4 | 2.6 | 0.7 |
| 12 | 18.5 | 8.4 | 7.2 | 4.5 | 3.8 | 2.7 | No Growth |
| 13 | 5.5 | 6.2 | 7.9 | 6.2 | 6.9 | 1.7 | 0.7 |
| 14 | 7.3 | 8.2 | 8.1 | 7.1 | 8.1 | 1.1 | 1.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deszczynski, J.M.; Albrewczynski, T.; Shannon, C.; Paley, D. Radial Club Hand Treated by Paley Ulnarization Generation 3: Is This the New Centralization? Children 2021, 8, 562. https://doi.org/10.3390/children8070562
Deszczynski JM, Albrewczynski T, Shannon C, Paley D. Radial Club Hand Treated by Paley Ulnarization Generation 3: Is This the New Centralization? Children. 2021; 8(7):562. https://doi.org/10.3390/children8070562
Chicago/Turabian StyleDeszczynski, Jaroslaw M., Tomasz Albrewczynski, Claire Shannon, and Dror Paley. 2021. "Radial Club Hand Treated by Paley Ulnarization Generation 3: Is This the New Centralization?" Children 8, no. 7: 562. https://doi.org/10.3390/children8070562
APA StyleDeszczynski, J. M., Albrewczynski, T., Shannon, C., & Paley, D. (2021). Radial Club Hand Treated by Paley Ulnarization Generation 3: Is This the New Centralization? Children, 8(7), 562. https://doi.org/10.3390/children8070562